Revista de Saúde Pública
I SSN 0034- 8910 versão im pressaRev Saúde Pública 2003; 37(6)
Dental anxiety in an emergency dental service
Kazue Kanegane, Sibele Sart i Penha, Maria Aparecida Borsat t i and Rodney Garcia Rocha
Depar t am ent o de Est om at ologia da Faculdade de Odont ologia da Univer sidade de São Paulo. São Paulo, SP, Brasil
ABSTRACT
Objective
The pur pose of t his st udy w as t o assess t he fr equency of dent al anx iet y and/ or fear am ong pat ient s in an em er gency dent al ser v ice.
Methods
Resear ch w as based on int er v iew s w it h 252 pat ient s, aged 18 y ear s - old and over, at t ending a school of dent ist ry’s em ergency service in Sao Paulo, Brazil, from August t o Novem ber, 2001. Two m et hods w ere used t o m easure dent al anxiet y: t he Modified Dent al Anxie t y Scale ( MDAS) and t he Gat chel Fear Scale. The st udy group answ ered quest ions concerning m aj or com plaint , how m uch t im e elapsed since t heir last v isit t o t he dent ist and since t he init ial sy m pt om s leading t o t he cur r ent v isit t o t he em er gency ser v ice, level of educat ion, fam ily incom e and pr evious t r aum as. St at ist ical analysis (χ2 and Fisher Ex act Test ) w as per for m ed t o ev aluat e t hese char act er ist ics.
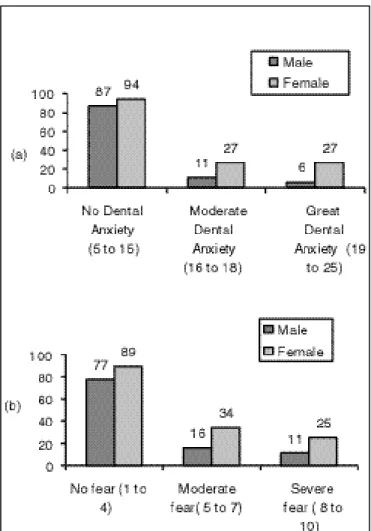
I t w as found t hat 28.17% of t his sam ple w as dent ally anxious, accor ding t o t he MDAS, and 14.29% , f elt fear r elat ed t o dent al t r eat m ent accor ding t o t he Gat chel Fear Scale. Wom en w er e m or e anx ious t han m en at a st at ist ically significant r at e ( MDAS) . The t im e elapsed since t he onset of init ial sym pt om s was m ore t han 7 days for 44.44% of t he part icipant s. A large proport ion of anxious wom en r et ur ned t o t r eat m ent dur ing t he past y ear . A pr ev ious t r aum at ic ex per ience w it h dent al t r eat m ent w as ident ified in 46.48% of t he dent ally anxious pat ient s. No significant r elat ion bet w een level of educat ion or incom e and dent al anxiet y or fear was found.
Conclusions
Dent ally anxious pat ient s frequent ly at t end em ergency care. Fem ales are m ore likely t o report high dent al anxiet y t han m ales. Previous experience seem s t o be an im port ant fact or cont ribut ing t o av oidance of dent al care.
Keywords
Dent al anx iet y . Em er gencies. Fear . Socioeconom ic fact or s.
I ntroduction
One of t he difficult ies encount er ed by t he clinician dur ing dent al car e is t he fear t hat som e pat ien t s express w it h respect t o procedures w hich w ill t ake place during t heir visit . Com ing t o t heir dent al appoint m ent s m ay represent a m aj or problem for t hese pat ient s.
Fear is a prim ary and powerful em ot ion which alert s us about im m inent danger, wit h respect t o an obj ect or sit uat ion. When danger is r ecognized, t he individual r eact s w it h a set of behavior al and neur ov eget at iv e r esponses w hich ar e accom panied by a disagr eeable sensat ion.1 6
When danger is not evident , but pr esent s it self in a vague and per sist ent m anner, or w hen signs of im m inent danger are not consciously perceived, it is denom inat ed a st at e of apprehension, in w hich t he ex ist ence of anx iet y m ay be v er ified.1 6 I t is not consciously cont r olled, t hat is, people do not hav e t he capacit y t o int er r upt it . Anx iet y also aggr av at es psy chological suffer ing caused by pain.
