w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Prevalence
of
sexual
dysfunction
among
female
patients
followed
in
a
Brasília
Cohort
of
early
rheumatoid
arthritis
Thaís
Ferreira
Costa
a,∗,
Carolina
Rocha
Silva
a,
Luciana
Feitosa
Muniz
a,
Licia
Maria
Henrique
da
Mota
baServiceofRheumatology,HospitalUniversitáriodeBrasilia,UniversidadedeBrasília,Brasilia,DF,Brazil bMedicineSchool,UniversidadedeBrasília,Brasilia,DF,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received20February2013
Accepted6October2014
Availableonline7January2015
Keywords:
Sexualdysfunction
Sexuality
Rheumatoidarthritis
Qualityoflife
a
b
s
t
r
a
c
t
Objective:Todeterminetheprevalenceofsexualdysfunctioninwomendiagnosedwithearly
rheumatoidarthritis(RA)(lessthanoneyearofsymptomsatthetimeofdiagnosis),aswell
astoevaluatethepossibleassociationbetweensexualdysfunctionwithARactivityand
functionaldisability.
Methods:Cross-sectionalstudyassessingwomendiagnosedwithearlyRA,accompanied
perprotocolintheBrasiliaCohort,HospitalUniversitáriodeBrasília.Demographics,disease
activityindex(DiseaseActivityScore28–DAS28)andfunctionaldisabilityquestionnaire
(HealthAssessmentQuestionnaire–HAQ),wereobtainedbydirectinterviews.TheFemale
SexualFunctionIndex(FSFI)wasusedquestionnairewhichcontains19itemsthatassess
sixdomains:sexualdesire,sexualarousal,vaginallubrication,orgasm,sexualsatisfaction
andpain.
Results:68 patientsstudied,ofwhom54(79.4%)reportedsexualactivityinthelastfour
weeks.Theparticipantswere49.7±13.7(mean±SD)yearsoldandthemajoritywere
mar-ried(61.4%).ThemeanDAS28was3.6±1.5andthemeanHAQwas0.7.Theprevalenceof
sexualdysfunction(FSFI≤26)was79.6%.Therewasnoassociationofdiseaseactivityor
offunctionaldisabilitywiththeoccurrenceofsexualdysfunctioninthefemalepatients
evaluated.
Conclusion: Theprevalenceofsexualdysfunctionfoundinthisstudywashigherthanthat
reportedintheliteratureinhealthywomen.Aknowledgeoftheextentoftheproblemis
neededtoprovideadequatetherapeuticoptionsforthesepatients.
©2014ElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](T.F.Costa).
http://dx.doi.org/10.1016/j.rbre.2014.10.006
Prevalência
de
disfunc¸ão
sexual
entre
pacientes
acompanhadas
na
coorte
Brasília
de
artrite
reumatoide
inicial
Palavras-chave:
Disfunc¸ãosexual
Sexualidade
Artritereumatoide
Qualidadedevida
r
e
s
u
m
o
Objetivo: Determinaraprevalênciadedisfunc¸ãosexualemmulherescomdiagnósticode
artritereumatoide(AR)inicial(menosdeumanodesintomasaodiagnóstico),bemcomo
avaliarapossívelassociac¸ãoentredisfunc¸ãosexualcomatividadedaAReincapacidade
funcional.
Métodos: Estudotransversal,queavalioumulherescomdiagnósticodeARinicial,
acom-panhadas deforma protocolarnacoorte Brasília,noHospital UniversitáriodeBrasília.
Dadosdemográficos,índicedeatividadedadoenc¸a(DiseaseActivityScore28–DAS28)
edadosdoquestionáriodeincapacidadefuncional(HealthAssessmentQuestionnaire–
HAQ)foramobtidosporentrevistasdiretas.Usou-seoíndicedefunc¸ãosexualfeminina
(FemaleSexualFunctionIndex–FSFI),questionárioquecontém19itensqueavaliamseis
domínios:desejosexual,excitac¸ãosexual,lubrificac¸ãovaginal,orgasmo,satisfac¸ãosexual
edor.
Resultados: Foramestudadas68pacientes,dasquais54(79,4%)relataramatividade
sex-ualnasúltimasquatrosemanas.Amédiadeidadefoide49,7±13,7anoseamaioriaera
casada(61,4%).ODAS-28médiofoide3,6±1,5eamédiadoHAQfoide0,7.A
prevalên-ciade disfunc¸ãosexual(FSFI≤26)foi de79,6%. Nãohouveassociac¸ãode atividadede
doenc¸anemdeincapacidadefuncionalcomaocorrênciadedisfunc¸ãosexualnaspacientes
avaliadas.
