www.rpped.com.br
REVISTA
PAULISTA
DE
PEDIATRIA
ORIGINAL
ARTICLE
Family’s
presence
in
the
pediatric
emergency
room:
opinion
of
health’s
professionals
Francine
Fernandes
Pires
Mekitarian
a,∗,
Margareth
Angelo
baHospitalUniversitáriodaUniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil bUniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
Received25November2014;accepted12March2015 Availableonline28August2015
KEYWORDS
Pediatrics;
Emergencymedical services;
Patientcareteam; Professional---family relations
Abstract
Objective: Tolearntheopinionofhealthprofessionalsregardingthepresenceoffamilyduring pediatricemergencycare.
Methods: Cross-sectionalstudy,performedwith46healthprofessionals,membersofthe medi-cal and nursing team of a pediatric emergency service. The data were collected via the applicationofaquestionnairecomposedby variablesrelatedtotheopinionofprofessionals aboutthestudiedsubject,inlinewiththeprofessionalcategoryandthevocationaltraining time,aswellasinvasiveproceduresduringwhichthepresenceoffamilyisauthorizedbythe professionals.
Results: Themedicalstaffandtheprofessionalswithshortertimeaftergraduation(<10years) weremorefavorabletothepresenceoffamilyduringemergencyprocedures.Regardingthe complexityoftheprocedures,thenursingstaffprovedmorefavorabletothepresenceoffamily duringlesscomplexprocedures---peripheralvenouspunctureandfluidsample---whereasthe consent ofthe medicalstaff was similar, regardless theperformed procedure ---peripheral venouspuncture,fluidsample,intraosseouspuncture,trachealintubationandcardiopulmonary resuscitation.
Conclusions: Inordertoallowthepresenceoffamilyintheemergencyroom,itisnecessaryto sensitizehealthprofessionals,especiallythenursingstaffandthelonger-termacting profes-sionals,whicharemoreresistanttoallowthefamilytostaywiththechildduringtheemergency care.
©2015SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-license(https://creativecommons.org/licenses/by/4.0/).
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.rpped.2015.03.010
∗Correspondingauthor.
E-mail:[email protected](F.F.P.Mekitarian).
2359-3482/©2015SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC
PALAVRAS-CHAVE
Pediatria;
Servic¸osmédicosde emergência;
Equipedeassistência aopaciente;
Relac¸ões
profissional-família
Presenc¸adafamíliaemsaladeemergênciapediátrica:opiniõesdosprofissionaisde saúde
Resumo
Objetivo: Conhecer asopiniões deprofissionais de saúdeem relac¸ãoàpresenc¸a dafamília duranteoatendimentoemsaladeemergênciapediátrica.
Métodos: Estudotransversal,realizadocom46profissionaisdesaúde,integrantesdasequipes médicaedeenfermagem,deumservic¸odepronto-socorroinfantil.Osdadosforamcoletados pormeiodaaplicac¸ãodeumquestionáriocompostoporvariáveisrelacionadasàopiniãodos profissionaisem relac¸ãoaotemaestudado,associadaàcategoria profissionaleaotempode formac¸ãoprofissional,alémdequaisprocedimentosinvasivosemqueosprofissionaisautorizam apresenc¸adafamília.
Resultados: Aequipemédicaeosprofissionaiscommenortempodeformac¸ão(<10anos)foram maisfavoráveisàpresenc¸adafamíliaduranteosprocedimentosdeemergência.Emrelac¸ão à complexidade dos procedimentos,a equipede enfermagem se mostrou mais favorável à presenc¸adafamíliaemprocedimentosmenoscomplexos---punc¸ãovenosaperiféricaecoletade líquor,enquantoaconcordânciadaequipemédicafoisimilar,independentedoprocedimento realizado---punc¸ãovenosaperiférica,coletadeliquor,punc¸ãointraóssea,intubac¸ãotraqueale reanimac¸ãocardiopulmonar.