Childhood is t he crit ical period for t he developm ent of anxiet y. Approxim at ely one fourt h of t he adult Am erican populat ion regularly avoids dent al t reat m ent due t o t raum at ic experienc es w hich occur r ed during t his period.2
Rosa & Ferreira1 7 ( 1997) also st at ed t her e w as an associat ion bet w een fear and poor or al healt h. This could be t he r esult of less fr equent at t endance t o dent al ser v ices by pat ient s w ho fear t r eat m ent . Usually, pat ient s w ho suffer fr om dent al anxiet y w ait longer per iods of t im e befor e scheduling an appoint m ent and oft en cancel it . Am ong t he m aj or r easons given for avoiding dent al visit s ar e cost s ( 75. 4% ) and fear ( 36. 9% ) of t r eat m ent . Tw ent y - t hr ee per cent of t he people who did not regularly at t end dent al ser v ices, st at ed t hat fear w as t he r eason for non - at t en dan ce. 8
Accor ding t o Milgr om et al1 3 ( 1988) , pat ient s under fort y years old m ay be 1.5 t im es m ore anxious t han t hose over for t y. Anot her finding m ent ioned in t he lit er at ur e is t hat w om en t end t o r epor t higher levels of anxiet y t han m en.4 , 1 0 , 1 1 , 1 7
I n em er gency dent al ser v ices, bot h in pr iv at e and in dent al school clinics, t he r eason for at t endance is, in t he m aj or it y of cases, a com plaint of pain.
Clinical pr act ice suggest s t hat lev els of anx iet y and fear am ong em er gency pat ient s com ing t o a clinic are great er t han in t he general populat ion.
Since a delay in seek ing car e m ay be due t o dent al anx iet y or fear , t his st udy pr oposed t o assess t he frequency of anxious pat ient s at t ending a dent ist r y school’s em er gency clinic, associat ing anx iet y t o t he under t ak en pr ocedur e, t im e elapsed since t he last v isit t o t he dent ist , t im e since t he sy m pt om s appeared, previous hist ory of t raum a and socio - econom ic char act er ist ics of t he sam ple.
Methods
Resear ch w as based on st r uct ur ed int er v iew s, under t ak en w it h pat ient s w ho sought t he em er gency clinic of a dent ist ry school in t he m unicipalit y of Sao Paulo bet ween August and Novem ber 2001, while w ait ing t o be at t ended. An av er age of eight hundr ed pat ient s of all ages is at t ended per m ont h at t his ser v ice. The m aj or com plaint , in t he m aj or it y of cases, w as t oot hache, r esult ing eit her fr om t oot h decay and it s consequences or from periodont al disease. I nclusion crit eria for part icipat ing in t his st udy w ere: being 18 years old or over and agreeing t o part icipat e in t he invest igat ion and signing a t erm of inform ed consent . Pat ient s w ho did not know how t o read w ere not excluded from t his st udy. I n t hese cases, t he t er m of consent and t he quest ionnair e w er e r ead t o t hose w ho w ished t o par t icipat e. All int er v iew s w er e conduct ed by t he sam e per son. The pat ient s int er v iew ed w er e select ed by syst em at ic random sam pling, com prising a sam ple of 252 pat ient s ( 9.1% ) am ong t he 2,707 who at t en ded t h is ser v ice dur ing t he st udy per iod. On t he av er age, sev en pat ient s par t icipat ed in t his st udy per day , in alt er nat e day s of t he w eek so as t o cont em plat e all day s. One pat ient w as allot t ed t o par t icipat e in t he inv est igat ion am ong each t hr ee w ho fulfilled t he r equirem ent s m ent ioned above. The r at e of r efusal w as sm all: only 3 of 255 pat ient s w ho w er e inv it ed t o par t icipat e did not agr ee t o fill out t he quest ionnaire.
