www.reumatologia.com.br
REVISTA BRASILEIRA DE
REUMATOLOGIA
Original article
The modiied US7 score in the assessment of synovitis in
early rheumatoid arthritis
José Alexandre Mendonça
a,*, Michel Alexandre Yazbek
a, Beatriz Lavras Costallat
b,
Marwin Gutiérrez
c, Manoel Barros Bértolo
aa Department of Rheumatology, Universidade Estadual de Campinas, Campinas, SP, Brazil
b Radiology Department, Hospital Vera Cruz, Campinas, SP, Brazil c Università Politecnica delle Marche, Jesi, Ancona, Italy
a r t i c l e i n f o
Article history:
Received 8 November 2013 Accepted 19 March 2014
Keywords:
Ultrasound Synovitis
Early Rheumatoid arthritis Score
a b s t r a c t
Objective:To evaluate the modiied US7 score (MUS7 score SYN) in the assessment of pa-tients with early rheumatoid arthritis (ERA). In addition, dorsal and palmar recesses of the wrists as well as of small joints of the hands and feet were examined for the presence of synovitis by means of a global assessment of joints.
Methods: The study sample comprised 32 patients treated for arthritis, with an average di-sease duration of 13 months. An ultrasound machine with high frequency transducer was used. Hands were also X-rayed and analysed by Larsen score.
Results:Out of the 832 examined joints, synovitis was detected in 173 (20,79%), tenosyno-vitis in 22 (4,91%), and erosions in 3 (1,56%). Synotenosyno-vitis was predominantly detected in the dorsal recess (73,38%) of MCP and PIP joints, when compared with palmar recess (26%). The presence of synovitis in the joints evaluated correlated with clinical (HAQ-DI, DAS28), laboratory (ACPA, RF, CRP), and ultrasound results (r = 0,37 to r = 0,42; p = 0,04 to p = 0,003). We found correlation of the MUS7 score SYN of the gray scale US or of the power Doppler US with DAS28 (PCR) values (r = 0,38; p = 0,0332), and with CRP results (r = 0,39; p = 0,0280), respectively.
Conclusion: The dorsal recess, the wrist, and small joints can be considered as important sites to detect synovitis by the MUS7 score SYN in patients with ERA.
© 2014 Sociedade Brasileira de Reumatologia. Published by Elsevier Editora Ltda. All rights reserved.
* Corresponding author.
E-mail: [email protected] (J.A. Mendonça).
Escore US7 modiicado na avaliação de sinovite em pacientes com artrite reumatoide inicial
Palavras-chave:
Ultrassom Sinovite
Artrite reumatoide inicial Escore
r e s u m o
Objetivo: Avaliar o escore US7 modiicado (escore MUS7 SIN) na avaliação de pacientes com artrite reumatoide inicial (ARI). Além disso, foram examinados recessos dorsais e palmares dos punhos, bem como pequenas articulações das mãos e dos pés, para o diagnóstico de sinovite, mediante uma avaliação global das articulações.
Métodos: A amostra do estudo compreendeu 32 pacientes tratados para artrite, com 13 me-ses como duração média da doença. Foi utilizado um aparelho de ultrassonograia (US) com transdutor de alta frequência. As mãos dos participantes também foram radiografadas e analisadas pelo escore de Larsen.
Resultados: Nas 832 articulações examinadas, detectou-se sinovite em 173 (20,79%), tenossi-novite em 22 (4,91%) e erosões em três (1,56%). A sitenossi-novite foi predominantemente detectada no recesso dorsal (73,38%) das articulações MCF e IFP, quando comparado com o recesso palmar (26%). A presença de sinovite nas articulações avaliadas teve correlação com os re-sultados clínicos (HAQ-DI, DAS28), laboratoriais (anti-PCC, FR, PCR) e ultrassonográicos (r = 0,37 a r = 0,42; p = 0,04 a p = 0,003). Encontramos correlação do escore MUS7 SIN para US na técnica da escala de cinzas (gray scale)ou na técnica de Doppler de amplitude (power Dop-pler) com os valores do instrumento DAS28 (PCR) (r = 0,38; p = 0,0332) e com os resultados da PCR (r = 0,39; p = 0,0280), respectivamente.
Conclusão: O recesso dorsal, o punho e as pequenas articulações podem ser considerados como locais importantes para a detecção de sinovite pelo escore MUS7 SIN em pacientes com ARI.
© 2014 Sociedade Brasileira de Reumatologia. Publicado por Elsevier Editora Ltda. Todos os direitos reservados.
Introduction
Rheumatoid arthritis (RA) is a chronic inlammatory and sys-temic disease that results in structural damage of synovium, cartilage, and bone. Because it is a chronic and progressive disease, it may result in joint deformities with functional loss and may compromise quality of life.
