SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Rheumatic
hand’s
clinical,
functional
and
imagiological
correlations
following
metacarpophalangeal
joint
silicone
arthroplasty
夽
Sergio
Figueiredo
a,∗,
Ana
Daniela
Pereira
a,
Marta
Santos
Silva
b,
Luciana
Leite
b,
Grac¸a
Costa
b,
Cesar
Silva
baDepartmentofOrthopaedicsII,CentroHospitalardeLeiria,Leiria,Portugal bDepartmentofOrthopaedics,CentroHospitalardoPorto,Oporto,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:Received21December2016 Accepted17February2017 Availableonline30March2017
Keywords: Arthritis,Rheumatoid Arthroplasty Metacarpophalangealjoint Handstrength Silicones
a
b
s
t
r
a
c
t
Objective:Evaluation ofrheumatoidhand-associatedmetacarpophalangealjointsilicone arthroplastymostoftenreliesonfunctionalscoresalone.Thisstudyaimedtounderstand thecorrelationbetweenperceivedandobservedfunction,strength,andalignment. Methods:Cross-sectionalstudyincludingall11women(15hands)submittedtosecondto fifthmetacarpophalangealjointarthroplastyduetorheumatoidarthritisinvolvementfora timeperiodofsevenyears.MeasurementsreliedontheMichiganHandOutcomes Ques-tionnaire,LafayettePurduePegboard,pinchandgripstrength, andanalysisofa lateral “OK-sign”X-rayview.CorrelationanalysisusedSpearman’scoefficient,assumingstatistical significanceforp-values<0.05.
Results:Objectivefunctionwasstronglycorrelatedwithallothervariables(p<0.05),while perceivedfunction failed to correlate with articular alignment in both measurements (p=0.240andp=0.354).Strengthandalignmentwerealsostronglycorrelated(p<0.05). Conclusions:Most measurements stronglycorrelate with eachother, with emphasis on objectivedexteritymeasurement.
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽WorkperformedattheDepartmentofOrthopaedics,CentroHospitalardoPorto,Oporto,Portugal. ∗ Correspondingauthor.
E-mail:sergio.figueiredo@gmail.com(S.Figueiredo). https://doi.org/10.1016/j.rboe.2017.03.012
2255-4971/©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Thisisanopenaccessarticle undertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Correlac¸ões
clínicas,
funcionais
e
imagiológicas
após
artroplastia
da
articulac¸a˜o
metacarpofalangiana
com
implante
de
silicone
na
mão
reumatóide
Palavras-chave: Artritereumatoide Artroplastia Articulac¸ão metacarpofalangiana Forc¸adamão Siliconesr
e
s
u
m
o
Objetivo: Na maioria dasvezes, a avaliac¸ão da artroplastiada articulac¸a˜o metacarpo-falangeanacomimplantedesiliconeéfeitaapenaspormeiodeescoresfuncionais.Este estudotevecomoobjetivocompreenderacorrelac¸ãoentrefunc¸ão,forc¸aealinhamento percebidoseobservados.
Métodos: Esteestudotransversalincluiutodasas11mulheres(15mãos)queforam sub-metidasaartroplastiametacarpofalangeananosegundoaoquintodedodevidoaartrite reumatoideemumperíododeseteanos.Asmedic¸õesbasearam-senoMichiganHand Out-comesQuestionnaire,noLafayettePurduePegboardenasforc¸asdepinc¸aepreensão,além daanálisederadiografiadamãoemleque.OcoeficientedeSpearmanfoiusadoparaavaliar acorrelac¸ão;valoresdep<0,05foramconsideradosestatisticamentesignificantes. Resultados: A func¸ãoobjetivafoifortementecorrelacionadaa todasasoutrasvariáveis (p<0,05).Poroutrolado,afunc¸ãopercebidanãofoicorrelacionadaaoalinhamentoarticular emambasasmedic¸ões(p=0,240ep=0,354).Aforc¸aeoalinhamentotambémestiveram fortementecorrelacionados(p<0,05).
Conclusões: Amaioriadasmedic¸õessecorrelacionoufortementeentresi,comênfasena medic¸ãoobjetivadadestreza.
