w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Review
Article
Management
of
ulcerative
colitis:
a
clinical
update
Fabio
Vieira
Teixeira
a,b,∗,
Rogerio
Saad
Hosne
c,
Carlos
Walter
Sobrado
d aUniversidadeEstadualPaulista(UNESP),SãoPaulo,SP,BrazilbClínicaGastrosaúdedeMarília,Marília,SP,Brazil
cDepartmentofSurgeryandOrthopedics,UniversidadeEstadualPaulista(UNESP),SãoPaulo,SP,Brazil
dDisciplineofColoproctology,HospitaldasClínicas,UniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received8July2015 Accepted15August2015
Availableonline26September2015
Keywords:
Ulcerativecolitis Acutecolitis Clinicaltreatment Surgery
Complications
a
b
s
t
r
a
c
t
Theobjectiveofthisstudywastoevaluatetheconsensusofexpertsocietiesandpublished guidelinesonthemanagementofulcerativecolitis,andtocomparewiththeexperienceof theauthors,inordertostandardizeproceduresthatwouldhelpthereasoningand decision-makingprocessofthephysician.Asearchwasperformedinscientificliterature,specifically inelectronicdatabases:Medline/Pubmed,SciELO,EMBASEandCochrane,andthefollowing descriptorswereused:ulcerativecolitis,acutecolitis,clinicaltreatment,surgeryand ran-domizedtrial.Itcanbeconcludedthatthegoalsoftherapyinulcerativecolitisareclinical andendoscopicremission,deep,sustainedremissionwithoutcorticosteroids,prevention ofhospitalizations andsurgeries,andimprovedqualityoflife.Thesurgical indications arereservedforselectedcases,rangingfrommedicalintractability,complications(severe refractoryacutecolitis,toxicmegacolon,perforationandhemorrhage) andmalignancy. Informationinthisreviewarticlemustbesubmittedtoevaluationandcriticismofthe spe-cialistresponsiblefortheconducttobefollowed,inthefaceofhis/herrealityandtheclinical statusofeachpatient.
ThedegreeofrecommendationandstrengthofevidencewerebasedusingtheGRADE sys-tem(TheGradesofRecommendation,Assessment,Development,andEvaluation)described below:
1.A:Experimentalorobservationalstudiesofhigherconsistency. 2.B:Experimentalorobservationalstudiesoflowerconsistency. 3.C:Casereports(non-controlledstudies).
4.D:Opinionwithoutcriticalevaluation,basedonconsensus,physiologicalstudiesor animalmodels.
©2015SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](F.V.Teixeira). http://dx.doi.org/10.1016/j.jcol.2015.08.006
Tratamento
da
retocolite
ulcerativa:
atualizac¸ão
clínica
Palavras-chave:
Coliteulcerativa Coliteaguda Tratamentoclínico Cirurgia
Complicac¸ões
r
e
s
u
m
o
Oobjetivodestetrabalhofoiavaliarosconsensosdesociedadesdeespecialistase guide-linespublicadossobreomanejodaretocoliteulcerativa,econfrontarcomaexperiência dosautores,afimdepadronizarcondutasqueauxiliemoraciocínioeatomadadedecisão domédico.Foirealizadabuscanaliteraturacientífica, maisprecisamentenasbasesde dadoseletrônicos:Medline/Pubmed,SciELO,EMBASEeCochrane,tendosidoutilizadoos descritores:ulcerativecolitis,acutecolitis,clinicaltreatment,surgeryerandomizedtrial. Pode-seconcluirqueosobjetivosdaterapianaretocoliteulcerativasão:remissãoclínicae endoscópica,aremissãoprofundasustentadasemcorticosteróides,evitarhospitalizac¸ões ecirurgias,emelhoranaqualidadedevida.Asindicac¸õescirúrgicasficamreservadaspara casosselecionadosquevariamdeintratabilidadeclínica,complicac¸ões(Coliteagudagrave refratária,megacólon tóxico,perfurac¸ão e hemorragia)e malignizac¸ão.Asinformac¸ões contidasnesteartigoderevisãodevemsersubmetidasàavaliac¸ãoeàcríticadomédico especialista,responsávelpelacondutaaserseguida,frenteàsuarealidadeeaoestado clínicodecadapaciente.
Ograuderecomendac¸ã˜oeforc¸¸adeevidênciaforambaseadosusandooGRADEsystem (TheGradesofRecomendation,Assessment,Development,andEvaluation),descritoabaixo:
A:Estudosexperimentaisouobservacionaisdemelhorconsistência. B:Estudosexperimentaisouobservacionaisdemenorconsistência. C:Relatosdecasos(estudosnãocontrolados).
D:Opiniãodesprovidadeavaliac¸ãocrítica,baseadaemconsensos,estudosfisiológicos oumodelosanimais.
©2015SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
and
epidemiology
Nonspecificulcerativerectocolitis(NURC)isachronic inflam-matory bowel disease (IBD) with a not fully understood etiologythatmanifestsitselfpreferablyinyoungpeopleand whosemainsymptomsare amucousand bloodydiarrhea, withorwithoutabdominalpain(A).
Itssymptomsdependon the extentand severityofthe disease;whenlimitedtotherectum(proctitis),NURCtends toexhibitintensemucorrhea,tenesmus,fecalincontinence anddefecationurgency.Inseverecasesofcolitis,other asso-ciatedsymptomssuchasvomiting,fever,anorexia,bloating andabdominaldistensioncanemerge.
