Research
Paper
Trauma
Do
erupted
third
molars
weaken
the
mandibular
angle
after
trauma
to
the
chin
region?
A
3D
finite
element
study
T. P.Bezerra,F.I.SilvaJuniorH.C.Scarparo,F.W.G.Costa,E.C.Studart-Soares: Doeruptedthirdmolarsweakenthemandibularangleaftertraumatothechinregion? A3Dfiniteelementstudy. Int.J.OralMaxillofac.Surg.2013;42:474–480. #2012 InternationalAssociationofOralandMaxillofacialSurgeons.PublishedbyElsevier Ltd.Allrightsreserved.
T.P.Bezerra,F.I.SilvaJunior, H.C.Scarparo,F.W.G.Costa, E.C.Studart-Soares
Post-GraduationPrograminDentistryofthe FederalUniversityofCeara´,St.Monsenhor Furtado,Ceara´,Brazil
Abstract. Ithasbeensuggestedthatthirdmolarsincreasemandibularfragility becausetheydonotcontributetoitsstrength.Forethicalreasons,ahumanstudy designthatwouldpermittheelucidationofthisinterferenceisnotpossible.This study evaluatedtheimpactofthepresenceoferuptedthirdmolarsonthe mandibular angleofresistancewhensubmitted totrauma.Athree-dimensional (3D)mandibularmodelwasobtainedthroughfiniteelementmethodologyusing computed tomography(CT)withthegeometryandmechanicalproperties to reproduceanormalmandibularstructure.Humanmandibleswithno,oneortwo eruptedthirdmolarswereevaluated.Wheneverthethirdmolarwaspresentthere was agreaterconcentrationoftensionsaroundthecervicalpartofitsalveolus. ApproximatedVonMisesequivalentstressofthethirdmolarregionwas 107.035MPainthemandiblewithteeth and64.6948MPainthemandible withoutteeth.Inthecondylarregionitwas151.65MPawhenthethirdmolarwas presentand184.496MPawhenitwasabsent.Thedigitalmodelscreatedproved thatthemandibularanglebecomesmorefragileinthepresenceofthirdmolars. Whentheyareabsenttheenergyconcentratesonthelateraleposterioraspectof thecondylarneck.
Keywords: finiteelementanalysis;molar,third; mandible.
Acceptedforpublication5October2012 Availableonline15November2012
The mandible is one ofthe bones most susceptibletotraumainthefacialregion due toitsmore projectedpositioninthe facialskeleton.1–3Thisprevalenceis influ-enced byfactorssuchassex,age, socio-economic condition and the type of trauma.4Anexperimentalstudywith mon-keyshasshownthatmandiblescontaining unerupted third molars fractured at
approximately 60%oftheforcerequired to fracture mandibles with eruptedthird molars.5Bezerra et al.6 reported a 1.94-foldhigherriskofmandibularangle frac-tureswhenthethirdmolarispresent.
Forceapplieddirectlyinthesymphysis region inaxialplaneisdistributed along the arch of the mandible. The condylar headsarefreetorotatewithintheglenoid
fossa, to a certain degree, thus tension develops along the lateral aspect of the condylar neck and mandibular body regions,aswellasalongthelingualaspect ofthesymphysis.Thisleadstoabilateral condylar fracture and a symphysis frac-ture,unlessafragilityfactorexists.7
Thereasonfortheincreasedprevalence ofmandibularanglefracturesisnotwell
http://dx.doi.org/10.1016/j.ijom.2012.10.009,availableonlineathttp://www.sciencedirect.com
established.1Thepresenceofthirdmolars has been suggested to contribute to an increased mandibular fragility because themandiblelosespartofitsbone struc-turetoharbourtissuesthatdonot contri-bute to its strength.4,8,9 Some authors suggest that completely unerupted teeth aremoreassociatedwithmandibular fra-gilitybecausetheycompromisethebone structure toa greatextent. Theeffectof partially erupted teeth on the support structures of the mandibular framework (external oblique line) should also be takenintoaccount.3–5,10Areviewof retro-spective datafilesindicatedthatthe pre-valence and relative risk of mandibular anglefracturearebothsignificantlyhigher insubjectswithfullyeruptedthirdmolars thaninindividuallackingthoseteeth.11
For ethical reasons, no human study design would permit the elucidation of thisinterference,sinceitwouldbe impos-sible tosubmitexperimentalandcontrol groups to injuries likely to fracture the mandible, in orderto evaluate the resis-tance ofthis bone and the effect ofthe thirdmolaronmandibularfractures.