Conclusão: A prevalência de disfunc¸ão sexual encontrada neste estudo foi superior
à relatado na literatura em mulheres saudáveis. Há necessidade de conhecimento
da extensão do problema para oferecer possibilidades terapêuticas adequadas aos
pacientes.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Rheumatoidarthritis(RA)isasystemicchronicand
progres-sivediseasethatpreferentiallyaffectsthesynovialmembrane
ofjointsand canlead toboneand cartilage destruction.1,2
Thediseaseleadstovariousdegreesofdisabilityandhasa
profoundimpactonthesocial,economicandpsychological
aspectsofthepatient’slife.3
Sexualfunction(FS) isamajorcomponent ofquality of
life,withhigheramplitudethansexualintercourseitself.4,5
Sexual expressionis acrucial partof the individual’sown
identity,andthereforeimportantinallstagesofhealthand
disease.6Afullsexualfunctioningconsistsinthetransition
betweenphases, from excitement torelaxation,with
plea-sureandsatisfaction.7Sexualdysfunction(SD)isdefinedas
the inability to participatein the sexual actwith
satisfac-tion,compromisingthedesireand/orarousaland/ororgasm.4
Sexualityinfluencesbehavioranddefinesgenderroles;and
bothinthephysicalandpsychologicalsense,becomespart
of the lifestyle of the individual ofall ages.3 SD not only
compromisessexualsatisfaction,but alsooverall life
satis-faction,determiningalowerqualityoflife,lowself-esteem,
depression,anxietyandprejudiceininterpersonaland
part-nerrelationship.4ThemainriskfactorsforSDhaveorganic,
psychosocialandsociodemographicorigin,withemphasison
age,familyincomeandeducation.4,8 Someauthorssuggest
thatfemalesexualdysfunctionsometimesreachesmorethan
40%ofwomen.9
Competence, motivation and sexual expression are
decreasedinpatientswithRA.10Mostofthesexualproblems
experiencedbythesepatientsarerelatedtodiseaseactivity,
pain, lossofjointmotion,functional disability,orfatigue.11
Otherfactorsincludedepression,anxiety,lossofself-esteem
anddifficultyindiscussingthedisease.11Thepercentageof
patientswitharthritiswhoexperiencesexualproblemsvaries
acrossstudies,from31to76%.4,7,10–12
Thetwo mainfields ofsexual problemsexperiencedby
patientswithRAare:difficultyinperformingthesexualact
(sexualdisability)anddecreasedsexdrive,reflectedbothin
sexualdesireandinadecreasedsexualsatisfaction.Sexual
incapacityismanifestedbyproblemssuchasjointpainand
fatigueduringintercourse,presentedby50–61%ofpatients
withRA. Difficultyinassumingcertainpositionswhen hip
orkneemovementsarelimitedanddyspareuniadueto
vagi-naldrynessinsecondarySjögren’ssyndromeare observed.
Decreasedsexdriveismanifested byadecreaseddesirein
50–60%ofpatientswithRA,andbyalowfrequencyofsexual
intercoursein73%ofpatients.3,7,13
AlthoughSF’scommitmentisamajorproblemforpatients
diagnosedwithRA,adequateinformationonthissubjectare
scarce.3 Sexuality is rarelyaddressed in questionnaireson
Itisvery importantthatrheumatologists and other health
professionals acknowledge the impact that RA promotes
insexuality,sincethisknowledgefacilitatesthediscussion
betweendoctorandpatient,whenaddressingtheinfluence
ofthediseaseinseveraldomainsofpatients’qualityoflife.
Additionally, it allows anoptimization ofthe treatment of
RA,hereencompassingtheattentiontothepatient’ssexual
difficulties.11
NoBraziliandataexiston theprevalenceofsexual
dys-functioninwomenwithearlyRA.Thisstudyaimstodescribe
theprevalenceofsexualdysfunctioninfemalepatientswith
earlyrheumatoidarthritisfollowedintheoutpatientclinicof
RAandtoevaluatethepossibleassociationbetweensexual
dysfunctionwithdiseaseactivityandfunctionaldisability.
Patients
and
methods
RApatientspertainingtotheBrasíliaCohortwereevaluated.
BrasiliaCohort14–17isanincidentcohortofpatientswithearly
RA,accompaniedattheoutpatientclinicofRheumatology,
HospitalUniversitário de Brasília, Universidade de Brasília.
Forinclusioninthiscohort,earlyRAisdefinedasthe
occur-renceofcompatiblejointsymptoms(jointpainandswelling
withaninflammatorypattern,withorwithoutmorning
stiff-nessorothermanifestationssuggestiveofinflammatoryjoint
disease,assessedbyasingleobserver)lastingmorethan 6
weeksandlessthan12months,regardlessofthefulfillment
ofthe American College of Rheumatology (ACR) criteria.18
AllpatientsselectedfulfilledretrospectivelyEULAR/ACR2010
criteria.19
From the time of diagnosis, the patients are followed
prospectively,receivingthestandardtreatmentregimenused
in the Service, including the traditional disease-modifying
antirheumaticdrugs(DMARDs)orbiologicalresponse
mod-ifiers (biological therapy), according to the patient’s need.
Currently,patientsfollowedperprotocolforupto10yearsafter
theinitialdiagnosisparticipateinthiscohort.
ThestudywasconductedfromJanuarytoMay2012,with
directinterviewsandclinicalrecordreviews.Informationon
age, durationofdisease,yearsofeducation,maritalstatus,
DiseaseActivityScore28(DAS-28)20andfunctionaldisability
questionnaire(HealthAssessmentQuestionnaire–HAQ)were
obtained.21
Thepresenceofsexualdysfunctionwasassessedthrough
completion of the Female Sexual Function Index (FSFI), a
questionnaireproposedbyRosenetal.in200022,23and
vali-datedforthePortugueseidiombyPacagnellaetal.in20099
FSFIisaself-administeredquestionnairethataimstoassess
femalesexualresponseintosixdomains:sexualdesire,sexual
arousal,vaginallubrication,orgasm,sexualsatisfactionand
pain. FSFIpresents 19questions thatevaluatesexual
func-tion inthe last four weeks.Eachquestion receives ascore
rangingfrom0to5points,andtheendresultisthesumof
the scoresforeachdomain,multipliedbyacorrection
fac-torthathomogenizestheinfluenceofeachdomain.Atotal
score≤26indicatessexualdysfunction.9,22,23Giventhatthe
instrumentusedinthisstudytoassesssexualfunction
con-templatedonlyfemalepatients,malepatientswereexcluded
fromtheanalysis.