Thediseasetendstobeginintherectumandthenextends cranially,affectinguniformlyandalsocontinuouslythe prox-imalsegments,presentingadistalgradient.
Inrecentdecades,anexponentialincreaseinIBDhasbeen describedworldwide.There isevidencethatthesediseases have a direct relationship with industrial progress, which wouldjustify its increasingincidenceinsomecountries in recent decades,evenin those hitherto classified asoflow frequency(B).
ThereiswidevariationbetweentheincidenceratesofIBD. InEurope,incidenceratesrangefrom4.1/100,000(Romania) to81.5/100,000(FaroesIslands).1Withregardtoulcerative
col-itis,onerecentsystematicreviewestimatedthattheincidence inEuroperangedfrom0.4to24.3newcasesdiagnosedper 100,000inhabitants(A).2InAsiaandtheMiddleEast,onthe
otherhand,theincidencewaslower:0.1–6.3/100,000.2Onthe
otherhand,inNorthAmericatheincidenceofNURChad inter-mediaterates,rangingfrom0to19.2/100,000population.3
AstheprevalenceofNURC,themostrecentdataavailable intheliteraturearefromapopulation-basedstudypublished at the beginning of 2014that showed a slight increase in Scandinavia (C).4 Currentlythere are about 61,000patients
diagnosedwithIBDinSweden,andmostpatientsare carri-ersofNURC,withaprevalenceof0.35%(95%CI:0.34–0.35).5
IthasalsobeenobservedthattheprevalenceofIBDishigher incountriesofthenorthernhemisphere,thatis,thosecloser totheArctic.6InFinlandtheprevalenceofNURCwashigher
inOuluandTampere,citieslocatedfurthernorth,compared toHelsinki,acitylocatedfurthersouthinthatScandinavian country(C).7
InBrazil,anepidemiologicalstudyconductedbythe Botu-catuMedicalSchoolevaluatedtheincidenceandprevalence ofIBDinamicro-regionofSãoPaulostate.Duringtheperiod from1986to2005,anincreaseinincidencewasobservedover thistime,butwithlowervalueswhenincidencerateswere comparedworldwide,thatis,theincidencerateinthisregion islow,matchingLatinAmericaandsouthernEuropecountries (C).8Itisnoteworthythatitsincidencehasaninverserelation
withsmoking.
Signs
and
symptoms
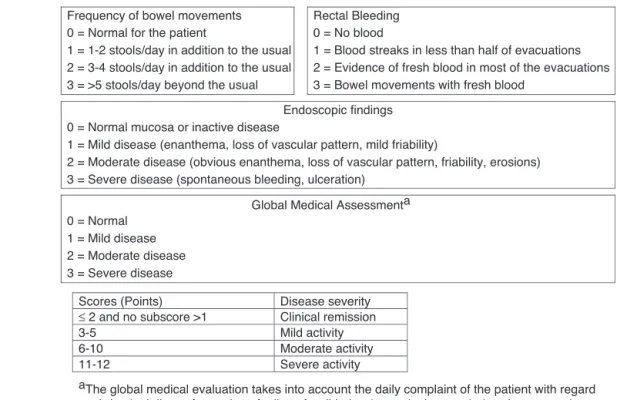
Disease severity Scores (Points)
Clinical remission
≤ 2 and no subscore >1
Mild activity 3-5
Moderate activity 6-10
Severe activity 11-12
aThe global medical evaluation takes into account the daily complaint of the patient with regard to abdominal discomfort, pain, a feeling of well-being (normal, above or below the average), physical examination findings and the patient’s performance of daily activities.
Frequency of bowel movements Rectal Bleeding 0 = No blood 0 = Normal for the patient
1 = 1-2 stools/day in addition to the usual 2 = 3-4 stools/day in addition to the usual
3 = Bowel movements with fresh blood
2 = Evidence of fresh blood in most of the evacuations 1 = Blood streaks in less than half of evacuations
3 = >5 stools/day beyond the usual
Endoscopic findings 0 = Normal mucosa or inactive disease
1 = Mild disease (enanthema, loss of vascular pattern, mild friability)
2 = Moderate disease (obvious enanthema, loss of vascular pattern, friability, erosions) 3 = Severe disease (spontaneous bleeding, ulceration)
Global Medical Assessmenta 0 = Normal
1 = Mild disease 2 = Moderate disease 3 = Severe disease
Fig.1–MayoClinicScore:severityindexofulcerativecolitis.
systemicinvolvement.Thediseasecanbelimitedtothe rec-tum(proctitis);caninvolvetheleftsemicolon(leftcolitis)or oftenextendsthroughoutthecolon(pancolitis).
Thus,thesignsandsymptomsvaryaccordingtotheextent andintensityoftheinflammatoryprocess,althoughthereis notalwaysproportionalitybetweentheextentofdiseaseand severityofsymptoms(A).
Theclinicalpictureconsistsofepisodesofdiarrheaof mod-eratetosevere intensity,mostoften accompaniedbyfresh bloodand/ormucus,usuallyprecededbyabdominalcramps, andwithreliefafterdefecation.Thisincreaseinbowelrhythm canoccurduringthedayoratnight.Othersymptomsmaybe present,suchasanorexia,fever,asthenia,defecationurgency, flatulence,andtenesmus;theseverityofdiarrheatendsto cor-relatewiththeextentandseverityofcolonicinflammation(A). Theabdominalpainvariesaccording totheintensity of inflammation,beinggenerallyofmildtomoderatetype,but maybecomesevereincomplicationssuchasfulminantcolitis andtoxicmegacolon.