Pat ient s w er e char act er ized accor ding t o sex , age, educat ional lev el and fam ily incom e. They w er e ask ed quest ions concer ning t he t im e per iod elapsed since t heir last visit t o a dent al ser v ice and bet w een t he onset of t he cur r ent sy m pt om s and t he pr esent v isit t o t he em er gency dent al ser v ice. Each pat ient w as also ask ed t o st at e t he cur r ent com plaint , int ensit y of pain ( if he/ she w as not in pain at t he m om ent of t he int er v iew , t he pat ient w as ask ed t o r eply how int ense t he pain w ould hav e t o be, supposing he/ she w as in pain, for him / her t o seek a dent ist ) and if he/ she associat ed any previous experience w it h his/ her fear of dent al t r eat m ent . The em er gency pr ocedur e car r ied out in each case w as also r egist er ed.
How ev er , since Cor ah’s or iginal scale, t r anslat ed t o Por t uguese by Per eir a et al1 4 ( 1995) , did not refer t o local anest hesia, Hum phris et al.9 int r oduced an addit ional quest ion on anest hesia in t he MDAS, w hich w as also included in t his st udy . The MDAS is com posed of fiv e quest ions each of w hich has fiv e alt ernat ive answers, ranging from 1 ( no anxiet y) t o 5 ( ext rem e anxiet y). Upon answering all five qu est ions, t he low est scor e possible is fiv e, w hich w ould cor r espond t o no anx iet y and t he highest scor e possible is t w ent y fiv e, w hich w ould cor r espond t o ex t r em e anx iet y . The aut hor s hav e est ablished t hat subj ect s w it h MDAS scor es of 16 and abov e ar e dent ally anxious w hereas t hose w it h scor es higher t han 19 ar e consider ed dent ally phobic.9
The Gat chel Fear Scale is a t en- point fear scale, in w hich one r epr esent s “ no fear ” and 10 r epr esent s “ int ense fear ” . Subj ect s scor ing for m eight t o t en w er e classified as having a high level of fear.6
The dat a obt ained w as subm it t ed t o st at ist ical analy ses, using t w o non- par am et r ic t est s – Chi- square d t est s and Fisher Ex act Test - t o det er m ine t he ex ist ence of significant differ ences bet w een t he gr oups.
I n order t o det erm ine r eliabilit y of t he MDAS, Cr onbach’s alpha coefficient , a m et hod ut ilized t o m easure int ernal consist ency, w as em ployed.
Validit y of t he MDAS in discrim inat ing different groups was det erm ined by dividing t he sam ple in four subgr oups. The hy pot hesis t hat all subgroups analyzed m aint ained t he sam e m ean levels of dent al anx iet y w as t est ed by calculat ing t he m ean v ar iance bet w een gr oups and t he m ean v ar iance w it hin each gr oup.
Correlat ion bet ween t he MDAS and t he Gat chel Fear Scale was assessed using Spearm an’ s cor r elat ion coef f icien t .
RESULT S
One hundr ed and for t y- eight wom en and 104 m en, varying from 18 t o 81 years old were int erviewed. Am ong t he pat ient s at t ending t he em ergency service, 61.5% ( 155/ 252) had com e due t o pain not associat ed t o any ot her com pla int s. Ot her com plaint s such as edem a, periodont al com plaint s, bleeding, bad br eat h, lesions and t r aum a, occur r ed in 4.8% ( 12/ 252) of t he cases. Pain associat ed t o one of t he ot her com plaint s m ent ioned above occurred am ong 17.5% ( 44/ 252) of t he respondent s. Com plaint s not involving pain, such as rem oval of sut ures, cem ent at ion of t em porary crow ns or professional advice, w as t he m ot ive for at t ending t he service am ong 16.3% ( 41/ 252) of t he pat ient s. The t im e elapsed bet w een t he onset of t he cur r ent sy m pt om s and t he pr esent v isit t o t he em er gency dent al service was great er t han seven days in 44.4% ( 112/ 252) of t he sam ple populat ion. And 48.0% ( 121/ 252) of t he pat ient s st at ed t hat , w hen in pain, t hey only sought or w ould seek t r eat m ent once t he int ensit y of t he pain becam e unbearable.
Figure 1 - Distribution of patients according to the Modified Dental Anxiety Scale (a) and to the Gatchel Fear Scale (b).
The pr ocedur es m ost fr equent ly car r ied out w er e r elat ed t o endodont ics ( 134/ 252) , follow ed by t hose r elat ed t o per iodont ics ( 32/ 252) and t o car ies ( 30/ 252) . No significant differ ence w as found bet w een t he gr oup of pat ient s pr esent ing dent al anx iet y and/ or fear and t he gr oup of pat ient s w ho w er e not anxious (χ2> 0,05) .