FemalepatientsselectedconsecutivelyintoBrasiliaCohort
participated as volunteers in the study, after clarification
on its content and after signing the Free and Informed
ConsentForm.ThestudywasapprovedbytheEthics
Com-mittee, Medicine School, Universidade de Brasília (CEP-FM
030/2010).
Statisticalanalysis
Adescriptiveanalysiswasusedtodescribethegeneral
char-acteristics ofthe population. Student’st or Mann–Whitney
Table1–ComparisonsbetweenpatientswithearlyRAdividedintogroupswithandwithoutsexualdysfunction.
Characteristics ♀Withsexualdysfunction(n=43) ♀Withoutsexualdysfunction(n=11) P
Ageinyears,mean(±SD) 48.51(±12.59) 42.09(±12.64) 0.208a
Diseaseduration(±SD) 6.05(±2.19) 5.0(±2.28) 0.13a
DAS-28(±SD) 3.84(±1.53) 3.32(±1.29) 0.29a
HAQ 0.80 0.39 0.09a
Education
Illiterate(n%) 2(4.65%) 1(9.09%) 0.502b
<7yearsofeducation(n%) 13(30.23%) 2(18.18%) 0.253b
>7yearsofeducation(n%) 28(65.11%) 9(81.81%) 0.470b
Maritalstatus
Married(n%) 24(55.81%) 8(72.72%) 0.493b
Stableunion(n%) 8(18.60%) 0 0.184b
Single(n%) 3(6.97%) 2(18.18%) 0.266b
Separate(n%) 6(13.95%) 1(9.09%) 1.0b
Widower(n%) 2(4.65%) 0 1.0b
Weight
Normalweight(n%) 17(40.47%) 4(44.44%) 1.000b
Overweight(n%) 17(40.47%) 4(44.44%) 1.000b
Obesity(n%) 8(19.04%) 1(11.11%) 0.667b
a Student’st-test.
Table2–FSFIdomainsdiscriminated.
FSFIdomains Possibleanswers
Domain:sexualdesire
Question#1–Inthelastfourweeks,howoftendid youfeeldesireorsexualinterest?
1.Almostalwaysoralways
2.Mostofthetime(morethanhalfofthetime) 3.Sometimes(abouthalfofthetime)
4.Afewtimes(lessthanhalfthetime) 5.Almostnever,ornever
Question#2–Inthelastfourweeks,howdoyou rateyourlevelofdesireorsexualinterest?
1Veryhigh 2.High 3Moderate 4Low
5Veryloworabsolutelyabsent Domain:sexualarousal
Question#3–Inthelastfourweeks,howoftenyou feltsexuallyarousedduringsexualactivityor intercourse?
1.Nosexualactivity 2.Almostalways,oralways
3.Mostofthetime(morethanhalfofthetime) 4.Sometimes(abouthalfofthetime)
5.Afewtimes(lessthanhalfthetime) 6.Almostnever,ornever
Question#4–Inthepast4weeks,howwouldyou rateyourlevelofsexualarousalduringsexual activityorintercourse?
1.Nosexualactivity 2.Veryhigh 3.High 4.Moderate 5.Low
6.Verylow,orabsolutelyabsent Question#5–Inthelastfourweeks,howdoyou
rateyourlevelofassurancetobecomesexually arousedduringsexualactivityorintercourse?
1.Nosexualactivity 2.Veryhighassurance 3.Highassurance 4.Moderateassurance 5.Lowassurance
6.Verylowornoassurance Question#6–Inthepast4weeks,howoftenyou
weresatisfiedwithyoursexualarousalduring sexualactivityorintercourse?
1.Nosexualactivity 2.Almostalways,oralways
3.Mostofthetime(morethanhalfofthetime) 4.Sometimes(abouthalfofthetime)
5.Afewtimes(lessthanhalfthetime) 6.Almostnever,ornever
Domain:vaginallubrication
Question#7–Inthelastfourweeks,howoftenyou hadvaginallubrication(gota“wet”vagina)during sexualactivityorintercourse?
1.Nosexualactivity 2.Almostalways,oralways
3.Mostofthetime(morethanhalfofthetime) 4.Sometimes(abouthalfofthetime)
5.Afewtimes(lessthanhalfthetime) 6.Almostnever,ornever
Question#8–Inthelastfourweeks,howdoyou rateyourdifficultyinhavingvaginallubrication(got a“wet”vagina)duringintercourseorsexual activities?
1.Nosexualactivity
2.Extremelydifficult,orimpossible 3.Verydifficult
4.Difficult 5.Slightlydifficult 6.Notatalldifficult Question#8–Inthelastfourweeks,howdoyou
rateyourdifficultyinhavingvaginallubrication(got a“wet”vagina)duringintercourseorsexual activities?
1.Nosexualactivity
2.Extremelydifficult,orimpossible 3.Verydifficult
4.Difficult 5.Slightlydifficult 6.Notatalldifficult Question#9–Inthelastfourweeks,howoftenyou
keptvaginallubrication(gota“wet”vagina)until theendofsexualactivityorintercourse?
1.Nosexualactivity 2.Almostalways,oralways
3.Mostofthetime(morethanhalfofthetime) 4.Sometimes(abouthalfofthetime)
Table2–(Continued)
FSFIdomains Possibleanswers
6.Almostnever,ornever Question#10–Inthelastfourweeks,whichwas
yourdifficultyinmaintainingvaginallubrication (staywitha“wet”vagina)untiltheendofthesexual activityorintercourse?
1.Nosexualactivity
2.Extremelydifficult,orimpossible 3.Verydifficult
4.Difficult 5.Slightlydifficult 6.Notatalldifficult Domain:orgasm
Question#11–Inthelastfourweeks,whenyouhad sexualstimulationorpracticedintercourse,how oftenyoureachedorgasm(“sexualclimax”)?