Extra-intestinalconditionsmaybepresent,suchasjoint, dermatological,ophthalmologic, hepatobiliaryand hemato-logicmanifestations that may precede or appear afterthe intestinalevent.
Classificationofseverity
Thediseasecanbeclassifiedaccordingtotheclinicalpicture, inassociation with laboratory and endoscopic parameters. In the 1960s, a study published by University of Oxford (UK)investigators,producedtheTruelove-Wittsclassification (1955).9 However,the English classification didnot include
criticalparameters toassessthe severityofthe disease,as
wellasendoscopicfindingsandthegeneralconditionofthe patient.In1987,theMayoClinicgroupinRochester,Minnesota (USA),10publishedaclassificationthathasbecomethemost
widelyusedintheliterature,bothinclinicalpracticeandin mostofthetrialsinvolvingpatientswithNURC(Fig.1).The diseasecanbeclassifiedasmild,moderateorsevere,and2/3 ofpatientsexhibitamild-to-moderatepicture(A).10The
treat-mentisbasedontheintensityandextentoftheinflammatory process.
Diagnosis
There is no single test that can be considered the “gold standard”forthediagnosisofNURC.Thediagnosisofthis con-ditionisbasedondatafromtheclinicalhistoryandphysical examination, together with laboratory tests and radiologi-cal,endoscopicandhistologicalstudies.Themaintestsare colonoscopy,pathology,serumandfecalbiochemicaltestsand radiologicalstudies(D).11
Colonoscopy
Unlike Crohn’sdisease,NURC ischaracterizedbya diffuse mucosalandsubmucosalinflammationlimitedtothecolon andrectum.Afewpatientsmayexperienceaninflammation of5–10cmfromterminalileumthatwasreferredtoasreflux ileitisor“backwashileitis”;thereiscontroversyastowhether thisfindingisrelatedornotwithdiseaseseverity.
withactiveNURC,onecanobserveacontinuousanddiffuse inflammatoryprocesswithedema,congestion,friabilityand granularityofthemucosa,andmicroulcerationsthatmayor maynotbecoveredbyfibrin.In95%ofthetime,therectum iscompromisedbythe inflammatoryprocess;onthe other hand,rarelytheterminalileumwillbeaffected(5%).Another frequentendoscopicfindingistheinflammationgradient,in whichamoreintenseinvolvementintherectumandamilder involvementinproximalsegmentsareobserved.
Inaddition, the histologicalevaluation iscritical tothe diagnosisofthisdisease,instagingproceduresthedegreeof inflammation,inthefollow-upafterthebeginningof treat-ment,andeventoexcludedysplasiaandcancerassociatedto NURC(B).11,12
Itisoftheutmostimportanceagoodintegrationbetween thesurgeon,endoscopistandpathologisttoimprove diagnos-ticaccuracy(A).11
Complementarytests
Sometestsmayhelpinassessingtheseverityof inflamma-tion.SerumlevelsofC-reactiveprotein(CRP)anderythrocyte sedimentationrate(ESR)areusefultestsintheevaluationof theinflammatoryprocess,butthesearenotspecificandmust beanalyzedinconjunctionwithother clinical,endoscopic, radiologicalandhistopathologicaldata(B).11–13
SomeserologicalmarkersaspANCAandASCA,although notspecific, can predict years ahead(in case ofapositive result)ifthepatientwilldevelopinflammatoryboweldisease; thesemarkersarealsovaluableindifferentiatingcolitisand Crohn’sdisease.ThereisalsoevidencethatpANCA-positive NURCpatients are ata higher risk of being colectomized, whichmayreflectgreaterdiseaseseverity(B).11–13
Fecalcalprotectinisanewlyaddedtesttotheclinical arma-mentarium;this isaverysensitivetestforthediagnosisof bowelinflammation,althoughwithlittlespecificity.Fecal cal-protectinreflectsthepresenceofinflammation,andthereis adirectcorrelationoftheirliveswiththeseverityandofthe extenttheinflammatoryprocess.
Thus,thistestisveryusefulinmonitoringtheresponse totreatment,aswellasinthediagnosis ofrelapses. Nega-tivelevelsshouldnotbeinterpretedasalackofbowelorganic pathology,butastheabsenceofaninflammationcausedby neutrophils(B).13,14
Inpatients treated withbiological agents and benefited withgoodclinicalandendoscopicresponse,asharpdropin fecalcalprotectinlevelisobserved,whichshowsgood correla-tionwiththemucosalhealingprocess.11,14Itcanbeconcluded
that theclinical disease activity index, in association with serumandfecalmarkers,increasestheaccuracyin determin-ingandpredictingtheacutizationstageofthediseaseandto monitortheresponsetotreatment.11,12
Treatment
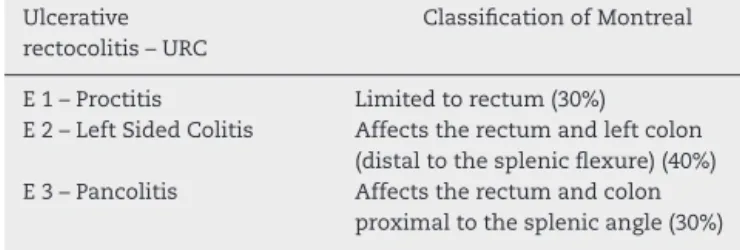
Thetreatmentofulcerativecolitisisbasedonseverity,activity, locationandextentofthedisease.Consideringthatin gen-eralNURCinvolvesmoredistalsegmentsofthelargebowel (rectumandsigmoid),thisdiseasecanbeclassified,according toitslocation,into3groups(MontrealClassification,Table1).