Tim e per iod elapsed bet w een t he onset of t he cur r ent sym pt om s and t he pr esen t v isit t o t h e em er gency dent al ser v ice did not pr esent st at ist ically significant differ ences (χ2> 0.05) in t he MDAS, w it hin t he t im e per iods analy zed: up t o t w o day s ( 19 pat ient s w hose scor es indicat ed dent al anx iet y , 54 w hose scor es indicat ed t her e w as no dent al anxiet y) ; fr om t hr ee t o seven days ( 19 anxious pat ient s, 48 pat ient s w it h no anx iet y ) ; and, m or e t han sev en day s ( 33 anx ious pat ient s, 79 pat ient s w it h no anx iet y ) . How ev er , t her e w er e st at ist ically significant differ ences, accor ding t o t he Gat chel Fear Scale, bet w een t he gr oup w ho w ait ed up t o t w o day s t o seek t r eat m ent ( 57) and t he gr oup w ho w ait ed fr om t hr ee t o sev en day s t o do so ( 64) , at a lev el of 1% .
Am ong t he r espondent s, t her e w er e no st at ist ically significant differ ences bet w een age groups and anx iet y and/ or fear (χ2> 0.05) . The dist ribut ion of t he sam ple in age groups according t o bot h MDAS and Gat chel Fear Scale scor es is pr esent ed in Figur e 2.
Figure 2 - Distribution of patients in relation to age groups according to Corah (a) and Distribution of patients in relation to age group according to the Gatchel Fear Scale(b).
Am ong t he 252 pat ient s int erview ed, 55 st at ed t hey had a previous t raum at ic experience. A previous t oot h ex t r act ion w as r epor t ed by 17 pat ient s; 11 pat ient s w ere afr aid of local anest hesia, 7 w er e afraid of drilling and t he rem aining 20 pat ient s referred t o diverse past experiences. Previous t raum a w as ident ified in 46.5% ( 33/ 71) of t he pat ient s w ho pr esent ed dent al anxiet y, accor ding t o MDAS scor es. Ther e w er e st at ist ically significant differ ences bet w een t his gr oup and t hat of t he pat ient s w it h no anxiet y (χ2= 0.01) .
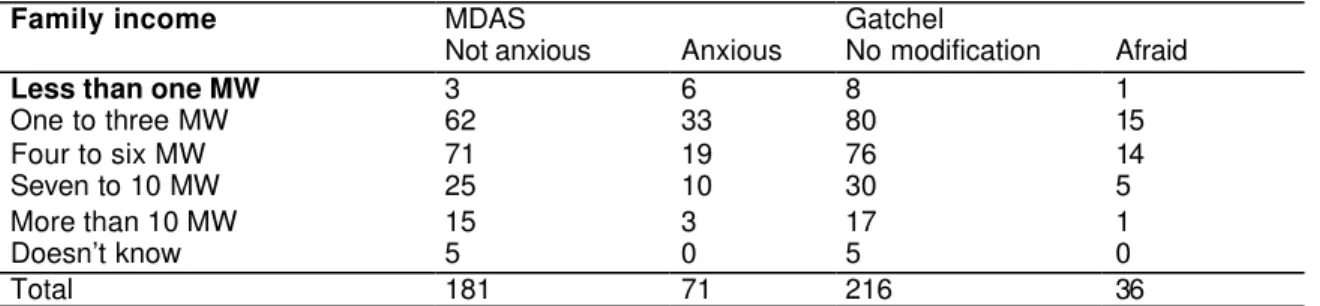
am ong t he group com posed of respondent s whose fam ilies earned up t o six m inim um wages per m ont h and t he one com posed of respondent s whose fam ilies earned m ore t han six m inim um wages.
Table 1 – Distribution of dentally anxious patients according to the MDAS and Gatchel Fear Scale in relation to family income.
