rev bras reumatol.2015;55(2):95–102
w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Pregnancy
outcomes
in
dermatomyositis
and
polymyositis
patients
Larissa
Sayuri
Missumi
a,
Fernando
Henrique
Carlos
de
Souza
a,
Joelma
Queiroz
Andrade
a,
Samuel
Katsuyuki
Shinjo
b,∗aDivisionofRheumatology,HospitaldasClínicasdaFaculdadedeMedicinadaUniversidadedeSãoPaulo,SãoPaulo,SP,Brazil
bDivisionofRheumatology,FaculdadedeMedicinadaUniversidadedeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received17May2014 Accepted6October2014 Availableonline6January2015
Keywords: Dermatomyositis Inflammatorymyopathies Obstetricintercurrences Polymyositis
Pregnancy
a
b
s
t
r
a
c
t
Background:Currently, thereare few studiesthatdescribepregnancy in
dermatomyosi-tis/polymyositispatients,andtheyarelargelylimitedtocasereportsorstudieswithfew samples.
Objectives: Therefore,wedescribethepregnancyinalargesampleofpatientswith
dermato-myositis/polymyositisandtoanalyzetheoutcomesinthosewhobecamepregnantduring orafterdiseaseonset.
Methods:The presentsingle-center study analyzed 98 female patients with idiopathic
inflammatorymyopathies(60dermatomyositisand38polymyositispatients).Theywere interviewedtoobtainobstetricantecedentanddemographicdatafromJune2011toJune 2012.
Results:Seventy-eight(79.6%)ofthe98patientshadobstetrichistories.Sixpolymyositisand
9dermatomyositispatientsbecamepregnantafterdiseaseonset.Thepregnancyoutcomes inthesecasesweregood,exceptinthefollowingcases:1diseasereactivation,1intrauterine growthretardation,1diabetesmellitus,1hypertension,1hypothyroidism,and2fetallosses (samepatient).Moreover,2patientsdevelopeddermatomyositisduringpregnancyand4(2 polymyositisand2dermatomyositis)duringthepostpartumperiodwithgoodcontrolafter glucocorticoidandimmunosuppressanttherapy.
Conclusions: Theadverseobstetriceventswererelatedtoclinicalintercurrencesandthe
pregnancydoesnotseemtocarryaworseprognosisspecificallyindisease(forexample: diseaserelapsing).Moreover,dermatomyositisorpolymyositisonsetduringpregnancyor thepostpartumperiodhadgoodoutcomeafterdrugtherapy.
©2014ElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](S.K.Shinjo).
http://dx.doi.org/10.1016/j.rbre.2014.11.001
96
rev bras reumatol.2015;55(2):95–102Desfechos
da
gestac¸ão
em
pacientes
com
dermatomiosite
e
polimiosite
Palavras-chave: Dermatomiosite Miopatiasinflamatórias Intercorrênciasobstétricas Polimiosite
Gestac¸ão
r
e
s
u
m
o
Introduc¸ão: Há poucos estudos que descrevem a gravidez em pacientes com
der-matomiosite/polimiosite.São,emgrandeparte,limitadosarelatos decasosouestudos comamostraspequenas.
Objetivos: Analisar a gestac¸ão em uma grande amostra de pacientes com
der-matomiosite/polimiositeeosdesfechosnaquelasqueengravidaramduranteoudepoisdo iníciodadoenc¸a.
Métodos: Foramanalisados98pacientesdosexofemininocommiopatiasinflamatórias
idiopáticas(60comdermatomiositee38compolimiosite).Elasforamentrevistadasentre junhode2011ejunhode2012paracoletarseusantecedentesobstétricosedados demográ-ficos.
Resultados: Tinhamantecedentesobstétricos78(79,6%)das98pacientes.Seispacientes
compolimiositeenovecomdermatomiositeengravidaramapósoiníciodadoenc¸a.O des-fechodagravideznessaspacientesfoibom,excetonosseguintescasos:umdereativac¸ãoda doenc¸a,umderetardodocrescimentofetal,umdediabetesmellitus,umdehipertensão arte-rial,umdehipotireoidismoedoisdeaborto(mesmapaciente).Alémdisso,duaspacientes desenvolveramdermatomiositeduranteagravidezequatro(duaspolimiositeeduas der-matomiosite)duranteoperíodopós-parto,combomcontroleaseguircomglucocorticoides eterapiaimunossupressora.