1.Nosexualactivity 2.Almostalways,oralways
3.Mostofthetime(morethanhalfofthetime) 4.Sometimes(abouthalfofthetime)
5.Afewtimes(lessthanhalfthetime) 6.Almostnever,ornever
Question#12–Inthelastfourweeks,whenyouhad sexualstimulationorpracticedintercourse,which wasyourdifficultyinreachingorgasm(sexual climax)?
1.Nosexualactivity
2.Extremelydifficult,orimpossible 3.Verydifficult
4.Difficult 5.Slightlydifficult 6.Notatalldifficult Question#13–Inthepast4weeks,howsatisfied
wereyouwithyourabilitytoreachorgasm(sexual climax)duringsexualactivityorintercourse?
1.Nosexualactivity 2.Verysatisfied 3.Moderatelysatisfied
4.Almostequallysatisfiedanddissatisfied 5.Moderatelydissatisfied
6.Verydissatisfied Domain:sexualsatisfaction
Question#14–Inthepast4weeks,howsatisfied haveyoubeenwiththeemotionalcloseness betweenyouandyourpartnerduringsexual activity?
1.Nosexualactivity 2.Verysatisfied 3.Moderatelysatisfied
4.Almostequallysatisfiedanddissatisfied 5.Moderatelydissatisfied
6.Verydissatisfied Question#15–Inthepast4weeks,howsatisfied
haveyoubeenwithsexualrelationshipbetweenyou andyourpartner?
1.Nosexualactivity 2.Verysatisfied 3.Moderatelysatisfied
4.Almostequallysatisfiedanddissatisfied 5.Moderatelydissatisfied
6.Verydissatisfied Question#16–Inthepast4weeks,howsatisfied
haveyoubeenwithyoursexuallifeingeneral?
1.Nosexualactivity 2.Verysatisfied 3.Moderatelysatisfied
4.Almostequallysatisfiedanddissatisfied 5.Moderatelydissatisfied
6.Verydissatisfied Domain:pain
Question#17–Inthelastfourweeks,howoftenyou feltdiscomfortorpainduringvaginalpenetration?
1.Nosexualactivity 2.Almostalways,oralways
3.Mostofthetime(morethanhalfofthetime) 4.Sometimes(abouthalfofthetime)
5.Afewtimes(lessthanhalfthetime) 6.Almostnever,ornever
Question#18–Inthelastfourweeks,howoftenyou feeldiscomfortorpainfollowingvaginal
penetration?
1.Nosexualactivity 2.Almostalways,oralways
3.Mostofthetime(morethanhalfofthetime) 4.Sometimes(abouthalfofthetime)
5.Afewtimes(lessthanhalfthetime) 6.Almostnever,ornever
Question19–Inthepast4weeks,howwouldyou rateyourlevelofdiscomfortorpainduringor followingvaginalpenetration?
1.Nosexualactivity 2.Veryhigh 3.High 4.Moderate 5.Low
test was usedto analyze continuous variables. Categorical
variableswereanalyzedbyChi-squaredorFisher’sexacttest,
whereappropriate.WeconsideredP<0.05asstatistically
sig-nificant.
Results
Ofthe78patientswithearlyRAevaluatedintheperiod,68
femalepatients(87.1%ofthesample)wereselected;10male
patients(12.8%ofthesample)wereexcluded.Themeanage
ofthestudypopulationwas49.7±13.7years(mean±SD).
Regardingmaritalstatus,61.4%(35patients)reportedbeing
married,11.7%(8patients)reportedmaintainingastable
rela-tionship with a partner, 13.2% (9 patients) reported being
single,8patients(11.7%)declaredthemselvesseparateand8
patients(11.7%)reportedbeingwidowed.Withregardto
edu-cation,4.4%ofpatientswereilliterate,32.3%hadbetween1
and7yearsofformaleducationand63.2%reportedmorethan
7yearsofschooling.
Fifty-fourwomen(79.4%)reportedsexualactivityinthelast
fourweeksand14(20.5%)declaredthemselveswithnosexual
activityinthemonthprecedingthequestionnaire.The
preva-lenceofsexualdysfunction(FSFI≤26)amongthe54patients
withsexualactivitywas79.6%(43patients).
The general characteristics of patient groups with and
withoutsexualdysfunctionareshowninTable1.Inthesexual
dysfunctiongroup(43patients),97.67%wereusingsynthetic
DMARDsand 13.95%were usingbiologicalDMARDs
(inflix-imab,2;adalimumab,1;abatacept,2;andrituximab,1patient).
In the group without sexual dysfunction (11 patients),
90.90%wereusingsyntheticDMARDsand18.18%wereusing
biological DMARDs (infliximab,1 patient; and rituximab, 1
patient).
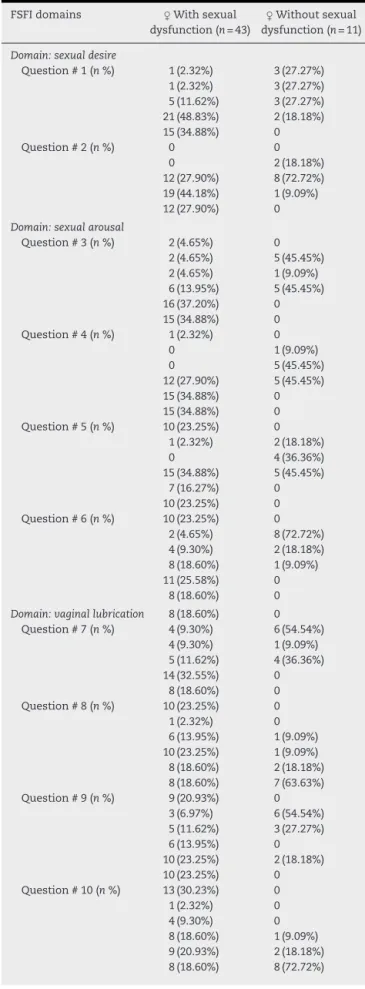
Tables2and3show,respectively,thedomainsofFSFIand
thepossibleoutcomes,separatelyforeachoneof
question-naire’squestions.
