www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Laryngoscopy
evaluation
protocol
for
the
differentiation
of
essential
and
dystonic
voice
tremor
夽
,
夽夽
Bruno
Teixeira
de
Moraes
a,b,∗,
Noemi
Grigoletto
de
Biase
aaDepartmentofOtorhinolaryngology,HealthSciences,UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil bDepartmentofOtorhinolaryngology,UniversidadeFederaldePernambuco(UFPE),Recife,PE,Brazil
Received21July2014;accepted3February2015 Availableonline3December2015
KEYWORDS
Tremor;
Essentialtremor; Dystonia; Laryngoscopy
Abstract
Introduction:Althoughsyndromesthatcausevoicetremorhavesingularcharacteristics,the differentialdiagnosisofthesediseasesisachallengebecauseoftheoverlap oftheexisting signsandsymptoms.
Objective:Todevelopatask-specificprotocoltoassessvoicetremorbymeansof nasofibro-laryngoscopyandtoidentifythosetasksthatcandistinguishbetweenessentialanddystonic tremorsyndromes.
Methods:Cross-sectional study. The transnasal fiberoptic laryngoscopy protocol, which consistedoftheassessmentofpalate,pharynxandlarynxtremorduringtheperformanceof severalvocalandnon-vocaltaskswithdistinctphenomenologicalcharacteristics,wasapplied to19patients withvoicetremor.Patientswerediagnosedwithessentialordystonictremor accordingtothephenomenologicalcharacterizationofeachgroup.Oncetheywereclassified, thetasksassociatedwiththepresenceoftremorineachsyndromewereidentified.
Results:Thetasksthatsignificantlycontributedtothedifferentialdiagnosisbetweenessential anddystonic tremor were /s/ production, continuous whistlingand reductionoftremor in falsetto.Thesetaskswerephenomenologicallydifferentwithrespecttothepresenceoftremor inthetwosyndromes.
夽
Pleasecitethisarticleas:deMoraesBT,deBiaseNG.Laryngoscopyevaluationprotocolforthedifferentiationofessentialanddystonic
voicetremor.BrazJOtorhinolaryngol.2016;82:88---96.
夽夽
Institution:DepartmentofOtorhinolaryngologyandHeadandNeckSurgery,UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,
SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](B.T.deMoraes). http://dx.doi.org/10.1016/j.bjorl.2015.11.001
Conclusion: Theprotocolofspecifictasksbymeansoftransnasalfiberopticlaryngoscopyisa viablemethodtodifferentiatebetweenessentialanddystonicvoicetremorsyndromesthrough thefollowingtasks:/s/production,continuouswhistlingandreductionoftremorinfalsetto. © 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Tremor;
Tremoressencial; Distonia;
Laringoscopia
Protocolodeavaliac¸ãoporlaringoscopiaparadiferenciartremorvocalessencial edistônico
Resumo
Introduc¸ão: Apesardehavercaracterísticasprópriasentreassíndromescausadorasdotremor vocal, odiagnóstico diferencial destas doenc¸as é um desafio pela sobreposic¸ão de sinaise sintomaspresentes.
Objetivo: Desenvolverprotocolodetarefasespecíficasnaavaliac¸ãodotremorvocalpor nasofi-brolaringoscopia e identificar aquelas que diferenciem as síndromes de tremor essencial e distônico.
Método: Estudotransversal.Oprotocolodenasofibrolaringoscopia,queconsistiunaavaliac¸ão dotremorempalato,faringeelaringeduranteexecuc¸ãodediversastarefasfonatóriase não-fonatórias comcaracterísticas fenomenológicasdistintas, foiaplicadoem 19 pacientescom tremorvocal.Ospacientesforamdiagnosticadoscomotremoressencialoudistônicoapartir dacaracterizac¸ãofenomenológicadecadagrupo.Umavezclassificados,determinou-sequais tarefasestavamassociadasàpresenc¸adetremornasdiferentessíndromes.
Resultados: As tarefas que contribuíram significativamente na distinc¸ão do tremor essen-cial edistônico foramaemissão/s/, assobiocontínuo ereduc¸ãodotremor noagudo,pois apresentaram-sefenomenologicamentediferentesquantoàpresenc¸adotremorentreasduas síndromes.
Conclusão:Oprotocolodetarefasespecíficaspornasofibrolaringoscopiaéummétodoviável para diferenciaras síndromes de tremor vocalessencial e distônico por meio das tarefas: emissão/s/,assobiocontínuoereduc¸ãodotremornoagudo.