Conclusões: Oseventosobstétricosadversosestiveramrelacionadoscomasintercorrências
clínicaseagravideznãoparecelevarespecificamenteaumpiorprognósticonadoenc¸a(por exemplo:recidiva).Alémdisso,adermatomiositeoupolimiositedeinícioduranteagestac¸ão ounoperíodopós-partoapresentouboaevoluc¸ãodepoisdotratamentofarmacológico.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Dermatomyositis (DM) and polymyositis (PM) are systemic inflammatoryautoimmunemyopathiescharacterizedbythe subacuteonsetofsymmetricweaknessintheproximal mus-culature. Furthermore, cutaneous manifestations, such as heliotrope rash and Gottron’s papules, are present in DM. Additionally,extra-muscularmanifestations,suchas articu-lar,cardiorespiratoryandgastrointestinalabnormalitiesmay befoundinbothdiseases.1,2TheannualincidenceofDM/PM is0.5–8.4casespermillionhabitants,affectingtwiceasmany womenasmen,withnoracialpredilection.TheDMaffects bothchildrenandadults,whereasPMisseemaftertheforth decadeoflifeandveryrarelyinchildhood.3–5
Variousstudiesconductedworldwidehaveassessed preg-nancy in systemic rheumatic diseases. In systemic lupus erythematosus,forexample,thematernalmortalityriskis20 timeshigherthanthatofahealthypregnantfemale.These womenalsohaveahigh riskofcesarean delivery,preterm labor,preeclampsia,thromboembolicevents,andinfectious andhematologicalcomplications.6Forrheumatoidarthritis, variousstudieshaveshownimprovementofsymptomsduring pregnancy.7However,especiallyinactiverheumatoid arthri-tis, there is a slight increase in the rate of children with decreasedbirthweightandgestationalage.8
Currently,therearefewstudiesthatdescribepregnancyin DM/PMpatients,andtheyarelargelylimitedtocasereportsor studieswithsmallsamples.9–27Thus,littleisknownaboutthe effectsofpregnancyonDM/PM,whetherthesepatientsfind
ithardertoconceiveorifpregnancyoutcomesareadversely affectedbymyositis.Herein,weevaluatepregnancyinalarge sampleofDM/PMpatientsanddescribetheoutcomesinthose whobecamepregnantduringorafterdiseaseonset.
Materials
and
methods
Thepresentretrospectivecohortstudywasperformedata sin-glecenterandincluded98consecutiveDM/PMpatients(≥18 yearsold)fromJune2011toJune2012.Allpatientsmetatleast fourofthefiveBohanandPetercriteriaitems,28andtheywere regularlyfollowingatourmyopathyunitofourtertiarycare centerfrom1993to2012.Patientswithotherassociated sys-temicautoimmunediseasewerenotincludedinthepresent study.
Thestudywasapprovedbythelocalethicscommittee,and allofthestudyparticipantssignedaninformedconsentform. Alloftheparticipantsunderwentastandardizedinterview, andtheirmedicalchartswereextensivelyreviewed.The fol-lowing datawere collected:basicdemographicdata,ageof diseaseonset,treatment,numberofpregnanciesbeforeand afterdiseaseonset,activityofthediseaseduringpregnancy andpregnancyoutcomes.
Therapy
rev bras reumatol.2015;55(2):95–102
97
disease was severe (progression of dyspnea, dysphagia, significant loss of muscle strength), pulse therapy with methylprednisolone(1g/dayforthreeconsecutivedays)was performed.Thefollowingcorticosteroidsparingagentswere used as monotherapy or in combination: methotrexate (20–25mg/week),azathioprine(2–3mg/kg/day)orcyclosporine (2–4mg/kg/day), chroloquine diphosphate (3–4mg/kg/day), and cyclophosphamide (0.5–1.0g/m2 of body surface). The cyclophosphamidewas usedinthe presenceofprogressive dyspnea associated with pulmonary parenchymal change confirmedoncomputedtomography(“ground-glass”opacity ofhoneycombing).
Statisticalanalysis
Thedataareexpressedasthemeanandstandarddeviation (SD)forcontinuousvariablesorasfrequenciesand percent-agesforcategoricalvariables.