Aeronauticalengineering studies have allowed the development of a computa-tional method for mechanical tests by creating virtual elements with finite dimensionsandphysical properties.This maybeadaptedtorealstructures,to recre-ateloadapplicationsandpresentthe dis-tribution of stresses and deformation.12 This methodology, called finite element analysis (FEA), is a powerful tool for computational modelling that is being widely used to predict the mechanical behaviour of complex biological struc-tures such as bone.13 The accuracy of FEAtodescribethebiomechanical beha-viourofbonespecimenshasbeenshown bydifferentauthors.13–16
In the present study, a three-dimen-sional(3D)computedtomographic-based
finite element reconstruction of three human mandibles with or without third molars was performed to evaluate these mechanical properties. The aim was to evaluate the impact of the presence of eruptedthirdmolarsonmandibularangle stiffnesswhensubmittedtoatraumatothe chinregion.
Materialsandmethods
Theethicscommitteeofthelocal institu-tionapprovedtheprotocolforthisstudy. Informed written consent was obtained froma30yearold,malepatientselected for the studywho underwent computed tomography(CT),basedonthefactthat he had allthe mandibularteeth, andno structural mandibular changes (osseous callus/fracture, pathologic entities, pre-vious orthodontic treatment maxilla-mandibular discrepancy or periodontal illness).
The images were obtained by a cone beamCT,andwereimportedbythe Sca-nIPsoftware(Simpleware1Ltd.,Exeter,
UK) in which the tomographic density window applicabletotheobjectinstudy (2240550UH)andpixelsizetobeused (0.55mm)weredefined.
Inordertoproducethevirtualstructure, the3Dmeshandallthestepstoperform theFEAwereadaptedfromtheprocedure describedbySilvaetal.17Themesh pro-ductionbeganbyseparatingthemasksof the mandibular structures in order to includetheminthemodel(discretization). Thesemaskswereobtainedby digitaliza-tionofeachCTslice,andapixel-by-pixel individualization ofthetissuesevaluated inthestudy(corticalbone,marrowbone, enamel,dentin,cement,pulp,periodontal ligament),basedonthetomographic den-sity.Duringsegmentationonlybone-and teeth-relatedstructureswerekeptandsoft tissuesweredisregarded.
Aftertheproductionofthefinalmodel inallslices,thesoftwaregenerateda3D structure maintaining each discretized maskinposition.Forgreatersmoothness onthesurfaceofthestructure,asoftware tool was used to fill in small gaps and round angles. The result was a very detailed3Dmesh.
