www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
The
sphenoid
sinus,
foramen
rotundum
and
vidian
canal:
a
radiological
study
of
anatomical
relationships
夽
Alireza
Mohebbi,
Shahin
Rajaeih
∗,
Mahdi
Safdarian,
Parisa
Omidian
IranUniversityofMedicalSciences,DepartmentofOtolaryngology,HeadandNeckSurgery,Tehran,Iran
Received10March2016;accepted14April2016 Availableonline24May2016
KEYWORDS Foramenrutundum; Sphenoidsinus; Vidiancanal
Abstract
Introduction:Thesphenoidsinusisanimportantstructureinventralskullbasesurgeriesthatis surroundedbyseveralvitalanatomicalstructuresincludingtheinternalcarotidarteries,optic nerveandcranialnervesinsidethecavernoussinus. Inaddition,theforamenrotundumisa smallcanaldeeplysituatedinthebaseoftheskull,whichrepresentsthewayforexitofthe maxillarynerve.Understandingofthesphenoidboneanatomicalrelationshipsiscentraltothe expandedendonasalapproachestotheskullbase.
Objective: Torecordandanalyzethemeasurementindexesofthesphenoidsinusandforamen rotunduminthecoronalplaneofnormalcomputertomographyscans.
Methods:PatientsunderwentparanasalsinusescomputertomographyscanfromJune2014to November2015wereretrospectivelyenteredthiscross-sectionalstudy.Weobtainedseveral morphometricmeasurementsfromboththerightandleftsidesusingcomputersoftware.We alsoclassifiedforamenrotundumandvidiancanaltypesanddeterminedpositionoftheforamen rotundumregardingtobaseoflateralpterygoidplate.
Results:One-hundredpatients withthemeanageof38.56±18.51 yearsenteredthisstudy. MeanbilateralFRdistanceswere38.48±3.87mm.AveragerightandleftFRsdistancesto mid-linewere19.00±2.07and19.34±2.17mm,respectively(p=0.03).Twenty-eightcases(28%) hadtypeIvidiancanal,48%and24%hadtypeIIandIIIvidiancanals,respectively.Fourpatients (4%)hadtypeIrotundumforamen,28%and44%hadtypeIIaandIIb,respectivelyand24%had typeIIIrotundumforamen.Thepositionofforamenrotundumsregardingtothebaseoflateral pterygoidplatewasonlinein50%ofcases,mediallyplacedin47%andlaterallyplacedin3%of cases.
Conclusion: Theresultsofthisstudycanbeusedtoprovideabetteranatomicalunderstanding ofthearea,whichisnecessaryforendoscopicskullbasesurgeons.
© 2016 Publishedby Elsevier Editora Ltda. onbehalf of Associac¸˜ao Brasileira de Otorrino-laringologiaeCirurgiaC´ervico-Facial.ThisisanopenaccessarticleundertheCCBYlicense (http://creativecommons.org/licenses/by/4.0/).
夽 Pleasecitethisarticleas:MohebbiA,RajaeihS,SafdarianM,OmidianP.Thesphenoidsinus,foramenrotundumandvidiancanal:a radiologicalstudyofanatomicalrelationships.BrazJOtorhinolaryngol.2017;83:381---7.
∗Correspondingauthor.
E-mail:[email protected](S.Rajaeih).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCervico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.04.013
PALAVRAS-CHAVE Forameredondo; Seioesfenoidal; Canalpterigoideo
Seioesfenoidal,forameredondoecanalpterigoideo:estudoradiológicodasrelac¸ões
anatômicas
Resumo
Introduc¸ão:Oseioesfenoidal(SE)éumaestruturaimportanteemcirurgiasdabasedocrânio, queestácercadaporváriasestruturasanatômicasvitais,comoasartériascarótidasinternas,o nervoópticoeosnervoscranianosnointeriordoseiocavernoso.Alémdisso,oforameredondo (FR)éumpequenocanalprofundamentesituadonabasedocrânio,querepresentaaformade saídadonervomaxilar.Compreenderasrelac¸õesanatômicasdoossoesfenoidaléfundamental paraasabordagensendonasaisexpandidasdabasedocrânio.
Objetivo:Registrareanalisar osíndicesdemedic¸ãodoSEeFRnoplanocoronaldeexames normaisdeTC.