Conclusões: Parapermitirapresenc¸adafamíliaemsaladeemergência,énecessário sensibi-lizarprofissionaisdesaúde,especialmenteaequipedeenfermagemeosprofissionaisformados hámais tempo, quesãomais resistentesapermitirque afamíliafique ao lado dacrianc¸a duranteoatendimentodeemergência.
©2015SociedadedePediatriadeS˜aoPaulo.PublicadoporElsevierEditoraLtda.Esteéumartigo OpenAccesssobalicençaCCBY(https://creativecommons.org/licenses/by/4.0/deed.pt).
Introduction
Family-CenteredCare(FCC)isaglobaltrendinhealthcare provision. Itsmain premiseis thatthe assistanceshall be plannedfortheentirefamilyandnotjustforthepatient. Thiscaremodel startedbetweenthedecadesof1950---60, fromthemomentwhenthenegativepsychological effects that physical separation of parents had onchildren were recognized,andthereforeparentscouldbeincludedinthe careoftheirchildwithinthehospitalenvironment.1
In Brazil, this model ofcare is not yet integrated into thehealthcareservices.AlthoughtheChildandAdolescent Statute(EstatutodaCrianc¸aedoAdolescente)recommends the permanent presence of parents next to the hospital-izedchild,itisnotonlythispresencethatwillensurethat FCCwillbefollowed.2Inadditiontoallowingthepresence of the family, one must also recognize the family needs, perspectivesandchoices.3
According to the FCC guideline, families should be encouraged toparticipate in patient care at all levelsof hospitalcare.3 Considering theintroduction of thismodel of care in the emergency room, it becomes necessary to allow families todecide whetherthey want or not to be close tothe patientduring invasive and cardiopulmonary resuscitation(CPR)procedures.4
Althoughinternationalorganizations,suchasthe Amer-icanHeartAssociation andtheEmergencyNurses Associa-tion,recommendamodelofcarethatfavorsthepresence offamilymembersduringinvasiveandCPRproceduresinthe emergencyroom,familymembersarestillinvitedbyhealth professionalstoleavetheroom.5,6Itisessentialthatsuch
practicebe normalized by institutional protocols, sothat thisdecisiondoesnotdependexclusivelyonthehealthcare team.4
In general, as it is the healthcare team who decides whetherthefamilycan stay inthe emergencyroom,it is importanttounderstandtheirperspectives.Health profes-sionalsjustify that theyaskthe familiestoleave for fear the family willlose emotional control and interfere with theprovidedcare.Theyalsobelievethat,withthefamily presentduring care,the professionalsmight feelanxious, especiallythe professionalsintraining,whichcould inter-ferewiththeircapacityandconcentrationwhenperforming theprocedures.Additionally,theyreportthefearthatthe family will keep stressful memories related to the care, evenmoresoinunfavorableoutcomes.7 Althoughthereis noscientificevidencetosupportthesebeliefs,thisremains awidelydebatablesubject.
Method
This wasacross-sectional study,performed by applyinga questionnaireinthechildemergencyroomofHospital Uni-versitário(HU)ofUniversidadedeSãoPaulo(USP).Thestudy site is a secondary-care public teaching hospital, which treatschildrenfrombirthto14yearsofage.Thisservicehas noprotocolthatregulatesthepresenceoffamilymembers intheemergencyroom,butthispracticeisoftenaccepted byhealthprofessionalsintheunit.Thedecisiontoallowor notthepresenceoffamilymembersintheemergencyroom ismadeatthetimeoftreatment.
Study subjects were professionals from the multidis-ciplinary team working in the emergency care service, consistingofphysiciansandmedicalresidents,nurses, nurs-ing technicians and assistants. The other professionals of themultidisciplinaryteamwerenotincluded,becauseonly themedicaland nursing staffs workat the study site.No exclusioncriteriaweredefinedtoselectthesample.