Early detection and careful characterization of the inlam-matory process play a key role in both diagnostic and thera-peutic procedures in RA.1 Currently, the most commonly used
clinical instrument to determine the disease activity in RA patients is the 28-joint count Disease Activity Score (DAS28), which indirectly denotes the joint inlammatory status.2,3
Ultrasound (US) is a sensitive imaging technique for as-sessment of anatomical changes, disease activity, and ther-apy eficacy in patients with RA. Its sensitivity is greater than that of other imaging techniques in the early detection of aggressive arthritis and surveillance of disease activity.4-6
Moreover, US is patient-friendly, safe and non-invasive, free of ionizing radiation, less expensive, and allows multiple tar-get assessment in real time, besides therapeutic changes.7-10
The semiquantitative US scoring system, US7 score, has been proposed to assess established RA and other inlammatory arthropathies.11 It was developed to standardize the US
ex-amination in daily rheumatologic practice and in multicenter studies. The US7 score includes the assessment of 7 joints us-ing palmar and dorsal scan of the clinically dominant hand and foot including: wrist, second and third metacarpophalan-geal (MCP) joints, second and third proximal interphalanmetacarpophalan-geal (PIP) joints, and second and ifth metatarsophalangeal (MTP)
joints. These joints have been evaluated for synovitis, tenosy-novitis, paratenonitis, and bone erosion by semiquantitative scoring systems including grayscale (GS) and power Doppler (PD) techniques.12
To date, there are evidence demonstrating the ability of ultrasonography to detect synovitis in patients with early rheumatoid arthritis (ERA).13 Moreover, there is no consensus
on which recess, dorsal or palmar, is the most sensitive for detecting synovitis by PD or GS. The aim of this study was to evaluate the feasibility of modiied US7 score (MUS7 score SYN) in the assessment of synovitis in patients with ERA. In addition, dorsal and palmar recesses of the wrists and the small joints of the hands and feet were evaluated for the pres-ence of synovitis by means of global assessment of joints.
Material and methods
Patients
Thirty-nine ERA patients (30 women and 9 men) attending the outpatient and inpatient clinics of the Rheumatology De-partment of Universidade Estadual de Campinas – UNICAMP – Campinas, São Paulo, Brazil, during a 2-year period were enrolled in this study. Inclusion criteria were as follows: age ≥20 years; ≥3 months and <24 months of disease history, ac-cording to the ACR 1987 revised criteria;14 and the presence of
synovitis in at least one joint by US examination, according to 2010 ACR/EULAR Rheumatoid Arthritis Classiication Cri-teria.15 Seven patients were excluded from the study because
to OMERACT criteria.12 Thus, a total of 32 patients (24 women
and 8 men) with diagnosis of ERA comprised the inal sample. The study was approved by the Research Ethics Committee of the State University of Campinas (UNICAMP). The patients signed the Informed Consent and were informed about the guidelines for participation in the study.
Clinical and laboratory assessment
The following clinical data were obtained: age, sex, race, time of onset of pain and articular swelling, dosage and duration of glucocorticoid treatment, and use of biological and disease-modifying anti-rheumatic drugs (DMARDs). Patients were then blindly evaluated by a rheumatologist, by counting and recording the number of joints with swelling and tender to calculate the DAS28 (CRP) score. The patients were asked to ill in the health assessment questionnaire (HAQ).
All patients underwent the following laboratory tests: ESR, CRP, rheumatoid factor, and anti-cyclic citrullinated peptide (ACPA).
X-ray assessment
Conventional X-ray of wrists and hands was performed in anteroposterior projection. The radiographs were scored us-ing the modiied Larsen method and the feet were not evalu-ated this study. Joints received the following grades: grade 0 – normal, grade I – mild abnormality (presence of one or more of the following lesions: edema of soft tissues, osteopenia around the joint, and a slight decrease in joint space); grade II – deinite abnormality (presence of small erosions, decreased joint space is not obligatory), grade III – marked abnormality (presence of erosions and decreased joint space), grade IV – se-vere abnormality (the original joint surface remains partially preserved), and grade V – mutilating abnormality (the original joint surface has disappeared; huge deformity is present).16,17
US assessment
US examinations were performed using a General Electric LOGIQ Book XP Ultrasound machine (USA) equipped with a high frequency (8-10 MHz) linear transducer.
All joints were scanned using a multiplanar technique, adopting the indications provided by the EULAR guidelines for musculoskeletal ultrasound in rheumatology.18 In brief,
the dorsal aspect of the wrist, and dorsal and palmar scans of MCP and PIP joints were examined by US with the patient seated with hands lying in prone position on the examina-tion table. The longitudinal dorsal scan of MTP joints was per-formed with the patient supine and legs bent at the knee.
The longitudinal scan was performed moving the trans-ducer slightly from radial to ulnar on dorsal and palmar aspect to enable maximum coverage of the anatomical surface area.
US grayscale imaging parameters were set to obtain the maximal contrast between all the structures under examina-tion. PD settings were standardized at the following values: pulse repetition frequency: 800-900 MHz, frequency PD: 5.5 MHz and low wall ilter: Color gain was set just below the level at which color noise appeared in the underlying bone (no low should be visualized at the bony surface).