Método: OspacientesqueforamsubmetidosaTCdosseiosparanasais(SPN)dejunhode2014a novembro2015foramretrospectivamenteincluídosnesteestudotransversal.Obtivemosvárias medidasmorfométricasdeambososladosdireitoeesquerdousandosoftwaredecomputador. TambémclassificamosostiposdeFRecanalpterigoideo(CP)edeterminamosaposic¸ãodoFR emrelac¸ãoàbasedaplacapterigoidelateral.
Resultados: Cempacientescomamédiadeidadede38,56±18,51anosforamincluídosneste estudo.AsdistânciasmédiasbilateraisdeFRforamde38,48±3,87milímetros.Asdistâncias médiasdireitaeesquerdadosFRatéalinhamédiaforamde19,00±2,07e19,34±2,17mm, respectivamente(p=0,03).Vinteeoitocasos(28%)tinhamcanalpterigoideodotipoI,48%e 24%canaispterigoideosdetipoIIeIII,respectivamente.Quatropacientes(4%)tinhamforame redondodotipoI,28%e44%dotipoII-aeII-b,respectivamente,e24%forameredondodotipo III.Aposic¸ãodosFRemrelac¸ãoàbasedaplacapterigoidelateraleraemlinhaem50%dos casos,medialmenteposicionadosem47%elateralmenteposicionadosem3%doscasos.
Conclusão:Osresultadosdesteestudopodemserutilizadosparapromoverumamelhor com-preensãoanatômicadaárea,necessáriaparacirurgiasendoscópicasdabasedocrânio. ©2016Publicado porElsevier EditoraLtda.em nome deAssociac¸˜ao Brasileirade Otorrino-laringologia eCirurgiaC´ervico-Facial.Este ´eum artigo OpenAccess sobuma licenc¸aCC BY (http://creativecommons.org/licenses/by/4.0/).
Introduction
The sphenoid sinus (SS) is an important structure in ven-tralskullbase surgeriesthat isnotonly thenatural route for access to the sellar, parasellar, suprasellar and clival regions, but also a path of access to Meckel’s cave and themiddle cranial fossa. It is surrounded by severalvital anatomicalstructuresincludingtheinternal carotid arter-ies, optic nerve and cranial nerves inside the cavernous sinus. The surgical window to the middle cranial fossa is locatedinthepterygoidbodyofthesphenoidbone.1
The SS is present as a small cavity at birth, but its maindevelopmenttakesplaceafterpuberty.Inearlylife, it extends posteriorly into the presellar area and subse-quentlyexpandsintothe areabelowandbehindthesella turcica, reaching its full size during adolescence. As the sinus enlarges, it maypartially encircle the optic canals. When thesinus is exceptionally large, itextends intothe rootsofthepterygoidprocessesorgreaterwingofthe sphe-noidboneandmayevenextendintothebasilarpartofthe occipitalbone.Inthewell-pneumatizedSS,onlyathinlayer ofbone mayseparatethesinusfromimportantcontiguous structures.Thecloseproximityoftheseneurovascular struc-tureswithpotentiallyverythinbonyseparationorevenbony dehiscencecontributestotheclinicalimportanceofthese anatomicalrelationships.
Few studies used thin-cut (1mm) CT data to study the pneumatization of the lateral sphenoid or pterygoid recess.2,3The emergenceof endoscopicskullbase surgery
asanacceptedsurgicalmodalityoverthepastyearshasled tonewchallengeswithrespecttogainingabetter under-standing of the endonasal anatomyof the area. As such, new paradigms of anatomical relationships have evolved into instrumental landmarksto the endoscopic skullbase surgeon.4
Alongside the past development of endoscopic sinus surgery, knowledge about theanatomy of the sinuses has become crucial for surgeons. The SS is one of the most variable of all sinuses. Its relations to vital vascular and nervouselementsmakeitsapproachachallengefor endo-scopicsurgeons.5 Inaddition,theforamen rotundum(FR),
is a smallcanal deeply situated in the base of the skull, whichrepresentsthewayforexitofthesecond branchof thetrigeminalnerve(maxillarynerve).6Itsmedialborderis
formed bylateral wallofSS andruns downwardsand lat-erallyinanobliquepathandjoinsthemiddlecranialfossa withthepterygopalatinefossa.7
IndividualizationandanalyzeofSSisdifficultand necessi-tatesapreciseandadaptedtechnique,aswellasknowledge ofitspropertiesanatomicalrelationships.6Itsinvolvement
modifiestheprognosisofthediseaseandnecessitatea mul-tidisciplinarytherapeuticdiscussion.6Impressionscausedby
neurovascular coursing provide several important surgical landmarksfor locating thesevital structuresandavoiding theirinjury.8 Understandingofthesphenoidbone
anatom-ical relationships is central to the expanded endonasal approachestotheskullbase.4
Eventhoughcomputertomography(CT)openedthenera ofdetailedmorphologicalstudies,duetolackofsufficient andpreciseliteratureinvicinityandpropertiesoftheFR, we designed thisanatomicalstudy to evaluatenormal CT scansofpatients,recordandanalyzedistancesandangles. Thegoalofthisstudywastopresentaclassificationbased onthemeasurementindexesinthecoronalplanethatcan be used to instruct preoperative planning for endoscopic endonasalsurgery.