Theparticipantswereaddressedbythemain investiga-tor,a nursefrom that sector, and received, after signing theInformed Consent Form, aquestionnaire consisting of variablesrelatedtoage,gender,professionalcategory,time since graduation,whether professionals had had a previ-ousexperiencewiththepresenceoffamilymembersinthe emergencyroom(yesorno)andduringwhichinvasive pro-cedureshealth professionals would allow the presence of thefamily(peripheralvenouspuncture,CSFsample collec-tion,intraosseouspuncture, intubationand CPR).Forthis lastitem,theparticipantswereabletocheckasmanyitems astheyconsideredadequate.
To betterunderstand the viewsof professionalsonthe assessedsubject,qualitativequestionswereincluded,with thefirstonebeing‘‘whodoyouthinkmustdecidewhether thefamilycanstayintheemergencycareroom?’’Another questionwasalsomadethatallowedassessingthereasons whyprofessionalsincludeorexcludethefamiliesfromthe room--- ‘‘Whatdoyouthinkabout the presenceof family membersintheemergencyroomduringthechild’scare?’’
Thequestionnairewascreatedbytheauthors,basedon evidenceofstudiesavailableintheinternationalliterature. Thefinalversionwassubmittedtoexaminers---professionals thatwereexpertsintheassessedsubjectandexperienced intheconstructionoftools ---toassesstheclarityandthe semanticaspectofthequestions.Consideringthepositive toolassessment,apilotstudywasnotcarriedout.The par-ticipantsagreedtoreturnthefilledoutquestionnairetothe maininvestigatoroneweekafterreceivingit.
To allow statistical analysis, the professionals were groupedaccording totheirprofessionalcategory: medical staff(doctorsandresidents)andnursingstaff(nurses, nurs-ingtechniciansandassistants).Anothergroupwascreated in relation to time since graduation: less than 10 years and10yearsor moreafter graduation.Asthe profession-als’answerstothequalitativequestion‘‘whodoyouthink should decide whether the family can stay in the emer-gencycareroom?’’wereonly:familyorhealthprofessionals, thesetwogroupsofresponsesweregroupedandthe statisti-calanalysisstepswerefollowed,accordingtothevariables professionalcategoryandtimesincegraduation.
Inordertoverifytheexistence ofastatistical associa-tionbetweenallowingthe presenceof familymembersin
theemergencyroom,theprofessionalcategory,timesince graduation and who must decide whether the family can be present during care, chi-square test or Fisher’s exact testwereused.8Regardingtheassociationbetween allow-ingthepresenceoffamilymembersintheemergencyroom andthetypeofprocedureperformed,generalized estimat-ingequations withbinomialdistributionfunctionandlogit associationwereapplied.9Alltestswereperformedusinga 5%significancelevel,andSPSS15.0software(IBM,Chicago, USA)wasusedforthestatisticalanalyses.
Theanalysisoftheanswersgiventothequalitative ques-tion ‘‘What do you think about the presence of family membersintheemergencyroomduringthechild’scare?’’ followed the thematic coding steps.10 Initially, the data were interpreted individually and codes were developed that wereappropriatetothe opinion ofeach participant. Subsequently,thedataweregroupedbytheir similarities, amongthemthereasonswhyprofessionalsallowordonot allowfamiliestostayintheemergencyroom.
The study was approved by the HU USP’s (protocol 1182/12)andEscoladeEnfermagemdaUSP’sInstitutional ReviewBoard(protocol1102/2011).Thedatacollectionwas carriedoutinMarch2012.
Results
Allhealthunitprofessionals(n=46)wereinvitedto partici-pateinthestudy,andthereturnrateofthequestionnaires was 100%. Most professionals were females (78.3%) and belonged to the nursing staff (56.5%), reported they had already provided care in the emergency room when the family was present (95.7%), and had 10 years or more sincegraduation(65.2%).Whenconsideringthedistribution amongtheprofessionalcategoriesandthetimesince grad-uation:70%ofthenursingteamhad10ormoreyearssince graduation,whileonly30%ofthemedicalstaffhadthesame periodoftimesincegraduation.