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Rheumatoidarthritis(RA),achronic,systemic,Tcell-driven autoimmunedisease,iswidelyknownforitsrepercussions inthehand,particularlyinthe middle-agedwoman.1 Early and severeinvolvementofthe metacarpophalangeal (MCP) andinterphalangealjointsleadstothenearlypathognomonic handdeformitycomposedbysubluxationoftheformerand ulnar deviation ofthe fingers.2 Afterinitial efforts in con-trolling the disease through a conservative approach, late stagesofthediseasefrequentlyrequiresurgicalintervention inordertorestorehandalignment.SiliconeMCParthroplasty (SMPA),popularizedbySwansonnearly50 yearsago,relies onthereactiveencapsulation oftheprosthesis.3 By raising the MCP joint arc of motion, it aims to improve function andaesthetics,whileattainingpainrelief.4,5 Arcofmotion measurementshavealreadyproventhemselvesasareliable method toapproach patient satisfaction. However, despite thisandotherobjectivetechniques,postoperativeevaluation mostoftenreliesonperceivedfunctionscoring,notablyusing MichiganHandOutcomes’Questionnaire(MHQ), aswell as pinchandgripstrengths.5Radiologicalfingeralignment,asan example,hasbeenscarcelyused.5Toourknowledge,however, objectivehanddexterityhasnotsofarbeenevaluatedforthe post-operativerheumatoidhand.Thegoalofourstudywasto determinetherelevanceofhanddexteritymeasurementasan objectiveapproachtoevaluatepostoperativeresultsofSMPA.
Materials
and
methods
Weperformedacross-sectionalstudyincludingall11patients submittedto2ndto5thMCPjointsiliconearthroplastyusing
theNeuflexMCPprosthesis(DepuySynthes,Warsaw,IN,USA) due to local involvementof rheumatoid arthritis, between July 1st, 2008 and June 30th, 2015. This gave us a conve-niencesampleof15hands,fourofwhichwerenon-dominant. All patientswerewomen,withamedianageof67.0 years-old (interquartilerange:12.63)andafollow-uptimeof30.0 months(interquartilerange:32.43).Perceivedhandfunction was evaluatedbyMHQ, withoutmedicalsurveillance, with strict helponlyin situations ofdoubt, aimingforlowering answering bias. MHQ comprises 37 outcome questions for eachhand,onitsfunction,itsinfluenceondailyroutineand work,relatedpain,aestheticsandpatientsatisfaction, scor-ingfrom0to100.Objectivefunctionmeasurementreliedon Purdue Pegboard’s test(Lafayette InstrumentCo, Lafayette, IN,USA),inanadaptationoftwoofitsfour designed exer-cises.Afteranadaptationtryout,patientsperformedthefirst exercise,modifiedfromtheoriginal,inwhichthemeasured hand was the one already submitted to surgery, consist-ing ofsequential pin placement in a predefined board for a time periodof 30s (in the original form, bothdominant andnondominanthandsaremeasuredforthefirstand sec-ondexercises).Eachpincorrectlyplacedcountedasapoint. The second exerciseconsisted on a60-s runin which the patienthadtoassembleapin-washer-collar-washerstructure inasequentialmanner,usingbothhands.Eachpieceapplied countedasapoint.Tip-pinchandgripstrengths,measured inkilograms-force,weregatheredcalculatingthemeanof 5-tryoutmeasurements,usingaJamar hydraulicpinchgauge andaJamarhydraulichanddynamometer(Lafayette Instru-mentCo, Lafayette,IN,USA).Lastly,dexterity-relatedfinger alignmentwasmeasured onalateral “OK-sign”X-rayview, consistingontheangleformedbythedistalphalanxofboth thethumbandtheindexfinger(D1–2␣),aswellastheindex
Fig.1–Determinationoftheangleformedbythedistal phalanxofboththethumbandtheindexfinger(D1–2␣),in alateral“OKsign”sideX-ray.
formed by the minor over major diameters of the ellipse formedbythefirstandsecondfingers(Figs.1and2).Duetoour smallsamplesize,correlationanalysishadtorelyona non-parametrictest,thusthechoiceforSpearman’scoefficients. Statisticalsignificancewasconsideredwheneverwefounda p-valueunder0.05.AnalysiswasperformedusingIBMSPSS Statisticsv20.0.0(IBMCorporation,Armonk,NY,USA).
Results
Table 1 summarizes the descriptive data. It is noteworthy to mention high interquartile ranges for most measured variables,incompliance withhighlydifferent surgical out-comes.Subjective function,asmeasured byMHQ,revealed statisticallysignificant correlationswithobjective function, asmeasuredbyPP’saffectedhand(rho=0.702;p=0.004)and assembly scores (rho=0.521; p=0.047), and also with tip-pinch strength (rho=0.746; p<0.001). Neither grip strength (rho=0.298; p=0.280) nor X-rayalignment as measured by D1–2␣(rho=−0.323;p=0.240)andminorovermajorelliptical diameterindex(rho=−0.257;p=0.354)foundthesame.Apart fromsubjectivefunction,asmentionedabove,objective func-tionmeasurementinitsassemblyscorealsocorrelatedwith
Fig.2–Determinationoftheindexformedbytheminor(a) overmajor(b)diametersoftheellipseformedbythefirst andsecondfingers,inalateral“OKsign”sideX-ray.