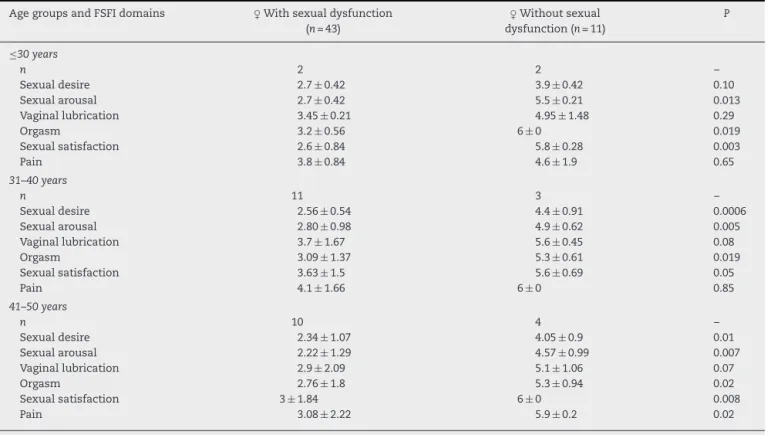
Intheevaluationofdifferentagegroups,weobserved
dif-ferencesinaffecteddomainsinFSFIinthegroupswithand
withoutsexualdysfunction(Table4).Inthegroupaged51–60
yearsandinthatgroup≥61years,onlyonepatientineach
groupshowednosexualdysfunction.Regardingthestatusof
“nosexualactivity”inthelastfourweeks,weobservedthe
followingdistribution according toage groups: ≤ 30 years,
20%(n=1)ofpatientshadnosexualactivity;31–40years,all
patientshadanactivesexuallife;41–50,6.7%hadnosexual
activity;51–60,24%(n=4)hadnosexualintercourse;≥61years,
47%(n=8)hadnosexualactivity.
Therewasnostatisticaldifferencebetweengroups(with
andwithoutsexualdysfunction)withrespecttomarital
sta-tus, length of formal education, body mass index (BMI),
disease activity(DAS-28), functional disability(HAQ) oruse
medications(syntheticDMARDsandbiologicals).
Discussion
RAcaninfluencesexualfunctioninseveralaspects.10The
rea-sonsfordisturbanceinsexualfunctioningaremultifactorial
andincludeaspectsrelatedtothedisease itself,aswell as
Table3–Resultsdetailedforeachofthesixdomainsof FSFI.
FSFIdomains ♀Withsexual dysfunction(n=43)
♀Withoutsexual dysfunction(n=11)
Domain:sexualdesire
Question#1(n%) 1(2.32%) 3(27.27%) 1(2.32%) 3(27.27%) 5(11.62%) 3(27.27%) 21(48.83%) 2(18.18%) 15(34.88%) 0 Question#2(n%) 0 0
0 2(18.18%) 12(27.90%) 8(72.72%) 19(44.18%) 1(9.09%) 12(27.90%) 0 Domain:sexualarousal
Question#3(n%) 2(4.65%) 0 2(4.65%) 5(45.45%) 2(4.65%) 1(9.09%) 6(13.95%) 5(45.45%) 16(37.20%) 0 15(34.88%) 0 Question#4(n%) 1(2.32%) 0
0 1(9.09%) 0 5(45.45%) 12(27.90%) 5(45.45%) 15(34.88%) 0 15(34.88%) 0 Question#5(n%) 10(23.25%) 0
1(2.32%) 2(18.18%) 0 4(36.36%) 15(34.88%) 5(45.45%)
7(16.27%) 0 10(23.25%) 0 Question#6(n%) 10(23.25%) 0
2(4.65%) 8(72.72%) 4(9.30%) 2(18.18%) 8(18.60%) 1(9.09%) 11(25.58%) 0
8(18.60%) 0 Domain:vaginallubrication 8(18.60%) 0
Question#7(n%) 4(9.30%) 6(54.54%) 4(9.30%) 1(9.09%) 5(11.62%) 4(36.36%) 14(32.55%) 0
8(18.60%) 0 Question#8(n%) 10(23.25%) 0 1(2.32%) 0 6(13.95%) 1(9.09%) 10(23.25%) 1(9.09%) 8(18.60%) 2(18.18%) 8(18.60%) 7(63.63%) Question#9(n%) 9(20.93%) 0
Table3–(Continued)
FSFIdomains ♀Withsexual dysfunction(n=43)
♀Withoutsexual dysfunction(n=11)
Domain:orgasm
Question#11(n%) 11(25.58%) 0 0 5(45.45%) 2(4.65%) 4(36.36%) 5(11.62%) 1(9.09%) 16(37.20%) 1(9.09%)
9(20.93%) 0 Question#12(n%) 11(25.58%) 0 1(2.32%) 0 7(16.27%) 0 10(23.25%) 0
9(20.93%) 3(27.27%) 5(11.62%) 8(72.72%) Question#13(n%) 14(32.55%) 0
2(4.65%) 7(63.63%) 10(23.25%) 4(36.36%)
5(11.62%) 0 6(13.95%) 0 6(13.95%) 0 Domain:sexualsatisfaction
Question#14(n%) 14(32.55%) 0 5(11.62%) 9(81.81%) 9(20.93%) 1(9.09%) 6(13.95%) 0 5(11.62%) 1(9.09%) 4(9.30%) 0 Question#15(n%) 15(34.88%) 0
5(11.62%) 10(90.90%) 9(20.93%) 1(9.09%) 8(18.60%) 0 5(11.62%) 0 1(2.32%) 0 Question#16(n%) 13(30.23%) 0
1(2.32%) 8(72.72%) 11(25.58%) 3(27.27%)
5(11.62%) 0 6(13.95%) 0 7(16.27%) 0
Domain:pain
Question#17(n%) 11(25.58%) 0 6(13.95%) 0 2(4.65%) 1(9.09%) 7(16.27%) 0 8(18.60%) 0 9(20.93%) 10(90.90%) Question#18(n%) 11(25.58%) 0
4(9.30%) 0 3(6.97%) 0 3(6.97%) 1(9.09%) 10(23.25%) 1(9.09%) 12(27.90%) 9(81.81%) Question#19(n%) 12(27.90%) 0
3(6.97%) 0 1(2.32%) 0 11(25.58%) 1(9.09%)
4(9.30%) 1(9.09%) 12(27.90%) 9(81.81%)
to treatment.7,24 Physicaland emotionalproblemsand
dif-ficultiesinfindingpartnershipasaresultofdisease-related
stresscontributetoalessactiveandoftenlesspleasant
sex-ual life.7,24 Chronic pain, fatigue and low self-esteem can
diminishthesexualinterest,thusreducingthefrequencyof