Results
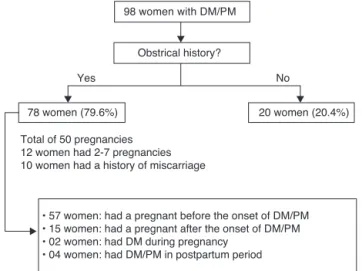
Obstetricalhistorywasnotedin78(79.6%)outof98women with DM/PM (Fig. 1). Of these, 57 women, who were not describedinthisstudy,hadapregnancybeforetheonsetof DM/PM.
Of the remaining patients, 15 became pregnant after disease diagnosis; whereas 2 women developed the dis-easeduringpregnancyand4postpartummothersdeveloped DM/PM.Intotal,therewere50pregnancies,and10womenhad ahistoryofmiscarriage.Twelvepatientshad2–7pregnancies, and1–4pregnanciesoccurredbeforetheDM/PMdiagnosis.
Theaverageageofpregnantwomenwithestablished dis-easewas 30.6±3.7years (range22–37years), witha mean durationofdiseaseof13.4±4.3years.Therewere9casesof DMand6PMinatotalof21pregnancies.Amongtheclinical complications,therewere2fetallosses,1caseof intrauter-inegrowthretardation,1caseofdecompensatedgestational diabetesmellitus,1caseofsystemicarterialhypertension,1 caseofdecompensatedhypothyroidismand1caseofvenous thrombophilia.Only1casehadworseningdiseasestatus,for
• 57 women: had a pregnant before the onset of DM/PM • 15 women: had a pregnant after the onset of DM/PM • 02 women: had DM during pregnancy
• 04 women: had DM/PM in postpartum period 98 women with DM/PM
Obstrical history?
Yes No
78 women (79.6%) 20 women (20.4%)
Total of 50 pregnancies 12 women had 2-7 pregnancies 10 women had a history of miscarriage
Fig.1–Descriptionofdermatomyositisandpolymyositis patients.
which corticosteroidswere reintroduced,and good disease controlwasachieved.Fourpatientsreceivedcorticosteroids throughoutpregnancywithgoodclinicalandlaboratory dis-easecontrol(Table1).
In 2cases,the disease(DM) developedduringthe preg-nancy (Table 2). Particularly in the patient n◦ 16, the
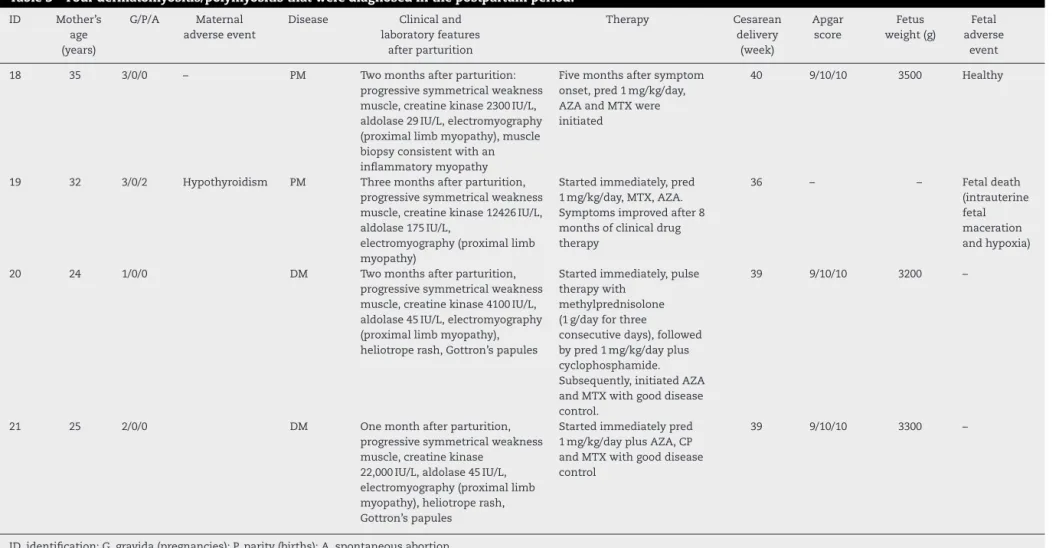
corticosteroidwasstartedtwomonthslater,sincethe cuta-neouslesionswereinitiallyattributedtoallergicreactionand theprogressivemuscleweaknesswasnotsoclinicallyevident. Infourcases,DM/PMwere diagnosedinthepostpartum period(Table3).
Discussion
Herein,weassessedpregnancyinalargesampleofDM/PM patients and theoutcomes inthose who became pregnant duringorafterdiseaseonset.
