www.jped.com.br
REVIEW
ARTICLE
Nutritional
screening
in
hospitalized
pediatric
patients:
a
systematic
review
夽
,
夽夽
Adriana
Fonseca
Teixeira
a,∗,
Kátia
Danielle
Araújo
Lourenc
¸o
Viana
baUniversityHospital,UniversidadeFederaldoMaranhão(UFMA),SãoLuís,MA,Brazil
bDepartmentofPhysiologicalSciences,UniversidadeFederaldoMaranhão(UFMA),SãoLuís,MA,Brazil
Received17July2015;accepted26August2015 Availableonline6February2016
KEYWORDS
Screening; Malnutrition; Pediatrics; Systematicreview
Abstract
Objective: Thissystematicreviewaimedtoverifytheavailablescientificevidenceonthe clini-calperformanceanddiagnosticaccuracyofnutritionalscreeningtoolsinhospitalizedpediatric patients.
Datasource:A search was performed in the Medline (National Library of Medicine United States),LILACS(LatinAmericanandCaribbeanHealthSciences),PubMed(USNationalLibrary ofMedicineNationalInstitutesofHealth),intheSCIELO(ScientificElectronicLibraryOnline), throughCAPESportal(Coordenac¸ãodeAperfeic¸oamentodePessoaldeNívelSuperior),bases Scopus eWebofScience.ThedescriptorsusedinaccordancewiththeDescriptorsinHealth Sciences(DeCS)/MedicalSubjectHeadings(MeSH)listwere‘‘malnutrition’’,‘‘screening’’,and ‘‘pediatrics’’,aswellastheequivalentwordsinPortuguese.
Summaryofthefindings: Theauthorsidentified270articlespublishedbetween2004and2014. Afterapplyingtheselectioncriteria,35wereanalyzedinfullandeightarticleswereincluded inthesystematicreview. We evaluatedthemethodological quality ofthestudiesusingthe QualityAssessmentofDiagnosticAccuracyStudies(QUADAS).Fivenutritionalscreeningtoolsin pediatricswereidentified.Amongthese,theScreeningToolfortheAssessmentofMalnutritionin Pediatrics(STAMP)showedhighsensitivity,almostperfectinter-rateragreementandbetween thescreeningandthereferencestandard; theScreeningToolRiskonNutritional Statusand Growth(STRONGkids)showedhighsensitivity,lowerpercentageofspecificity,substantial intra-rateragreement,andeaseofuseinclinicalpractice.
夽
Pleasecitethisarticleas:TeixeiraAF,VianaKD.Nutritionalscreeninginhospitalizedpediatricpatients:asystematicreview.JPediatr
(RioJ).2016;92:343---52.
夽夽
StudyassociatedwiththeMultidisciplinaryResidencyPrograminHealth,HospitalUniversitário,UniversidadeFederaldoMaranhão
(UFMA),SãoLuís,MA,Brazil.
∗Correspondingauthor.
E-mail:[email protected](A.F.Teixeira). http://dx.doi.org/10.1016/j.jped.2015.08.011
344 TeixeiraAF,VianaKD
Conclusions: Thestudiesincludedinthissystematicreviewshowedgoodperformanceofthe nutritionalscreeningtoolsinpediatrics,especiallySTRONGkidsandSTAMP.Theauthors empha-sizetheneedtoperformformorestudiesinthisarea.Onlyonetoolwastranslatedandadapted totheBrazilianpediatricpopulation,anditisessentialtocarryoutstudiesoftooladaptation andvalidationforthispopulation.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/ 4.0/).
PALAVRAS-CHAVE
Triagem; Desnutric¸ão; Pediatria;
Revisãosistemática
Triagemnutricionalempacientespediátricoshospitalizados:umarevisãosistemática
Resumo
Objetivo: Esta revisão sistemática tem por objetivo verificar as evidências científicas disponíveis sobreodesempenho clínicoe acuráciadiagnóstica dosinstrumentos detriagem nutricionalempacientespediátricoshospitalizados.
Fontededados: Realizou-sebuscanasbasesdedadosMedline(National LibraryofMedicine UnitedStates),LILACS(LatinAmericanandCaribbeanHealthSciences),PubMed(USNational Library of Medicine National Institutes of Health), na biblioteca eletrônica SCIELO (Scien-tific Electronic Library Online), atravésdo portal de periódicos daCAPES (Coordenac¸ão de Aperfeic¸oamentodePessoaldeNívelSuperior),basesScopuseWebofScience.Osdescritores utilizados conforme lista do DeCS (Descritores em Ciências da Saúde)/MeSH (Medical Sub-jectHeadings)foram‘‘desnutric¸ão’’,‘‘triagem’’e‘‘pediatria’’,bemcomo,‘‘malnutrition’’, ‘‘screening’’e‘‘pediatrics’’,respectivamente.
Síntesedosdados: Identificou-se 270artigos, publicados entre 2004e2014. Apósaplicac¸ão doscritériosdeselec¸ão,35foramanalisadosnaíntegra,sendoincluídos8artigosnarevisão sistemática.Avaliou-seaqualidademetodológicadosestudosutilizando-seoQUADAS(Quality AssessmentofDiagnosticAccuracyStudies).Verificou-se05instrumentosdetriagemnutricional empediatria.Dentreestes,oSTAMP(ScreeningToolfortheAssessmentofMalnutritionin Pedi-atrics)apresentousensibilidadeelevada,concordânciaquaseperfeitainter-avaliadoreentre atriagemepadrãodereferência;oSTRONGkids(ScreeningToolRiskonNutritionalStatusand Growth)evidenciousensibilidadeelevada,menorpercentualdeespecificidade,concordância intra-avaliadorsubstancialefacilidadedeusonapráticaclínica.