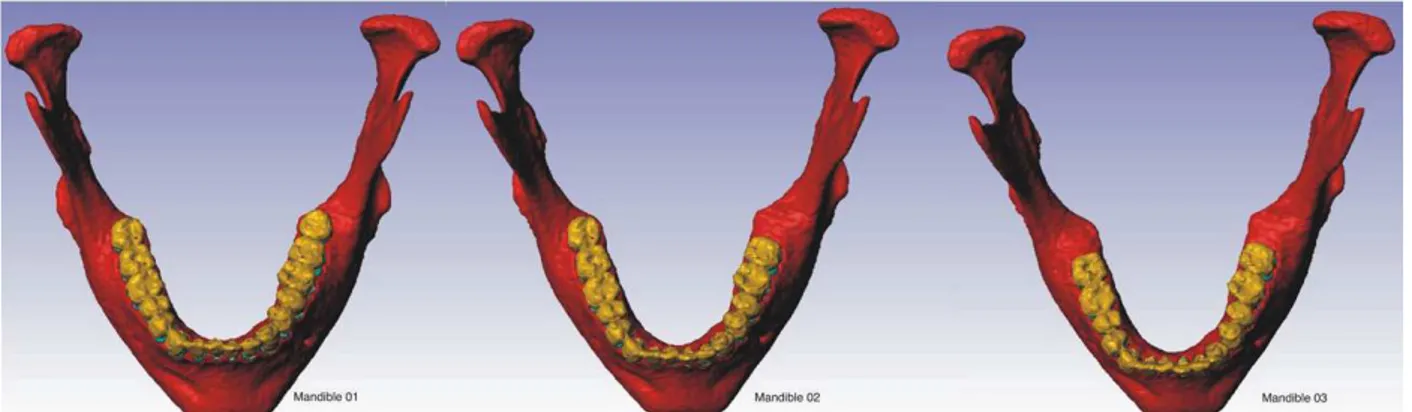
To create the three meshes to be includedinthisstudy,theinitial mandib-ular structure (mandible 01) was sub-mittedtoadigitalmasksubstitution. On the software interface the pixels of the thirdmolarwerechangedfromtheinitial toothstructure maskstothose from cor-ticalandmedullarboneineachCTslicein accordance with an anatomic aspect. Therefore, it was possible to create a second structure without the left third molar(mandible02),andathirdone with-out third molars (mandible 03) (Fig. 1). Theremainder ofthestructure remained thesame.
IntheScanFE1software(Simpleware
Ltd.,Exeter,UK),eachofthethree mand-ibles was exported to a finite element mesh that consisted of triangular and tetrahedral elements to interconnect the nodes. Themesheswereexportedtothe software ANSYS1 (SIMULIA,
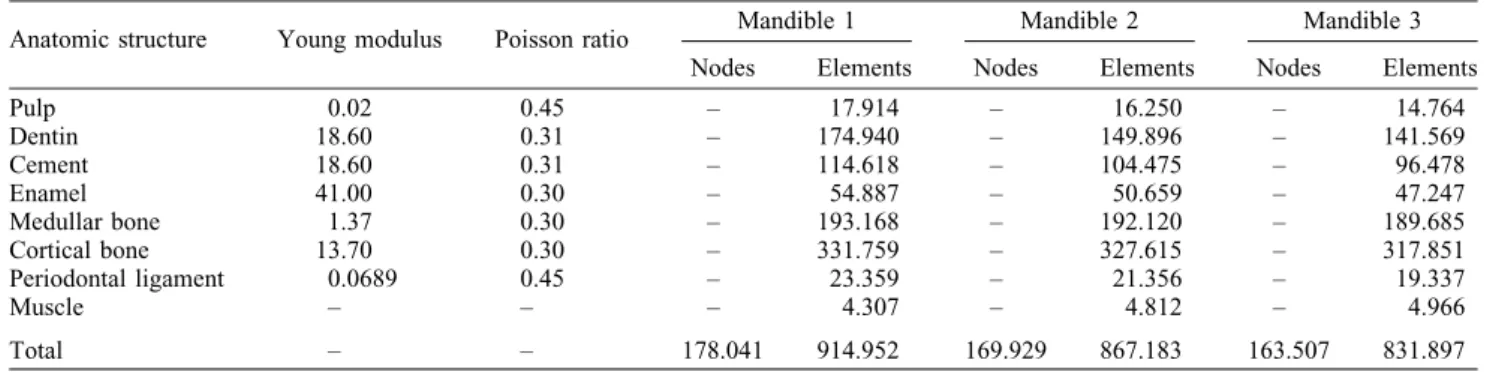
Provi-dence,RI,USA),version13.0,for struc-turalanalysisofthemechanicaltests.The homogeneityofthestructures,linear elas-ticdeformationpattern,andthe standar-dization of the isotropic mechanical propertieswereensuredforeach discre-tizedmask(Table1).ThevaluesofYoung modulusandPoissonratiowerebasedon Lottietal.18
To simulate an anatomically normal mandibular function, the external nodes ofthemostposteriorandsuperiorpartof themandibularcondylewerefixatedinall degrees of freedom bilaterally (Fig. 2). The actions of the masticatory muscles werereproducedbythecreationofspring
resistance elements with vectors as describedbyBujta´retal.,19andthe rigid-itywas basedonanestimationof defor-mationofthemuscles.
