jcoloproctol(rioj).2015;35(4):227–229
w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Case
Report
Repair
of
post
polypectomy
colonic
perforation
by
Endoclip:
a
case
report
Ahmad
Hormati
a,∗,
Mohmad
Reza
Ghadir
a,
Pezhman
Alavinejad
b,
Seyed
Saeed
Sarkeshikian
a,
Mahdi
Pezeshki
Modares
aaDivisionofGastroenterologyandHepatology,DepartmentofInternalMedicine,QomUniversityofMedicalSciences,Qom,Iran
bResearchCenterforInfectiousDiseasesofDigestiveSystem,AhvazJundishapurUniversityofMedicalSciences,Ahvaz,Iran
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received16June2015 Accepted28August2015
Availableonline21September2015
Keywords:
Polypectomy Colonicperforation Endoclip
a
b
s
t
r
a
c
t
A73-year-oldwomanwasadmittedtoevaluateforirondeficiencyanemia,increasedserum creatinine,andascites.Hercolonoscopyrevealedapolypatthejunctionofsigmoidand descendingcolon,andafterpolypectomy,a6mmcolonicperforationwasseen.The per-forationwasdetectedbyradiographyandCTscan;andbesideconservativemanagement andantibiotics,herperforationwasclosedbyusingEndoclip.Thepatientwasobservedand dischargedfromhospitalwithoutanysurgery5dayslater,andinfollow-uptherewasno problemregardingperforation.
©2015SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
Reparo
de
perfurac¸ão
de
cólon
pós-polipectomia
por
Endoclip:
relato
de
caso
Palavras-chave:
Polipectomia Perfurac¸ãodecólon Endoclip
r
e
s
u
m
o
Mulher,73anos,internadaparaavaliac¸ãoparaanemiaferropriva,comaumentoda cre-atininaséricaeascite.Acolonoscopiarevelouumpóliponajunc¸ãodoscolossigmoidee descendentee,emseguidaàpolipectomia,foiobservadaumaperfurac¸ãode6mmnocólon, comprovadaporradiografiasetomografiacomputadorizada.Alémdotratamento conser-vadoredaantibioticoterapia,aperfurac¸ãofoiocluídacomEndoclip.Apacienteficousob observac¸ãoerecebeualtadohospitalsemqualquercirurgia5diasmaistarde.Duranteo seguimento,nãoforamobservadosproblemascomrelac¸ãoàperfurac¸ão.
©2015SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
∗ Correspondingauthor.
E-mail:[email protected](A.Hormati).
http://dx.doi.org/10.1016/j.jcol.2015.08.002
228
jcoloproctol(rioj).2015;35(4):227–229Introduction
Perforation is one of the most important complication of colonoscopythatisrarebutpotentiallyhasahighrateof mor-talityandmorbidity.1,2 Incidenceofperforationis0.016%in
diagnosticcolonoscopybutraisesupto5%following thera-peuticcolonoscopy3andthemostcommonsiteofperforation
issigmoidcolon.4Inthiscasereport,wereviewendoscopic
managementofcolonperforationafterpolypectomy.
Case
report
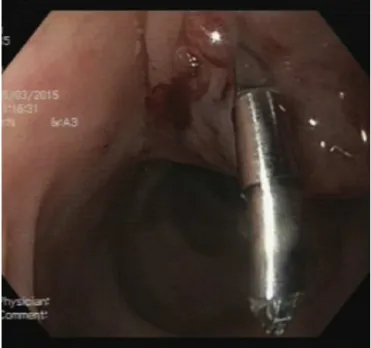
A73-year-old ladyhasbeen admittedinhospitalto evalu-ateforirondeficiencyanemia,raisingserumcreatinine,and abdominalascites. Adiagnostic colonoscopywasrequested duetoheranemia,and colonoscopyrevealedafew sessile polypsinsigmoidanddescendingcolon.Thepatientwasa candidateforpolypectomyandan1cmsessilepolypatthe junctionofthesigmoidtodescendingcolonwasexcisedby snarefollowingsubmucosalinjectionof1mlnormalsaline.
Afterpolypectomy,a6mmperforationwasinduced(Fig.1); theairpumpwasturnedoffandthesecretionsaroundsite ofperforationweresuctioned.Afterinjectionof2mlnormal salineattheborders,twoEndoclip(BostonScientificCo.)were insertedandtheperforationwasclosed(Fig.2).Theluminal airwassuctionedand the scope gotretrieved.Thepatient wasputonNPO,andintravenousantibiotics(Ceftriaxoneplus Metronidazole)started.AbdominopelvicCTscanwithout con-trastrevealedthepresenceofalotoffreeairinperitoneal cavity(Fig.3).
Surgicalconsultationwasrequestedandthepatientwas observed.Duringherdailyvisit,therewasnosignof peritoni-tisofleukocytosisandvitalsignswerestable.Threedayslater, abdominopelvicCTscanwithoralcontrastrevealedno con-trastagentleakage(Fig.4)sooralregimenwasdulystarted. Withserumhydration,thecreatinineleveldeclinedfrom2.3 to0.8andantibioticregimenchangedfromintravenoustooral andcontinuedfor2weeks.Thepatientwasdischarged,and
Fig.1–Perforatedcolonafterpolypectomy.