Methods
Approvalstatementoftheethicscommittee
This studywasapprovedbythe localethicscommitteeof theENT--- Head&Necksurgeryresearchcenterof Hazrat-e-RasoolAkramHospitalwiththeapprovalprotocolnumberof 94-11860.Theinformationofpatientsremainedconfidential andwasonlyusedforresearchpurposes.
Studydesign
This retrospective cross-sectional study was designed on adult patients whounderwent paranasalsinuses (PNS) CT scan (3mm slices thickness) for any reason, from June 2014toNovember2015 inHazrat-e-RasoolAkramHospital (atertiary-caremedicalcenter)Iran Universityof Medical Sciences,Tehran, Iran. Exclusioncriteriaincluded individ-uals younger than 18 years of age or with known skull basepathology includingmaxillofacialfractures,sinonasal tumorsorpolyposis,disruptionoftheskullbaseornotable rhinosinusitis(inflammatorychangesthatprecluded visual-izationofskullbaseanatomy).Foreachincludedpatient,we obtainedmeasurementsfromboth therightandleftsides usingMacroPACSsoftwareinbothaxialandcoronalplanes. The firstcoronal imagesection at which both theVC and FRwerevisualizedwaschosenforthequantitativeanalysis. This section (as determined onaxial andsagittal images) wasusuallyatthemidpointofsphenoidsinus(Fig.1).
Measurements
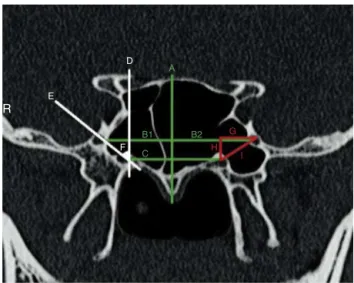
We measuredseveral morphometricparametersaccording toanimaginarymidlineverticaltotherostrum(Fig.2):
DistancebetweenrightandleftFRs; DistancesfrommidlinetorightandleftFRs;
DirectdistancebetweentheVCandtheFRoneachside; Horizontal distance betweenthe VC andthe FRoneach side(distancesbetweentwoverticallinethatintersecting theFRandtheVC);
VerticaldistancebetweentheVCandtheFRoneachside (distancebetweentwohorizontallinethatintersectingthe FRandtheVC).
OC
VC
SS
T
LPtP FR
LR
Rostrum
Figure1 Thecoronalsectionatwhichboththevidiancanal andforamenrotundumarevisualized(usuallyatthemidpoint ofsphenoidsinus).SS,sphenoidsinus;FR,foramenrotundum; VC,vidiancanal;LPtP,lateralpterygoidplate;OC,opticcanal; LR,lateralrecess.
R
E
D
A
B1
C
B2 G
H I
F
Figure 2 Measurement indexes of the study. A, Imaginary midlineverticaltotherostrum;B(1),distancebetweenrightFR tomidline;B(2),distancebetweenleftFRtomidline;C, imag-inaryhorizontallineconnectingtheVCs;D,imaginaryvertical linepassingtheVC;E,imaginarylineconnectingFRtoVC;F,the rotundumanglewiththeverticalline;G,HandI,horizontal, verticalanddirectdistancesbetweenFRandVC,respectively (R,right).
Right and left rotundum angles (calculatedas the angle betweentheimaginarylineconnectingFRtoVCand verti-callinepassingtheVC).