©2015Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Voice tremor can be present in defined syndromes when it is associated with other neurological signs (especially for limbs and head), or it is frequently described as an isolated voice tremor when the voice tremor is the only manifestation.1Consideringthephenomenology,thetremor
can be present at rest or with action depending on the conditions present when the tremor occursand the main clinical data that contribute to the syndromic diagnosis. Thisdescriptionalsoappliestothephonatoryapparatusand canbeevaluatedbymeansofnasofibrolaryngoscopy,which allowsa functionalassessment duringthe performanceof severaltasks.2
Among the neurological syndromes with possible voice tremormanifestations,essential tremorismost prevalent followed by Parkinsonian tremor and dystonic tremor.3,4
Despitebeingarelativelycommonentity,somecaseseries show that Parkinson’s disease rarely exhibits a laryngeal tremor.5,6Consideringthattremoratrestisphysiologically
andclinicallydifferentfromtheothers,thegreatest diag-nosticdifficultyliesindistinguishingbetweenessentialand dystonictremor.7
Essentialtremorpresentswithvocaldisordersin11---30% ofcases.5,8,9Therhythmicoscillationofthepalate,pharynx
or larynxmay bepresent during alltasks, includingquiet breathingandspeech,becausethesearetheactivitiesthat requirethemaintenanceof adefinitelaryngeal posture10;
however,the possibility of relaxing the laryngeal muscles duringquietbreathingisquestionable.11
KoufmanandBlalock(2004)12proposedaclassificationof
laryngealdystonia,inwhichtheydescribedystonictremor asavariationoftheadductorlaryngealdystonia, wherein glottalhyper-adductions arerhythmic. It differs fromthe essentialtremor,asitistypicallymorefocal(usuallywithout theinvolvementofotherbodystructures)andtask-specific, sinceitdependsonphonatoryactivityfor itsonset,andis absentduringquietbreathing.
Although there are specific characteristics among the syndromesthatcausevoicetremor,thereisnosufficiently specificdiagnosticmethodbywhich todifferentiatethese diseasesbecauseoftheiroverlap ofsignsandsymptoms.5
theanalysisofthetremoranditsclinicalcharacterization. Thus,oneofthehypothesesofthisstudyisthatthepresence oftremorinthephonatoryapparatusduringthe/s/ produc-tiontask can differentiate the essential (present tremor) fromthedystonicvoicetremor(absenttremor)syndromes, assumingthatthisisanon-phonatorytask(production with-outvocalfoldvibration)andthatthedystonicvoicetremor is task-dependent with tremor manifestation only during speech. It would differ from the essential voice tremor, whichexhibitsthetremorinanyactionwithposture main-tenance.
The objective of this study is to develop a protocol of specific tasks for the evaluation of vocal tremor by nasofibrolaryngoscopy and to identify the tasks that phe-nomenologically differentiate the syndromes of essential anddystonictremor.
Method
Caseseries
AfterapprovalbytheInstitutionalEthicsCommitteeunder protocolnumber1853/10andthefreeandinformedwritten consent,this cross-sectional study included subjects with voicetremortreatedattheneurolaringologysectorofa uni-versityhospital.Patientassessmentincludedclinicalhistory, generalphysicalandheadandneckexamination, auditory-perceptualassessment of voiceand nasofibrolaryngoscopy evaluationwithspecifictaskprotocol.
Inclusion criteria: (a) patients aged 18 and older; (b)tremblingvoiceintheauditory-perceptualassessment; (c)tremorofthephonationdevicestructuresidentifiedat nasofibrolaryngoscopy;(d)voicetremorcomplaintforover ayear;(e)absenceofperiodsofcompleteremissionofvoice tremor.
Exclusion criteria: (a) treatment of the tremor or use ofantihypertensivebeta-adrenergicblockersinthepastsix months;(b) laryngealparalysis ormorphologicallesionsin thephonatoryapparatus;(c)signsofParkinson’sor cerebel-lardisease;(d)thyroidhormonealteration.
Specifictaskprotocol
Thenasofibrolaryngoscopywasperformedwiththepatient in the sitting position with no topical anesthesia. Three anatomic subsites (palate, pharynx and larynx) were observedduringthefollowingspecifictasks:prolonged pro-ductionof phonemes(/é/,/i/,/s/, /z/), quiet breathing andcontinuouswhistling.Thetasks wereevaluatedfor at least5s.Phonemeswereproducedusingpitchandintensity thatwerecomfortableforthepatient,withtheexception of /i/, which was produced in falsetto. The tests lasted an averageof 2min and werecarried outwitha KayPEN-TAXFNL-15RP3flexibleendoscopeundercontinuoushalogen lighting,connectedtoaTOSHIBAIK-CU44Acamcorderand recordedindigitalvideosystem.
Visual---perceptualassessmentoftremor
The video images of nasofibrolaryngoscopy tests were editedinordertoidentifyeachspecifictaskperformedand removetheaudiotracktoreducetheobservationbias.The visual---perceptualanalysis of the videos, omittingpatient identification, was performed through the consensus of three otorhinolaryngologist examiners with experience in neurolaringology. The evaluators were instructed to: (1)assessthepresenceorabsenceoftremorateachsubsite evaluated for each of the proposed tasks of the study; (2)identifywhethertherewasareductionintheintensity or disappearance of tremorin the /i/ task in falsetto in relation tothe/é/task(forevaluationpurposesitwillbe called tremor reduction in falsetto task). There were no limitsastotherepetitionofthevideosfortheexaminer’s assessment.