MDAS Gatchel
Family income
Not anxious Anxious No modification Afraid
Less than one MW 3 6 8 1
One to three MW 62 33 80 15
Four to six MW 71 19 76 14
Seven to 10 MW 25 10 30 5
More than 10 MW 15 3 17 1
Doesn’t know 5 0 5 0
Total 181 71 216 36
MW - Minimum Wage
MDAS – Modified Dental Anxiety Scale.
Gatchel – Fear Scale
Table 2 indicat es t hat t he educat ional lev el of pat ient s par t icipat ing in t his st udy did not pr esent st at ist ically significant differ e n ce s (χ2> 0.05) when groups A+ B+ C ( illit erat e + elem ent ary school + incom plet e j unior high school educat ion) , D+ E ( com plet e j unior high school + incom plet e high school educat ion) and F+ G+ H ( com plet e high school + incom plet e undergraduat e + com plet e undergradu at e educat ion) w er e com par ed w it h each ot her , accor ding t o bot h MDAS and Gat chel Fear Scale scor es.
Table 2 – Distribution of patients according to level of education and relation to the MDAS and Gatchel Fear Scale.
MDAS Gatchel
Level of Education
Men Women Men Women
A+B+C 7*/30** 21*/32** 9***/28**** 7***/46****
D+E 7*/26** 18*/23** 1***/32**** 9***/32****
F+G+H 3*/31** 15*/39** 1***/33**** 9***/45****
A+B+C – illiterate + elementary school + incomplete junior high school education
D+E – complete Junior high school + incomplete high school education
F+G+H – complete high school + incomplete undergraduate school+ complete undergraduate school
*/** - anxious/not anxious
***/****- afraid/no modification
quart ile analysis. The 95% confidence int ervals did not overlap ( quart ile 1: 6.6786~ 7.3849; quart ile 2: 10.5645~ 11.1498; quart ile 3: 14.1356~ 14.6263; quart ile 4: 18.6803~ 19.9228) , t hat is, all groups pr esent ed dist inct m eans. The ANOVA t est indicat ed t hat t he v ar iat ion bet w een gr oups w as m uch great er t han t he variat ion wit hin groups ( F= 663.55, P= 0, 000) .
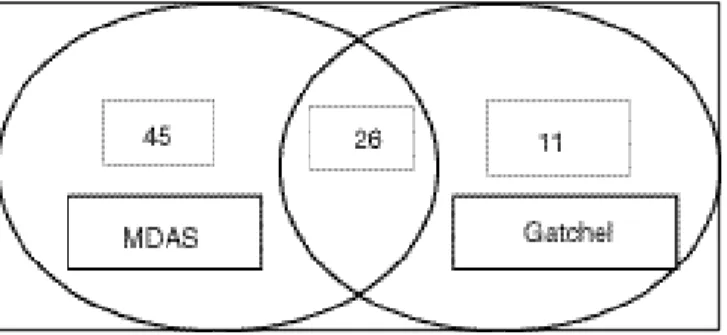
The r esult s obt ained indicat e t hat t he t w o scales ut ilized w er e not ent ir ely in agr eem ent w it h each ot her . Spear m an’s cor r elat ion coefficient bet w een t he t w o scales w as significant at t he 1% lev el w it h t he r v alue calculat ed in 0.58. Figur e 3 pr esent s a com par ison of t he t w o scales for pat ient s w it h anxiet y and/ or fear.
Figure 3 – Overlap between the two scales utilized for detecting patients with fear and/or anxiety.
D ISCUSSION
I n spit e of im provem ent s in dent al equipm ent s and procedures and m et ho ds of pr ev ent ion, dent al anx iet y , pain and/ or discom for t associat ed t o dent al t r eat m ent seem not t o hav e changed ov er t he y ear s.
I n t his inv est igat ion, t he pat ient s w er e 18 y ear s old and ov er , and t hey w er e int er v iew ed w hile w ait ing t o be at t ended in t he em er gency ser vice of a dent ist r y school. I n t his set t ing, bot h individuals w ho w er e anx ious due t o t he sit uat ion and t hose w ho had dent al anx iet y could be found. I n a st udy car r ied out am ong new pat ient s of a dent al em er gency clinic, Kaakko et al 1 0 ( 1999) found a 21.8%
pr ev alence of dent al anx iet y . Am ong adult s int er v iew ed at hom e, pr ev alence of dent al anx iet y r anged from 7.2% t o 23.4% , when using ut ilizing diverse inst rum ent s developed in order t o m easure dent al anx iet y .5 , 8 , 1 2 , 1 3
An analysis of t he int ern al consist ency of t he MDAS w as car r ied out in or der t o assess t he r eliabilit y of t he inst r um ent and a 0.74 coefficient w as obt ained, suggest ing good int er nal consist ency of t his scale. Aft er analy zing discr im inant v alidit y , it w as possible t o conclude t hat t he MDAS result ed in a m easure capable of discrim inat ing not only ext rem e groups but also t he four quart ile groups.