Conclusões: Osestudosincluídosnestarevisãosistemáticademonstraramumbomdesempenho dosinstrumentosde triagemnutricionalempediatria, principalmenteSTRONGkidseSTAMP. Evidencia-seanecessidadedemaispesquisasnessaárea.Apenasuminstrumentofoitraduzido eadaptadoparaapopulac¸ãopediátricabrasileira,sendoimprescindívelarealizac¸ãodeestudos deadaptac¸ãoevalidac¸ãodeinstrumentosparaessapopulac¸ão.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4. 0/).
Introduction
Ithas been widely described inthe literature that inade-quatenutritional status has negative implications for the child, resultingin important consequences for the child’s healthanddevelopment.1---3
Malnutritioninpediatricpatientsisaseverepathological condition anda risk factor for unfavorableoutcome. It is associated with immune system vulnerability, increased risk of infections, postoperative complications, impaired wound healing, and development of pressure ulcers, as wellasincreased morbidityand mortalityof theaffected individuals.4---8
This clinical condition slows down the recovery pro-cess, demanding prolonged hospital stay and increasing costs related to medication and health care.4,5,8,9 Even withthefrequentassociationbetweenhospitalmalnutrition
and risk ofadverse clinical events, this is aproblem that remains largely underestimated and that sometimes goes unnoticed.3,10---12
In recent decades, within the scenario of the epi-demiological and nutritional transition, Brazilian studies haveevidencedasignificantdecreaseintheprevalenceof child malnutrition in the country.13,14 However,in opposi-tion to a downward trend in malnutrition in the general population, the situation is getting worse in hospitals, as demonstrated by the increase in its incidence15,16 and prevalence.17
Althoughitisdifficulttoquantifytheactualprevalence ofmalnutritioninhospitalizedchildren,scientificevidence emphasizestheirfrequencyinthisgroup.International stud-ies show malnutrition rates between 19% and 45.6% in hospitalizedchildren.1,18---20InBrazil,surveysindicaterates
Duringhospitalization,childrencanbemalnourishedor aggravateapre-existingmalnutritionsituation.Therefore, itisessentialtoachievetheearlydetectionofnutritional depletionduringhospitalstay.1,25
In thissense, thepatientnutritional statusassessment identifiesonlythosewhoarealreadymalnourished,andnot thoseatriskofmalnutrition.5,26Topreventhospital malnu-trition,studiesshowthattheearlydetectionofnutritional riskisessential,asitallowsappropriatenutritional interven-tionstopreventmalnutritionanditsconsequences.2,4,5,8,12,27 Foradultpatients,severalscreeningtoolshavebeen val-idatedinavarietyof clinicalscenariosandwithdifferent groups of patients.4 However, appropriate tools for pedi-atric use arescarce,28,29 and thereis no consensusabout the best method to assess risk of malnutrition in these patients.1,8,30
Although there are recommendations of several soci-eties toperformnutritional riskidentification inpediatric patients,3,31 in practice,due tothe lack of a simple and validated method, nutritional screening is not yet widely performed.4,9Anytooldesignedfornutritionalscreeningin pediatricsshouldbesimple,fast,reproducible,7andhave goodsensitivityandspecificity.4,29,32
Therefore, this systematic review aimed to verify the availablescientificevidenceontheclinicalperformanceand diagnosticaccuracyofthetoolsusedfor screening malnu-tritionriskinpediatricpatients.
Methods
Thiswasasystematicreviewoftheliteratureonthe avail-able scientific evidence on the clinical performance and diagnosticaccuracy ofthetools usedfor malnutritionrisk screeninginpediatricpatients,publishedbetween2004and 2014.
The search strategy used included searches in the MEDLINE, LILACS, PubMed, the SciELO electronic library databases; the CAPES Portal was used to access the Scopus and Web of Science databases. The descriptors were chosen according to the Descriptors in Health Sci-ences (DeCS) and Medical Subject Headings (MeSH) list. In accordance with the DeCS list, the used terms were ‘‘desnutric¸ão,’’‘‘triagem,’’and‘‘pediatria’’inPortuguese; the MeSHdescriptors were‘‘malnutrition,’’ ‘‘screening,’’ and‘‘pediatrics’’,inEnglish.Inadditiontodescriptors,the Booleanoperator‘‘AND’’wasappliedforthecombination oftermsinthedatabases.
Searchesusingthereferencesofselectedarticleswere alsoperformed, aiming toidentifypublications not previ-ously found that were relevant to the review topic. The searcheswereperformedfromNovember2014toApril2015. The following inclusion criteria were defined for ade-quate article selection: studies on hospitalized pediatric patients, which assessed the use of some nutritional risk screening tool; and articles published in the last decade (2004---2014) in Portuguese, English, and/or Spanish. The exclusioncriteriawere:qualitativestudies,reviewarticles, editorials,letterstotheeditor,bookchapters,articlesnot availabletobeaccessedinfull,andalsoarticlesthatdidnot havedataonthesensitivityandspecificityofthescreening tools.
The article selection process was carried out in four stages, according to the model recommended by the Cochrane Collaboration:33 1 --- identification of the arti-cles by searching the databases and articles retrieved throughthereferencesofselectedarticles;2---selection, atthisstage,theduplicatearticleswereexcluded,andby screeningthetitlesandabstractsoftheremainingarticles, the authors excluded those that had no association with thekeywordsdefinedforthesearch;3---theeligibilitywas assessedbyreadingthearticlesinfull(excludingthosethat didnot meet the pre-established eligibility criteria) and; 4---inclusionofeligiblearticlesinthesystematicreview.
Toevaluatetheclinicalperformanceanddiagnostic accu-racyof the tools, the following criteriawere considered: sensitivity--- screening capacity todetect individuals who wereactuallyatnutritionalrisk;specificity---thecapacity todiagnoseindividualswithnonutritionalrisk;positive pre-dictivevalue---thepatient’sprobabilitytobeatriskamong those whotested positive; and negativepredictive value ---thepatient’sprobabilitytobehealthyamongthosewho testednegative.34
The authors also verified whether the studies ana-lyzed the reproducibility and reliability of the screening tools, using data from the agreement analysis between the assessed nutritional risk screening and the used ref-erence standard, as well as the intra- and inter-bserver agreement shown in the studies. To interpret the Kappa statistical value, the classification of Landis and Koch was considered:35 no agreement (<0); poor agreement (0---0.19);mildagreement(0.20---0.39);moderateagreement (0.40---0.59);substantialagreement(0.60---0.79);andalmost perfectagreement(0.80---1.00).