Table1–ClassificationofMontreal(2006)–accordingto URClocation.
Ulcerative rectocolitis–URC
ClassificationofMontreal
E1–Proctitis Limitedtorectum(30%) E2–LeftSidedColitis Affectstherectumandleftcolon
(distaltothesplenicflexure)(40%) E3–Pancolitis Affectstherectumandcolon
proximaltothesplenicangle(30%)
Astotheseverityofthedisease,itcanbeconsideredmild, moderateorsevere,basedontheaforementionedcriteria.It isnoteworthythatthevastmajorityofpatientsexperience mild-to-moderateillness(85%)andtherestpresentswiththe severeform(15%).15–17
ThemaingoalsofNURCmanagementareclinical remis-sion of active disease, remission maintenance without corticosteroids, prevention ofcomplications, and improve-ment of the quality of life. However, since the advent of the management with biological agents (and in line with themanagementofCrohn’sdisease),thehealingprocessof the inflamed intestinalmucosamust beanobjective tobe pursued,sincethereisevidencethataneffectivecontrolof inflammationisassociatedwithadecreaseinratesof recur-renceofthedisease,reducingtheneedforhospitalizationand eveninthenumberofcolectomyindications(B).17
Table2liststhemaindrugs,routesofadministration,and dosages.
ThetreatmentofNURCisbasedontheextentandactivity ofthedisease.17,18
Proctitis
The first-line therapy for active colitis limited to the rec-tum(proctitis)istopicalmesalazine(A).9Asystematicreview
fromof38clinicaltrialsfromCochranedatabaseon procti-tisandleftcolitismanagementconfirmedthesuperiorityof thistherapyversusplacebofortheinductionofclinical remis-sion,besidesendoscopicandhistologicalimprovement.Ina head-to-headcomparison,topicalmesalazine,isalsobetter thanoralmesalazine,beingmoreeffectivethantopical cor-ticosteroids toachieve clinical,endoscopicand histological remission(A).19,20
Mesalazine1g/dayinsuppositoryistheinitialtreatment formildormoderateproctitis;onealternativeistheuseof mesalazineenema(A).19,20 Inthissense, thesuppositoryis
bettertolerated,itsapplicationiseasierandshowsthe bet-terrectaldistributionofthedrug,withnodifferenceinthe applicationinasingleversusdivideddose.
The combined use of oral and topical mesalazine, or with a topical steroid, may be tried in those cases with noinitialimprovement;thisisthesecondtreatmentoption (A).18–20 Inthestaggeredtherapeuticsequence,ifthe
Table2–Maindrugsusedtotreatulcerativecolitis.
Drug Commercialbrand Presentation Initialdose Maintenancedose
Mesalazine Pentasa Tablets500mg 3g–4g 1g–2g
Sachetsde1gand2g
Mesalazine Pentasa Suppository 1g 500mg
Mesalazine Pentasa Enema1g 1g 1g
Mesalazine Mesacol Tablets400and800mg 2.4–4g 1.6–2.4g
Mesalazine Mesacol Suppository500mg 1g 500mg
Mesalazine MesacolMMX Tablets1.2g 3.6–4.8g 1.2–2.4g
Sulfasalazine Azulfin Tablets500mg 4–5g 2g
Sulfasalazine Azulfin Suppository 1g 500mg
Azathioprine Imuran Tablets50mg 2–2.5mg/kg 2–2.5mg/kg
Infliximab Remicade Ampoules100mg 5mg/kgweightatweeks
0,2and6
5mg/kgevery8weeks
Adalimumab Humira Prefilledsyringe40mg 160mgSCatweeks0
and80mgatweek2
40mgSCevery2weeks
Left
Sided
Colitis
The treatment ofchoice in cases ofmild-to-moderate left
sidedcolitisisacombinationoforalandtopicalmesalazine; thereisevidencethat theconcentration levelsof5-ASA in therectalmucosaaregreaterinthecombinedtherapyversus
monotherapywiththisagent(A).19,20
Thiscombined effect ismore significant when the dis-easeextendsbyatleast50cmabovetheanalmargin,thatis, aproctosigmoiditis.12,13Arecentmeta-analysisshowedthat
mesalazineissuperiortoplaceboininducingand maintain-ingclinicalremissioninpatientswithNURC(numberneeded to treat [NNT]=6). Doses of mesalazine over 2g/day were moreeffectivethandoses<2g/dayinthepreventionofclinical recurrence.19
Furthermore, the ASCEND II study demonstrated that mesalazine4.8g/dayproducedbetterscarringprocess/clinical response rateversus 2.4g/day.21 As toenemas, the
recom-mended dose is1g/day, withno difference between large-orlow-volume enemas,the latterbeing bettertoleratedby patients(A).13,22 Althoughthereiscontroversyamongsome
meta-analyze,theuseofrectalcorticosteroids(enema)seems tobeequivalenttothetopicaluseof5-ASA.22,23 Adherence
totreatmentwithsalicylatesisaserious problemthatcan impactabout40–60%ofpatients.Thereisevidencethatlow adherencetotreatmentregimeisrelatedtoadosingregime higherorequalto3dailydoses(A).13,20
Withthenewformulationsofmesalazine(mesalazinein sachet,orMMX®),patientscantakeahigherdose,andthe result isa smaller number ofdaily doses, thus improving adherencetotreatment.