A blunt trauma with a magnitude of 250kgf was applied perpendicularly to thefrontalplane,onacirculararea1cm indiameter(centreonthepogonium),in themidlineofthesymphysis, perpendicu-larly to the coronal plane. This was a simulationrepresentativeofapunch (fron-talaggression).Theresultswereevaluated byadescriptiveanalysisofthechromatic Von Misses stress distribution after the impact.
Results
A highly detailed, patient-specific, cus-tom-made, high-resolutionyetsimplified modelofthemandiblecouldbegenerated withaverydensevolumemeshof914.952
finite elementsformandible01;867.183 for02,and831.897for03.Basedonthis methodthedetailsofthemandiblecould beemphasized andsuccessfullyincluded in an analysis of the dynamics of a responsetoanimpact.
Themaximumstresseswerelocatedat the symphysis (point of impact), in the retromolarareaandbothcondylesonthe threeexperimentalmodels.
The presence of the third molars resulted inadifference inthestress dis-tribution on the three meshes studied. Whenever the third molar was present therewasagreaterconcentrationofstress around the cervical part ofthe alveolus (Fig.3).Itwasnoticeablethattheimpact resultedinaconcentrationofstressonthe externalobliqueridge,andwhenthethird molar was present this concentration extended to the alveolar process (Fig. 4). On mandibles 2 and 3, the
structural reinforcementprovided by the boneintheretromolarareawithout third molarsmadethestressconcentratemore onthecondylarregiononthesidewithout athirdmolar(Fig.5).
Approximated Von Mises equivalent stress in the third molar region was 107.035MPainthemandiblewithathird molarand 64.6948MPain themandible without a third molar. In the condylar region the Von Misses equivalent stress was151.65MPawhenthethirdmolarwas present and 184.496MPa when it was absent.
Discussion
FEAhasbeendevelopedintoabranchof appliedmathematicsfor numeric model-lingofphysicalsystems,whichisusedin manyengineering disciplines.Inits sim-plestmathematical terms, thisnumerical Table1. Mechanicalproperties,referencesofnumberofnodesandelementsineachmaskreconstructed.