all othervariables inastatisticallysignificantfashion (key-pinchstrength:rho=0.850,p<0.001;gripstrength:rho=0.677, p=0.006;D1–2␣:rho=−0.543,p=0.037;minorovermajor ellip-ticaldiameterindex:rho=−0.619,p=0.014).Theaffectedhand scoresolely correlatedwithkey-pinch strength (rho=0.659; p=0.008),apartwiththeassemblyscore(rho=0.675;p=0.006) andMHQ.Alignment(boththefirst-secondfingerdistal pha-lanxangle andminorover majorellipticaldiameterindex) wasalsostatisticallysignificantlycorrelatedwithbothpinch (rho=−0.798;p<0.001andrho=−0.720;p=0.002,respectively) and grip strengths (rho=−0.798; p<0.001 and rho=−0.720; p=0.002).ThisissummarizedinTable2.
Discussion
SynovitisoftheMCPjointendsupinitsulnardeviationand volarjointsubluxationcausedbychangesinthevolarplate andligamentoussupport.Thisalsoleadstoshorteningofthe intrinsicmusclesand consequentproximalinterphalangeal joint hyperextension, aggravated by long extensor tendon attachmentchangesattheproximalphalanx.4 Allthismay posedifficultiesinhandfunction,mainlyonstrengthand dex-terity,lastlyleadingtoadecreaseinpatient’ssatisfaction.In
Table1–Collectedmeasurementdataregarding perceived(MHQ)andobjective(PP)functions,strength (key-pinchandgrip)andalignment(throughX-ray measurements).
Median P25–P75
A.MichiganHandOutcomes Questionnaire(%) 21.00 48.00 1.Generalscore 41.18 43.64 2.Workscore 25.00 55.00 3.Painscore 25.00 65.00 4.Appearancescore 12.50 32.25
5.Finalquestionsscore 5.17 70.83
B.PurduePegboarddexteritytest(points)
1.Affectedhandscore (30s) 10 6 2.Assemblyscore(60s) 15 10 C.Strength(KgF) 1.Tip-pinch 3.00 1.50 2.Grip 5.00 4.00 D.X-raymeasurements 1.DistalphalanxD1–D2 angle(◦) 91.0 70.8 2.D1–D2ellipse:minor overmajordiameter index
0.55 0.20
awaytosolve it,SMPA hasalready provenitselfeffective, consideringproperlyselected patients.6 Ahigh focus relies onmeetingpatients’expectations,thusrenderingit impor-tanttounderstandwhat,onobjective terms,isunderstood assuch.7 In ourtrial, the existenceofstrongrelationships betweenmostof the measuredvariables stronglysuggests theirvalidityinmeasuringsuccessfollowingSMPA.Thisisnot surprisingconsideringhandfunctiondependsonitsstrength andproperjointalignment.Whatendsupassurpriseisthe majorutilityofhanddexteritymeasurementswhencompared withMHQ.Itismorerelatableand,therefore,more univer-salandmostlikelylesspronetobias.Whencomparingpre withpostoperativepatientsatisfaction,regardingSMPA,ithas alreadybeenfoundthatitisnotdirectlyrelatedwithpinch andgripstrengthbut rathertoimprovementsinalignment andarc ofmotion.3,5,7 Postoperativesatisfaction perse,on anygivenmoment,wasnotyetanalyzed,toourknowledge.