TheMOTUSstudycomparedtheuseofmesalazine(sachet) 4gtakenintwodosesof2gevery12hversusasingledose of 4g per day. Clinical remission at 8 weeks for patients treated with a single dose ofmesalazine was 52.1% com-paredto41.8%inthosetreatedwithtwodailydoses(p=0.14). Theratesofmucosalhealingandtheimprovementin symp-tomscores(UC-DAI)werestatisticallybetterversusinthose patientstreatedwith2doses/day24(B).
Incasesnotbenefitedwithagoodclinicalresponsewith theuseofsalicylicderivativesafter14–21daysoftreatment,or incasesofdiseaseexacerbation,corticosteroidscanbeadded.
Prednisoneisthecorticosteroidmostoftenused,witha sug-gested dose of 0.75–1mg/kg/day, with a maximumdose of 60mg/day.Prednisoneisasyntheticglucocorticoidof inter-mediatepower,beingconvertedintheliverintoprednisolone, theactiveform.Theaveragedailydoseis40mg/dayfor1–2 weeksor untilthe occurrenceofclinical remission; atthis point,thecorticosteroidmustbereduced(10mg/week,until 5mg/kg/day),whenthedrugwillbegraduallyreduced(5mg eachweek)untilitscompletediscontinuation.23
If,duringthecorticosteroidweaningprocess,thedisease relapses, the dose should be increasedto the penultimate dose preceding that in which the relapse occurred; after-wards, the gradual discontinuation of procedure will be carriedon.Thesalicylicderivativesshouldbemaintainedfor longperiods,inordertominimizethechanceofrelapse.In caseofsteroiddependence (inabilitytoreducethe doseof 20mg/daywithouttheoccurrenceofrelapse)orincasesof refractoriness tocorticosteroids (no response to treatment with prednisone60mg/day after4–6 weeksoftherapy) the physicianshouldsuggesttheuseofimmunomodulators (aza-thioprine,6-mercaptopurine)(A).24
Azathioprine at a dose of 2–2.5mg/kg/day is the main immunomodulator or immunosuppressant used in clinical practice.Azathioprineisasyntheticanalogofpurineandwas developedinthefinalyearsofthe1950s.Thisisapro-drug of6-mercaptopurineandactsbyinhibitingDNAsynthesisin proliferatingcells,forinstance,BandTlymphocytes.25,26
mustbeavoided,aswellasitsfrequentreintroductions. How-ever, the study concludedthat thereis little evidencethat theuseofazathioprine,asamaintenancedrug,issuperior tosalicylates(A).25
Otherimmunomodulatorydrugssuchas 6-mercaptopur-ine(1–1.5mg/kg/day)andmethotrexate(15–25mg/week)can alsobeusedinrefractorycases.Ameta-analysispublished recentlyshowedthatabout2/3ofpatientsrefractoryto aza-thioprinemay benefitfrom theuse of6-mercaptopurine in maintainingremissioninpatientswithNURC(B).26
Pancolitis
or
extensive
colitis
Mild-to-moderatecasesofpancolitisshouldbetreated simi-larlytothetreatmentgiventopatientswithleftcolitis,thatis, withoralmesalazine4–4.8g/dayassociatedwithmesalazine enema1g/day(A).13,17,22
Likewise,ifthesymptomspersistafter14–21daysof treat-ment or if a sustained relief of symptoms has not been achieved after 30–40 days of treatment with mesalazine, one can introduce an induction therapy with oral corti-costeroids (prednisone) at an average dose of 40mg/day (0.75–1mg/kg/day – notexceeding 60mg/day).The mainte-nancetreatmentiscarriedout withmesalazine2–2.4g/day (A).23,24
Patientswithproctitis,leftcolitisormild-to-moderate pan-colitisrefractorytoconventionaltherapywithsalicylatesand immunomodulatorsshouldbetreatedwithbiologicalagents combinedwithazathioprine,orasmonotherapy(B).13,25,27,28
Proctitis,
left
colitis
or
moderate-to-severe
pancolitis
refractory
to
conventional
treatment
Infliximabisachimericmonoclonalantibodyanti-TNF(tumor necrosis factor), being indicated for patients with NURC refractory to conventional therapy. (B) Two randomized, placebo-controlledstudiespublishedin2005,ACT1andACT 2, showed that the use ofinfliximab ata dose of 5mg/kg was superior toplacebo in the treatment of patients with moderate-to-severe ulcerative colitis refractory to conven-tionaltherapywithsalicylatesandazathioprine.28,29
Patients treated with infliximab had a better clinical responseandimprovedclinicalremissionandmucosal heal-ingversuspatientstreatedwithplacebo.Infliximabshouldbe usedintravenously atadose of5mg/kgbody weight, with aninductiondoseatweek0,anotherdose2weeksafterthe first,andathirddose6weeksaftertheinitialdose(Induction therapy:weeks0,2and6).Maintenancetherapymustbe per-formedwithinfusionsevery8weeksatadoseof5mg/kg.28,29
Currently, there is evidence that the use of infliximab incombination withazathioprineissuperiorto monother-apy with infliximab or with azathioprine in patients with moderate-to-severeNURCrefractorytosalicylates, corticoste-roids,andimmunomodulators.30