intercourse.7,24
In ourstudy, wefounda high frequencyofsexual
dys-function(79.6%)ofpatientswithactivesexuallife,ahigher
figurethaninmostpreviousstudiesinpatientswith
estab-lishedRA.4,7,10–12 Abdel-Nasseretal.3showedintheirstudy
thatover60%offemalepatientswithRAhaddifficultyin
sex-ualperformance(sexualdisability)andasignificantdecrease
insexdrive.3
Inapreviousstudyconductedbyourgroup25thatevaluated
163 patientswithdiagnoses ofvarious rheumaticdiseases,
including 24 patients with established RA, we found
sex-ual dysfunctionin18.4% ofevaluatedpatients,and 8.3%of
patientswithRAhadaFSFIscore<26.Itisimportantto
men-tion that in this previous study, 24.2% of all patients and
17% ofRApatientshadnosexualactivityduringthestudy
period.However,wewouldexpectalowerfrequencyof
sex-ualdysfunctioninpatientswithearlyRAthaninthosewith
establishedRA,inviewofanearliertreatment,andpossibly
thepresenceoflessdeformityinpatientswithearlydisease.
Thisdifferenceinprevalencemaybeexplainedbyother
fac-torsthatinfluencesexualfunction,suchasemotionalissues
andcomorbidities,suchasdepression,whichwerenot
eval-uatedinourstudy.Insupportofthis explanation,Karlsson
et al.26 foundthat patientswithearly RAare less satisfied
withtheirlifeasawhole,comparedwithareferencegroup
ofpatientswithlong-termillness.
Patients withearly RAalsoreported lowlevels of
satis-faction withself-care,work and sexuallifeactivities.7,26 In
ourstudy,wedidnotevaluatelaborandself-careability
vari-ables.
Hill et al. evaluated the effect of RA on the
rela-tionship between partners and demonstrated that 35% of
patients believed thatthe disease interfered withthe
rela-tionshipwiththepartner,duetoproblemssuchasdecrease
in daily and social activities and emotional and financial
changes.4,6
In the present study,we found no association between
the occurrence of sexual dysfunction and disease activity.
Also,nosignificantassociationbetweenfunctionaldisability
andsexualdysfunctionwasobserved.However,inthestudy
ofAbdel-Nasseretal.,3sexualdisabilitywasrelated,among
otherfactors,todiseaseactivity,painanddisabilitymeasured
byHAQ.Inanotherstudy,ElMiedanyetal.10showeda
preva-lenceof45.7%ofSDinfemalepatientsdiagnosedwithRA,
showing correlationof SDwith several markersof disease
activity.
We observed the influence ofage in relation to sexual
dysfunction,asexpected.Withincreasingage,moreofFSFI
domainswereaffected,withanincreaseofthepercentageof
patientswithoutsexualactivity.
In 2007, a French study from the Association Franc¸aise
des Polyarthritiquesevaluated theimpact ofRAon patients’
sexuality bysendingquestionnairestoabout7700patients.
Table4–FSFIdomainsaccordingtoagegroups.
AgegroupsandFSFIdomains ♀Withsexualdysfunction (n=43)
♀Withoutsexual dysfunction(n=11)
P
≤30years
n 2 2 –
Sexualdesire 2.7±0.42 3.9±0.42 0.10
Sexualarousal 2.7±0.42 5.5±0.21 0.013
Vaginallubrication 3.45±0.21 4.95±1.48 0.29
Orgasm 3.2±0.56 6±0 0.019
Sexualsatisfaction 2.6±0.84 5.8±0.28 0.003
Pain 3.8±0.84 4.6±1.9 0.65
31–40years
n 11 3 –
Sexualdesire 2.56±0.54 4.4±0.91 0.0006
Sexualarousal 2.80±0.98 4.9±0.62 0.005
Vaginallubrication 3.7±1.67 5.6±0.45 0.08
Orgasm 3.09±1.37 5.3±0.61 0.019
Sexualsatisfaction 3.63±1.5 5.6±0.69 0.05
Pain 4.1±1.66 6±0 0.85
41–50years
n 10 4 –
Sexualdesire 2.34±1.07 4.05±0.9 0.01
Sexualarousal 2.22±1.29 4.57±0.99 0.007
Vaginallubrication 2.9±2.09 5.1±1.06 0.07
Orgasm 2.76±1.8 5.3±0.94 0.02
Sexualsatisfaction 3±1.84 6±0 0.008
Pain 3.08±2.22 5.9±0.2 0.02
Student’st-testusedinalltheseanalyzes.