The criteria used to consider the presence of tremor were:(a)tremoronthepalate---rhythmicoscillationofthe
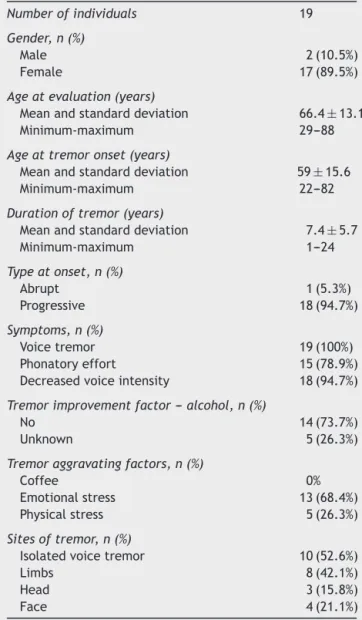
Table 1 Descriptive analysis of the clinical and demo-graphic characteristicsofindividualswithvoice tremorin theassessedsample.
Numberofindividuals 19
Gender,n(%)
Male 2(10.5%)
Female 17(89.5%)
Ageatevaluation(years)
Meanandstandarddeviation 66.4±13.1 Minimum-maximum 29---88
Ageattremoronset(years)
Meanandstandarddeviation 59±15.6 Minimum-maximum 22---82
Durationoftremor(years)
Meanandstandarddeviation 7.4±5.7
Minimum-maximum 1---24
Typeatonset,n(%)
Abrupt 1(5.3%)
Progressive 18(94.7%)
Symptoms,n(%)
Voicetremor 19(100%)
Phonatoryeffort 15(78.9%) Decreasedvoiceintensity 18(94.7%)
Tremorimprovementfactor---alcohol,n(%)
No 14(73.7%)
Unknown 5(26.3%)
Tremoraggravatingfactors,n(%)
Coffee 0%
Emotionalstress 13(68.4%) Physicalstress 5(26.3%)
Sitesoftremor,n(%)
Isolatedvoicetremor 10(52.6%)
Limbs 8(42.1%)
Head 3(15.8%)
Table2 Descriptionofthesyndromicclassificationofpatientsaccordingtothepresenceofhorizontaltremorofthelarynxat /s/production.
Horizontaltremorofthelarynxat/s/production
No Yes
Numberofindividuals 7 12
Syndrome Dystonictremor Essentialtremor
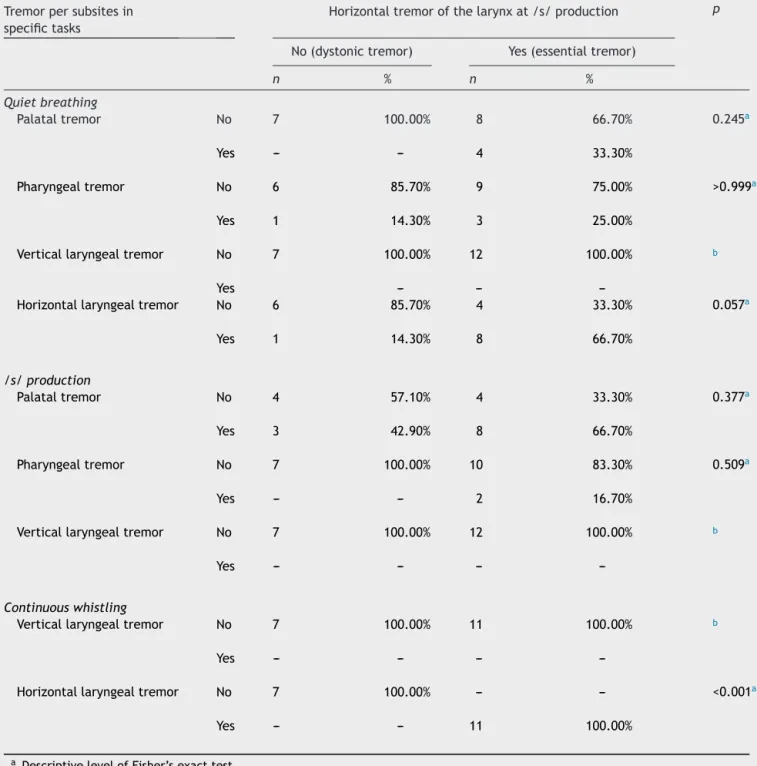
Table3 Associationoftheessentialanddystonictremorsyndromeswiththepresenceoftremorpersubsitesinnon-phonatory tasks.