To assess the methodological quality of the studies, a modifiedversionofQualityAssessmentofDiagnostic Accu-racyStudies (QUADAS) was used.36 Recommended by the CochraneHandbook,37thistoolisdesignedtomeasurethe sourcesofbias,variability,andqualityofinformationinthe studies.36 Thisversionevaluates 11ofthe 14itemsofthe originalversion,consideringthattheremainingitems(2,8, and9)refertoproblemsrelatedtohowtoreportdata,and notexactlytothemethodologicalqualityofthestudy.38 A goodstudy performanceis verifiedwhen it hasa positive evaluationinatleasteightofthe11itemsofQUADAS.39
Results
Initially,270articleswereidentified,andattheendofthe selectionprocess,accordingtothemodelrecommendedby theCochraneCollaboration,eightarticleswerequantified, which met all the pre-established eligibility criteriaand, therefore,wereincludedinthissystematicreview(Fig.1). Ofthe eightselectedstudies, three(37.5%) were pub-lishedin2012.Theageoftheindividualswhoparticipated inthestudiesrangedfrom1monthto18years.Acomplete descriptionofthearticlesisshowninTable1.
346 TeixeiraAF,VianaKD
Identification
Identified references
PubMed (n=76), Medline (n=45), LILACS (n=13), SCIELO (n=2) and capes journal portal (n=128)
total (n=264)
References identified by manual search from
other sources (n=6)
Selection
Duplicate references removed (n=52)
Selected references (n=218)
Full articles reviewed for eligibility
(n=35)
Studies included in the synthesis
(n=08)
Full articles excluded from the analysis
(n =27)
Eligibility
Inclusion
References excluded by title and summary
(n=183)
Figure1 Flowchartofarticleselectionforthesystematicreview,accordingtotheCochraneCollaborationmodel.
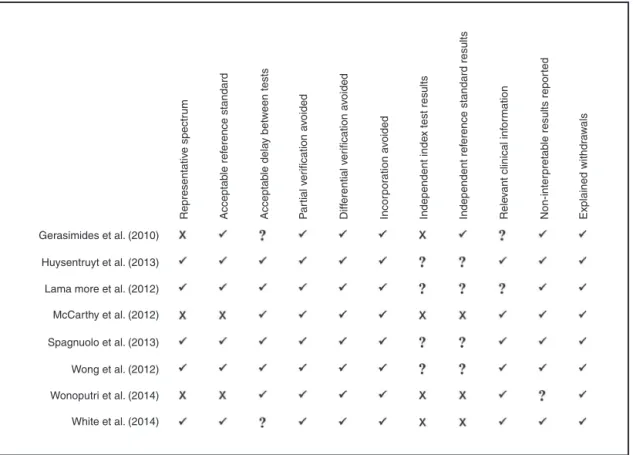
haveanadequatereferencestandard(anthropometry),and furthermore,theinformationoffourstudies (50%)didnot allow to verify whether the interpretation of results of the reference test and the index test was independently performedin theincluded studies, or iftherewasreview bias.The resultofthemethodologicalqualityassessment, accordingtothemodifiedversionofQUADAS,36 isshownin
Fig.2.
The analysis of the studies showed the use of five nutritional risk screening tools in hospitalized pediatric patients: Screening Tool for the Assessment of Malnutri-tioninPediatrics(STAMP)40---43 infour(50%)ofthestudies, Screening Tool Risk on Nutritional Status and Growth (STRONGkids)5,43,44 inthree(37.5%),PediatricYorkhill Mal-nutritionScore(PYMS)28,43intwo(25%),PediatricNutrition ScreeningTool(PNST)29 inone(12.5%),andtheSubjective GlobalNutritionalAssessment(SGNA)29inone(12.5%).
Thesensitivityofthescreeningtoolsrangedfrom59%28 to100%.43 STAMPandSTRONGkidsshowedthebestresults regardingsensitivity(100%).
Most tools had a specificity between 53%5 and 92%;28 forthisparameter,STRONGkidsandSTAMPhadthelowest percentages of specificity, 7.7%43 and 11.54%,43 respec-tively,whereasPYMShadhighspecificity(92%).28Itwasalso observedthatallstudieshadhighnegativepredictivevalue (between73.6%and100%).
The agreementbetween nutritional risk screening and thereferencestandard wasverifiedin fourof thestudies (50%),withbetter performanceofSTAMP40 (k=0.882,95% CI:0.646---1.000). Regardingthe interobserveragreement,
it varied from moderate (0.40---0.59)28 to almost perfect (0.80---1.00);40,41 the STAMP tool showed the best inter-observer agreement. For the intraobserver agreement, STRONGkids44showedthebestperformance,with substan-tialagreement(k≥0.60---.79;Table2).
Discussion
A systematic review is a valuable tool, both in individual diagnostictest assessment andtocompare differenttests in a same target-condition. Itsresults may dispelclinical doubtsorexploreotherquestions,showingthewaysothat theanswercanbefoundinthebestway.45
This systematic review of diagnostic accuracy studies synthesized the results of several studies that evaluated nutritional risk screening tools tobe used in hospitalized pediatricpatients.
Themethodologicalqualityofmoststudieswas consid-eredhigh.Themainmethodologicalproblemswererelated tolack ofadequate informationtodeterminewhetherthe interpretation of thenutritional screening usedwas inde-pendentorwhethertherewasinfluenceoftheknowledgeof thereferencestandardresults,orviceversa,characterizing areviewbiasoftheresults.
screening
in
pediatrics
347
Table1 Characterizationofthearticlesincludedinthesystematicreview.