OMERACT preliminary deinitions were adopted for the identiication of synovial luid and synovial hypertrophy.12
GS and PD for each target was graded on the basis of the semiquantitative scoring systems previously adopted. GS sy-novitis was scored as follows: 0 – absence, 1 – mild (describes a small hypoechoic or an echoic line beneath the joint cap-sule), 2 – moderate (the joint capsule is elevated parallel to the joint area), and 3 – severe or marked (characterizes the strong extensional of the joint capsule). PD indings were scored as follows: 0 – absence (no intra-articular color signal), 1 – mild (single signals or a conluent signal in the intra-articular area), 2 – moderate (greater than grade 1 to <50% of the intra-articular area illed with colour signals), and 3 – marked (≥50% of the intra-articular area illed with color signals) (Fig. 1).19
The inter and intraobserver reliability of the US7 score showed moderate to substantial kappa values and good agreements and the median overall kappa for detecting sy-novitis was 0.51.20
The US7 score includes a combination of semiquantitative GS and PD indings obtained by a formula that includes the sum of different parameters.11 Its score ranges from 0 to 39 for
GS, and from 0 to 39 for PD.
GS_synovitis (GSUS-Score 7) = GS_D _wrist + GS_P _wrist + GS_U _wrist + GS_D_MCP2 + GS_P_MCP2 + GS_D_MCP3 + GS_P_MCP3 + GS_D_PIP2 + GS_P_ PIP2 + GS_D_PIP3 + GS_P_PIP3 + GS_D_MTP2 + GS_D_MTP5 = 13 (scanning) x 3 (highest GS score 0-3) = 39.
PD_synovitis (PDUS-Score 7) = PD_D_wrist + PD_P_wrist + PD_U_wrist + PD_D_MCP2 + PD_P_ MCP2 + PD_D_MCP3 + PD_P_MCP3 + PD_D_PIP2 + PD_P_PIP2 + PD_D_PIP3 + PD_P_PIP3 + PD_D_MTP2 + PD_D_MTP5 = 13 (scanning) x 3 (highest PD score 0-3 ) = 39.
(1)
GS, grayscale; D, dorsal scan; P, palmar scan; U, ulnar scan; MCP, metacarpophalangeal joint; PIP, phalangeal interproxi-mal; MTP, metatarsophalangeal joint; PD, power Doppler.
We developed a simpliied US7 score for exclusive asses-ment of synovitis. It does not consider the synovial evaluation of the palmar and ulnar recesses of the wrist joint, and of pal-mar recess of the small joints for PD. The modiied US7 score ranges from 0 to 33 for GS, and 0 to 21 for PD, and is calculated according to the following formula:
GS_synovitis (GSUS-MUS7 score SYN) = GS_DC _wrist + GS_D_MCP2 + GS_P_MCP2 + GS_D_MCP3 + GS_P_MCP3 + GS_D_PIP2 + GS_P_PIP2 + GS_D_PIP3 + GS_P_PIP3 + GS_D_MTP2 + GS_D_MTP5 = 11
(scan-ning) x 3(highest GS score 0-3) = 33(max GS SYN)
PD_synovitis (PDUS-MUS7 score SYN) = PD_DC_ wrist + PD_D_MCP2 + PD_D_MCP3 + PD_D_PIP2 + PD_D_PIP3 + PD_D_MTP2 + PD_D_MTP5 = 7(scanning) x 3(highest PD score 0-3) = 21(max PD SYN)
(2)
SYN, modii ed US7 Score for synovitis; max GS SYN, maxi-mum possible score using grayscale; max PD SYN, maximaxi-mum possible score using power Doppler.
Statistical analysis
The statistical analysis was performed with SAS System for Windows, version 9.2 (SAS Institute Inc, 2002-2008, Cary, NC, USA).
We performed a descriptive statistical analysis, present-ing frequency tables for categorical variables and measures of position and dispersion for numerical variables. The Mann-Whitney test was used for comparison of continuous and sequential measurements between the two clinical groups (pain and swelling of joints). The Spearman correlation coef-i ccoef-ient was used to vercoef-ify the lcoef-inear correlatcoef-ion between the variables. The chi-square or Fisher exact tests were used to assess the association or to compare proportions, when nec-essary. The weighted Kappa coefi cient was used as a mea-sure of agreement between observers.
Results
Thirty-two patients (8 male and 24 female) were included in the study, with an average age of 32.5 years. Two patients (6.2%) were smokers. Comorbidities were observed in 3 patients (9.3%): one was diagnosed with hypothyroidism, other with hy-perthyroidism, and another with type 2 diabetes.
The average duration of the disease was 13.2 months. Table 1 shows demographic, clinical, and laboratory data.
Five (15.6%) patients were in clinical remission according to DAS28-CRP ≤2.6.
Twenty (62.5%) patients were treated with 12.5 to 25.0 mg methotrexate, 19 (59.3%) with 5 to 20 mg prednisone, and 1 (3.1%) with biological agent. Seven (21.8%) patients were not using corticosteroids, disease-modifying anti-rheumatic drugs (DMARDs), or biological agents at the time of US examination.