As almost the entire sample had had the experience of providing care with the presence of the family in the emergency room, the statistical association between this variableandthe professionals’opinion regardingthe ana-lyzedpracticewasnotcarriedout.
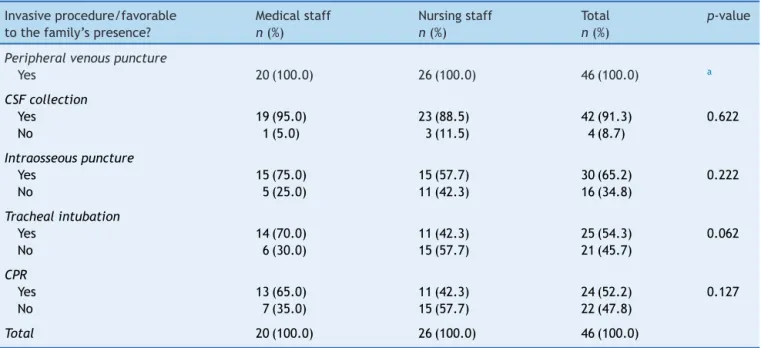
According to Table 1, the opinion of the professionals regardingthepresenceoffamilymembersintheemergency roomwasnotassociatedtotheprofessionalcategoryforany ofthestudiedprocedures.Thedatasuggest,however,that themedicalstaffwasmorefavorabletothepresenceofthe familyforallassessedinvasiveprocedures,comparedtothe nursingstaff.
Table 2 shows that professionals with less time since graduationconsidered,ascomparedtothosewith10years or more sincegraduation,that the familycan bepresent while thestaffis performingtrachealintubationsandCPR procedures(p=0.007andp=0.024,respectively).Forother procedures,thedataalsoindicate,althoughwithout statis-ticalassociation,thatprofessionalsmorerecentlygraduated aremore favorableto thefamily’s presencein the emer-gencyroom.
Table1 Healthcare professionals’ opinion regardingthe presence of familymembers in thepediatric emergency room, accordingtotheprofessionalcategoryandtypeofprocedureperformed.
Invasiveprocedure/favorable tothefamily’spresence?
Medicalstaff n(%)
Nursingstaff n(%)
Total n(%)
p-value
Peripheralvenouspuncture
Yes 20(100.0) 26(100.0) 46(100.0) a
CSFcollection
Yes 19(95.0) 23(88.5) 42(91.3) 0.622
No 1(5.0) 3(11.5) 4(8.7)
Intraosseouspuncture
Yes 15(75.0) 15(57.7) 30(65.2) 0.222
No 5(25.0) 11(42.3) 16(34.8)
Trachealintubation
Yes 14(70.0) 11(42.3) 25(54.3) 0.062
No 6(30.0) 15(57.7) 21(45.7)
CPR
Yes 13(65.0) 11(42.3) 24(52.2) 0.127
No 7(35.0) 15(57.7) 22(47.8)
Total 20(100.0) 26(100.0) 46(100.0)
CSF,cerebrospinalfluid;CPR,cardiopulmonaryresuscitation. a Allprofessionalsacceptthefamily’spresenceforthisprocedure.
than10yearssincegraduationaremoreinclinedtoaccept (p=0.034) that families shouldparticipate in thisdecision (Table3).