Author/year Screening Place Population Objective Sample Agerange Referencestandard
used
Gerasimidis etal./201028
PYMS UnitedKingdom Clinicalandsurgical patients
Toassessthediagnosticaccuracy ofthenewPediatricYorkhill MalnutritionScore(PYMS)
247 1---16years Anthropometric measurements,body compositionand dietarymeasures Huysentruyt
etal./201344
STRONGkids Belgium Clinicalandsurgical patients
Testtheeasyhandlingand reproducibilityofSTRONGkidsto confirmthevalidityinaBelgian populationofhospitalized children
368 4months to15.5 years
Anthropometrics (HFA<−2SDand WFH<−2SD)
LamaMore etal./201241
STAMP Spain Clinicalandsurgical
patients
Validatethepediatricnutritional screeningtoolSTAMPforaSpanish population
250 1monthto 18years
Specializednutritional assessment(clinical, anthropometric,body composition)
McCarthy etal./201240
STAMP UnitedKingdom Clinicalandsurgical patients
Developandevaluateanutritional screeningtobeusedbythe nursingstaffintheearly identificationofmalnutritionin hospitalizedchildren
122 2---17years Fullnutritional assessmentbya nutritionist
Spagnuolo etal./20135
STRONGkids Italy Clinicalandsurgical patients
Toinvestigatetheefficacyofthe STRONGkidsscreeningtoolina populationofchildrenadmittedto 12Italianhospitals
144 1---18years Anthropometrics (HFA<−2SDand BMI<−2SD)
Wong
etal./201242
STAMP UnitedKingdom Patientswithspinal trauma
ValidatetheSTAMPscreeningtool inpediatricpatientswithspinal injuriesadmittedtotheNational CenterforSpinalTrauma
51 6months
to18years
Fulldietaryassessment (clinical,nutritional, andbiochemical)
Wonoputri etal./201443
STAMP; STRONGkids; PYMS
Indonesia Clinicalpatients Verifytheconcurrentvalidity betweenthethreenutritional screeningtoolsincomparisonto theSubjectiveGlobalAssessment ofNutrition(SGNA)
116 1---15years SGNA
White
etal./201429
PNST;SGNA Australia Clinicalandsurgical patients
Reporttheaccuracyofanew, quickandsimplePediatric NutritionScreeningTool(PNST) designedtobeusedinpediatric patients
295 1---16years Anthropometricsand SGNA
PYMS,PediatricYorkhillMalnutritionScore;STRONGkids,ScreeningToolRiskonNutritionalStatusandGrowth;STAMP,ScreeningToolfortheAssessmentofMalnutritioninPediatrics;PNST,
348 TeixeiraAF,VianaKD
Representativ
e spectr
um
Acceptab
le ref
e
rence standard
Acceptab
le dela
y betw
een tests
P
a
rtial v
er
ification a
voided
Diff
erential v
er
ification a
voided
Incor
por
ation a
voided
Independent inde
x test results
Independent ref
erence standard results
Rele
vant clinical inf
or
mation
Non-inter
pretab
le results repor
ted
Explained withdr
a
w
als
Gerasimides et al. (2010)
Huysentruyt et al. (2013)
Lama more et al. (2012)
McCarthy et al. (2012)
Spagnuolo et al. (2013)
Wong et al. (2012)
Wonoputri et al. (2014)
White et al. (2014)
Figure2 Resultsofthemethodologicalqualityevaluationofeachstudyincludedinthesystematicreview,accordingtoQUADAS.
√,Yes;
×,No;?,Unclear.
In37.5%ofthestudies,thesamplewasnot representa-tive,contrarytowhatrecommendstheCochraneHandbook for diagnosticaccuracy studies,37 whichrecommends that anappropriatesampleshouldbedefined,configuringoneof themainfactorsthatcanaffectthetestaccuracy.
Regardingthereferencestandardused,thisisstilla con-troversialpoint,giventhelackofauniversallyacceptedgold standardforthediagnosisofnutritionalriskinchildren.43
Among the studies, it was observed that some used theassessmentperformed byanutritionist asareference standard. This parameter is considered inappropriate by other authors, whopoint out that not all countries have nutritionprofessionals, andtheir rolecan varydepending onthe country.32,43,46 In this matter, anthropometrics has beenbetterassessedasareferencestandard,sinceituses universallyacceptedparameters44 andisrecommendedby aninternationalreferenceorganization.47
The nutritional screening tool must be able to iden-tifythosepatientsthatmaybenefitfromtheintervention, because they are either at risk of having or developing complications that areavoidable through adequate nutri-tionalsupport.41
Screeningmethodsconsistinthesystematizationof ques-tionsthatinvestigatetheexistenceof characteristicsthat mayreflectorberelatedtonutritionaldeterioration.15 In thisregard,nutritionalscreeningdetectsonlythepresence ofmalnutritionrisk.Conversely,nutritionalassessment,not onlydetectsmalnutrition,butalsoclassifiesitsdegreeand
allows for the collection of information to assist in its correction.48
The STAMP toolwasvalidated in a study performed in theUnited Kingdom.49 This nutritionalscreening tool con-sidersthreeelements: the patient’sclinical diagnosis and itsnutritional implications (ifany), the child’snutritional intakeduringhospitalization,andanthropometric measure-ments(wherethemeasuredvalueofthechild’sheightand weightisrecordedandcomparedtoreferencevaluesbyage andgender).10
ThePYMS wasdeveloped andvalidatedby Gerasimides etal.28intheUnitedKingdom.Itevaluatesfourpredictorsor recognizedsymptomsofmalnutritionrisk:bodymassindex (BMI),recentweightlosshistory,changesinfoodintake,and theexpectedeffectofthecurrentmedicalconditiononthe patient’snutritionalstatus.28
TheSTRONGkids,proposedbyHulstetal.ina multicen-terstudyintheNetherlands,1isaquestionnairecomprising four areas: global subjective assessment; nutritional risk of the patient’s disease (presence of high-risk disease or predicted major surgery); nutritional intake and losses (decreasedfoodintake,diarrheaandvomiting),andlossor absenceofweightgain.1,30,50,51This istheonly tool trans-latedandculturallyadaptedintoPortuguese.30
Table2 Sensitivity,specificity,predictivevalues,andreproducibilityofthestudiesincludedinthesystematicreview.