Anatomicstructure Youngmodulus Poissonratio Mandible1 Mandible2 Mandible3
Nodes Elements Nodes Elements Nodes Elements
Pulp 0.02 0.45 – 17.914 – 16.250 – 14.764
Dentin 18.60 0.31 – 174.940 – 149.896 – 141.569
Cement 18.60 0.31 – 114.618 – 104.475 – 96.478
Enamel 41.00 0.30 – 54.887 – 50.659 – 47.247
Medullarbone 1.37 0.30 – 193.168 – 192.120 – 189.685
Corticalbone 13.70 0.30 – 331.759 – 327.615 – 317.851
Periodontalligament 0.0689 0.45 – 23.359 – 21.356 – 19.337
Muscle – – – 4.307 – 4.812 – 4.966
Total – – 178.041 914.952 169.929 867.183 163.507 831.897
technique is used to find approximate solutionsforpartialdifferentialand inte-gral equationsthrough the generationof meshesofacontinuousdomainforasetof discretesubdomainsorelements. Numer-icalmethodsarethenused topredictthe behaviour of the object in question in varioussituations,forexample,under con-ditions ofloading.20 Theexternal forces and the mechanical properties/geometry are usedto calculate thenodal displace-ments;thedifferentiationofthe displace-ment field yields the strain distribution; and the stress distribution is determined mathematically.21
FEA is being developed to overcome theexperimentalmodelsinbiomechanical studies.Itisdifficulttocreatean experi-mental modelof the mandible;the geo-metry,internalstructuresandthefunction cannotbegrosslysimplified.The muscu-lar action cannot be reproduced as a uniquevectorofforceattachedtoasingle
point.22Muscletensionisneededtocause an angle fracture.23 This reduction in detail leads toa simplifiedmodelofthe item’s behaviour that may often lead to incompleteorincorrectmechanicsofthe structuremodels.22Byavoidingthese sig-nificantvariables,theexperimental com-putationalmodeldevelopedinthis study approached the real mandibular beha-viour. Its geometric shape was recon-structed based on a real mandibular structure, the masticatory muscles were attachedtothemandibleasinananatomic body, and the physical and mechanical properties were reproduced similarly to thenormalbody.
In addition, to allow the comparison betweenthestructuresinordertoevaluate theinfluenceofthethirdmolarpresence, theonlydifferencewasinthemechanical properties ofthe thirdmolar pixels.The restofthestructuresremainedexactlythe sametoreducestructuralbias.
It is important to study this subject because full understanding of the facial bonefracturemechanismsisnecessaryto enable appropriate treatment to be pro-vided and this modelling provides more information than clinical experience alone.Ithaspreviouslybeenreportedthat bonefailsandfracturesmorereadilyunder tension thancompression.24 In undertak-inganytherapythataffectstheskeleton,it is important to understand the potential problemofexcessiveloadingofbone.25
obliqueridgenearthethirdmolar,andin the neck region of the condyle on its buccalandposteriorsides.
Thirdmolarscanberelatedtothe fra-gility of the angle, since their presence significantlyaltersitsbiomechanics. Ret-rospective studies,caseseriesand litera-turereviewshaveshownthatthepresence ofthirdmolarsislinkedtotheincreased prevalenceofmandibularanglefracture.6 There are not enough studies from the perspectiveofbiomechanics,whichshow thetrueimpactofthirdmolarpresenceand theoccurrenceoffractures,because repro-ducing a real model of the mandible is difficult.
FEAisavalidandnon-invasivemethod thatprovidesusefulresultstopredict dif-ferent parametersofthecomplex biome-chanicalbehaviourofhumanmandibles.14 In the present study, the digital models provedthatthemandibularanglebecomes morefragilewhenthethirdmolaris pre-sent. The study by Gallas-Torreira and
Fernandez15 istheonlypublishedarticle with a similar methodology and results. They highlighted that clinical extrapola-tionsfrommathematicalmodelsmaynot giveabsolutevalues.Thereasonforthisis inadequate recreation of the computa-tional model, considering that they did notapplydifferentialmechanical proper-tiestotheteeth,allowingthemtofunction as a part of the mandibular structure. Vollmer et al.14 added the necessity of attributing the boundary conditions of the condyles and the distribution of the masticatorymusclestoobtainanadequate computational model,aswasdoneinthe presentcomputationalmethod.
ThestudyofSzu¨csetal.25showedthat themandibularexternalobliqueridge on each side was the location where stress was concentrated.Themodelsdeveloped in the present study had similar stress distribution. Mandibularthirdmolarsare usually situatedclosetothisridge.They candiminishthestructuralreinforcement
ofthemandible.Szu¨csetal.25showedthat the removal of these teeth with bone osteotomycouldincrease thefragilityof the mandibular angle. It is important to knowthiswhendeciding onthirdmolar removal.
absent.Whencomparingthesubcondylar regionamongthethreemandiblesitcanbe seenthatwhen thethirdmolar was sub-stituted bynormal bone,the energywas concentrated more on the subcondylar region.Thatiswhyamandiblewiththird molars tends tofail inthe angle region, whileonewithouttheseteethtendstofail atthecondylarneck.