Fig.2–ClosureofperforationwithEndoclip.
inherfollow-up 2monthslater,the generalconditionwas satisfactory withnoloculatedfluidcollectioninabdominal cavity.Afterimprovingofrenalfunctionandnormalizationof serumcreatinine,theascitesgraduallydisappearedfollowing thediuretictherapy.
Discussion
Thepossibilityofperforationishigheramongthese condi-tions:polypectomyofpolypsmorethan2cmorsessilepolyps, submucosaldissection,polypectomyatrectosigmoidjunction orjunctionofsigmoidtodescendingsegment,colon diverticu-losis,colonicobstruction,andhistoryofabdominalsurgery.3,5
The most common clinical clues for diagnosing of per-foration include visualization of site of perforation during
jcoloproctol(rioj).2015;35(4):227–229
229
Fig.4–Absenceofcontrastagentleakageinfollow-upCT scan.
colonoscopy,signsofperitonitis(abdominalpainand tender-ness)inthefirstfewhoursanddelayedsymptomsfollowing micro-perforations.2 Presenceoffreeairinradiography,CT
scanorMRIorextravasationofcontrastmediacouldbe diag-nosticforperforation.
Choosingsurgicalornon-surgicaltherapyforperforationof coloniscontroversialbutmostofthepatientsneedsurgical intervention,6 althoughnon-surgicalor laparoscopic
proce-duresareapplicableinspecialsituations.7Theconservative
managementwhichincludesintravenousfluids,NPO,bowel restandbroadspectrumantibiotics,isjustproperforpatients witha good generalcondition. Inthe absence ofany sign ofperitonitis and incaseof peritonitis, anurgentsurgical intervention is necessary and advisable. The success rate ofconservativemanagementforcolon perforationisabout 33–73%.8 Insmallcolonicperforations, resultsof
therapeu-ticcolonoscopyarebetterthanconservativemanagement.8
Endoscopicapproachforclosureofperforationincludesusing multi-channelscope andEndoclipwhichshouldbeapplied by an experienced endoscopist and is often successful in perforationsless than 10mm.7,9 During the procedure, the
luminalairshouldbesuctionedandthesuccessratedeclines dramatically if the laceration be more than 10mm. After endoscopicrepair,thepatientshouldbeobservedwithbroad spectrumantibioticsandintravenousfluids.9Thesuccessrate
ofEndoclipwasreportedtobe69–93%andsurgeryhasbeen recommended inthepresenceofany sign ofperitonitis or failureofconservativeand/orendoscopictreatmentand dete-rioratingofclinicalcourse.1,2,10
Inthepresentedcase,byusingsinglechannelPentaxScope (HD Series, EPK-i)and Endoclip(Boston Scientific Co.), the perforationwasrepairedsuccessfullywhichhighlights impor-tanceofadequatecolonicprepandavailabilityofaccessory devisesbesideclinicalexperience.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.LohsiriwatV,SujarittanakarnS,AkaraviputhT,
LertakyamaneeN,LohsiriwatD,KachinthornU.Colonoscopic perforation:areportfromWorldGastroenterology
OrganizationendoscopytrainingcenterinThailand.WorldJ Gastroenterol.2008;14:6722–5.
2.LüningTH,Keemers-GelsME,BarendregtWB,TanAC, RosmanC.Colonoscopicperforations:areviewof30,366 patients.SurgEndosc.2007;21:994–7.
3.GattoNM,FruchtH,SundararajanV,JacobsonJS,GrannVR, NeugutAI.Riskofperforationaftercolonoscopyand sigmoidoscopy:apopulation-basedstudy.JNatlCancerInst. 2003;95:230–6.
4.GedebouTM,WongRA,RappaportWD,JaffeP,KahsaiD, HunterGC.Clinicalpresentationandmanagementof iatrogeniccolonperforations.AmJSurg.1996;172:454–7, discussion457–458.
5.WayeJD.Colonoscopicpolypectomy.DiagnTherEndosc. 2000;6:111–24.
6.AvgerinosDV,LlagunaOH,LoAY,LeitmanIM.Evolving managementofcolonoscopicperforations.JGastrointest Surg.2008;12:1783–9.
7.BarbagalloF,CastelloG,LatteriS,GrassoE,GagliardoS,La GrecaG,etal.Successfulendoscopicrepairofanunusual colonicperforationfollowingpolypectomyusinganendoclip device.WorldJGastroenterol.2007;13:2889–91.
8.OrsoniP,BerdahS,VerrierC,CaamanoA,SastreB,Boutboul R,etal.Colonicperforationduetocolonoscopy:a
retrospectivestudyof48cases.Endoscopy.1997;29:160–4.
9.TreccaA,GajF,GagliardiG.Ourexperiencewithendoscopic repairoflargecolonoscopicperforationsandreviewofthe literature.TechColoproctol.2008;12:315–21,discussion 322.