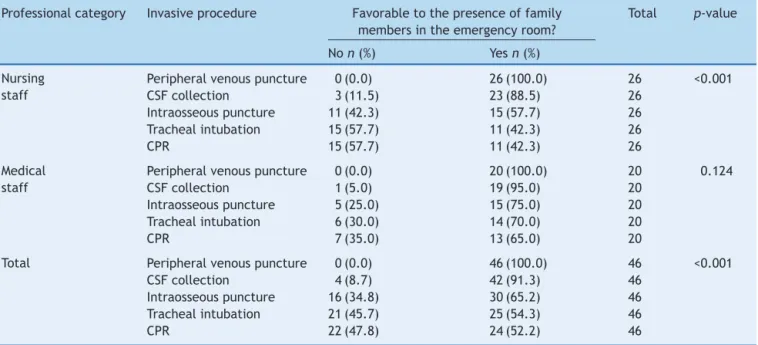
Regarding the association between the presence of familymembersin thepediatricemergencyroomand the complexity of the performed procedures, the following increasing order of acceptance was observed (Table 4): peripheral venous puncture, CSF sample collection,
intraosseous puncture, tracheal intubation and CPR. The nursingstaffwasmorefavorabletothefamily’spresencein lesscomplex procedures(peripheral venous puncture and CSFsamplecollection;p<0.001)comparedtomorecomplex procedures (intraosseous puncture, intubation and CPR). However, the agreement of the medical team regarding the presence of family members was similar (p=0.124), regardlessoftheperformedprocedure.
Table2 Healthcareprofessionals’opinionregardingthefamily’spresenceinpediatricemergencyroom,accordingtotime sincegraduationandtypeofprocedure.
Invasiveprocedure/favorable tothefamily’spresence?
Timesincegraduation Total p-value
<10yearsn(%) ≥10yearsn(%) n(%)
Peripheralvenouspuncture
Yes 16(100.0) 30(100.0) 46(100.0) a
CSFcollection
Yes 16(100.0) 26(86.7) 42(91.3) 0.282
No 0(0.0) 4(13.3) 4(8.7) *
Intraosseouspuncture
Yes 13(81.3) 17(56.7) 30(65.2) 0.095
No 3(18.8) 13(43.3) 16(34.8)
Trachealintubation
Yes 13(81.3) 12(40.0) 25(54.3) 0.007
No 3(18.8) 18(60.0) 21(45.7)
CPR
Yes 12(75.0) 12(40.0) 24(52.2) 0.024
No 4(25.0) 18(60.0) 22(47.8)
Total 16(100.0) 30(100.0) 46(100.0)
CPR,cardiopulmonaryresuscitation.
Table3 Opinionaboutwhoshoulddecideifthefamilymayormaynotbepresentduringemergencyproceduresinapediatric emergencyroom,accordingtoprofessionalcategoryandtimesincegraduation.
Whoshoulddecidewhetherornotthefamilycan stayintheemergencyroom
p-value
Familyn(%) Healthcareprofessionalsn(%)
Professionalcategory 0.707
Medicalstaff 6(33.3) 12(66.7) Nursingstaff 7(28.0) 18(72.0)
Timesincegraduation 0.034
<10years (53.3) 7(46.7)
≥10years 5(17.9) 23(82.1)
Total 13(30.2) 30(69.8)
Threecaseswereexcludedfromthisanalysisduetotheimpossibilityofdeterminingtheanswertothisquestion.
Table4 Opinionofeachprofessionalcategory regardingthepresenceoffamilymembersinthepediatricemergencyroom accordingtotheprocedureperformed.
Professionalcategory Invasiveprocedure Favorabletothepresenceoffamily membersintheemergencyroom?