The t w o scales being assessed w er e not ent ir ely in agr eem ent w it h each ot her. I n t he pr esent st udy , t he pr ev alence of anx iet y w as 28.2% . I n ot her st udies t hese v alues v ar ied due t o differ ences in t he basis of each scale, as w ell as differ ences in t he populat ion sam ples select ed for each inv est igat ion. While t he Gat chel Fear Scale present s m ore rigid lim it values, t he MDAS analyses bot h em ot ional and physiological r esponses.1 2
scales.9 Furt herm ore, pat ient s m ay have difficult ies in adm it t ing t heir em ot ions. However, our st udy indicat ed t hat w om en adm it t heir anxiet y m ore t han m en do, w hich is consist ent w it h t he result s found in ot her st udies as w ell. 4 , 1 0 , 1 1 , 1 7
Wom en w hose scor es indicat ed t he pr esence of dent al anx iet y sought t r eat m ent m or e fr equent ly t han m en and r et ur ned t o t he dent ist in less t han one year , w hich w as sooner t han t heir m ale count er par t s. The m aj or it y of t he dent ally anx ious pat ient s had sought t r eat m ent w it hin t he 12 m ont hs pr ior t o t he cur r ent dent al v isit . I n t his case, t he r esult s of our st udy differ from t hose of Hakeberg et al7 ( 1992) , in w hich anxious pat ient s resum ed t reat m ent aft er a period of over t w o years. Rosa & Ferreira1 7 ( 1997) verified t hat 75.28% of t he respondent s classified as dent ally anxious had n ot gon e t o t h e dent ist in t he past 12 m ont hs. How ev er , in a dom est ic sur v ey car r ied out in t he m et ropolit an region of Sao Paulo in order t o verify t he reasons for non- at t endance am ong dent al pat ien t s, Cesar et al3 ( 1999) observed t hat am ong 68.2% of t he individuals w ho had not been t o t he dent ist in t he previous 12 m ont hs, only 3.25% claim ed t hey did not do so due t o “ fear of t he dent ist ” .
Ther e w er e st at ist ically significant cor r elat ions bet w een dent al fear , accor ding t o scor es obt ained by t he Gat chel Fear Scale, and t w o differ ent per iods of t im e elapsed bet w een t he onset of sy m pt om s and t he cur r ent v isit t o t he em er gency dent al ser v ice. When t he gr oup of pat ient s w ho at t ended t r eat m ent w it hin t w o day s of t he onset of sy m pt om s w er e com par ed t o t he gr oup w ho sought t r eat men t t h r ee t o sev en day s aft er t he onset of sy m pt om s, it w as obser v ed t hat t he m aj or it y of pat ient s w ho pr esent ed scor es associat ed w it h dent al fear sought t r eat m ent sooner . This suggest s t hat em er gency pat ient s w ho pr esent dent al fear seek t r eat m ent at t he onset of sy m pt om s. This at t it ude m ay r epr esent an at t em pt t o solve t he odont ological com plaint as quickly as possible, avoiding possible com plicat ions and t he r ecr udescence of t he pr oblem .
I t w asn’t possible t o est ablish a r elat ionship bet w een age and anxiet y in t he st udy sam ple, in consonance w it h Doer et al5 ( 1998) and Kaakko et al1 0 ( 1999) . However, som e aut hors affirm t hat
t her e is an inv er se r elat ion bet w een t hese fact or s.7 , 1 1 , 1 3
Fear is a pr im ar y em ot ion t hat indicat es t hat a danger ous sit uat ion w as r ecognized, leading t he indiv idual t o concent r at e all his at t ent ion on t his ev ent . Anx iet y r epr esent s a fear w hich w as t ransferred from a real t o an im aginary sit uat ion, result ing from sim ilar fact s or t hat recall a previous sit uat ion.2 Thus 46.48% of t he pat ient s classified as anxious report ed having lived a t raum at ic ex per ience r elat ed t o r ecent odont ological pr ocedur es. How ev er , Ander son2 ( 1997) st at es t hat dent al anx iet y and fear is oft en a consequence of a pr ev ious t r aum at ic st or y of t r eat m ent , w hich fr equent ly occur s in childhood.