The SUCESS study revealed that patients treated with infliximabcombinedwithazathioprinehadabetterclinical response,clinicalremissionandamucosalhealingprocess, whencomparedwiththosewhoreceivedmonotherapy(B).30
Recently,attheendof2014,ANVISAapprovedtheuseof adalimumab,anotheranti-TNFagent,indicatedforthe treat-mentofmoderate-to-severeNURCrefractorytoconventional therapy. Adalimumab is a fully human monoclonal anti-bodywhichbindseffectivelytosolubleandtransmembrane TNF.ThepivotalstudiesULTRA(UlcerativeColitisLong-Term RemissionandMaintenancewithAdalimumab)1and2 eval-uatedpatientswithNURCrefractorytoconventionaltherapy treated with adalimumab and compared them with those treatedwithplacebo.Asobservedinstudieswithinfliximab, NURCpatientsrefractorytoconventionaltherapyandtreated withadalimumabhadabetterclinicalresponseandimproved clinical remission, besidesa better mucosal healing versus
thosetreatedwithplacebo.Adalimumabshouldbeused sub-cutaneouslyataloadingdoseof160mggivenatweek0,with 80mgadministeredatweek2.Themaintenancedoseis40mg SCadministeredevery2weeks.23,31,32
We conclude that there is strong scientific evidence regarding the effectiveness of anti-TNF agents (infliximab andadalimumab)inthemanagementofmoderate-to-severe NURC refractory to conventional treatment. Recent meta-analysis with over 2200 patients enrolled in randomized trials showed that, in patients treated with infliximab or adalimumab,alower numberofhospitalizationsandfewer complicationsoccurred.Thosewhoweretreatedwith inflix-imabalsowereless likelytobecolectomized.Furthermore, the useofanti-TNF agentsinpatientswithNURCwasnot associatedwithanincreasedriskofseriousadverseeffects (A).33
Severe
acute
colitis
of
any
extent
Severeacuteulcerativecolitisisapotentiallyfatalcondition that has been described byTruelove & Wittsin 1954,who usedthefollowingcriteriaforitsdefinition:bloodydiarrhea(> episodes/day),analbleeding,fever(>37.8◦C),tachycardia(HR >90bpm),anemia(Hb<10.5g/dL) andincreasederythrocyte sedimentationrate(ESR>30mm).9Otherclinicalparameters
must beevaluated atadmission: degreeofhydration, ane-mia,andmalnutrition.Allpatientsmeetingcriteriaforsevere colitisshouldbehospitalizedfortreatmentintheintensive careunitwithamultidisciplinaryapproach(coloproctologist, gastroenterologist, a nutrition specialist, psychologist, and nurse).Despitethefactthatcasesofsevereacutecolitisoften areassociatedwithinflammatoryboweldisease,thisdisease canhaveothercausesthatshouldbeinvestigatedat admis-sionand,ifpresent,treated:infectiouscolitisbyClostridium difficile,cytomegalovirus,shigella,salmonella,and enterohe-morrhagicE.coli,amongothers.
Prevention of thromboembolic disease is mandatory. Whererequired,patientsshouldreceiveenteralorparenteral nutritional support, intravenous corticosteroidsand broad-spectrumantibiotics.
be averted. Toxic megacolon is characterized by an acute dilation of the colon (colon >5.5cm diameter), in asso-ciation with signs of toxemia (fever, tachycardia, pain, bloating, confusion, anemia and leukocytosis). In the face ofadiagnosticsuspicion,oneshouldavoidusingnarcotics, nonsteroidal anti-inflammatory drugs, and antidiarrheals, which can worsen the clinical picture. Furthermore, bar-ium enema and colonoscopy should also be avoided. The treatment consistsof supportivemeasures, fasting, hydra-tion, intravenous corticosteroids, antibiotics (ciprofloxacin 1–1.5g/day) and metronidazole 20–30mg/kg/day and cef-triaxone 2g/day+metronidazole 20–30mg/kg/day); and, if needed,abloodtransfusion.Ontheotherhand,anacute per-foratedabdomenisanindicationofemergencysurgery.
Thepatientseverelyaffectedshouldbeevaluatedcarefully; andinthe absence ofclinical and laboratoryimprovement after 3–4 days of parenteral corticosteroid therapy, a res-cuetherapy(cyclosporineorinfliximab)shouldbeinstituted (B).34,35 Theuseofinfliximabin thisscenario,atadose of
5mg/kg ofbodyweight, hasbeen shown tobeeffective in preventingcolectomybothinshort-andlong-term(B).36,37
Thus,itiscriticalthatallpatientswithsevereIBD(Crohn diseaseor NURC)or frequentrelapsesundertake screening tests(PPD-MantouxreactionandchestRx),serologyfor hep-atitis,and–inemergencysituations–collectionofsamples fortestsinthefaceofanyneedforbiologicor immunosup-pressivetherapy.Forthispurpose,itisimportanttobewith vaccinationupdated.