Duan andZang23 considered that low force trauma was able to fracture the mandible in one site, moderate trauma intwo,andhightraumainthreeormore. With respectto prophylacticthird molar extraction,itappearsthatimpactedteeth inpatientswithahighriskofsufferinglow traumaforces, such asincontact sports, should be extracted, whereas patients moreoftensubjectedtomoderateorhigh traumaforcesmightnotbenefitfrom pro-phylactic third molar extraction. After analyzingtherelationshipbetween multi-plemandibularfracturesandthepresence oflowerthirdmolars,Choietal.11found
that, in mandibleswithembedded lower thirdmolars,themandibularsymphysisis themostcommonsiteofcomorbid frac-ture in individuals with a mandibular anglefracture.Thestudies indicatedthat the presence ofthird molarspredisposes themandibletofractureinthethirdmolar region when the trauma is of moderate intensityandcancausetwofractures,one attheplaceoftheimpact(symphysis)and the other in the angle. The images obtainedinthepresentstudysupportthis information asfarastheenergy concen-tratesontheimpactpointandonthe retro-molarareaofthethirdmolar.
Bujta´ret al.19 evaluated reconstructed modelsofthreesubjectsofdifferentages andstatedthatphysiologicloadstressand straindistributionalchangesinthe mand-ible vary according to age, with higher elasticity in younger models. This is a limitation of a study with a real body simulationinvivoandcanbeextrapolated to computational models. To overcome
this limitation alarger sample wouldbe needed,butinarealsituationitwouldbe impossible tosubmit a large number of subjects to mandibular impacts, and to performcomputational simulationwould bealaboriousandtime-consumingtask.
dentistrymayfacilitatetheuseofFEAin the preoperative analysisofspecific sur-gicalsites.25
Funding
Thisresearch receivedthe financial sup-portofGrant#478819/2010-2from Con-selho Nacional de Desenvolvimento Cientı´fico e Tecnolo´gico (MTC/CNPq No.14/2010).
Competinginterests
Nonedeclared.
Ethicalapproval
Thisstudywassubmittedandapprovedby thelocalcommitteeonhumanresearchof Walter Cantı´dio University Hospital, registeredunderprotocol0.43.04.11.
References
1. InaokaSD,CarneiroSC,VasconcelosBC, Leal J, Porto GG. Relationship between mandibular fracture and impacted lower thirdmolar.MedOralPatolOralCirBucal
2009;14:349–54.
2. LibersaP,RozeD,CachartT,LibersaJC. Immediate and late mandibular fractures afterthirdmolarremoval.JOralMaxillofac Surg2002;60:163–5.
3. Ma’aita J, Alwrikat A, Jordan A. Is the mandibularthirdmolarariskformandibular fracture.OralSurgOralMedOralPathol
OralRadiolEndod2000;89:143–6.
4. MeisamiT,SojatA,SandorGKB,Lawrence HP,ClokieCML.Impactedthirdmolarsand riskofanglefractures.IntJOralMaxillofac Surg2002;31:140–4.
5. ReitzikM,LownieJF,Cleaton-JonesP, Aus-tin J. Experimental fractures of monkey mandibles.IntJOralSurg1978;7:100–3. 6. Bezerra TP, Studart-Soares EC, Pita-Neto
IC, Costa FWG, Batista SHB. Do third molarsweakenthemandibularangle?Med
OralPatolOralCirBucal2009;16:e657–63.
http://dx.doi.org/10.4317/medoral.16970.
7. ChaconGE,LarsenPE.Principlesof man-agementofmandibularfractures.In:Miloro M,editor.Peterson’sprinciplesoforaland
maxillofacialsurgery.London:BCDecker;
2004.p.401–33.