As a surrogatemeasurement, arc ofmotiondoes notalso directlyreflectfunction,asitdoesnotmeasurethemajor ben-efitscomingoutofit.Handdexteritymeasurements,onthe other hand,arewidelyusedinindustrialand medical pur-poseswithinterestingresults.8Anapparentbenefitcoming outfromregularhandpractice,despiteinfluencesoriginating onhandsizeandage,hasalreadybeenreported.8Asacross sectionalstudy,itislimitedbyreadingsperformedat differ-entfollow-up timesatdifferentages.Althoughnotdirectly affectingtheobservedcorrelationbetweenmeasurements,it hasalready beenobservedthat handfunction, asawhole, declinesovertime,lastlyresultinginimplantfailure.9–11This isofmajorconcernwhendesigningnewimplants,asRAis punishingnotonlyjointsurfacesbutalsocapsularand tendi-nousstructures.Themaingoalistoallowforencapsulation, inordertoreachstability,atthesametimeproperalignment andfunctionareachieved.Siliconeimplantsrelytheir move-mentonacentralhinge,whichcannotbeeithertoothin,for resistancepurposes,nortoothick,forflexibilitypurposes.12,13 Theimplantitselfisnotdesignedtoaspecificpatientleading tovariableresults,withcomplicationratesvaryingfromstudy tostudy,withoursinbetween.11,13,14Asstrengthseemsnot tobeofmajorconcerninregardsofperceivedand objecti-fiedfunction,andalthoughnoneofourpatientshadfailed implants or was submitted to revision surgery, it may be of interest to design prosthesis better related to durabil-ity,althoughfailedimplantsseemnottobecorrelatedwith patientsatisfaction.5,9,14 Assemblyscoresondexterity mea-surementrequiresbothhands,whichmayposebiasedresults assomepatientsweresubmittedtobilateralsurgerieswhile themajoritywasnot.Anyhow,thisdidnotdisturb correla-tionanalysis,possiblybecausetheirdiseasewasalreadymore severeinregardsofjointinvolvement.Thesmallsamplesize isrelatedtothereasonablysmallpopulationundergoing com-pletesecondtofifthSMPAinourinstitution,possiblydueto theincreasingsuccessofnon-surgicalapproacheswhen deal-ingwithRA.Wealsofailedinnotdirectlysurveyingforpain, eitheritbeingconstantorrecurrent,relyingontheMHQalone, althoughitcouldcomeasamajorindependentfactor relat-ing topatients’satisfaction.15 All added,and comparingto what’sbeendiscoveredsofarinregardsofsurgicalsuccess, ourstudyisimportantinsuggestingdexteritytestsasmajor playersinmeasuringobjectivefunction.5Thismaybefuturely
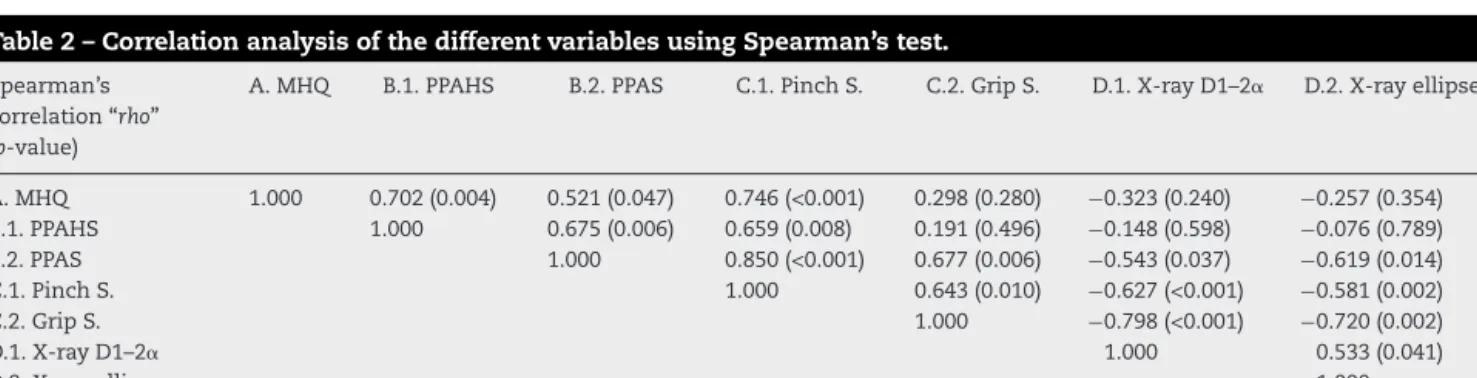
Table2–CorrelationanalysisofthedifferentvariablesusingSpearman’stest.
Spearman’s correlation“rho” (p-value)
A.MHQ B.1.PPAHS B.2.PPAS C.1.PinchS. C.2.GripS. D.1.X-rayD1–2␣ D.2.X-rayellipse
A.MHQ 1.000 0.702(0.004) 0.521(0.047) 0.746(<0.001) 0.298(0.280) −0.323(0.240) −0.257(0.354) B.1.PPAHS 1.000 0.675(0.006) 0.659(0.008) 0.191(0.496) −0.148(0.598) −0.076(0.789) B.2.PPAS 1.000 0.850(<0.001) 0.677(0.006) −0.543(0.037) −0.619(0.014) C.1.PinchS. 1.000 0.643(0.010) −0.627(<0.001) −0.581(0.002) C.2.GripS. 1.000 −0.798(<0.001) −0.720(0.002) D.1.X-rayD1–2␣ 1.000 0.533(0.041) D.2.X-rayellipse 1.000
MHQ,MichiganHandOutcomesQuestionnaire,totalscore;PPAHS,PurduePegboard’stestaffectedhandscore;PPAS,PurduePegboard’stest assemblyscore;PinchS.,keypinchstrength;GripS.,gripstrength;X-rayD1–2␣,Thumb-indexfingerdistalphalanx“OK-sign”sideangle;X-ray ellipse,indexofminorovermajorellipticaldiameterformedbythe“OK-sign”.