Total p-value
Non(%) Yesn(%)
Nursing staff
Peripheralvenouspuncture 0(0.0) 26(100.0) 26 <0.001 CSFcollection 3(11.5) 23(88.5) 26
Intraosseouspuncture 11(42.3) 15(57.7) 26 Trachealintubation 15(57.7) 11(42.3) 26
CPR 15(57.7) 11(42.3) 26
Medical staff
Peripheralvenouspuncture 0(0.0) 20(100.0) 20 0.124 CSFcollection 1(5.0) 19(95.0) 20
Intraosseouspuncture 5(25.0) 15(75.0) 20 Trachealintubation 6(30.0) 14(70.0) 20
CPR 7(35.0) 13(65.0) 20
Total Peripheralvenouspuncture 0(0.0) 46(100.0) 46 <0.001 CSFcollection 4(8.7) 42(91.3) 46
Intraosseouspuncture 16(34.8) 30(65.2) 46 Trachealintubation 21(45.7) 25(54.3) 46
CPR 22(47.8) 24(52.2) 46
The reasons why professionals include families in the emergency room were: to have the family observe their effortstosave thechild’slife;tohavethefamilyprovide importantinformationaboutthepatient;itisthefamily’s righttobethere, andtohave thefamilyprovide reassur-ance to the child. The reasons that led them toexclude familieswere:professionalsdonothavetimetopay atten-tionto the families,the family presence hinders training providedtostudents,thefamilyinterfereswiththe profes-sionals’work,theneedfor aprofessionaltostay withthe family,andfamilykeepsnegativememoriesofthecare.
Discussion
Thisstudyisapioneerinthenationalliteratureonthe opin-ionofhealthprofessionalsworkinginachildren’semergency roomregardingthepresenceoffamilymembersintheER. As, ingeneral, the health professionals arethe ones who
decide whether the familywill be allowed tostay in the emergency care room,knowing their opinions is essential todrawstrategies thatcanmodifythehealthcareteam’s approachandrecognizethefamily’sneedsintheemergency environment.
Thenumberofprofessionalswhoreportedhaving partic-ipatedin an emergencycallwhen thefamilywaspresent isfarsuperiortothosepreviouslyreportedintheliterature --- 23.1---70.1%.11,12 This findingcouldmean a positive sce-nariofor theimplementationofstrategiesoftheFCCcare model,asthepreviousexperiencewiththepresenceof fam-ily members in the emergencyroom hasshown tobe the mostfavorabledeterminantforattainingthispractice.13
The factthatprofessionalswithlesstimesince gradua-tionaremorefavorabletothepresenceoffamilymembers during emergency care reinforces the observed results regardingthefactthatthemedicalstaffwasmorefavorable tothefamily’spresenceintheemergencyroom,sincemost oftheseprofessionals(70%)hadgraduatedlessthan10years before.There is nocorrelation in the literaturebetween timeofexperienceinemergencyservicesandactionstaken bytheprofessionalsregardingthepresenceofthefamilyin theemergencyroom.16
Most professionals believe that the family should not participateinthedecision-makingregardingtheirown pres-ence in the emergency room. These data mainly reflect theviewsoftheprofessionalswithlongertimesince grad-uation. Results available in the literature also show that healthprofessionalsdisregardthefamily’sautonomyinthis decision-makingprocess.12,17
The increased practice related to less invasive proce-dures in daily life seems to give professionals a greater degree of confidence in carrying out these procedures, whichcouldexplainthefindingsintheliterature,17,18which showthatthemoreinvasivetheprocedure,thelessoften professionals arefavorabletothe presenceof the family. However,inourstudy,onlythenursingstaffdemonstrated thispreferenceregardingthefamilypresenceonlyfor the lessinvasiveprocedures.