8. IidaS,HassfeldS,ReutherT,NomuraK, MuhlingJ.Relationshipbetweentheriskof mandibularanglefracturesandthestatusof incompletely erupted mandibular third molar. J Craniomaxillofac Surg 2005;33: 158–63.
9. Ugboko VI,Oginni FO, Owotade FJ. An investigation intotherelationship between mandibularthirdmolarsandanglefractures in Nigerians. Br J Oral Maxillofac Surg
2000;38:427–9.
10. Halmos DR, Ellis 3rd EE, Dodson TB. Mandibularthirdmolarsandanglefractures.
JOralMaxillofacSurg2004;62:1076–81.
11. ChoiBJ,ParkS,LeeDW,OheJY,Kwon YD. Effect of lower third molars on the incidenceofmandibularangleandcondylar fractures. J Craniomaxillofac Surg 2011; 22(4):1521–5.
12. MaurerP,HolwegS,KnollWD,SchubertJ. Study by finite element method of the mechanicalstressofselectedbiodegradable osteosynthesis screws in sagittal ramus osteotomy. Br J Oral Maxillofac Surg
2000;40:76–83.
13. GroningF,LiuJ,FaganMJ,O’HigginsP. Validating a voxel-based finite element model ofa humanmandible usingdigital speckle pattern interferometry. J Biomech
2009;42:1224–9.
14. VollmerD,MeyerU,JoosU,VeghA,Piffko J.Experimentalandfiniteelementstudyofa humanmandible.J CraniomaxillofacSurg
2000;28:91–6.
15. Gallas-TorreiraM,FernandezJR.A three-dimensionalcomputermodelofthehuman mandibleintwosimulatedstandardtrauma situations.JCraniomaxillofacSurg2004;32: 303–7.
16. Liao SH,Tong RF,DongJX.Anisotropic finiteelementmodelingforpatient-specific mandible. Comput Methods Programs
Biomed2007;88:197–209.
17. Silva BR, MoreiraNeto JJS, Silva JrFI, AguiarASW.Finiteelementanalysisapplied to dentoalveolar trauma: methodology
description. ISRN Dentistry 2011;2011: 1–5.
18.Lotti RS, Machado AW, Mazzieiro ET, Landre Ju´niorJ. Aplicabilidade cientı´fica dome´tododoselementosfinitos.RevDent
Press Ortodon Ortop Facial 2006;11(2):
35–43.
19.Bujta´rP,SandorGKB,BojtosA,SzucsA, Barabas J. Finite element analysis of the humanmandibleat3differentstagesoflife.
Oral Surg Oral Med Oral Pathol Oral
RadiolEndod2010;110:301–9.
20.Strang G,FixG.An analysisof thefinite element method. Englewood Cliffs (NJ): Prentice-Hall;1973.
21.WongRCW,TidemanH,MerkxMAW, Jan-senJ,GohSM,LiaoK.Reviewof biome-chanical models used in studying the biomechanics of reconstructed mandibles.
Int J Oral Maxillofac Surg 2011;40:
393–400.
22.RuddermanRH,MullenRL.Biomechanics of the facial skeleton. Clin Plast Surg
1992;19:11.
23.Duan DH, ZangY. Does thepresence of mandibular third molars increase the risk of angle fracture and simultaneously decrease therisk ofcondylar fracture.Int
JOralMaxillofacSurg2008;37:25–8.
24.HuelkeDF,HargerJH.Maxillofacial inju-ries:theirnatureandmechanismsof produc-tion.JOralSurg1969;27:451–60. 25.Szu¨csA,Bjuta´rP,SandorGKB,Baraba´sJ.
Finiteelementanalysisofthehuman mand-ible to assess the effect of removing an impacted third molar. J Can Dent Assoc
2010;76:a72.
Address:
Ta´cioPinheiroBezerra St.TomazPompeu 340 apto802 Meireles 60.160-080Fortaleza Ceara´ Brazil