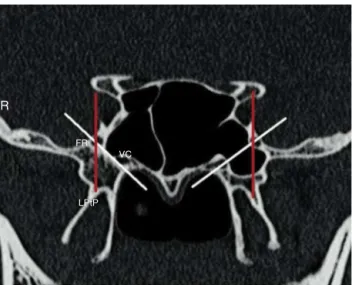
PositionoftheFRregardingtobaseoflateralpterygoid platedefinedas(Fig.3):
Online---whenFRistangenttothelateralpterygoidplate; Medial --- when FR is placed medially regard the lateral pterygoidplate;
R
FR VC
LPtP
Figure 3 Sphenoid sinus pneumatization classification accordingtotheimaginarylineconnectingforamenrotundum tovidiancanal;whitelines(right,lateralrecess;left,tangent) andpositionoftheFR regardingtobaseoflateralpterygoid plate;redlines(rightandleft,online)(R,right).
SSpneumatizationwasclassifiedaccordingtothe imagi-narylineconnectingFRtoVC(Fig.3):
Lateralrecess--- whenthesinusispneumatizedtothe lat-eraloftheimaginaryline;
Tangent ---whenthesinus is pneumatizedtangent tothe imaginaryline;
Lesspneumatized---whenthesinusispneumatizedmedial totheimaginaryline.
Mid-sphenoidpositionwasdefinedaccordingtothespace belowthemid-sphenoidcoronalsectionthatis nasopharyn-geal,choanaornasalcavity.
ThreetypesofFRdefinedasthefollowing(Fig.4):
Type I --- when FR is placed completely withinthe sinus cavity;
TypeIIa---whenapartofFRisinthesinuscavityorpartially protrudingintotheSS;
TypeIIb---whenFRistangenttothesinuswall;
TypeIII---whenFRisplacedcompletelywithinthesphenoid bone.
TheVCwasalsoclassifiedintothreetypesbasedonCT findings(Fig.4):
Type1---whenVCiscompletelywithinthesphenoidsinus; Type2---whenVCisonthefloorofthesphenoidsinusor partiallyprotrudingintothesphenoidsinus;
Type3---whenVCiscompletelyembeddedinthesphenoid corpus.
A
LR LR VC
VC FR
FR LR
L NP
FR
VC
T
C
FR
B
C
D
TheclassificationusedforthetypesofFRiscreatedby ourselves but the VCclassification wasadopted fromLee etal.9
Statisticalanalysis
Data entered and analyzed via SPSS version 22 software (SPSSInc,Chicago,IL,USA).Quantitativevariables (includ-ing distances) expressed asmean and standard deviation (SD).The Student’s ttest and pared T-test were usedto determinestatisticalsignificancebetweenrightandleft dis-tances.Thenullhypothesisassumednodifferencebetween thegroupstested.p-Valueslessthan0.05definedas signif-icant.
Results
Imagingdata
Atotalnumberofone-hundredpatientswiththemeanage of38.56±18.51years(rangingfrom18to86)wererandomly selectedfromtheradiographicdatabaseoftheDepartment ofOtolaryngology-Head&Neck surgeryofHazrat-e-Rasool AkramHospital.Halfofthepatients(50cases)weremale. Mean bilateral FR distances were 38.48±3.87mm (range 30---48mm). The SSpneumatization wascategorizedtobe lateralrecessin54%ofcases,tangentin26%andless pneu-matizedin20% ofcases.Mid-sphenoid positionwasabove thechoanain74%ofcases,andabovethenasopharyngeal andnasalcavitiesin10%and16%ofcases,respectively.
Average right and left FRs distances to midline were 19.00±2.07 and 19.34±2.17mm, respectively (p=0.03). AveragerightFRtorightVCdistancewere5.89±2.4mmand 5.06±2.03mm, horizontally and vertically, respectively; directdistance calculatedas8.16±2.27mm.Average left FRtoleftVCdistancewere5.93±2.13and5.49±2.13mm, horizontallyandvertically,respectively;directdistance cal-culated as9.20±2.15mm. Horizontal, verticaland direct distances between the right and left FRs to VCs, had notstatisticallysignificantdifference(p=0.764---0.676 and
p=0.952,respectively)(Table1).
Twenty-eight cases (28%) had type I vidian canal, 48% and24%hadtypeIIandIIIvidiancanals,respectively.Four patients(4%)hadtypeIrotundumforamen,28%and44%had typeIIaandIIb,respectivelyand24%hadtypeIIIrotundum foramen(Table2).