Therearevariousstudiesthatanalyzepregnancyin sys-temic rheumatic diseases, but not in DM/PM. Hence, the presentstudycontributedtothefewavailablestudiesinthe literature.Moreover,theadvantageofthisstudywasthe anal-ysis of obstetric antecedents in a large sample ofDM/PM patients.
There are twotypes ofpregnancy-related myositis: one presenting during pregnancy and the other, less common, developingpostpartum.Inthepresentstudy,wedidnot con-sidertheoutcomesofpregnanciesthatoccurredpriortothe diagnosisofDM/PM.
Theevolutionandbehaviorofpregnancyininflammatory myopathiesthatareeitheractiveorinremissionisstill con-troversialintheliterature.Thereis,forexample,adescription ofpregnancyinpatientswithfrankDM/PMactivity.However, withtheintroductionofdrugtherapy,thediseaseiscontrolled without complications after delivery.9–13 England et al.16 reported acasewithoutneonatalcomplications but result-inginmaternaldeathduetoacuteexacerbationofdiabetes. Silva et al.29 reported eight cases of disease development postpartum. Gutierrezetal.30 observed threepatientswith previouslyinactivediseasethathadanexacerbationduring pregnancy.Otherstudieshavereportedillnessafterchildbirth orabortion,suggestingthatthefetusactsasaforeignbody, perpetuatingdisease activityonlyduringpregnancy.18–21 In thisstudy,allpatientshadstabledisease,and4patientsused corticosteroidstocontrolthemyopathyduringpregnancy.In contrast, only1 case demonstrated clinical and laboratory reactivationofthediseaserequiringcorticosteroids,butwith goodcontrolofdiseaseactivity.Fromtheobstetricstandpoint, withtheexceptionof6cases,successfulpregnancieswithout feto-maternalcomplicationsweretheruleintheperipartum period.
There are few studies involving a large enough sam-ple to allow generalizations about pregnancy in DM/PM patients.9,29–32 Based on these studies, the main obstetric complicationsdescribedareintrauterinegrowthretardation, prematurityandfetaldeath.
98
r
e
v
b
r
a
s
r
e
u
m
a
t
o
l
.
2
0
1
5;
5
5(2)
:95–102
Table1–Generalcharacteristicsofpregnancyoutcomesindermatomyositisandpolymyositispatients.
ID Mother’s
age (years)
G/P/A Maternal
adverseevent
Disease Disease
durationprior topregnancy
(years)
Disease statusat pregnancy
Previous therapy
Current therapy(at pregnancy)
Gestational age(week)
Fetusweight (g)
Fetal adverse
event
1 33 6/0/5 Venous
throm-bophilia
DM 12 Stable MTX25mg/week,
AZA3mg/kg/day,CD 4mg/kg/day
CD 4mg/kg/day
32w2d 2090 Healthy
1 35 7/1/5 Hypothyroidism DM 14 Stable MTX25mg/week,
AZA3mg/kg/day,CD 4mg/kg/day
CD 4mg/kg/day Pred 10mg/day
37w3d 2410 Healthy
2 30 2/1/0 Healthy DM 6 Stable AZA3mg/kg/day,CD
4mg/kg/day
– Healthy
2 35 3/2/0 Healthy DM 11 Stable AZA3mg/kg/day,CD
4mg/kg/day
– Healthy
3 28 1/0/0 Healthy DM 9 Stable MTX25mg/week,
AZA3mg/kg/day,CD 4mg/kg/day
CD 4mg/kg/day
Healthy
4 24 3/2/0 Healthy DM 6 Stable AZA3mg/kg/day – Healthy
5 22 1/0/0 Healthy DM 18 Stable AZA3mg/kg/day,CD
4mg/kg/day
CD 4mg/kg/day
3410 Healthy
6 33 1/0/0 Healthy PM 12 Stable AZA3mg/kg/day Pred
20mg/day
3180 Healthy
7 29 1/0/0 Healthy DM 5 Stable CYC0.5–1.0g/bs2 – 3420 Healthy
8 34 4/1/2 Healthy PM 17 Stable AZA3mg/kg/day Pred
30mg/day
39w1d 3090 Healthy
9 28 2/1/0 Healthy PM 13 Stable MTX25mg/week,
CD4mg/kg/day
– Healthy
9 30 3/2/0 Healthy PM 15 Stable MTX25mg/week,
CD4mg/kg/day
– Healthy
9 37 4/3/0 Diabetes
mellitus
PM 17 Stable MTX25mg/week,
CD4mg/kg/day
– 3390 Healthy
10 31 1/0/0 Healthy DM 13 Stable MTX25mg/week – Fetalloss
10 32 2/0/1 Healthy DM 14 Worse MTX25mg/week Pred
1mg/kg/day
Fetalloss
10 34 3/0/2 Healthy DM 16 Stable MTX25mg/week – 40w IUGR
11 33 2/1/0 Healthy PM 21 Stable MTX25mg/week – 3600 Healthy
12 30 1/0/0 Healthy PM 19 Stable MTX25mg/week,
AZA3mg/kg/day
Pred 20mg/day
Healthy
13 29 3/2/0 Healthy PM 13 Stable MTX20mg/week – 3200 Healthy
14 30 3/2/0 Healthy DM 17 Stable AZA3mg/kg/day – Healthy
15 26 2/1/0 Hypertension,
healthy
DM 14 Stable AZA3mg/kg/day – Healthy
r
e
v
b
r
a
s
r
e
u
m
a
t
o
l
.