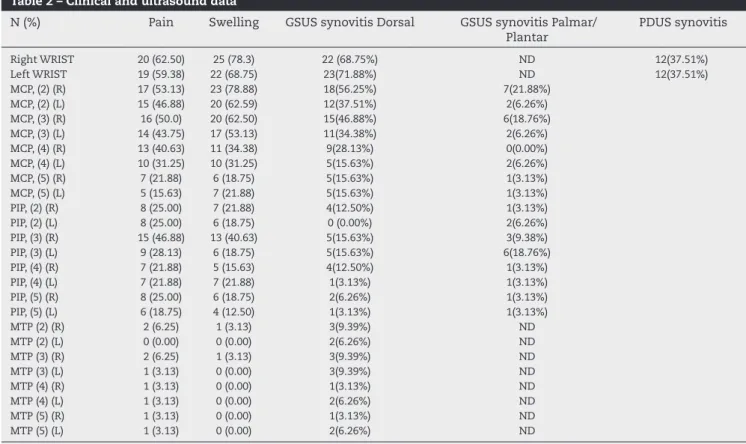
A total of 832 joints were examined, resulting in 173 (20.8%) joint recesses with synovitis. GSUS-examination revealed sy-novitis in 22 (68.7%) right wrist joints, in 23 (71.8%) left wrist joints, and an increased synovial involvement of MCP (2) (right) in 17 joints (53.1%), of MCP (2) (left) in 11 joints (34.3%); of MCP (3) (right) in 14 joints (43.7%), and of MCP (3) (left) in 12 joints (37.5%). In addition, 102 (73.3%) and 37 (26.1%) cases of synovi-tis were respectively detected in the dorsal and in the palmar recesses between MCP and PIP joints (Table 2).
On a semiquantitative scale, active synovitis was scored 2 by PDUS, 9 (28.1%) in the left and 5 (15.6%) in the right wrist, featuring a moderate inl ammatory activity in the wrists. Syno-vitis was graded 2 by GSUS, 6 (18.7%) and 4 (12.5%) in the dorsal recess of right and left MCP (2) joints, respectively.
Subclinical synovitis was depicted in 6 (9.3%) wrists in DAS28 remission patients (DAS28 ≤2.6).
Comparison between clinical and US fi ndings
For joints such as right wrists and certain small joints of the hands, the comparison of clinical and US i ndings revealed Fig. 1 – Synovitis identii ed by grayscale (GS) ultrasound and power Doppler (PD) ultrasound.
a = grade 0; b = grade 1; c = grade 2; d = grade 3. T: tendon; S: synovitis; R: radius; L: lunate; C: capitate bone; c: cartilage; D: dorsal; P: palmar
R
R L
L
C C
C C
T
T
T R
R
R R
R R
S
S
S
C C
L
L C L
S C L
L
L
C
T
T T
T
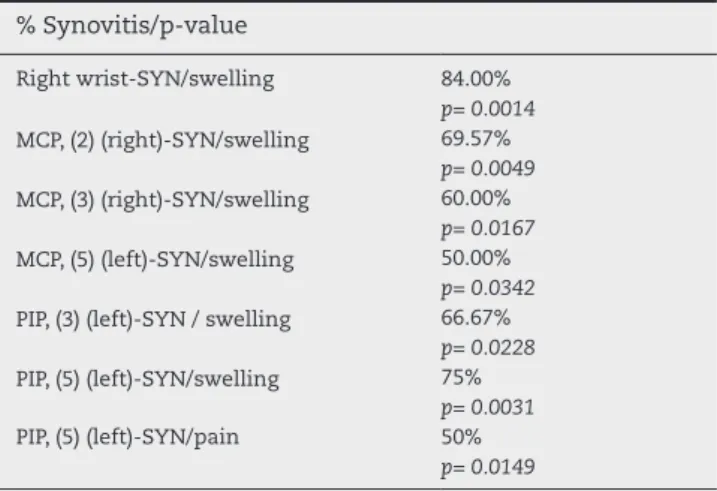
that in 50% to 84% of the cases, swelling was associated with the presence of synovitis, as detected by US. In 50% of the cases, pain was found to be associated with the presence of synovitis in the PIP (5) (left) joint. No association was found for other examined joints (Table 3).
Clinical, laboratory, and imaging correlations
Positive, signiicant and moderate correlations were found for the presence of synovitis as detected by GSUS-examination of wrist with CRP results (r=0.42; p=0.0163),and for synovitis in the small joints of the toes, as detected by GSUS-examination, with HAQ-DI, RF, and CRP results (r=0.37 to 0.42; p=0.0161 to 0.0337). PDUS-examination of wrist correlated with CRP re-sults (r=0.40; p=0.00337) (Table 4).