Author/year Screening Sensitivity(%) Specificity(%) PPV(%) NPV(%) Agreement(Kappa)
Gerasimides
etal./201028
PYMS 59 92 47 95 AR:k=0.46(95%CI
0.27---0.64)
Inter-observer:k=0.53 (95%CI0.38---0.67)
Huysentruyt
etal./201344 STRONGkids
71.9a 49.1a 11.9a 94.8a Inter-observer:k=0.61 69b 48.4b 10.4b 94.8b Intra-observer:k=0.66
LamaMore etal./201241
STAMP 75 60.8 39.7 87.6 Inter-observer:k=0.85
McCarthy etal./201240
STAMP 70
(95%CI51---84) 91
(95%CI86---94)
54.8
(95%CI38.8---69.8)
94.9
(95%CI90.5---97.4)
AR:k=0.882 (95%CI0.646---1.000) Inter-observer: k=0.921
(95%CI0.763---1.000)
Spagnuolo etal./20135
STRONGkids 71
(95%CI48---89) 53
(95%CI43---63) 21
(95%CI17---25)
85
(95%CI85---90)
---Wong etal./201242
STAMP 83.3 66.7 78.1 73.6 AR:k=0.507
(95%CI0.646---1.000) Inter-observer: k=0.752 Intra-observer: k=0.635
Wonoputri etal./201443
PYMS 95.31
(95%CI0.87---0.98) 76.92
(95%CI0.63---0.86) 83.56
(95%CI0.73---0.9)
93.02
(95%CI0.81---0.97)
AM:k=0.348(95%CI 0.191---0.506) CM:k=0.125(95%CI 0---0.299)
STAMP 100
(95%CI0.94---1)
11.54
(95%CI0.05---0.23) 58.2
(95%CI0.48---0.67) 100
(95%CI0.61---1)
AM:k=0.018(95%CI 0---0.140)
CM:k=0(95%CI 0---0.140) STRONGkids 100
(95%CI0.94---1) 7.7
(95%CI0.03---0.18) 57.14
(95%CI0.479---0.659) 100
(95%CI0.51---1)
AM:k=0.028(95%CI 0---0.149)
CM:k=0(95%CI 0---0.144)
White
etal./201429 PNST
89.3c 66.2c 22.5c 98.4c
---77.8d 82.1d 69.3d 87.6d
SGNA 96.5 72.5 27.7 99.5
---PYMS,PediatricYorkhillMalnutritionScore;STRONGkids,ScreeningToolRiskonNutritionalStatusandGrowth;STAMP,ScreeningToolfor
theAssessmentofMalnutritioninPediatrics;PNST,PediatricNutritionScreeningTool;SGNA,SubjectiveGlobalNutritionalAssessment;PPV,
positivepredictivevalue;NPV,negativepredictivevalue;AR,agreementwiththereferencestandardused;AM,acutemalnutrition;CM,
chronicmalnutrition;CI,confidenceinterval;HFA,heightforage;WFH,weightforheight;BMI,bodymassindexforage.
a Referencestandard:acutemalnutrition(WFH<
−2SD).
b Referencestandard:chronicmalnutrition(HFA<
−2SD).
c Referencestandard:BMI
≤−2SD.
d Referencestandard:SGNA.
ifthechildisthinorobese.32Nutritionalriskisconsidered whentherearetwopositiveanswerstothequestions.29,32
The SGNA is an adaptation of the Subjective Global Assessment, which has been validated for use in pedi-atricpatients.52 Itconsistsofaquestionnairethatcollects andanalyze severaldata: adequacyof the current height for age; adequacy of current weight for height; unin-tentional weightalterations; food intake; gastrointestinal symptoms; metabolic stress from the disease; and physi-calexamination. Although mentioned asascreening tool, it is better characterized as a structured nutritional assessment.4
Basedonthecomponentsevaluatedinthescreeningtools (STAMP,STRONGkids,andPYMS),ascorewasobtainedthat correspondstothemalnutritionrisklevel,describedaslow,
moderate,orhigh,differently fromtheSGNA,which clas-sifiespatientsaswellnourished,moderatelymalnourished, andseverelymalnourished.
Withthe exception of SGNA, which was developed for use in adult patients and subsequently validated for use inpediatric patients,52 allevaluatedscreening toolswere developedforthepediatricpopulation.
350 TeixeiraAF,VianaKD
The STRONGkids and STAMP tools showed higher sen-sitivity and very low levels of specificity. Conversely, the PYMS showed better percentage of specificity. This find-ing may be related to the reference standard used in thestudies, considering that,amongthe studies thathad anthropometrics asthe referencestandard, no significant differenceswerefoundregardingthesemeasurements,thus confirming the importance of an appropriate reference standard selection, since this choice can have important clinicalimplications.47
In the case of nutritional risk assessment in children, higher sensitivity and positive predictive value reflect an increased likelihood that the child who was identified at nutritionalriskbythetoolisactuallyinthissituation.40
Thetoolsthathavelowsensitivityaremoresusceptible tofalse-negativeresults;therefore,childrenwhoreallyare atnutritionalriskarenotdiagnosed.Asforthosethathave lowspecificity,theyaremorelikelytoprovidefalse-positive results,implyinginadiagnosisofriskinpatientsthatdonot haveit.