2
0
1
5;
5
5(2)
:95–102
99
Table2–Twodermatomyositisonsetatthepregnancy.
ID Mother’s
age(years)
G/P/A Maternal
adverseevent
Disease Clinicaland
laboratory features
Therapy Gestational
age(week)
Cesarean delivery(w)
Apgar score
Fetus weight(g)
Fetal adverse
event
16 29 1/0/0 Diabetes
Hypertension
DM Progressivesymmetrical
weaknessmuscle, heliotroperash,Gottron’s papules,creatinekinase 494IU/L,aldolase173IU/L, electromyography (proximallimbmyopathy)
Aftertwomonths,Pred 1mg/kg/daywerestarted withgoodresults.After parturition,AZAand subsequently,MTXandCP wereassociatedwithgood diseasecontrol
24 37 8/9/9 3210 Healthy
17 26 1/0/0 Hypothyroidism DM Dysphagia,progressive
symmetricalweakness muscle,heliotroperash, Gottron’spapules,creatine kinase22858IU/L,aldolase 159IU/L,electromyography (proximallimbmyopathy)
Pred1mg/kg/day.After parturition,MTXwas associatedwithgood diseasecontrol
25 38 9/10/10 3000 Healthy
100
r
e
v
b
r
a
s
r
e
u
m
a
t
o
l
.
2
0
1
5;
5
5(2)
:95–102
Table3–Fourdermatomyositis/polymyositisthatwerediagnosedinthepostpartumperiod.
ID Mother’s
age (years)
G/P/A Maternal
adverseevent
Disease Clinicaland
laboratoryfeatures afterparturition
Therapy Cesarean
delivery (week)
Apgar score
Fetus weight(g)
Fetal adverse
event
18 35 3/0/0 – PM Twomonthsafterparturition:
progressivesymmetricalweakness muscle,creatinekinase2300IU/L, aldolase29IU/L,electromyography (proximallimbmyopathy),muscle biopsyconsistentwithan inflammatorymyopathy
Fivemonthsaftersymptom onset,pred1mg/kg/day,
AZAandMTXwere
initiated
40 9/10/10 3500 Healthy
19 32 3/0/2 Hypothyroidism PM Threemonthsafterparturition,
progressivesymmetricalweakness muscle,creatinekinase12426IU/L, aldolase175IU/L,
electromyography(proximallimb myopathy)
Startedimmediately,pred 1mg/kg/day,MTX,AZA. Symptomsimprovedafter8 monthsofclinicaldrug therapy
36 – – Fetaldeath
(intrauterine fetal maceration andhypoxia)
20 24 1/0/0 DM Twomonthsafterparturition,
progressivesymmetricalweakness muscle,creatinekinase4100IU/L, aldolase45IU/L,electromyography (proximallimbmyopathy), heliotroperash,Gottron’spapules
Startedimmediately,pulse therapywith
methylprednisolone (1g/dayforthree
consecutivedays),followed bypred1mg/kg/dayplus cyclophosphamide. Subsequently,initiatedAZA andMTXwithgooddisease control.