A signiicant correlation was found between the presence of synovitis in the palmar recess of MCP (2) (right) and the period of treatment, or the dose of methotrexate (MTX) used (r=-0.36 to -0.37; p=0.0445 to p=0.0368).
In the evaluation of the MUS7 score SYN, we found a sig-niicant, moderate, and positive correlation between GSUS MUS7 score SYN and DAS28 (CRP) values (r=0.38; p=0,0332), and between PDUS MUS7 score SYN and CRP results (r=0.39; p=0.0280).
There was an overall disagreement between rheumatolo-gist’s evaluation of ultrasound and X-ray indings, as demon-strated by the variation of kappa coeficient from -0.2000 95% CI (-0.4972, 0.0972) to 0.3333 95% CI (0.0469, 0.7136).
Concerning the Larsen radiographic scoring, a good agree-ment was observed between Reader 1 (rheumatologist) and
Table 1 – Demographic data
Demographic data Mean ± SD Minimum Maximum Median
Disease duration (months) 13.2 ± 8.1 3 24 10
Age 42±14.6 20 75 45
DAS28 (CRP) 4.0±1.2 1.2 6.7 3.9
HAQ 1.2±0.7 0.0 2.9 1.3
ACPA (IU/dL) 137.2±95.8 0.0 250 161.9
RF (IU/dL) 195.4±435.1 0.0 2180 23.5
ESR (mm/h 1st) CRP (mg/dL)
34± 33 8.1±13.6
1.0 0
112 56
28 1.8
DAS28, Disease Activity Score 28; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein;
HAQ, health assessment questionnaire score; ACPA, anti-cyclic citrullinated peptide; RF, rheumatoid factor.
Table 2 – Clinical and ultrasound data
N (%) Pain Swelling GSUS synovitis Dorsal GSUS synovitis Palmar/
Plantar
PDUS synovitis
Right WRIST 20 (62.50) 25 (78.3) 22 (68.75%) ND 12(37.51%)
Left WRIST 19 (59.38) 22 (68.75) 23(71.88%) ND 12(37.51%)
MCP, (2) (R) 17 (53.13) 23 (78.88) 18(56.25%) 7(21.88%)
MCP, (2) (L) 15 (46.88) 20 (62.59) 12(37.51%) 2(6.26%)
MCP, (3) (R) 16 (50.0) 20 (62.50) 15(46.88%) 6(18.76%)
MCP, (3) (L) 14 (43.75) 17 (53.13) 11(34.38%) 2(6.26%)
MCP, (4) (R) 13 (40.63) 11 (34.38) 9(28.13%) 0(0.00%)
MCP, (4) (L) 10 (31.25) 10 (31.25) 5(15.63%) 2(6.26%)
MCP, (5) (R) 7 (21.88) 6 (18.75) 5(15.63%) 1(3.13%)
MCP, (5) (L) 5 (15.63) 7 (21.88) 5(15.63%) 1(3.13%)
PIP, (2) (R) 8 (25.00) 7 (21.88) 4(12.50%) 1(3.13%)
PIP, (2) (L) 8 (25.00) 6 (18.75) 0 (0.00%) 2(6.26%)
PIP, (3) (R) 15 (46.88) 13 (40.63) 5(15.63%) 3(9.38%)
PIP, (3) (L) 9 (28.13) 6 (18.75) 5(15.63%) 6(18.76%)
PIP, (4) (R) 7 (21.88) 5 (15.63) 4(12.50%) 1(3.13%)
PIP, (4) (L) 7 (21.88) 7 (21.88) 1(3.13%) 1(3.13%)
PIP, (5) (R) 8 (25.00) 6 (18.75) 2(6.26%) 1(3.13%)
PIP, (5) (L) 6 (18.75) 4 (12.50) 1(3.13%) 1(3.13%)
MTP (2) (R) 2 (6.25) 1 (3.13) 3(9.39%) ND
MTP (2) (L) 0 (0.00) 0 (0.00) 2(6.26%) ND
MTP (3) (R) 2 (6.25) 1 (3.13) 3(9.39%) ND
MTP (3) (L) 1 (3.13) 0 (0.00) 3(9.39%) ND
MTP (4) (R) 1 (3.13) 0 (0.00) 1(3.13%) ND
MTP (4) (L) 1 (3.13) 0 (0.00) 2(6.26%) ND
MTP (5) (R) 1 (3.13) 0 (0.00) 1(3.13%) ND
MTP (5) (L) 1 (3.13) 0 (0.00) 2(6.26%) ND
Reader 2 (radiologist) in the evaluation of some joints, such as the MCP (2) (right) and MCP (3) (left), as demonstrated by the variation of kappa coeficient from -0.062, 95% CI (-0.4020, 0.2775) to 0.473 95% CI (0.1134, 0.8340).
Discussion
In this study, we demonstrated the use of a modiied US7 score in the assessment of synovitis in ERA. Moreover, as shown by our results, the dorsal recess, the wrist, and small joints can be considered as appropriate sites to detect synovitis by the MUS7 score SYN in patients with ERA.