The reasons that led professionals toallow or not the presenceof familymembersinthe emergencyroomwere similartothosegivenbydoctorsandnursesininternational studies,showingthattheculturalcontexthadlittleimpact ontheperceptionofthehealthteamtodecidetoallowor notthefamilytobepresentduringemergencycare.19---21Itis essentialthattheneedsofthefamilies,eveninemergency situations,betakenintoconsiderationduringtheprovided care, asthe family’spresence in a situationin which the healthteammembers arenotpreparedtorecognize their needsmayhavemorenegativeconsequencesfor the fam-ilies thannot beingclosetotheirrelative.22 Studieshave shownthat,whenthe optionisgiven,thefamiliesusually choosetostayduringemergencycare,andtheirpresence helpsthemourningprocessincaseofdeath,providesamore effective communication with the multidisciplinary team andallowsthemtoverifythatallthenecessaryeffortswere madetosavethepatient’slife.23,24
A favorableenvironment topromotethe family’s pres-enceinthe emergencyroomincludesthe developmentof a professional awareness program for the team’s capaci-tation to include families in this scenario and recognize thebenefits thatthe familymembers bringtoemergency care.25Itisnecessarytocreatestrategiestoallowfamilies tobepresentintheemergencyroom,byconsidering their needs.Thiscanbeachievedbyassigningahealthcareteam membertostayexclusivelywiththefamily,providing sup-porttotheirpsychosocialneeds,which maycontributeto the lack of stressful memories in the future. In addition, thisprofessional---whichcanbeanymemberofthe multi-disciplinary team --- must evaluate the family’s emotional responses to the procedures, anticipating possible inter-ruptions during care.26 However, to create this favorable contextinourculturalreality,firstofallitisnecessaryto recognizethattheBrazilian pediatricemergencysituation differsfromthosedescribedintheinternational scenario,
anditismarkedbyhealthprofessionals’workoverloaddue to the overcrowding of emergency rooms and by limited resources---human,physical,andavailablematerials. More-over, unrestrictedaccesstoemergency servicesresults in longwaitingtimeforusers,whichcausesdistressandstress tothe health team, who performs under a greater work demandthantheyarepreparedtomeet.27,28
Thisstudyhasaslimitationtheexposureofprofessionals’ perceptioninagivenrealityandcontextthatcannotbefully replicatedinotheremergencyscenarios.However,itisan excellenttoolfor futurestudies toestablish strategies to includefamiliesintheemergencyroom.Itisstillnecessary tocarryoutnationalstudiesthatassesstheperceptionsof familiesinthiscontextandthecreationofaprotocolthat willregulate this care practice,adapted toour care and culturalreality.
Finally,the studyconcludes that themedicalstaffand healthcareprofessionalswithlessthan10yearssince gradu-ationaremorefavorabletothepresenceoffamilymembers intheemergencyroomwhencomparedtotheother profes-sionals.Thereasonswhyprofessionalsdonotallow family members to stay in the emergency room are related to discomfortandinsecurity feltby professionalsdue tothe presenceoffamilymembersduringcare.Ontheotherhand, thereasonsthatmakethemallowthepresenceofthe fam-iliesinthisscenarioareoftenassociatedtotheobjectiveof facilitatingtheir ownwork,disregardingthefamilies’real needs.
Funding
Thisstudydidnotreceivefunding.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.JolleyJ,Shields L. Theevolutionoffamily-centeredcare.J PediatrNurs.2009;24:164---70.
2.Cruz AC, Angelo M. Cuidado centrado na família em pedi-atria: redefinindo os relacionamentos. Cienc Cuid Saude. 2011;10:861---5.
3.InstituteforFamily-CenteredCare.Advancingthepracticeof patientandfamilycenteredcare:howtogetstarted.Available from:http://www.ipfcc.org/pdf/gettingstarted.pdf[accessed 20.11.14].
4.Mc Alvin SS,Carew-LyonsA. Family presence during resusci-tation and invasive procedures in pediatric critical care: a systematicreview.AmJCritCare.2014;23:477---85.
5.AmericanHeartAssociation.Part2:Ethicalissues.Circulation. 2005;112:IV6---11.
6.Egging D, Crowley M, Arruda T, et al. Emergency nursing resource: family presence during invasive procedures and resuscitation in the emergency department. J Emerg Nurs. 2011;37:469---73.
7.NishisakiA,DiekemaDS.Mindthegapandnarrowingit:family presence during pediatric resuscitation and invasive proce-dures.Resuscitation.2011;82:655---6.
9.McCullaghP,NelderJA.Generalizedlinearmodels.2nded.New York:ChapmanandHall;1989.