The screenings should have high sensitivity in order to minimize the number of false negatives.34 In this context, sensitivity is more important than specificity, becauseafalse-positiveresultwillonlyexposethepatient to a detailed nutritional assessment, whereas a false negative can result in an undetected malnourishment condition.44
Thehigherthedegreeofsensitivityofatest,thebetter itsnegativepredictive value is,andthus, the greaterthe certaintythattheindividualwithanegativeresultactually doesnothavethedisease.Andthemorespecificatestis, thebetteritspositivepredictivevalue(thatis,thegreater theconfidencethatapersonwithapositiveresulthasthe diseasebeingassessed).34
Regarding the analysis of reproducibility and reliabil-ity,keymeasurestoevaluatetheaccuracyofanutritional screening tool, better performance of the STAMP and STRONGkids tools was observed (inter and intraobserver agreement,respectively).Forthescreeningtooltohavea reproduciblemeasurement,itmusthaveagoodagreement, toreflectahighlevelofreliability.42
Regarding the applicability in pediatric practice, the idealscreening tool is the one that can quickly and reli-ably evaluate the patient’s nutritional risk in order to indicatethose whoneed a more detailedassessment and intervention.32,46Ifthescreeningtoolisextensive,itisless likelytobeusedbyhealthcareproviders.1
ThestudiesbySpagnuoloetal.5andHuysentruytetal.44 presented the STRONGkids as a simple structure tool, of practicalusein routinecare(meanof threeminutes)and easily applied in a hospital. A study that methodologi-callyanalyzedsixpediatricnutritionalscreeningtoolsalso pointedouttheSTRONGkidsastheeasiest,mostpractical, andmostreliabletest.46
AstudywithpediatricpatientsfromNewZealand, com-paringthePYMS,theSTAMPandtheSTRONGkidsscreening tests, showed that the all three are viable and able to identifynutritionalrisk,buttheSTRONGkidswasthemost reliableinthat population.53 In contrast,whencomparing thesesametoolsappliedtohospitalizedchildrenin Indone-sia, Wonoputri etal.43 recommend the PYMS asthe most reliableinthatsetting.
TheSTAMPis describedasamoredetailedinstrument, withlongerapplicationtime(±10min),possiblyduetothe interpretationofgrowthcharts.10 Inthisregard,theSGNA isreportedasanextensiveandtime-consumingtool.43The STRONGkidshasbeenconsideredfastertoapplyduetothe exclusionofweightandheight;11however,someauthors5,43 regardstheexclusionofanobjectiveevaluationasa disad-vantageofthistool.
The studies included in this review showed that most nutritionalscreening tools inpediatric patients areviable for nutritional risk screening in pediatrics. However, all thetoolspresentedadvantagesandlimitations,whichisin agreementwithseveralstudiesthatreinforcetheneedfor more researchin thearea.28,40,54---56 Moreover,only one of thesetoolshasbeentranslatedandadaptedintoPortuguese language,whichisagapinthescientificproductioninthis area.
Internationally, there are several recommendations regarding the performance of nutritional screening; how-ever,theyfocusonadultsandtheelderly,duetothelackof anappropriatetooltoidentifynutritionalriskinchildrenon hospitaladmission.40Inthissense,SykorováandZavˇrelová10 emphasize theneed for pediatric screeningtools thatare not onlyimplemented, buttruly functional, beingtargets of international accreditation standards and indicators of qualityofcare.
Furthermore, nutritional risk screening should be fol-lowed by regular assessments at the monitoring during hospitalization.46 In thisrespect,STRONGkids, STAMP, and PYMS were originally designed for regular use in patients withprolongedhospitalstay.However,theirapplicabilityfor thisobjectiverequiresfurtherinvestigations.
Regarding the limitations of this systematic review, although the search process was extensive and detailed, thereisaprobabilitythatimportantinformationhasbeen lostduetoarticlespublishedinotherlanguagesratherthan English,Spanish,andPortuguese.
Conclusion
Nutritionalriskscreeningisessentialforthecareof hospi-talizedpediatricpatients.Asforthechoiceofthescreening tooltobeusedinhospitalpractice,itisimperativetoknow theaspectsrelatedtotheirclinicalperformanceand diag-nosticaccuracy.
The studies included in this systematic review showed goodclinicalperformanceofthemalnutritionriskscreening tools in pediatric patients, mainly the STRONGkids and STAMPtools.
However,moreresearchisnecessaryinordertoexplore theseveralaspectsoftheclinicalapplicationofthesetools. Brazilian studies on this subject are incipient. Only the STRONGkids toolhasbeen translatedandadapted for the populationofhospitalizedBrazilianchildren,andtherefore, itiscriticalforfuturestudiestoadaptandvalidatetheother tools,consideringtheirclinicalperformanceanddiagnostic accuracyforthispopulation.
Conflicts
of
interest
References
1.HulstJM,Zwart H,HopWC, JoostenKF. Dutchnational sur-veytotesttheSTRONGkids nutritionalriskscreeningtool in hospitalizedchildren.AmJClinNutr.2010;29:106---11.
2.JonkersC,KlosM,KouwenoordK,Kruizenga H,RemijnseW.
Guidelinescreeningandtreatmentofmalnutrition.Translation
oftheDutchguideline screeningand treatmentof
malnutri-tion; 2011, version June 2011. Available from: http://www.
fightmalnutrition.eu[cited20Jan2015].
3.MehtaNM, Corkins MR, LymanB, Malone A, Goday PS, Car-neyLN,etal.Definingpediatricmalnutrition:aparadigmshift towardetiology-related definitions. J Parenter EnteralNutr. 2013;37:460---81.
4.Hartman C,ShamirR, Hecht C.Malnutrition screening tools for hospitalized children. Curr Opin Clin Nutr Metab Care. 2012;15:303---9.
5.SpagnuoloMI, Liguoro I, Chiatto F,Mambretti D, GuarinoA. Applicationofa scoresystemto evaluatetheriskof malnu-tritioninamultiple hospitalsetting. ItalJPediatr.2013;39: 1---7.