The inlammatory process in RA is generally identiied by means of the clinical history, physical examination, and lab results, which can be characterized by an array of
quality-of-life instruments that may not always identify synovitis in its full activity. By the time it is detected by X-ray, the disease has already caused structural damage to the bone, with early le-sions such as the presence of luids and synovial cell prolifera-tion.21-24
The dissociation between clinical indings and US-detected synovial damage is even greater, including cases of remission in which clinical indings were not able to pinpoint the inlam-matory inactivity. This study showed that 15.6% of patients in clinical remission presented synovitis with PD positive signal. Indeed, it has been shown that around 8% of patients in clini-cal remission have subcliniclini-cal synovitis by US examination.25,26
Prospective longitudinal studies have clearly demonstrated that US, along with MRI, is more effective in identifying cases of remission, subclinical activity in asymptomatic patients, progression of structural damage, and improvement of syno-vitis, highlighting its superior sensitivity and accuracy com-pared to other methods, which enables an earlier intervention on the inlammatory activity of RA, and in the treatments ad-opted.27,28 Studies have shown 75% to 79% agreement between
US and MRI in the detection of synovitis, pointing to the diag-nostic reliability of this method.29 A recent study showed that
both techniques have good diagnostic performance for ERA.30
In the global evaluation of the 832 joints, we found that the wrist was the most affected by moderately active synovitis, as detected by PD.31 GSUS-examination of the MCP and PIP joints
of hands revealed a higher number of cases of synovitis in the dorsal recesses than in the palmar recesses. We found posi-tive, signiicant and moderate correlations between the pres-ence of synovitis of the right wrist, as detected by GSUS, of MTP (4)(left) joints, by PDUS and CRP results. This fact charac-terizes CRP as an indicator of synovial inlammatory activity detected by US.
This study showed that for most of the joints, joint swell-ing as a clinical indswell-ing compares to the presence of synovitis as detected by US. We found negative correlation between the presence of synovitis in MCP (2) joints and the use of medica-tion: the higher the dose and duration of methotrexate treat-ment, the lower the detection of synovitis by US. This inding suggests that additional longitudinal studies should be carried out to conirm MTX as an effective DMARD in the initial dis-ease.
Regarding the evaluation of the 7 joints to elaborate the MUS7 score SYN, we found positive correlation between the simpliied score results with DAS28 (CRP) and CRP results. Even though the MUS7 score SYN includes the analysis of only 7 joints, as it excludes the evaluation of the palmar and ulnar recesses of the wrist joint, these results demonstrate that the dorsal recess is indicated for the detection of GS and PD sy-novitis.
The choice of some joints and dorsal recesses is considered promising for the diagnosis of synovitis in the early stage of ERA, when the disease is commonly misdiagnosed, resulting in uncertainty concerning treatment decisions, such as the type of treatment and the time to start it.32 US-examination
of wrists and dorsal recess for the detection of synovitis was shown to be an important tool to conirm or to complement the ERA diagnosis, given that these were the joints that showed the worst synovial damage. Erosion was not much evident in our sample, possibly because we evaluated the disease at an Table 3 – Descriptive analysis and comparation between
clinical and US indings on synovitis % Synovitis/p-value
Right wrist-SYN/swelling 84.00%
p= 0.0014
MCP, (2) (right)-SYN/swelling 69.57%
p= 0.0049
MCP, (3) (right)-SYN/swelling 60.00%
p= 0.0167
MCP, (5) (left)-SYN/swelling 50.00%
p= 0.0342
PIP, (3) (left)-SYN / swelling 66.67%
p= 0.0228
PIP, (5) (left)-SYN/swelling 75%
p= 0.0031
PIP, (5) (left)-SYN/pain 50%
p= 0.0149
SYN, Synovitis; MCP, Metacarpophalangeal joint; PIP, inter-proximal phalangeal
Table 4 – Correlation of US data with clinical and laboratorial data on synovitis
r/p-value
GSUS D of right wrist/CRP r= 0.42
p= 0.0163
PDUS D of right wrist/CRP r = 0.40
p= 0.00337
GSUS D-MTP (2) (right)/RF r= 0.40
p= 0.0245
GSUS D-MTP (3) (right)/HAQ- DI r= 0.37
p= 0.0354
GSUS D-MTP (4) (right)/HAQ- DI r= 0.38
p= 0.0337
GSUS D-MTP, (4) (left)/CRP r= 0.42
p= 0.0161
PDUS D-of right wrist/ACPA r= -0.38
p= 0.0412
GSUS D-PIP (2) (right)/HAQ-DI r= -0.35
p= 0.0478
early stage.33-35 Wrist, MCP2 and MCP3 were the joints that
were more affected by synovial inlammation in comparison to other joints. Our MUS7 score SYN results indicate the wrist and MCP2 as the most promising joints for ERA diagnosis and clinical follow-up. However, longitudinal studies are needed to validate this new score for synovitis identiication in ERA.