10.FlickU.Introduc¸ãoàpesquisaqualitativa.3rded.PortoAlegre: Artmed;2009.
11.VavaroutaA,XanthosT,PapadimitriouL,etal.Familypresence duringresuscitationandinvasiveprocedures:physicians’and nurses’attitudesworkinginpediatricdepartmentsinGreece. Resuscitation.2011;82:731---6.
12.Fulbrook P, LatourJM, Albarran JW. Paediatric critical care nurses’attitudesandexperiencesofparentalpresenceduring cardiopulmonaryresuscitation: aEuropeansurvey. IntJNurs Stud.2007;44:1238---49.
13.Sacchetti A, CarracioC, Leva E, et al. Acceptance of fam-ily member presence during pediatric resuscitations in the emergencydepartment:effectsofpersonalexperience.Pediatr EmergCare.2000;16:85---7.
14.Duran CR, Oman KS, Abel JJ, et al. Attitudes toward and beliefs about family presence: a survey of healthcare providers, patients’ families,and patients. Am J Crit Care. 2007;16:270---82.
15.MangurtenJ,ScottSH,GuzettaCE,etal.Effectsoffamily pres-enceduringresuscitationandinvasiveproceduresinapediatric emergencydepartment.JEmergNurs.2006;32:225---33.
16.WacthO,DopeltK,SnirV,etal.Attitudesofemergency depart-mentstafftowardfamilypresenceduringresuscitation.IsrMed AssocJ.2010;12:366---70.
17.Beckman AW, SloanBK, Moore GP, et al. Should parents be presentduringemergencydepartmentproceduresonchildren, and who should make that decision? A survey of emer-gencyphysicianandnurseattitudes.AcadEmergMed.2002;9: 154---8.
18.Egemen A, Ikizo˘glu T, Karapnar B, et al. Parental pres-ence during invasiveprocedures and resuscitation: attitudes
of health care professionals in Turkey. Pediatr Emerg Care. 2006;22:230---4.
19.MillerJH, StilesA. Familypresence duringresuscitationand invasiveprocedures:thenurse experience.Qual Health Res. 2009;19:1431---42.
20.GonzálezGS, Tomás RJ, Etxaniz JS. Family presence during pediatricemergencyprocedures:theperspectivesoffamilyand medicalstaff.Emergencias.2010;22:175---80.
21.Duran CR, Oman KS, Abel JJ, et al. Attitudes toward and beliefs about family presence: a survey of healthcare providers, patients’ families, and patients. Am J Crit Care. 2005;16:270---82.
22.Henneman EA, Cardin S. Family-centered critical care: a practical approach to making it happen. Crit Care Nurse. 2002;22:12---9.
23.PorterJ,Dip G,CooperSJ,et al.Attitudes,implementation andpracticeoffamilypresenceduringresuscitation(FPDR):a quantitativeliteraturereview.IntEmergNurs.2013;21:26---34.
24.MaxtonFJC.ParentalpresenceduringresuscitationinthePICU: theparents’experience.Sharingand survivingthe resuscita-tion:aphenomelogicalstudy.JClinNurs.2008;17:3168---76.
25.FerreiraCAG,BalbinoFS, Balieiro MMFG,etal. Presenc¸a da famíliadurantereanimac¸ãocardiopulmonareprocedimentos invasivosemcrianc¸as.RevPaulPediatr.2014;32:107---13.
26.Kingsnorth J, O‘Connel K, Guzetta CE, et al. Family pres-enceduringtrauma activationsand medicalresuscitationsin apediatricemergencydepartmentanevidence-basedpractice project.JEmergNurs.2010;36:115---21.
27.FelicianoKVO,KovacsMH,SarinhoSW.Sentimentosde profis-sionais dos servic¸os de pronto-socorro pediátrico: reflexões sobreoburnout.RevBrasSaudeMaternInfant.2005;5:319---28.