Tremorpersubsitesin specifictasks
Horizontaltremorofthelarynxat/s/production p
No(dystonictremor) Yes(essentialtremor)
n % n %
Quietbreathing
Palataltremor No 7 100.00% 8 66.70% 0.245a
Yes --- --- 4 33.30%
Pharyngealtremor No 6 85.70% 9 75.00% >0.999a
Yes 1 14.30% 3 25.00%
Verticallaryngealtremor No 7 100.00% 12 100.00% b
Yes --- ---
---Horizontallaryngealtremor No 6 85.70% 4 33.30% 0.057a
Yes 1 14.30% 8 66.70%
/s/production
Palataltremor No 4 57.10% 4 33.30% 0.377a
Yes 3 42.90% 8 66.70%
Pharyngealtremor No 7 100.00% 10 83.30% 0.509a
Yes --- --- 2 16.70%
Verticallaryngealtremor No 7 100.00% 12 100.00% b
Yes --- --- ---
---Continuouswhistling
Verticallaryngealtremor No 7 100.00% 11 100.00% b
Yes --- --- ---
---Horizontallaryngealtremor No 7 100.00% --- --- <0.001a
Yes --- --- 11 100.00%
softpalate;(b) tremorin pharynx---rhythmicconstriction of the pharyngeal wall; (c) vertical laryngeal tremor ---rhythmicoscillation of the larynxin the vertical plane in relationtothesurroundingaerodigestivetract;(d) horizon-taltremorofthelarynx---rhythmicoscillationofthevocal folds,vestibularfoldsorarytenoidsinthehorizontalplane. To identifyspecific tasks relatedtotremorsyndromes, initiallythepatientswereclassifiedashavingessentialand dystonic tremor according to the presence of horizontal tremorof thelarynx during the/s/ production,and then this task was combined with others (phonatory and non-phonatory),basedonthe assessmentsmade by consensus amongthethreeexaminers.
Statisticalanalysis
In the descriptive analysis of the sample characteristics, the mean, minimum value, maximum value and standard deviation were calculated for numeric variables; for the categoricalvariables,theabsoluteandrelativefrequencies were calculated. Fisher’sexact test was used toidentify associationsbetweencategoricalvariablesoftheprotocol. The˛significancelevelof5%wasusedfortheconclusions
obtainedthroughtheinferentialanalyses.
Results
Table1summarizesthemainclinicalanddemographic char-acteristicsofthestudysample.
The 19 individuals included in the study performed the protocol tasks adequately, except for one patient who failed to perform the continuous whistling. Through the information collected from the visual---perceptual assessment of the tremor by consensus among the three examiners, 12patients were classifiedas havingessential tremor and seven as dystonic tremor, according to the presenceor absenceof horizontaltremorofthe larynxin the/s/productiontask(Table2).
Whenstudyingtheassociationbetweenhorizontaltremor ofthelarynxinthe/s/productionandnon-phonatorytasks (Table3),atrendwasidentifiedthattheindividualclassified ashavingessentialtremormoreoftenexhibitedhorizontal tremorofthelarynxinthequietbreathingtask(p=0.057). The horizontaltremorof thelarynx inthe /s/ produc-tionwasstronglyassociatedwithhorizontaltremorofthe larynx in the continuous whistling task (p<0.001). In the selectedsample, the 11 individuals classified asessential tremor(exceptonewhofailedto performthecontinuous whistlingtask)had horizontaltremorof the larynxin the continuouswhistlingtask.
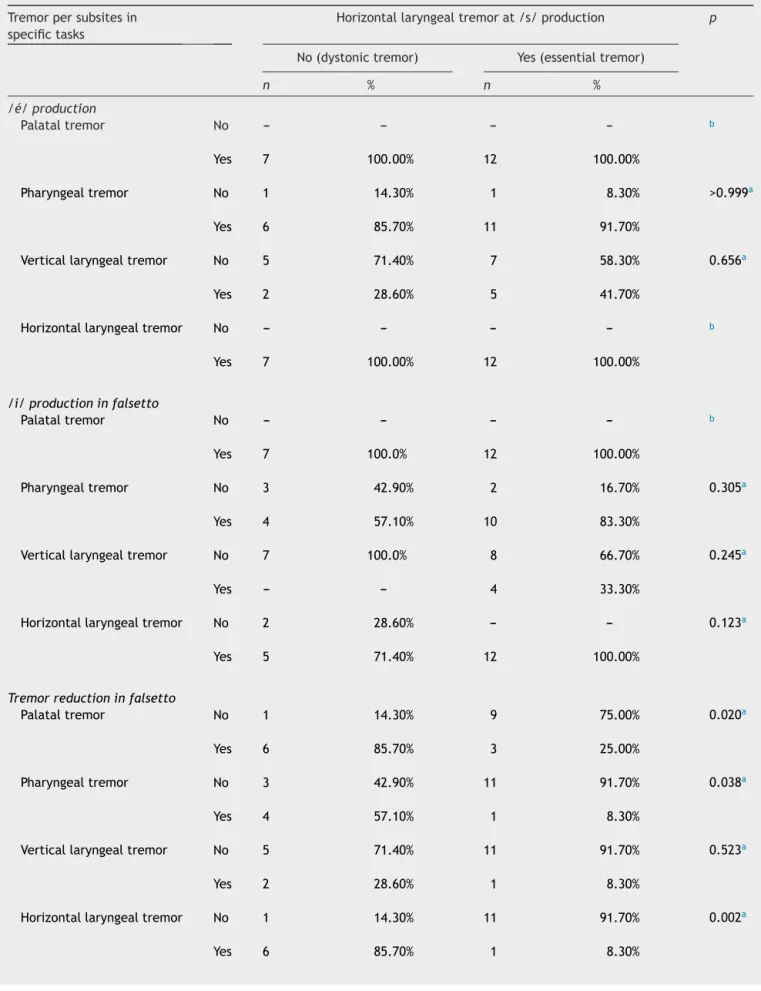
Comparing the phonatory tasks and the horizontal tremorof the larynx in the /s/ production (Table 4), we observed that a reduction of tremor in falsetto in the palate(p=0.020),pharynx(p=0.038)andhorizontallarynx (p=0.002)wasmorefrequentinpatientsclassifiedashaving dystonictremor.Nootherphonatorytaskcoulddifferentiate theessentialfromthedystonictremor.