39 9/10/10 3200 –
21 25 2/0/0 DM Onemonthafterparturition,
progressivesymmetricalweakness muscle,creatinekinase
22,000IU/L,aldolase45IU/L, electromyography(proximallimb myopathy),heliotroperash, Gottron’spapules
Startedimmediatelypred 1mg/kg/dayplusAZA,CP andMTXwithgooddisease control
39 9/10/10 3300 –
ID,identification;G,gravida(pregnancies);P,parity(births);A,spontaneousabortion.
rev bras reumatol.2015;55(2):95–102
101
case, a patient with DM, there were 2fetal losses; during hersecondpregnancy,sheexperienceddiseasereactivation as previously mentioned. In the third pregnancy, she had intrauterinegrowth retardation,but withstabledisease.In general,therewere nosignificant pregnancy complications inoursample,probablybecausethemajorityofpatientshad stabledisease.
Concerningfertility,ithasbeensuggestedthattheratesare significantlydifferentbeforeandaftertheonsetofDM/PM.9 However,thelateageofonsetandtheuseofcontraceptives precludeanaccurateevaluationoftheinfluenceofthedisease onfertility.Differentfollow-upperiods,lackofinformation ontheuseofcontraceptionandascarcityofcasesalsomake thisanalysisdifficult.Inthepresentstudy,6patientshadnew pregnancyaftertheonsetofDM/PM.Moreover,oneofthem hadtwopregnanciesafterdiseaseonset.
Inthepresentstudy,infourcases,DM/PMonsetoccurred duringthepostpartumperiod.Inallofthesecases,therewas good controlofthe disease after theintroduction of corti-costeroidsandimmunosuppressivedrugs.Kofteridisetal.14 describedanacuteonsetofdiabetesinpregnancythatleadto rhabdomyolysisandfetalloss.Autoimmunediseasemaybe inducedasaresultofmaternalhormonalchanges,alteration ofimmunefunctionduringpregnancyorasaconsequenceof maternalexposuretofetalantigens,33whichmayexplainthe onsetofDM/PMinthepostpartumperiod.
Therearesomelimitationstothepresentstudy.Ourstudy islimitedbyits retrospectivecohortstudy design. Further-more, this work includes the characteristics of the study population,whichwerefromatertiarycarecenterandmost likelyrepresentamoreseverediseasespectrum;therefore,the frequencyofpregnancyanditsrepercussionsinDM/PMmight nothavebeenwell-estimated.
Conclusions
Theadverseobstetriceventswererelatedtoclinical intercur-rences and thepregnancy does notseem tocarry aworse prognosisspecificallyindisease(forexample:disease relaps-ing).Moreover,dermatomyositisorpolymyositisonsetduring pregnancyorthepostpartumperiodhadgoodoutcomeafter drugtherapy.
Conflict
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
SKSreceivedgrantsupportfromtheFedericoFoundation;LSM receivedgrantsupporterfromFAPESP(#2011/15517-3).
r
e
f
e
r
e
n
c
e
s
1. CallenJP.Dermatomyositis.In:CallenJP,editor.
Dermatologicalsignsofinternaldisease.2nded.Saunders; 1995.
2.FathiM,LundbergIE.Interstitiallungdiseaseinpolymyositis anddermatomyositis.CurrOpinRheumatol.2005;17: 701–6.
3.DrakeLA,DinehartSM,FarmerER,GoltzRW,GrahamGF, HordinskyMK,etal.Guidelinesofcarefordermatomyositis. AmAcadDermatol.1996;34:824–9.
4.FeldmanBM,RiderLG,ReedAM,PachamnLM.Juvenile dermatomyositisandotheridiopathicinflammatory myopathiesofchildhood.Lancet.2008;281:2201–2.
5.GreenbergSA.Inflammatorymyopathies:evaluationand management.SeminNeurol.2008;28:241–9.
6.BaerAN,WitterFR,PetriM.Lupusandpregnancy.Obstetrical andgynecologicalsurvey.ObstetGynecolSurv.
2011;66:639–53.
7.HazesJMW,CouliePG,GeenenV,VermeireS,CarbonnelF, LouisE,etal.Rheumatoidarthritisandpregnancy:evolution ofdiseaseactivityandpathophysiologicalconsiderationsfor druguse.Rheumatology.2011;50:1955–68.
8.ChakravartyEF.Rheumatoidarthritisandpregnancy:beyond smallerandpretermbabies.ArthritisReum.2011;63:1469–71.
9.IshiiN,OnoH,KawaguchiT,NakajimaH.Dermatomyositis andpregnancy.Casereportandreviewoftheliterature. Dermatologica.1991;183:146–9.