Table2 Typesofvidiancanalandforamenrotundum.
I II III
Foramenrotundum 4 28(IIa) 44(IIb) 24
Vidiancanal 28 48 24
Table3 RightandleftFRspositionsinrelationtobaseof lateralpterygoidplate.
Right Left Total
Onlineplaced 48% 52% 50%
Mediallyplaced 50% 44% 47%
Laterallyplaced 2% 4% 3%
The positionof right FRregarding tothe base of right lateralpterygoidplatewasonlinein48%,mediallyplacedin 50%andlaterallyplacedin2%ofcases.Thepositionofleft FRregardingtothebaseofleftlateralpterygoidplatewas onlinein52%,mediallyplacedin44%andlaterallyplacedin 4%ofcases(Table3).
Discussion
Theresultsofthisstudyprovidesaradiologicalreviewabout theanatomicalrelationshipsoftheSSandFRwiththeother anatomicallandmarksofthe areasuchasVC andbase of lateral pterygoid plate which can take into accounts for sphenoidendoscopicandother surgical proceduresof the area.Wehave describedthe radiographicanatomy ofthe FRintermsofdistancefromthemidlineaxisandthetypes ofFRsandVCs.InCTscansinterpretedinthecoronalplane, theFRwasfoundtohaveasymmetricallydistancesfromthe midlineaxis,asshown inTable1.Thisserves asa critical pieceofinformationthattheendoscopicskullbasesurgeon canuse when attemptingto safely localize the FRduring approachesthroughtheSS.Inaddition,theFRsdistancesto VCsweresymmetricalinhorizontal,verticalanddirectaxes. ThisfindingmayhelpthebetterlocalizationofFRin rela-tiontoVC,whichfacilitateitssafeidentificationandhelp thesurgeonavoidaninadvertentinjurytotheiranatomical integrity.
AsitisshowninTable3,weobservedforthefirsttime thatalmostalloftheFRwereplacedeitheronlineormedial tothebaseoflateralpterygoidplateandonlyin3%ofall caseswereplacedlateraltothe baseof lateralpterygoid
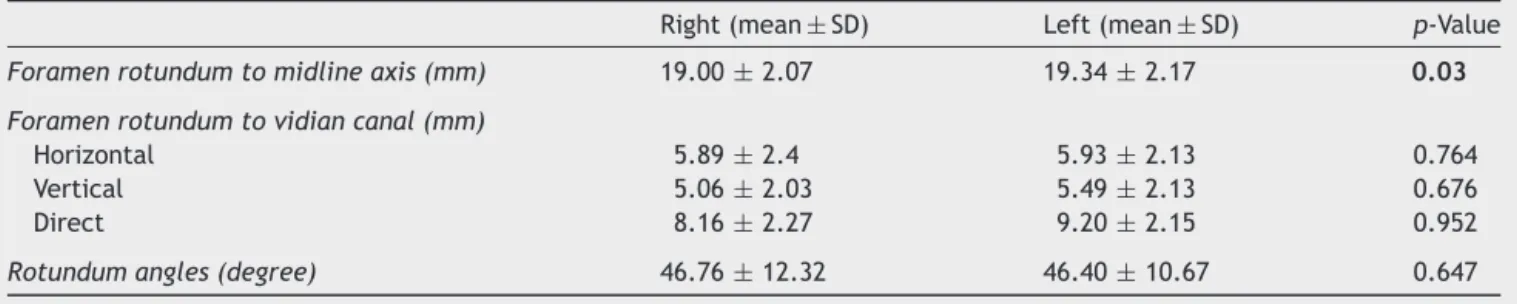
Table1 Measurementsindexofforamenrotundumdistancestowardmidlineaxis,vidiancanalandbaseoflateralpterygoid plate.
Right(mean±SD) Left(mean±SD) p-Value
Foramenrotundumtomidlineaxis(mm) 19.00±2.07 19.34±2.17 0.03
Foramenrotundumtovidiancanal(mm)
Horizontal 5.89±2.4 5.93±2.13 0.764
Vertical 5.06±2.03 5.49±2.13 0.676
Direct 8.16±2.27 9.20±2.15 0.952
plate.Inaddition,theclassificationthatshowedthe major-ity(74%)ofmidsphenoidsectionpositionswereatthelevel ofchoanawasforthefirsttimepresentedinourstudy.