Discussion
Despite the advances in neurolaringology, the distinction between theessential and dystonic voicetremor remains
challenging, and this directly impacts the choice among the several types of treatment. For this differentiation, several research methods have been used, among them the auditory-perceptual voice assessment, the transnasal fiberoptic laryngoscopy (nasofibrolaryngoscopy), acoustic measurements and larynx electromyography.10,13,14 The
common aspect of these assessments is that they usually searchforparticularitiesineachsyndromeduringphonatory tasks(soundproductionwithvocalfoldvibration),precisely the activityat which thediseases aremost similar.Based on this observation, we tried to identifyamong different phonatoryandnon-phonatorytasks(non-vocalproductions withoutvocalfoldvibration)theonesthatcanrepresentthe phenomenology of tremorappliedtothephonatory appa-ratus, bydefinition,thebasic conceptthatdeterminesits syndromicclassification.
The main characteristic of dystonic tremor is that it dependsonaspecifictasktomanifestitself,which,inthe caseofvoicetremor,isphonation.Inthesepatients,by def-inition,thetremorwouldnotbepresentinnon-phonatory situations (productions without vibration of vocal folds), even if there is muscle action to maintain the laryngeal posture, asduring the /s/ production. However, patients withessential tremorhavemuscle tremorwhenit is con-tracted,evenifitisonlytomaintaintheposture.Thus,the tremorinphonatoryapparatuswouldbepresentduringany activitywherethereisposturemaintenance,regardlessof phonationand,therefore,duringthe/s/production.Thus, the/s/productiontask,whichrepresentsanon-vocal frica-tivephonemewithoutvocalfoldvibration,appearstobea watershedbetweenthese twosyndromes, sinceduringits performancepatientswithdystonictremorwouldnothave tremor,whilepatientswithessentialtremorwouldmanifest it.Therefore,thistaskwaschosentoassessvariationsand differentiatepatients,classifyingthemashavingessential tremorsyndromeordystonictremorsyndrome,andalsoto identifyassociationsbetweenthesyndromesandtheseveral protocoltasks(Table2).
There is still no consensus on the muscle activity of the larynx during quiet breathing. According to a neuro-laringologycommitteereportoftheAmericanAcademy of Otolaryngology --- Head and Neck Surgery,10 during
respi-ration or phonation there is no real rest in the larynx. Theseactivitiesarebestdefinedasposturalmaintenance, which explains the presence of oscillation of the laryn-gealstructuresinessentialtremor.Duringquietbreathing, horizontal tremorofthe larynxwasidentifiedin 66.7% of individualsinthepresentcaseseries,classifiedasessential tremor(Table 3).Despite the controversy,basedon elec-tromyographic studies in healthy subjects, Hillel (2001)11
demonstratedthattheintrinsicmusclesofthelarynxmay beatrestduringquietbreathing,an observationthatmay explainthe absenceof tremorinonethird ofthese study patients classified as essential tremor. Initially, the pres-enceoftremorinquietbreathingisnotrequiredtodiagnose essential voicetremor,but thisisa signthat suggeststhe diagnosis as described by Koufman and Blalock (2004).12
Oneof thepatients classifiedasdystonic tremoralsohad horizontal tremor of the larynx during breathing, a find-ingthatis notexpectedaccordingtotheliterature,since this is not an activity that triggers dystonic posture.12,15
Table4 Associationofessentialanddystonictremorsyndromeswiththepresenceoftremorpersubsitesinphonatorytasks.