testedinapretopostoperativeanalysis,inordertoimprove bothimplantsandtechniquesrelatedtotherheumatoidhand. Obviouslysuchshouldbealwayscorrelatedwithqualityoflife assessmentsurveys,astheremaybealimitinwhichfunction doesnotnecessarilyresultingeneralpatientsatisfaction.16,17
Conclusions
Summarizing,hand dexterity as measured by Purdue Peg-board’s test offers a relatable and reliable approach to objectivelymeasurethe outcomeofpatientswith rheuma-toidhandsubmittedtoSMPA.Alignmentandstrength also correlatedstrongly,thuspointingouttherelevanceofproper arthroplastypositioningduringtheprocedure.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. GibofskyA.Overviewofepidemiology,pathophysiology,and diagnosisofrheumatoidarthritis.AmJManagCare. 2012;18(13):S295–302.
2. McMasterM.Thenaturalhistoryoftherheumatoid metacarpo-phalangealjoint.JBoneJointSurgBr. 1972;54(4):687–97.
3. SwansonAB.Flexibleimplantarthroplastyforarthriticfinger joints:rationale,technique,andresultsoftreatment.JBone JointSurgAm.1972;54(3):435–55.
4. LongoUG,PetrilloS,DenaroV.Currentconceptsinthe managementofrheumatoidhand.IntJRheumatol.
2015;2015:648073,http://dx.doi.org/10.1155/2015/648073[Epub 2015Jul8].
5. WaljeeJF,ChungKC.Objectivefunctionaloutcomesand patientsatisfactionaftersiliconemetacarpophalangeal
arthroplastyforrheumatoidarthritis.JHandSurgAm. 2012;37(1):47–54.
6.StirratCR.Metacarpophalangealjointsinrheumatoid arthritisofthehand.HandClin.1996;12(3):515–29. 7.AbboudJA,BeredjiklianPK,BozentkaDJ.
Metacarpophalangealjointarthroplastyinrheumatoid arthritis.JAmAcadOrthopSurg.2003;11(3):184–91. 8.FigueiredoS,MachadoL,PereiraAD,CasteloL,FardilhaML,
SaA.Physiciansversussurgeons.Apilotstudyonhand dexteritywithinacontrolledpopulation.ActaOrthopBelg. 2016;82(3):456–61.
9.BassRL,SternPJ,NairusJG.Highimplantfractureincidence withSuttersiliconemetacarpophalangealjointarthroplasty.J HandSurgAm.1996;21(5):813–8.
10.GoldfarbCA,SternPJ.Metacarpophalangealjointarthroplasty inrheumatoidarthritis.Along-termassessment.JBoneJoint SurgAm.2003;85(10):1869–78.
11.BurgessSD,KonoM,SternPJ.Resultsofrevision
metacarpophalangealjointsurgeryinrheumatoidpatients followingprevioussiliconearthroplasty.JHandSurgAm. 2007;32(10):1506–12.
12.FlattAE,FischerGW.Biomechanicalfactorsinthe replacementofrheumatoidfingerjoints.AnnRheumDis. 1969;28Suppl.(5):36–41.
13.FoliartDE.Swansonsiliconefingerjointimplants:areviewof theliteratureregardinglong-termcomplications.JHandSurg Am.1990;20(3):445–9.
14.SousaJM,OliveiraF,ClaroR,CardosoP,TrigueirosM,SilvaC. Mãoreumatoide:revisãode124PrótesesMCFdeSilicone.Rev IberoamCirMano.2010;38(1):47–52.
15.BeckenbaughRD,DobynsJH,LinscheidRL,BryanRS.Review andanalysisofsilicone-rubbermetacarpophalangeal implants.JBoneJointSurgAm.1976;58(4):483–7.
16.BirkmeyerJD,DimickJB,BirkmeyerNJ.Measuringthequality ofsurgicalcare:structure,process,oroutcomes?JAmColl Surg.2004;198(4):626–32.
17.StaigerDO,DimickJB,BaserO,FanZ,BirkmeyerJD. Empiricallyderivedcompositemeasuresofsurgical performance.MedCare.2009;47(2):226–33.