6.TouzetS,DuclosA,DenisA,Restier-MironL,OccelliP,PolazziS, etal.Multifacetedinterventiontoenhancethescreeningand careofhospitalisedmalnourishedchildren:studyprotocolfor thePREDIRE clusterrandomizedcontrolledtrial. BMCHealth ServRes.2013;13:1---8.
7.VillaresJM,CalderónVV,GarcíaCB,LamaMoreR,FerreiroSR, QuintanaLP.Evaluacióndelestadonutricionaldeni˜nos ingre-sadosenelhospitalenEspa˜na;estudioDHOSPE(Desnutrición HospitalariaenelPacientePediátricoenEspa˜na).NutrHosp. 2013;28:709---18.
8.CostaMV,PastoreCA.Herramientadecribadonutricionalversus valoraciónnutricionalantropométricadeni˜noshospitalizados: cuálmétodoseasociamejorconlaevoluciónclínica?Arch Lati-noamNutr.2015;65:12---20.
9.GholampourZ,HosseininasabM,KhademiG,SezavarM, Abdol-lahpourN,ImaniB.Assessmentofnutritionalstatusbasedon STRONGkidstool in Iranianhospitalizedchildren. IntJChild HealthNutr.2015;4:61---6.
10.Sikorová L, Zavˇrelová B. Evaluation of malnutrition of hospitalizedchildrenusingtheScreeningToolfor the Assess-mentof Malnutrition in Paediatrics. ˇCas Lék ˇCes. 2012;151: 397---400.
11.Durakbas¸aC¸U,Fettaho˘gluS,BayarA, Mutus M,OkurH. The prevalenceof malnutritionand effectiveness ofSTRONGkids toolintheidentificationofmalnutritionrisksamongpediatric surgicalpatients.BalkanMedJ.2014;31:313---21.
12.BaxterJB,Al-MadhakiFI,ZlotkinSH.Prevalenceofmalnutrition atthetimeofadmissionamongpatientsadmittedtoa Cana-diantertiary-carepaediatrichospital.PaediatrChild Health. 2014;19:413---7.
13.Batista Filho M, Rissin A. A transic¸ão nutricional no Brasil: tendênciasregionaisetemporais.CadSaudePublica.2003;19: 181---91.
14.MonteiroCA,BenícioMH,KonnoSC,SilvaAC,LimaAL,Conde WL. Causas do declínio da desnutric¸ão infantil no Brasil, 1996---2007.RevSaudePublica.2009;43:35---43.
15.AraújoMA,LimaLS,OrnelasGC,LogradoMH.Análise compara-tivadediferentesmétodosdetriagemnutricionaldopaciente internado.ComCienciasSaude.2010;21:331---42.
16.Waitzberg DL, Caiffa WT, Correia MI. Hospital malnutrition: theBraziliannationalsurvey (IBRANUTRI):a studyof40,000 patients.Nutrition.2001;17:573---80.
17.LeiteHP.Comoidentificarorisconutricionalemcrianc¸as hos-pitalizadas?RevBrasTerapIntens.2003;15:132.
18.DoganY,ErkanT,YalvacS,AltayS,C¸ulluC¸okugrasF,AydinA, etal. Nutritionalstatus ofpatients hospitalizedinpediatric clinic.TurkJGastroenterol.2005;16:212---6.
19.PawellekI,DokoupilK,KoletzkoB.Prevalenceofmalnutrition inpaediatrichospitalpatients.ClinNutr.2008;27:72---6. 20.Rodriguez YH, GuerraML, Cabrera YJ, Fonte LM,Montequín
ZC.Estado nutricionalde losni˜nosingresadosenelHospital Pediátrico de Pinar del Río. Rev Ciencias Medicas. 2012;16: 84---97.
21.Péret Filho LA, Penna FG,Rodrigues FG, Santana DP, Hanan B,OliveiraGN,etal.Avaliac¸ãonutricionaldecrianc¸as inter-nadasemenfermariageralde umhospital público.Pediatria (SãoPaulo).2005;27:12---8.
22.CruzLB,RodriguesFO,MaksudM,ZambranoM,RaimundoF, Dor-nelesCT.Estadonutricionalefatoresderiscoparadesnutric¸ão noatendimentonutricionalpediátricodaadmissãohospitalar. RevHCPA.2009;29:194---9.
23.SarniRO, CarvalhoMF,MonteCM,AlbuquerqueZP, SousaFI. Anthropometricevaluation, riskfactorsfor malnutrition,and nutritionaltherapyforchildreninteachinghospitalsinBrazil. JPediatr(RioJ).2009;85:223---8.
24.MagalhãesEA,MartinsMA,RodriguesCC,MoreiraAS.Associac¸ão entretempo de internac¸ãoeevoluc¸ãodoestado nutricional decrianc¸asinternadasemumhospitaluniversitário.Demetra. 2013;8:103---14.
25.Prado RC, Santos PF, Assis EM, Zaban AL. Desnutric¸ão e avaliac¸ão nutricional subjetiva em pediatria. Com Ciencias Saude.2010;21:61---70.
26.Sermet-GaudelusI,Poisson-SalomonA-S,ColombV,Brusset M-C,MosserF,BerrierF,etal.Simplepediatricnutritionalrisk scoretoidentifychildrenatriskofmalnutrition.AmJClinNutr. 2000;72:64---70.
27.EufrásioRE.Avaliac¸ãonutricionalsubjetivaglobalempediatria: Adaptac¸ãoe análise de um questionário [Monografia]. Natal (RN):UniversidadeFederaldoRioGrandedoNorte;2014. 28.GerasimidisK,KeaneO,MacleodI,FlynnDM,WrightCM.A
four-stageevaluationofthePaediatricYorkhillMalnutritionScorein atertiarypaediatrichospitalandadistrictgeneralhospital.Br JNutr.2010;104:751---6.
29.WhiteM,LawsonK,RamseyR,DennisN,HutchinsonZ,SohXY, etal.Asimplenutritionscreeningtoolforpediatricinpatients. JParenterEnteralNutr.2014;20:1---7.