Tremorpersubsitesin specifictasks
Horizontallaryngealtremorat/s/production p
No(dystonictremor) Yes(essentialtremor)
n % n %
/é/production
Palataltremor No --- --- --- --- b
Yes 7 100.00% 12 100.00%
Pharyngealtremor No 1 14.30% 1 8.30% >0.999a
Yes 6 85.70% 11 91.70%
Verticallaryngealtremor No 5 71.40% 7 58.30% 0.656a
Yes 2 28.60% 5 41.70%
Horizontallaryngealtremor No --- --- --- --- b
Yes 7 100.00% 12 100.00%
/i/productioninfalsetto
Palataltremor No --- --- --- --- b
Yes 7 100.0% 12 100.00%
Pharyngealtremor No 3 42.90% 2 16.70% 0.305a
Yes 4 57.10% 10 83.30%
Verticallaryngealtremor No 7 100.0% 8 66.70% 0.245a
Yes --- --- 4 33.30%
Horizontallaryngealtremor No 2 28.60% --- --- 0.123a
Yes 5 71.40% 12 100.00%
Tremorreductioninfalsetto
Palataltremor No 1 14.30% 9 75.00% 0.020a
Yes 6 85.70% 3 25.00%
Pharyngealtremor No 3 42.90% 11 91.70% 0.038a
Yes 4 57.10% 1 8.30%
Verticallaryngealtremor No 5 71.40% 11 91.70% 0.523a
Yes 2 28.60% 1 8.30%
Horizontallaryngealtremor No 1 14.30% 11 91.70% 0.002a
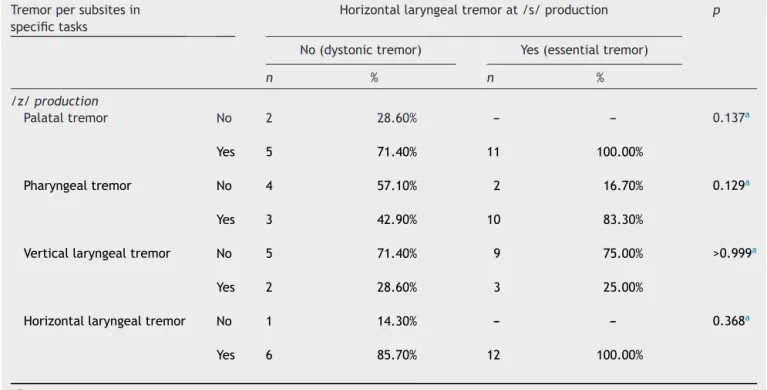
Table4 (Continued)
Tremorpersubsitesin specifictasks
Horizontallaryngealtremorat/s/production p
No(dystonictremor) Yes(essentialtremor)
n % n %
/z/production
Palataltremor No 2 28.60% --- --- 0.137a
Yes 5 71.40% 11 100.00%
Pharyngealtremor No 4 57.10% 2 16.70% 0.129a
Yes 3 42.90% 10 83.30%
Verticallaryngealtremor No 5 71.40% 9 75.00% >0.999a
Yes 2 28.60% 3 25.00%
Horizontallaryngealtremor No 1 14.30% --- --- 0.368a
Yes 6 85.70% 12 100.00%
aDescriptivelevelofFisher’sexacttest. b Nostatisticaltestcanbeapplied.
electromyographyof13patientswithdystonictremor,Hillel (2001)11alsoidentifiedanindividualwhoshowedrhythmic
activityinthismuscleduringquietbreathing.Additionally, arareoccurrencethatrepresents1%ofthecasesof laryn-gealdystonia,isadductorrespiratorydystonia,describedby Blitzeretal.(1998),16inwhichdystonicposturesinthe
lar-ynxarepresentduringbreathing.Therefore,despitebeing quiteunusual,patientswithdystonictremorwhohave hori-zontaltremorofthelarynxduringbreathingcaneventually beidentified.Anotherexplanationforthepresenceof hor-izontaltremorofthelarynxduringbreathinginthispatient classifiedashavingdystonic tremor,isthe possibilityofa mistakenobservationoftremorinthistask,orevenafalse negativeresultinthe /s/production test, andtherefore, thecorrectdiagnosisinthiscasewouldbeessentialtremor. The continuous whistling taskwaschosen for inclusion intheprotocol duetoitsresemblance tothe/s/ produc-tion,that is, it is a non-phonatory taskin which thereis evidentposturemaintenanceinthelarynx.Inthissample, the horizontal larynx tremorduring the whistling showed tobestronglyassociatedwithhorizontaltremorofthe lar-ynxduring the /s/production, with both tasks appearing alwaysequalinrelationtothepresenceoftremor(Table3). This observation confirms that these tasks are actually phenomenologicallysimilarandaddsevidencethatthe pres-enceof tremorin thesesituationsindicatesadiagnosis of essentialtremor.
In 2006, De Biase et al.17 evaluated patients with
adductor laryngeal dystonia using transnasal fiberoptic laryngoscopyandnoneofthesubjectshadspasmswhile per-formingthewhistling.Byunderstandingthedystonictremor as a variant of dystonia, the expectation is that it will
notexhibitdystonicposturing(irregulartremor)duringthe whistling,asitwasdemonstratedinthisstudy,inwhichall patientsclassifiedassuchshowednotremor.Itisimportant toemphasize thattheaccomplishmentof thistaskshould beacontinuouswhistling,becausetheintermittentwhistle isassociatedwithlaryngealstructuremovementthat inter-fereswithtremorperceptionanddoesnotrepresentposture maintenance.