Regarding clinical indings, we found that in 50% to 84% of the studied cases, joint swelling was associated with the pres-ence of synovitis as detected by US. CRP can be considered a signiicant indicator of the presence of synovial inlammation, as conirmed by the images. The results obtained by means of the MUS7 score SYN in the evaluation of initial synovial in-lammatory activity were associated with clinical and labora-tory indings, once again indicating this modiied score as an important tool for the initial diagnosis, and for the follow-up of patients with ERA. Active synovitis of the hands as detected by PDUS, analysed separately or along with 7 other joints by the MUS7 score SYN, can be an important predictor of the sy-novial damage in ERA, as demonstrated by the correlation be-tween PDUS and CRP results. The dorsal recess can be consid-ered an important site to detect active synovitis by PD and GS.
US is more precise than clinical examination in synovitis. US score shows some fundamental characteristics such as re-producibility, viability, and sensitivity to change over time like was observed in the systematic review study.36
MUS7 score SYN was proven to be very useful if adopted in daily clinical practice, for the dianogsis and therapeutic man-agement of patients with ERA, future studies may better vali-date this score to evaluate synovitis.
Acknowledgements
Professor Ana Terezinha Guillaumon, Department of Vascular Surgery, School of Medical Sciences, Universidade Estadual de Campinas for allowing the use of the ultrasound machine.
Conlicts of interest
The authors declare no conlicts of interest.
R E F E R E N C E S
1. Sokka T, Pincus T. Quantitative joint assessment in rheumatoid arthritis. Clin Exp Rheumatol. 2005;23:S58-62.
2. Scott DL, Antoni C, Choy EH, Vanriel PLCM. Joint counts in routine practice. Rheumatology. 2003;42:919-23.
3. Hart LE, Tugwell P, Buchanan WW, Norman GR, Grace M, Southwell D. Grading of tenderness as a source of interrater error in the Ritchie articular index. J Rheumatol. 1985;12:716-7. 4. Wakeield RJ, Brown AK, O’Connor PJO, Emery P. Power
Doppler sonography: improving disease activity assessment in inlammatory musculoskeletal disease. Arthritis Rheum. 2003;48:285-8.
5. Ostergaard M, Szkudlarek M. Ultrasonography a valid method for assessing rheumatoid arthritis. Arthritis Rheum. 2005;52:681-6.
6. Balint P, Sturrock RD. Musculoskeletal ultrasound imaging: a new diagnostic tool for the rheumatologist? Br J Rheumatol. 1997;36:1141-2.
7. Hau M, Schultz H, Tony HP et al. Evaluation of pannus and vascularization of the metacarpophalangeal and proximal interphalangeal joints in rheumatoid arthritis by high-resolution ultrasound (multidimensional linear array). Arthritis Rheum. 1999;42:2303-8.
8. Walther M, Harms H, Krenn V, Radke S, Trutz-Peter F, Gohlke F. Correlation of power Doppler sonography with vascularity of the synovial tissue of the knee joint in patients with osteoarthritis and rheumatoid arthritis. Arthritis Rheum. 2001;44:331-8.
9. Ostergaard M, Court-Payen M, Gideon P et al. Ultrasonography in arthritis of the knee. A comparison with MR imaging. Acta Radiol. 1995;36:19-26.
10. Backhaus M, Ohrndorf S, Kellner H, Strunk J, Backhaus T.M, Hartung W et al. Evaluation of a Novel 7-Joint Ultrasound Score in Daily Rheumatologic Practice: A Pilot Project. Arthritis Rheum. 2009;61:1194-201.
11. Wakeield RJ, D’Agostino MA, Iagnocco A, Filippucci E, Backaus M, Scheel AK et al. OMERACT Ultrasound group priorities. J Rheumatol. 2007;34:848-51.
12. Ten Cate DF, Luime JJ, Swen N, Gerards AH, De Jager MH, Basoski NM, Hazes JM, Haagsma CJ, Jacobs JW.Role of ultrasonography in diagnosing early rheumatoid arthritis and remission of rheumatoid arthritis – a systematic review of the literature. Arthritis Res Ther. 2013 Jan 8;15:R4.
13. Arnett, FC et al. The American Rheumatism Association 1987 revised criteria for classiication of rheumatoid arthritis. Arthritis Rheum. 1988;31:315-24.
14. Aletaha et al. 2010 Rheumatoid Arthritis Classiication Criteria. An American College of Rheumatology/European League Against Rheumatism Collaborative Initiative. Arthtiis & Rheum. 2010;62:2569-2581.
15. Larsen A, Dale K, Eck M. Radiographic evaluation of rheumatoid arthritis and related conditions by standard reference ilms. Acta Radiol Diagn (Stockh). 1977;18:481-91. 16. Larsen A, Thoen J. Hand radiography in 200 patients with
rheumatoid arthritis repeated after an interval of one year. Scand J Rheumatol. 1987;6:395-401.
17. Backhaus M, Burmester GR, Gerber T, Grassi W, Machold KP, Swen WA, Wakeield RJ, Manger B. Guidelines for musculoskeletal ultrasound in rheumatology.Ann Rheum Dis. 2001;60:641-649.