51% reported an adverse impact of the disease on their sexuality.10,11,27
StudiesinRApatientsunselectedfordiseaseduration
sug-gestthat obesityisassociatedindependently withaworse
quality oflife.28 Obesity is associatedwith higher
concen-trationsofinflammationmarkerssuchasC-reactiveprotein
(CRP), interleukin 6(IL-6) and tumornecrosis factor alpha
(TNF-␣)andthereforeobeseRApatientsmaypresentwitha
moresevereandactivedisease.28,29
García-Pomaetal.29reportedthat,inpatientswithRA,the
health-relatedqualityoflifeisimpairedduetoseveralfactors.
Intheirstudy,theseauthors suggestthat patientswithRA
whoare obesearemorelikelytopresentareducedquality
oflifecomparedwithnormal-weightpatients, regardlessof
othercharacteristicssuchasgender,age,activityofdisease,
extra-articulardisease,presenceofrheumatoidfactor,levelof
depression,socioeconomicstatus,ordiseaseduration.Inthis
study,wefoundnodirectrelationshipbetweentheprevalence
ofsexualdysfunctionandtheoccurrenceofobesityamong
patientswithearlyRA.
Sexual functioning isa neglected area of quality oflife
inpatients with rheumatic diseases.7 Rheumatologists are
increasingly willing to discuss areas that are not directly
relatedto thepharmacological treatmentofjoint diseases,
suchasquality oflife,fatigueandpatienteducation.
How-ever,sexualityisrarelyaddressedinrelationtothequalityof
life.11,30
Inarecentsurveywithtenrheumatologists,only12%of
patientsseenintheirclinicalpracticehavebeenevaluatedfor
sexualactivity.31Thisapparentlackofinterest,bythe
physi-cian,withrespectofthesexualfunctionoftheirpatientscould
be explained,according torespondents, byfactors suchas
limitedconsultationtime,discomfortwhendiscussing
sexu-ality(bothbyphysicianandpatient),anduncertaintiesabout
the role ofthe doctorsand theircompetence on issuesof
patients’sexuality.3,7,11,31Thisdemonstratestheimportance
offurtherstudiesthatevaluatesexualfunctioninrheumatic
diseasesandtheirdisclosureamongexperts,aimingatamore
comprehensivetreatmentofpatients.
Ourstudyhassomelimitations.Thisisacross-sectional
study, which, thus,does not allowthe establishment ofa
cause-effect relationship. The number of female patients
evaluated inthis study was relatively small,especially the
number ofpatients withearly RAwithout sexual
dysfunc-tion, which constituted a minority ofthe total number of
assessedwomen. Anotherlimiting factorwas thefact that
the patients were evaluated in a cohort study in a
ter-tiary hospital, aregionalreference inRheumatology. Thus,
probablyourevaluatedfemalepatientshadmoresevere
con-ditions thanpatients followed upina primaryhealthcare
service. Furthermore,wedidnotevaluateother
comorbidi-tiesthatmayinfluencesexualfunction,suchasdepression
andSjögren’ssyndrome.Thesefactorsshouldbetakeninto
consideration, so that the results observed should not be
extrapolated for all female patients diagnosed with early
RA.
However,thisisthefirststudy whichweare awarethat
RA,withaconcomitantevaluationoffunctionaldisabilityand
diseaseactivity.
Conclusion
Theprevalenceofsexualdysfunctionfoundinthisstudywas
highercomparedbothwiththefigurespublishedinthe
lit-erature in healthy women (up to 40%), as those found in
patientswithrheumatoidarthritis(31–76%),including
previ-ouscasesofestablishedRAinourService.Giventhatsexuality
isregardedasoneofthemajordeterminantsofreduced
qual-ity oflife, questions that address these aspects should be
amongtheparametersthat evaluatethecourseofdisease.
Studiesassessingtheextentofsexualdysfunctioninaspecific
mannerwithrespecttopatientswithearlyRAarenecessary,
sothattherapeuticalternativesaimingtoimprovenotonly
thephysicalhealth,butalsothequalityoflifeofthepatient,
beoffered.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
TheauthorswishtothankTatianeVazTeixeiradeOliveira,
MelianeTeixeiraCardosoandGabrielaPorfírioJardimSantos
fortheirassistanceindatacollectionforthepresentstudy.
r
e
f
e
r
e
n
c
e
s
1. MotaLMH,CruzBA,BrenolCV,PereiraIA,FronzaLSR,Bertolo MB,etal.ConsensodaSociedadeBrasileiradeReumatologia 2011paradiagnósticoeavaliac¸ãoinicialdaartrite
reumatoide.RevBrasReumatol.2011;51(3):199–219.
2. MotaLMH,CruzBA,BrenolCV,PereiraIA,FronzaLSR,Bertolo MB,etal.Consenso2012daSociedadeBrasileirade
Reumatologiaparaotratamentodaartritereumatoide.Rev BrasReumatol.2012;52(2):152–74.
3. Abdel-NasserAM,AliEI.Determinantsofsexualdisability anddissatisfactioninfemalepatientswithrheumatoid arthritis.ClinRheumatol.2006;25:822–30.
4. AraújoDB,BorbaEF,AbdoCHN,SouzaLAL,
Goldstein-SchainbergC,ChahadeWB,etal.Func¸ãosexual emdoenc¸asreumáticas.ActaReumatolPort.2010;35:16–23.