If,after48–72h,noimprovementwithsalvagetherapywas observedandifthepatient’sconditionworsens,oralsoifa bowelperforationwasdiagnosed,thesurgicaloptionwillbe mandatory.Inemergencysituationswithperitoneal contami-nationandinpatientswhorequiresurgeryandwhoarebeing treatedwith prednisone/prednisolone (dose >20mg/day for over6weeks),thesurgerymustbeperformedin2or3 sur-gicaltimes.(B)Inafirstsurgicaltime,totalcolectomywith ileostomyandburialoftherectumatthelevelof(orslightly above)theperitonealreflection;andinasecondtime,withthe reconstructionofboweltransit.38,39
Conflicts
of
interest
Dr.FabioVieiraTeixeiraisaspeakerofJanssen,Ferring,Nestlé, AbbvieandHospira.
r
e
f
e
r
e
n
c
e
s
1. BurischJ,MunkholmP.Inflammatoryboweldisease epidemiology.CurrOpinGastroenterol.2013;29:357–62. 2. MolodeckyNA,SoonIS,RabiDM,GhaliWA,FerrisM,
ChernoffG,etal.Increasingincidenceandprevalenceofthe inflammatoryboweldiseaseswithtime,basedonsystematic review.Gastroenterology.2012;142:46–54.
3. KappelmanMD,Rifas-ShimanSL,KleinmanK,etal.The prevalenceandgeographicdistributionofCrohn’sdisease andulcerativecolitisintheUnitedStates.ClinGastroenterol Hepatol.2007;5:1424–9.
4. SolbergIC,LygrenI,JahnsenJ,AadlandE,HøieO,Cvancarova M,etal.,IBSENStudyGroup.Clinicalcourseduringthefirst
10yearsofulcerativecolitis:resultsfromapopulation-based inceptioncohort(IBSENStudy).ScandJGastroenterol. 2009;44:431–40.
5.BüschK,LudvigssonJF,Ekström-SmedbyK,EkbomA,Askling J,NeoviusM.Nationwideprevalenceofinflammatorybowel diseaseinSweden:apopulation-basedregisterstudy. AlimentPharmacolTher.2014;39:57–68.
6.ManninenP,KarvonenAL,HuhtalaH,RasmussenM,CollinP. TheepidemiologyofinflammatoryboweldiseasesinFinland. ScandJGastroenterol.2010;45:1063–7.
7.JussilaA,VirtaLJ,SalomaaV,MäkiJ,JulaA,FärkkiläMA.High andincreasingprevalenceofinflammatoryboweldiseasein FinlandwithaclearNorth-Southdifference.JCrohn’sColitis. 2013;7:e256–62.
8.VictoriaCR,SassakiLY,NunesHRC.Incidenceandprevalence ratesofinflammatoryboweldiseases,inmidwesternofSão Paulostate,Brazil.ArqGastroenterol.2009;46:20–5. 9.TrueloveSC,WittsL.Cortisoneinulcerativecolitis:final
reportonatherapeutictrial.BMJ.1955;2:1041–8. 10.SchroederKW,TremaineWJ,IlstrupDM.Coatedoral
5-amino-salicylicacidtherapyformildlytomoderately activeulcerativecolitis.Arandomizedstudy.NEnglJMed. 1987;317:1625–9.
11.DignassA,EliakimR,MagroF,MaaserC,ChowersY,Geboes K,etal.SecondEuropeanevidence-basedconsensusonthe diagnosisandmanagementofulcerativecolitispart1: definitionsanddiagnosis.JCrohn’sColitis.2012;6:965–90. 12.VanAsscheG,DignassA,BokemeyerB,DaneseS,Gionchetti
P,MoserG,etal.,EuropeanCrohn’sandColitisOrganisation. SecondEuropeanevidence-basedconsensusonthediagnosis andmanagementofulcerativecolitispart3:special
situations.JCrohn’sColitis.2013;7:1–33.
13.DignassA,LindsayJO,SturmA,WindsorA,ColombelJF,Allez M,etal.SecondEuropeanevidence-basedconsensusonthe diagnosisandmanagementofulcerativecolitispart2: currentmanagement.JCrohn’sColitis.2012;6:991–1030. 14.GisbertJP,BermejoF,Pérez-CalleJL,TaxoneraC,VeraI,
McNichollAG,etal.Fecalcalprotectinandlactoferrinforthe predictionofinflammatoryboweldiseaserelapse.Inflamm BowelDis.2009;15:1190–8.
15.NerichV,MonnetE,EtienneA,LouafiS,RaméeC,RicanS, etal.Geographicalvariationsofinflammatoryboweldisease inFrance:astudybasedonnationalhealthinsurancedata. InflammBowelDis.2006;12:218–26.
16.RönnblomA,SamuelssonSM,EkbomA.Ulcerativecolitisin thecountyofUppsala1945–2007:incidenceandclinical characteristics.JCrohn’sColitis.2010;4:523.
17.FloresC,SassakiLY.Imunomoduladores.In:TeixeiraFV, KotzePG,editors.Retocoliteulcerativa:estadoatualdo tratamentonoséculo21.RiodeJaneiro:DOC;2013.p.51–61. 18.ZaltmanC,TeixeiraFV,ZerôncioM.Salicilatos.In:TeixeiraFV,
KotzePG,editors.Retocoliteulcerativa:estadoatualdo tratamentonoséculo21.RiodeJaneiro:DOC;2013.p.29–41. 19.FordAC,AchkarJP,KhanKJ,KaneSV,TalleyNJ,MarshallJK,
etal.Efficacyof5-aminosalicylatesinulcerativecolitis: systematicreviewandmeta-analysis.AmJGastroenterol. 2011;106:601–16.