Theliteratureregardingadductorlaryngealdystoniahas evaluatedthe change inthe intensity of spasmsin accor-dancewiththevariationofthepitch;phonationinfalsetto reducesthestimulusfortheoccurrenceofspasms.17
Bark-meierandCase(2000)14 reportedthatthehighpitchhasa
directinfluenceonthereductionofthevoicetremor mag-nitude,andthisisduetotheseparationofthevocalfolds. Almostallofpatientsinthepresentstudy,bothinthe/é/ productionasinthe/i/productioninfalsetto,showed hor-izontaltremorofthelarynxwithnostatisticallysignificant differences between the tasks,demonstrating that, when isolated,theydonot differentiatethe tremorsyndromes. Amongpatientsclassifiedasessentialtremor,91.7%hadno change in tremorwhenassessedin tasks withnormal and highpitch.However,casesofdystonictremorexhibited sig-nificantreductionoftremorinthe/i/productioninrelation tothe/e/production(Table4).Therefore,asthe/é/ pro-ductionis emittedwiththevocalfoldsin closerproximity thanwith/i/productioninfalsetto,themoreabductedare thevocalfolds,thesmallerthefluctuationsinpatientswith dystonictremor.
duringthisactivity(Table4).Despitethesimilaritybetween /z/ and /s/ productions, since they are fricative conso-nantsproducedinthesamearticulationpoint(tongueand palate),theydifferfromeachother, asthefirstoccursin adductionwithparticipationofvocalfoldvibration (phona-toryorsound),whereastheotherdoesnot(non-phonatory). This singledifferencejustifies theimportanceofphonetic composition in the diagnosis of dystonic tremor, as the oscillationoccursinsoundtasksandis absentduring non-phonatorytasks.Evidenceofsimilarspecifictaskisfoundin patientswithadductorlaryngealdystonia,whichmanifests symptomsworseninginsentenceswithsonorousconsonants (b,d, g,v,j,z, m,n)andimprovementinsentenceswith non-phonatoryconsonants(p,t,k,f,s,ch).18,19Incasesof
essentialtremor,theoscillationisindependentfromthetask (sonorousorsilent).20
Unlikedystonia,essentialvoicetremorusuallypresents asamorewidespreaddiseasemanifestation,inwhich the tremorisnotrestrictedtotheintrinsicmusclesofthelarynx andmayinvolvethepalate,pharynx,tongueand articula-torymuscles.10However,inthissample,boththepalateand
thepharynxdemonstratedthepresenceoftremorinseveral tasks, withno significant difference between the groups, demonstratingthatthesimplepresenceoftremorin extrala-ryngealsubsitesdoesnotdifferentiatesyndromes.Eventhe laryngeal vertical oscillation,suggesting tremorof extrin-siclaryngealmuscles,21 whichwasexpectedtobepresent
especially in cases of essential tremor, was not specific either(Tables3and4).Thisfactcouldrepresenta segmen-tal,ratherthanfocalinvolvementinpatientswithdystonic voice tremor. However,in the subsites of the palate and pharynx,the onlyassociation found wastremorreduction in falsetto in patients with acute dystonic tremor, simi-lar to what occurred with the horizontal tremor of the larynx.Therefore, it ispossible that thetremorobserved in the palate and pharynx of these patients is not a pri-marydystonicalterationofthismusculature,butsecondary toalaryngeal subsystemdysfunction,asthetremor mod-ulation in all structures was directly influenced by the transition between normaland acute pitch,an eminently laryngealfunction.This observationindicatesthe possibil-ity of an interactionbetween the central nervoussystem as the tremor generator and the peripheral neuromuscu-lar system, since a probable modulation in the afferent system ends up modifying the tremor in both the larynx and in other structures, such asthe palate and pharynx. Thesehypothesesarerelatedspecificallytodystonictremor, as oscillation modulation was not identified in essential tremor.
The absence of a gold-standard assessment for vocal tremor analysismakes it difficult to assess the reliability of this proposed protocol. As previously discussed, there is a possibilityof diagnostic error in this assessment, for instance, the presence of false negativeor false positive resultsintheexamination,andthereforeoneshouldavoid establishingadiagnosisbasedonthetremorrepresentation in a single task. To obtain greater reliability when defin-ing the nosological entity in question, the latter should bedeterminedonlywhenthetremormanifestationin dif-ferenttasks phenomenologically corresponds to the same tremorsyndrome.Incaseswherethetremormanifestation intheseveraltasksdoesnotpointtothesamesyndrome,
the implementationofthisprotocolbecomeslessreliable fordiagnosticdefinition.