VC and FR classifications were the same bilaterally in mostofthecases.Only2caseshaddifferenttypesofVCsand tencaseshaddifferenttypesofFRsonthetwosides,which wereclassifiedandanalyzedindifferentgroups according totheirclassification.Remarkably,wefoundthatthetype ofVCclassificationwasalwaysthesameoronelevelbehind theFRtypeinourpatients.Forexample,whentheVCwas completelywithintheSS(typeI),theFRwaseitherplaced completelywithinthesinuscavity(typeI)orpartially pro-trudingintotheSS(typeII).WhentheVCwasonthefloor oftheSSorpartiallyprotrudingintotheSS(typeII),theFR waseither partiallyprotruding intotheSS (typeIIa), tan-genttothesinuswall(typeIIb)orplacedcompletelywithin thesphenoidbone(typeIII).Finally,whentheVCwas com-pletelyembeddedinthesphenoidcorpus(typeIII),theFR wasalwayscompletelywithinthesphenoidbone(typeIII). Toourknowledge,thisisthefirstreportofsuchfindingin PNSCT-scan.AswefoundinPNSCTscansofourpatients, morethanhalfoftheSSs(54%)werepneumatizedlateralto theimaginarylineconnectingFRtotheVC.
Duringthepastyears,endonasalendoscopicsurgeryhas gainedgreatimportanceinsinussurgeryandinsome neu-rosurgicalapproaches. Duetothisgreatevolutionofsinus surgery,knowledge ofthe sinusanatomyhas become cru-cial.TherelationsoftheSSwithstructuresaroundareclose whenthesinusiswellpneumatized.Whenthishappens,the surroundingvesselsandnervesareseeninthesinuscavity asirregularitiesorridges.Thepneumatizationofthe sphe-noidtothepterygoidprocessesisanextensionofthesinus betweenthemaxillarynerveandthenerveofthepterygoid canal(vidiannerve).
Themostimportantrelationsofthesphenoidareonits superiorandlateralwalls,withtheinternalcarotidartery andtheopticnerve.Thesehavebeenshowntohavevariable pathways alongside the sphenoid.5 The SSs are
asymmet-riccavitiesinside the sphenoidbodyseparatedby a bony septum. Literature describes this septum as being rarely situatedonthe medianplanebutveryoftendeviated lat-erallyto oneside or the other.Itspathology is nowadays mostly approached trough endoscopic surgery, with some limits.Due toitslocationanditsrelations,itis modernly oftenusedbyrhinologistsandneurosurgeonsasapathway topartsofthecentralnervoussystem,withnewtechniques beinginventedataveryhighrate.Havingahighvariability, itsanatomicalrelationsandtheirvariationshavetobewell understoodpriortoanysurgicalintervention.5
It is vitalthat the surgeonis informed about the vari-ationsinordertoavoidvitalcomplicationsduringsurgery. Theendoscopicendonasalapproachesarecommonlyusedto accessthemiddleskullbaseareasofthelateralcavernous sinus(mostlyfortissuediagnosisorsurgicaldecompression), Meckel’scave (for removalof trigeminal schwannomas or meningiomas,nerveresectionmarginsforsinonasal malig-nancywithperineural invasion),and anterolateral middle fossa triangle (for repair of cerebrospinal fluid leaksand pseudomeningoceles).