5. KurizkyPS,MotaLMH.Sexualdysfunctioninpatientswith psoriasisandpsoriaticarthritis:asystematicreview.RevBras Reumatol.2014;52:943–8.
6. HillJ,BirdH,ThorpeR.Effectsofrheumatoidarthritison sexualactivityandrelationships.Rheumatology. 2003;42:280–6.
7. TristanoAG.Theimpactofrheumaticdiseasesonsexual function.RheumatolInt.2009;29:853–60.
8. LewisRW,Fugl-MeyerKS,BoschR,Fugl-MeyerAR,Laumann EO,LizzaE,etal.Epidemiologyriskfactorsofsexual dysfunction.JSexMed.2004;1:35–9.
9.PacagnellaRC,MartinezEZ,VieiraEM.Validadedeconstruto deumaversãoemportuguêsdoFemaleSexualFunction Index.CadSaúdePública.2009;25(11):2333–44.
10.ElMiedanyY,ElGaafaryM,ElAroussyN,YoussefS,AhmedI. Sexualdysfunctioninrheumatoidarthritispatients:arthritis andbeyond.ClinRheumatol.2012;31(4):601–6.
11.PerdrigerA,SolanoC,GossecL.Whyshouldrheumatologists evaluatetheimpactofrheumatoidarthritisonsexuality?J BoneSpine.2010;77:493–5.
12.VanBerloWTM,VandeWielHBM,TaalE,RaskerJJ,Weijmar SchultzWCM,VanRijswijkMH.Sexualfunctioningofpeople withrheumatoidarthritis:amulticenterstudy.Clin
Rheumatol.2007;26:30–8.
13.YoshinoS,UchidaS.Sexualproblemsofwomenwith rheumatoidarthritis.ArchPhysRehabil.1981;62(3): 122–3.
14.MotaLMH,SantosNetoLL,PereiraIA,BurlingameR,Ménard HA,LaurindoIM.Autoantibodiesinearlyrheumatoid arthritis:Brasíliacohort:resultsofathree-yearserial analysis.RevBrasReumatol.2011;51(6):564–71.
15.MotaLMH,DosSantosNetoLL,BurlingameR,MénardHA, LaurindoIM.Laboratorycharacteristicsofacohortofpatients withearlyrheumatoidarthritis.RevBrasReumatol.
2010;50(4):375–88.
16.MotaLMH,LaurindoIM,DosSantosNetoLL.Prospective evaluationofthequalityoflifeinacohortofpatientswith earlyrheumatoidarthritis.RevBrasReumatol.
2010;50(3):249–61.
17.MotaLMH,LaurindoIM,DosSantosNetoLL.Demographic andclinicalcharacteristicsofacohortofpatientswithearly rheumatoidarthritis.RevBrasReumatol.2010;50(3): 235–48.
18.ArnettFC,EdworthySM,BlochDA,McshaneDJ,FriesJF, CooperNS,etal.TheAmericanRheumatismAssociation 1987revisedcriteriaforclassificationofrheumatoidarthritis. ArthritisRheum.1998;31:315–24.
19.AletahaD,NeogiT,SilmanAJ,FunovitsJ,FelsonDT,Bingham CO3rd,etal.2010Rheumatoidarthritisclassificationcriteria. ArthritisRheum.2010;62:2569–81.
20.PrevooMLL,Van ´THofMA,KuperHH,VanLeewenMA,Vande Putte,VanRielPLC.Modifieddiseaseactivityscoresthat includetwenty-eight-jointcounts.Developmentand validationinaprospectivelongitudinalstudyofpatientswith rheumatoidarthritis.ArthritisRheum.1995;38:
44–8.
21.FriesJF,SpitzPW,KrainesRG,HolmanHR.Measurementof patientoutcomeinarthritis.ArthritisRheum.1980;23: 137–45.
22.RosenR,BrownC,HeimanJ,LeiblumS,MestonC,ShabsighR, etal.Thefemalesexualfunctionindex(FSFI):a
multidimensionalself-reportinstrumentfortheassessment offemalesexualfunction.JSexMaritalTher.2000;26: 191–208.
23.WiegelM,MestonC,RosenR.Thefemalesexualfunction index(FSFI):cross-validationanddevelopmentofclinical cutoffscores.JSexMaritalTher.2005;31:1–20.
24.Østensen´ M.Newinsightsintosexualfunctionandfertilityin rheumaticdiseases.BestPractResClinRheumatol.
2004;18:219–32.
25.FerreiraCC,MotaLMH,OliveiraACV,CarvalhoJF,LimaRAC,
SimaanCK,etal.Frequênciadedisfunc¸ãosexualem
mulherescomdoenc¸asreumáticas.RevBrasReumatol.2014,
http://dx.doi.org/10.1590/S0482-50042013000100004. 26.KalssonB,BerglinE,Wållberg-JonssonS.Lifesatisfactionin
earlyrheumatoidarthritis:aprospectivestudy.ScandJOccup Ther.2006;13(3):193–9.
28.Stavropoulos-KalinoglouA,MetsiosGS,KoutedakisY,Kitas GD.Obesityinrheumatoidarthritis.Rheumatology. 2011;50:450–62.
29.García-PomaA,SegamiMI,MoraCS,UgarteMF,TerrazasHN, RhorEA,etal.Obesityisindependentlyassociatedwith impairedqualityoflifeinpatientswithrheumatoidarthritis. ClinRheumatol.2007;26:1831–5.
30.AbourazzakF,ElMansouriL,HuchetD,Lozac’hmeurR, Hajjaj-HassouniN,IngelsA,etal.Long-termeffectsof therapeuticeducationforpatientswithrheumatoidarthritis. JointBoneSpine.2009;76:648–53.