10.KingCR,ChowS.Dermatomyositisandpregnancy.Obstet Gynecol.1985;66:589–92.
11.OhnoT,ImaiA,TamayaT.Successfuloutcomesofpregnancy complicatedwithdermatomyositis.Casereports.Gynecol ObstetInvestig.1992;33:187–9.
12.PinheiroGdaR,GoldenbergJ,AtraE,PereiraRB,CamanoL, SchmidtB.Juveniledermatomyositisandpregnancy:report andliteraturereview.JRheumatol.1992;19:1798–801.
13.HouckW,MelnykC,GastMJ.Polymyositisinpregnancy.A casereportandliteraturereview.JReprodMed.
1987;32:208–10.
14.KofteridisDP,MalliotakisPI,SotsiouF,VardakisNK,Vamvakas LN,EmmanouelDS.Acuteonsetofdermatomyositis
presentinginpregnancywithrhabdomyolysisandfetalloss. ScandJRheumatol.1999;28:192–4.
15.OrosJ,GilB,RiscoCortesR,TorresV,CerveraAguilarR,Ayala AR.Dermatomyositisandeclampsia.Analysisofacaseand reviewoftheliterature.GinecolObstetMex.1994;62:103–6.
16.EnglandMJ,PerlmannT,VeriavaY.Dermatomyositisin pregnancy.Acasereport.JReprodMed.1986;31:633–6.
17.KanohH,IzumiT,SeishimaM,NojiriM,IchikiY,KitajimaY.A caseofdermatomyositisthatdevelopedafterdelivery:the involvementofpregnancyintheinductionof
dermatomyositis.BrJDermatol.1999;141:897–900.
18.BauerKA,SieglerM,LindheimerMA.Polymyositis complicatingpregnancy.ArchInternMed.1979;139:449.
19.HarrisA,WebleyM,UsherwoodM,BurgeS.Dermatomyositis presentinginpregnancy.BrJDermatol.1995;133:783–5.
20.Ditzian-KadanoffR,ReinhardJD,ThomasC,SegalAS. Polymyositiswithmyoglobinuriainpregnancy:areportand reviewoftheliterature.JRheumatol.1988;15:513–4.
21.TojyoK,SekijimaY,HattoriT,TsuyuzakiJ,NakamuraA,Kita N,etal.Apatientwhodevelopeddermatomyositisduringthe 1sttrimesterofgestationandimprovedafterabortion. RinshoShinkeigaku.2001;41:635–8.
22.LeThiHuongD,WechslerB,CombesR,SeebacherJ,Cruveiller J,CailleB,etal.Twinpregnancyinpolymyositis.AnnMed Intern(Paris).1986;139:286–7.
23.KatzAL.Anothercaseofpolymyositisinpregnancy.Arch InternMed.1980;140:1123.
24.GattiCM,DeVitoEL,GoldembergDB.Polymyositisand pregnancy.Medicina(BAires).1984;44:402–6.
102
rev bras reumatol.2015;55(2):95–10226.EmyP,LenormandV,MaitreF,RobilltP,TescherM,BentataJ, etal.Polymyositis,dermatomyositisandpregnancy:high-risk pregnancy.Afurthercasereportandreviewoftheliterature.J GynecolObstetBiolReprod(Paris).1986;15:785–90.
27.PapapetropoulosT,KanellakopoulouN,TsibriE,PaschalisC. Polymyositisandpregnancy:reportofacasewiththree pregnancies.JNeurolNeurosurgPsychiatry.1998;64:406.
28.BohanA,PeterJB.Polymyositisanddermatomyositis.PtI.N EnglJMed.1975;292:344–407.
29.SilvaCA,SultanSM,IsenbergDA.Pregnancyoutcomein adult-onsetidiopathicinflammatorymyopathy. Rheumatology.2003;42:1168–72.
30.GutiérrezG,DagninoR,MintzG.
Polymyositis/dermatomyositisandpregnancy.Arthritis Rheum.1984;27:291–4.
31.Juárez-AzpilcuetaA,Pol-KipesG,Olivo-ArroyoG,Ortiz-Pavón A,Coronel-CruzF.Dermatomyositisandpregnancy.GacMed Mex.2003;139:509–11.
32.GlickmanFS.Dermatomyositisassociatedwithpregnancy.U SArmedForcesMedJ.1958;9:417–25.