30.CarvalhoFC,LopesCR,VilelaLC,VieiraMA,RinaldiAE,Crispim CA.Traduc¸ãoeadaptac¸ãoculturaldaferramentaSTRONGkids para triagem do risco de desnutric¸ão em crianc¸as hospital-izadas.RevPaulPediatr.2013;31:159---65.
31.KondrupJ,AllisonSP,EliaM,VellasB,PlauthM.ESPEN guide-linesfornutritionscreening2002.ClinNutr.2003;22:415---21. 32.ErkanT.Methodstoevaluatethenutritionriskinhospitalized
patients.TürkPedArs¸.2014;49:276---81.
33.DeVetHC, Eisinga A, RiphagenII, AertgeertsB, PewsnerD, Mitchell R. Chapter 7: searching for studies. In: Deeks JJ, BossuytPM,Gatsonis C,editors.Cochrane handbookfor sys-tematicreviewsofdiagnostictestaccuracyversion1.0.0.The Cochrane Collaboration; 2008. Available from: http://www. srdta.cochrane.org[cited18Jan2014].
34.Menezes AM, Santos IS. Cursode epidemiologia básica para pneumologistas: 4a
parte---Epidemiologia clínica. J Pneumol. 1999;25:321---6.
35.LandisJR,KochGG.Themeasurementofobserveragreement forcategoricaldata.Biometrics.1977;33:159---75.
36.WhitingP,RutjesAW,ReitsmaJB,BossuytPM,KleijnenJ.The developmentofQUADAS:atoolforthequalityassessmentof studiesofdiagnosticaccuracyincludedinsystematicreviews. BMCMedResMethodol.2003;3:1---13.
352 TeixeiraAF,VianaKD
38.MinistériodaSaúde,Brasil,SecretariadeCiência,Tecnologia eInsumosEstratégicos,DepartamentodeCiênciaeTecnologia. Diretrizesmetodológicas:elaborac¸ãoderevisãosistemáticae metanálisedeestudosdeacuráciadiagnóstica.Brasília: Min-istériodaSaúde,SecretariadeCiência,TecnologiaeInsumos Estratégicos,DepartamentodeCiênciaeTecnologia,Ministério daSaúde;2014,v.1.
39.Simões PW. Prevalênciade papilomavírus humano nocâncer de mama e apoio ao diagnóstico de câncer de mama pelas redes bayesianas: revisão sistemática e metanálise [Thesis]. Criciúma (SC):Universidade doExtremoSul Catari-nense;2012.
40.McCarthyH,DixonM,CrabtreeI,Eaton-EvansMJ,McNultyH. ThedevelopmentandevaluationoftheScreeningToolforthe AssessmentofMalnutritioninPaediatrics(STAMPa)foruseby
healthcarestaff.JHumNutrDiet.2012;25:311---8.
41.LamaMoreRA,LópezAM,ÁlvarezMH,ChicanoC,MartínezRG, Ruzafa EL. Validación de una herramienta de cribado nutri-cional para pacientes pediátricos hospitalizados. Nutr Hosp. 2012;27:1429---36.
42.WongS,GrahamA,HariniSP,GrimbleG,ForbesA.Validationof theScreeningToolfortheAssessmentofMalnutritionin Paedi-atrics(STAMP)inpatientswithspinalcordinjuries(SCIs).Spinal Cord.2012;51:424---9.
43.Wonoputri N, Djais JT, Rosalina I. Validity of nutritional screening tools for hospitalized children. J Nutr Metab. 2014;2014:1---6.
44.HuysentruytK,AllietP,MuyshontL, RossignolR, DevrekerT, BontemsP, etal. The STRONGkidsnutritional screeningtool inhospitalizedchildren:avalidationstudy.Nutrition.2013;29: 1356---61.
45.IaredW,ValenteO.Revisõessistemáticasdeestudosde acurá-cia.DiagnTratamento.2009;14:85---8.
46.Joosten KF, Huslt JM. Nutritional screening tools for hos-pitalized children: methodological considerations. ClinNutr. 2014;33:1---5.
47.HechtC,WeberM,GroteV,DaskalouE,Dell’eraL,FlynnD, etal.Diseaseassociatedmalnutritioncorrelateswithlengthof hospitalstayinchildren.ClinNutr.2014;34:53---9.
48.Raslan M, González MC, Dias MCG, Paes-Barbosa FC, Cec-conelloI,WaitzbergDL.Aplicabilidadedosmétodosdetriagem nutricional no paciente hospitalizado. Rev Nutr Campinas. 2008;21:553---61.
49.McCarthyH,McNultyH,DixonM,Eaton-EvansMJ.Screeningfor nutritionriskinchildren:thevalidationofanewtool.JHum NutrDiet.2008;21:395---6.
50.Ferreira AC. Caracterizac¸ão Nutricional de Crianc¸as e Ado-lescentescomdiagnósticodedoenc¸aoncológica. Porto(PO): UniversidadedoPorto;2012.
51.MoeeniV,WallsT,DayAS.Assessmentofnutritionalstatusand nutritionalriskinhospitalisedIranianchildren.ActaPaediatr. 2012;101:446---51.
52.SeckerDJ,JeejeebhoyKN.Subjectiveglobalnutritional assess-mentforchildren.AmJClinNutr.2007;85:1083---9.
53.MoeeniV,WallsT,DayAS.Nutritionalstatusandnutritionrisk screeninginhospitalizedchildreninNewZealand.Acta Paedi-atr.2013;102:419---23.
54.LingRE,HedgesV,SullivanPB.Nutritionalriskinhospitalised children:anassessmentoftwoinstruments.ESpenEurEJClin NutrMetab.2011;6:153---7.
55.CaoJ,PengL,LiR,ChenY,LiX,MoB,etal.Nutritionalrisk screeninganditsclinicalsignificanceinhospitalizedchildren. AmJClinNutr.2014;33:432---6.