18. Szkudlarek M, Court-Payen M, Strandberg C, Karlund M, Klausen T, Østergaard M. Power Doppler ultrasonography for assessment of synovitis in the metacar-pophalangeal joints of patients with rheumatoid arthritis. Arthritis Rheum. 2001;44:2018-23.
19. Ohrndorf S, Fischer IU, Kellner H, Strunk J, Hartung W, Reiche B, Burmester GR, Walther M, Schmidt WA, Backhaus M. Reliability of the novel 7-joint ultrasound score: results from an inter- and intraobserver study performed by rheumatologists. Arthritis Care Res (Hoboken). 2012 Aug;64:1238-43.
20. Naredo E, Bonilla G, Gamero F, Uson J, Carmona L, Laffon A. Assessment of inlammatory activity in rheumatoid arthritis: a comparative study of clinical evaluation with grey scale and power Doppler ultrasonography. Ann Rheum Dis. 2005;64:375-81.
21. Szkudlarek M, Narvestad E, Klarlund M, Court-Payen M, Thomsem HS, Østergaard M. Ultrasonography of the metatarsophalangeal joints in rheumatoid arthritis: Comparison with magnetic resonance imaging, conventional radiography, and clinical examination.Arthritis Rheum. 2004;50:2103-12.
22. Brown AK, O’Connor PJ, Roberts TE, Wakeield RJ, Karim Z, Emery P. Recommendations for musculoskeletal
23. D’Agostino MA, Ayral X, Baron G, Ravaud P, Breban M, Dougados M. Impact of ultrasound imaging on local corticosteroid injections of symptomatic ankle, hind-, and mid-foot in chronic inlammatory diseases. Arthritis Rheum. 2005;53:284-92.
24. Bresnihan B, Kane D. Sonography and subclinical synovitis. Ann Rheum Dis. 2004;63:333-4.
25. Brown AK, Conaghan PG, Karim MA. An explanation for the apparent dissociation between clinical remission and continued structural deterioration in rheumatoid arthritis. Arthritis Rheum. 2008;58:2958-67.
26. Taylor PC, Steuer A, Gruber J, Cosgrove DO, Blomley MJ, Marsters PA et al. Comparison of ultrasonographic assessment of synovitis and joint vascularity with
radiographic evaluation in a randomized, placebo-controlled study of inliximab therapy in early rheumatoid arthritis. Arthritis Rheum. 2004;50:1107-16.
27. Wakeield RJ, Gibbonw W, Conaghan PG et al.The value of sonography in the detection of bone erosions in patients with rheumatoid arthritis: a comparison with conventional radiography. Arthritis Rheum. 2000;43:2762-70.
28. Cyteval C. Doppler ultrasonography and dynamic magnetic resonance imaging for assessment of synovitis in the hand and wrist of patients with rheumatoid arthritis. Semin Musculoskelet Radiol. 2009;13:66-73.
29. Navalho M, Resende C, Rodrigues AM, Pereira da Silva JA, Fonseca JE, Campos J, Canhão H. Bilateral evaluation of the hand and wrist in untreated early inlammatory arthritis: a comparative study of ultrasonography and magnetic resonance imaging. J Rheumatol. 2013;40:1282-1292.
30. Mendonça JA. Yazbek MA, Laurindo IM, Bertolo MB. Wrist ultrasound analysis of patients with early rheumatoid arthritis. 2011;44:11-5.
31. Scheel AK, Hermann KG, Ohrndorf S, Werner C, Schimer C, Detert J et al. Prospective 7 year long term follow-up imaging study comparing radiography, ultrasonography and magnetic resonance imaging in rheumatoid arthritis inger joints. Ann. Rheum.Dis. 2006;65:595-600.
32. Backhaus M, Kamradt T, Sandrock D, Loreck D, Fritz J, Wolf KJ et al. Arthritis of the inger joints: A comprehensive approach comparing conventional radiography, scintigraphy, ultrasound, and contrast-enhanced magnetic resonance imaging. Arthritis Rheum. 1999;42:1232-45
33. Aletaha D, Nell VPK, Stamm T, Uffmann M, Plugbeil S, Machold K et al. Acute phase reactants add little to composite disease activity indices for rheumatoid athritis: validation of a clinical activity score. Arthritis Res Ther. 2005;7:R796-806. 34. Filippucci E, Luz KR, Di Geso L, Salafi F, Tardella M, Carotti M et al. Interobserver reliability of ultrasonography in the assessment of cartilage damage in rheumatoid arthritis. Ann Rheum Dis. 2010;69:1845-8.
35. Gutierrez M, Filippucci E, Ruta S, Salafi F, Blasetti P, Geso LD, Grassi W. Inter-observer reliability of high-resolution ultrasonography in the assessment of bone erosions in patients with rheumatoid arthritis: experience of an intensive dedicated training programme. Rheumatology. 2011;50:373-80.