20.KhanN,AbbasAM,KolevaYN,BazzanoLA.Long-term mesalaminemaintenanceinulcerativecolitis:whichismore important?Adherenceordailydose.InflammBowelDis. 2013;19:1123.
22.TeixeiraFV,KotzePG.Biológicos.In:TeixeiraFV,KotzePG, editors.Retocoliteulcerativa:estadoatualdotratamentono século21.RiodeJaneiro:DOC;2013.p.73–91.
23.FrancesconiC,PontesEL.Corticosteróides.In:TeixeiraFV, KotzePG,editors.Retocoliteulcerativa:estadoatualdo tratamentonoséculo21.RiodeJaneiro:DOC;2013. p.42–50.
24.TravisSPL,StangeEF,LémannM,ØreslandT,BemelmanWA, ChowersY,etal.Europeanevidence-basedconsensusonthe managementofulcerativecolitis:currentmanagement.J Crohn’sColitis.2008;2:24–62.
25.TimmerA,McDonaldJW,TsoulisDJ,MacdonaldJK. Azathioprineand6-mercaptopurineformaintenanceof remissioninulcerativecolitis.CochraneDatabaseSystRev. 2012;12:9.
26.KennedyNA,RhatiganE,ArnottID,NobleCL,ShandAG, SatsangiJ,etal.Atrialofmercaptopurineisasafestrategyin patientswithinflammatoryboweldiseaseintolerantto azathioprine:anobservationalstudy,systematicreviewand meta-analysis.AlimentPharmacolTher.2013;38:1255–66. 27.RutgeertsP,SandbornWJ,FeaganBG,ReinischW,OlsonA,
JohannsJ,etal.Infliximabforinductionandmaintenance therapyforulcerativecolitis.NEnglJMed.2005;353:2462–76. 28.JarnerotG,HertervigE,Friis-LibyI,BlomquistL,KarlenP,
GrannoC,etal.Infliximabasrescuetherapyinsevereto moderatelysevereulcerativecolitis:arandomized,
placebo-controlledstudy.Gastroenterology.2005;128:1805–11. 29.GustavssonA,JärnerotG,HertervigE,Friis-LibyI,Blomquist
L,KarlénP,etal.Clinicaltrial:colectomyafterrescuetherapy inulcerativecolitis–3-yearfollow-upoftheSwedish-Danish controlledinfliximabstudy.AlimentPharmacolTher. 2010;32:984–9.
30.PanaccioneR,GhoshS,MiddletonS,MárquezJR,ScottBB, FlintL,etal.CombinationtherapywithInfliximaband Azathioprineissuperiortomonotherapywitheitheragentin ulcerativecolitis.Gastroenterology.2014;146:392–400.
31.ReinischW,SandbornWJ,HommesDW,D’HaensG,Hanauer
S,SchreiberS,etal.Adalimumabforinductionofclinical
remissioninmoderatelytoseverelyactiveulcerativecolitis: resultsofarandomizedcontrolledtrial.Gut.2011;60:780–7. 32.SandbornWJ,vanAsschG,ReinischW,ColombelJF,D’Haens
G,WolfDC,etal.Adalimumabinducesandmaintainsclinical remissioninpatientswithmoderate-to-severeulcerative colitis.Gastroenterology.2012;142:257–65.
33.LopezA,FordAC,ColombelJ-F,ReinischW,SanbornWJ, Peyrin-BirouletL.Efficacyoftumornecrosisfactor
antagonistsonremission,colectomyandhospitalizationsin ulcerativecolitis:meta-analysisofplacebo-controlledtrials. DigLiverDis.2015;47:356–64.
34.LaharieD,BourreilleA,BrancheJ,AllezM,BouhnikY,FilippiJ, etal.,Grouped’EtudesThérapeutiquesdesAffections InflammatoiresDigestives.Ciclosporinversusinfliximabin patientswithsevereulcerativecolitisrefractoryto intravenoussteroids:aparallel,open-labelrandomised controlledtrial.Lancet.2012;380:1909–15.
35.VanAsscheG,D’HaensG,NomanM,VermeireS,HieleM, AsnongK,etal.Randomizeddouble-blindcomparisonofa 4mg/kgversus2mg/kgintravenouscyclosporineinsevere ulcerativecolitis.Gastroenterology.2003;125:1025–31. 36.KohnA,DapernoM,ArmuzziA,CappelloM,BianconeL,
OrlandoA,etal.Infliximabinsevereulcerativecolitis:a short-termresultsofdifferentinfusionregimensand long-termfollow-up.AlimentPharmacolTher. 2007;26:747–56.
37.JarnerotG,HertervigE,Friis-LibyI,BlomquistL,KarlénP, GrännöC,etal.Infliximabasrescuetherapyinsevereto moderatelysevereulcerativecolitis:arandomized,
placebo-controlledstudy.Gastroenterology.2005;128:1805–11. 38.GanSI,BeckPL.Anewlookattoxicmegacolon:anupdate
andreviewofincidence,etiology,pathogenesis,and management.AmJGastroenterol.2003;98:2363–71. 39.ShethSG,LaMontJT.Toxicmegacolon.Lancet.