The SSisoneofthe mostmorphologicallyvariableand surgicallyimportant structures of the skullbase. Located belowthe sellaturcica,neighbored by parasellarregions,
such as the orbital apex, pterygopalatine fossa and lat-eralsellar region(cavernous sinus),it is clinicallyrelated to these and surgically relevant as corridor for various approaches.10
Recently,someradiologicalstudies havebeen designed in order toprovide a better comprehension of this com-plexareaandbydefininganatomicalvariablesanddistances usingtheanatomicallandmarksofthearea.Afterstudying the CT images of 100 and 18 SSs in adults and cadavers, respectively,Wangetal.proposedanewclassification sys-temforsinusextensionincludinglateral,clival,lesserwing, anterior,and combined.3 Vescan etal. analyzed the
rela-tionshipsofVCtotheinternalcarotidarteryin44CTscan to describe the anatomy and relationships of the VC to knownendonasalandskullbaselandmarks.Theyfoundthat the degree of pneumatization of the SS is highlyvariable andreportedsomemeasurementindexessuchasthemean lengthoftheVCandtheanatomicallocationoftheVCand the anterior genuof the petrous internal carotid artery.4
Kasemsirietal.todefineanatomicallandmarksforthe pre-operativeplanningofendoscopicendonasaltranspterygoid approaches,reviewedimagesfromhigh-resolution maxillo-facialCT scans.They reportedtheaverage distance from midline to left FR 19.11mm and to right FR 17.67mm (p=0.04).Wealsofoundthattheaveragedistanceof mid-line to left FR to be significantly more than to right FR (p=0.03). The average horizontal and vertical distances fromFRtoVCinKasemsiri’sstudyshowednosignificant dif-ferencebetweenrightandleftsides,aswefoundthesame resultinourpopulation.11
Inanothersimilarstudy,Vaezietal.in2015used high-resolutionCTscanstopresentaclassificationbasedonthe degree of pneumatization of the SS inthe coronal plane. They also measured the association of SS pneumatization withthelocationoftheFRandtheVCandreportedthatthe distance separatingtheFRandthe VCcorrelatedstrongly withthedepthofthelateralrecess.1
Theaimofalloftheabovestudiesandthesimilarstudies likeoursistogiveabettercomprehensionoftheanatomical situation of this complexarea in order toinstruct better preoperative planningfor endoscopicendonasal surgeries. Asaresultofthesestudies,anendoscopicskullbasesurgeon hasanumberof anatomicallandmarksandmeasurements that may behelpful in safely localization of theforamen rotundumduringendonasalapproachestotheskullbase.
Conclusion
This papermakesareview abouttheanatomicalrelations of foramenrotundum withtheother endonasallandmarks suchasVCandlateralpterygoidplate. Theresults ofthis study can be used toprovide a better anatomical under-standing of the area, which is necessary for endoscopic skull base surgeons. In order togeneralize the results of thisstudy,epidemiologicalstudieswithlargersamplesizes arerecommendedin additiontoclinicalstudiesfor a bet-teridentification of therelationships betweenanatomical landmarksoftheskullbase.
Conflicts
of
interest
References
1.VaeziA,CardenasE,Pinheiro-NetoC,PaluzziA,BranstetterBFt, GardnerPA,etal.Classificationofsphenoidsinus pneumatiza-tion:relevanceforendoscopicskullbasesurgery.Laryngoscope. 2015;125:577---81.
2.CitardiMJ,GallivanRP,BatraPS,MaurerCRJr,RohlfingT,Roh HJ,etal.Quantitativecomputer-aidedcomputedtomography analysisofsphenoidsinusanatomicalrelationships.AmJRhinol. 2004;18:173---8.
3.Wang J, Bidari S, Inoue K, YangH, RhotonA Jr. Extensions of the sphenoid sinus: a new classification. Neurosurgery. 2010;66:797---816.
4.Vescan AD, Snyderman CH, Carrau RL, Mintz A, Gardner P, BranstetterBt,etal.Vidiancanal:analysisandrelationshipto theinternalcarotidartery.Laryngoscope.2007;117:1338---42. 5.BuduV,MogoantaCA,FanutaB,BulescuI.Theanatomical
rela-tionsofthesphenoidsinusandtheirimplicationsinsphenoid endoscopicsurgery.RomJMorpholEmbryol.2013;54:13---6.
6.Martin-DuverneuilN,Sarrazin JL,Gayet-DelacroixM, Marsot-DupuchK,PlantetMM.Theforamenrotundum.Anatomyand radiological explorations. Pathology. J Neuroradiol. 2000;27: 2---14.
7.Me C.Differential diagnosis inhead and neck imaging. Clin Radiol.2000;55:411.
8.LuY, Pan J, Qi S, ShiJ, ZhangX, Wu K. Pneumatizationof thesphenoidsinusinChinese:thedifferencesfromCaucasian anditsapplicationintheextendedtranssphenoidalapproach. JAnat.2011;219:132---42.
9.LeeJC, KaoCH,Hsu CH,LinYS.Endoscopic transsphenoidal vidianneurectomy.EurArchOtorhinolaryngol.2011;268:851---6. 10.Sandulescu M, Rusu MC, Ciobanu IC,Ilie A, Jianu AM. More actors,differentplay:sphenoethmoidcellintimatelyrelated tothemaxillarynervecanalandcavernoussinusapex.RomJ MorpholEmbryol.2011;52:931---5.