Although it seems arbitrary to syndromically classify voicetremorby thepresence of horizontaltremorof the larynx in the /s/ production, it is justified by the phen-omenological basis demonstrated in this study and the associationsfound intheseveraltasks,whichpartly repli-cate the characteristics traditionally described for each disease.Therefore, thedistinction betweenessential and dystonicvoicetremorseemstobefeasible,providedthat adequateevaluationisperformed,includinganassessment ofthephonatoryapparatusby transnasalfiberoptic laryn-goscopy,especiallyduring non-phonatory tasks.Moreover, basedonhigherdiagnosticaccuracy,itispossiblethat spe-cifictreatmentstargetedforeachtypeoftremormayallow abettertherapeuticresponse.
Conclusion
The protocol of specific tasks during transnasal fiberoptic laryngoscopyis a viable method todifferentiate between essentialanddystonicvoicetremorsyndromes.Taskswith significant importancefor this differentiation are the /s/ production,continuouswhistlingandobservationofreduced tremorinfalsetto.
Funding
sources
This study was supported by Coordenac¸ão de Aperfeic¸oamentodePessoaldeNívelSuperior---CAPES.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.DeuschlG,BainP,BrinM.ConsensusstatementoftheMovement DisorderSocietyonTremor.AdHocScientificCommittee.Mov Disord.1998;13:2---23.
2.KoufmanJA. Approach to thepatient witha voice disorder. OtolaryngolClinNorthAm.1991;24:989---98.
3.Deuschl G. Differentialdiagnosis oftremor.J NeuralTransm Suppl.1999;56:211---20.
4.ShuklaG, BehariM.Aclinicalstudyofnon-parkinsonian and non-cerebellartremorataspecialtymovementdisordersclinic. NeurolIndia.2004;52:200---2.
5.FindleyLJ,GrestyMA.Head,facial,andvoicetremor.Adv Neu-rol.1988;49:239---53.
6.WolraichD,VasileMarchis-CrisanC,ReddingN,KhellaSL,Mirza N.Laryngealtremor:co-occurrencewithothermovement dis-orders.ORLJOtorhinolaryngolRelatSpec.2010;72:291---4. 7.SchragA,MunchauA,BhatiaKP,QuinnNP,MarsdenCD.
Essen-tialtremor: anoverdiagnosedcondition. JNeurol.2000;247: 955---9.
8.LouJS,JankovicJ.Essentialtremor:clinicalcorrelatesin350 patients.Neurology.1991;41:234---8.
9.KollerWC,BusenbarkK,MinerK.Therelationshipofessential tremortoothermovementdisorders:reporton678patients. EssentialTremorStudyGroup.AnnNeurol.1994;35:717---23. 10.Merati AL, Heman-Ackah YD, Abaza M, Altman KW, Sulica
larynx:areportfromtheneurolaryngologycommitteeofthe AAO-HNS.OtolaryngolHeadNeckSurg.2005;133:654---65. 11.Hillel AD. The study of laryngeal muscle activity in
nor-mal humansubjects and in patientswithlaryngeal dystonia using multiple fine-wire electromyography. Laryngoscope. 2001;111:1---47.
12.Koufman JA, Blalock PD. Classification of laryngeal dysto-nias[Internet].NorthCarolina:CenterforVoiceDisordersof Wake Forest University; 2004. Available from: http://www. thevoicecenter.org/classld.html[cited08.08.04].
13.AronsonAE,HartmanDE.Adductorspasticdysphoniaasasignof essential(voice)tremor.JSpeechHearDisord.1981;46:52---8. 14.BarkmeierJM,CaseJL.Differentialdiagnosisofadductor-type
spasmodicdysphonia,vocaltremor,andmuscletension dyspho-nia.CurrOpinOtolaryngolHeadNeckSurg.2000;8:174---9. 15.BlitzerA,LovelaceRE,BrinMF,FahnS,FinkME.
Electromyo-graphicfindingsinfocallaryngealdystonia(spasticdysphonia). AnnOtolRhinolLaryngol.1985;94:591---4.
16.Blitzer A,Brin MF, StewartCF.Botulinum toxin management ofspasmodicdysphonia(laryngealdystonia):a 12-year expe-rience in more than 900 patients. Laryngoscope. 1998;108: 1435---41.
17.DeBiaseNG,LorenzonP,LeblMD,PadovaniM,GielowI,Madazio G,etal.Adductionlaryngealdystonia:proposalandevaluation ofnasofibroscopy.BrazJOtorhinolaryngol.2006;72:443---6. 18.EricksonML.Effectsofvoicingandsyntacticcomplexityonsign
expressioninadductorspasmodicdysphonia.AmJSpeechLang Pathol.2003;12:416---24.
19.RoyN,GouseM,MauszyckiSC,MerrillRM,SmithME.Task speci-ficityinadductorspasmodicdysphoniaversus muscletension dysphonia.Laryngoscope.2005;115:311---6.
20.Sulica L, Louis ED. Clinicalcharacteristicsof essential voice tremor:astudyof34cases.Laryngoscope.2010;120:516---28. 21.KodaJ,LudlowCL.Anevaluationoflaryngealmuscle