Educat ional level and fam ily incom e w ere not associat ed t o anxiet y in t his st udy, a result sim ilar t o t hat found by Hak eber g et al7 ( 1992) and Rosa & Ferreira1 7 ( 1997) . However, it should be considered t hat t he m aj or it y of pat ient s t hat sought t his em ergency clinic were from low incom e fam ilies and t heir lev el of educat ion cor r esponded t o high school gr aduat es or less. I t w ould be necessar y t o increase t he num ber of individuals in t he sam ple wit h larger fam ily incom es and higher levels of educat ion in or der t o confir m t hat t her e w as no r elat ionship bet w een t hese fact or s and anx iet y .
Based on t he fear and anx iet y scales, it w as v er ified t hat t he r esult s w er en’t ent ir ely in agr eem ent , alt hough t he v alidit y of t hese m et hods has been r ecognized and t hey m ay be useful t o ident ify pat ient s w it h dent al anx iet y or fear . I n t he pr esent st udy , anx ious w om en w er e pr esent in gr eat er num ber at t he em ergency dent al clinic. Previous hist ory of t raum a was an im port ant fact or in t he developm e nt of dent al anx iet y .
as socio - econom ic fact or s , genet ic fact or s and t hose associat ed w it h fam ily or ganizat ion ar e am ong t he fir st lev el of causat ion and m ay influence fact or s locat ed at low er lev els, such as behav ior al fact or s, w her e w e find t he r ole of t he dent ist as w ell as k now ledge and at t it udes relat ed t o dent al healt h, am ong which are anxiet y and fear.1 5 Ther efor e, ot her fact or s besides t hose included in t his st udy m ay be fur t her invest igat ed so as t o shed som e light on t he pr oblem of dent al anxiet y/ fear .
REFEREN CES
1. Aart m an I HA. Reliabilit y and validit y of t he short version of t he Dent al Anxiet y I nvent ory. Com m
Dent Oral Epidem iol 1998; 26: 350- 4 .
2. Anderson JW. Fear in dent al chair. Or al Healt h 1997; 87: 9- 12.
3. Cesar CLG, Narvai PC, Gat t ás VL, Figueiredo GM. “ Medo de dent ist a” e dem anda aos serviços odont ológicos. RGO 1999; 47: 191- 4 .
4. Corah NL, Gale EN, I llig SJ. Assessm ent of a dent al anx iet y scale. J Am Dent Assoc 1978; 97: 816- 9.
5. Doerr PA, Lang WP, Nyquist LV, Ronis DL. Fact ors associat ed w it h dent al anx iet y . J Am Dent Assoc
1998; 129: 1111- 9 .
6. Gat chel, R. The pr ev alence of dent al fear and av oidance: ex panded adult and r ecent adolescent sur v ey s. J Am Dent Assoc 1989; 118: 591 - 3 .
7. Hakeberg M, Berggren U, Carlsson SG. Prevalence of dent al anxiet y in an adult populat ion in a m aj or urban area in Sweden. Com m unit y Dent Oral Epidem iol 1992; 20: 97 - 101.
8. Haugej orden O, Klock KS. Av oidance of dent al v isit s: t he pr edict iv e v alidit y of t hr ee dent al anx iet y scales. Act a Odont ol Scand 2000; 58: 255- 9 .
9. Hum phris GM, Morrison T, Lindsay SJE. The m odified Dent al Anxiet y Scale: validat ion and Unit ed Kingdom norm s. Com m unit y Dent Healt h 1995; 12: 143- 50.
10. Kaakko T, Get z T, Mar t in MD. Dent al anxiet y am ong new pat ient s at t ending a dent al school emerg ency clinic. J Dent Educ 1999; 63: 748- 52.
11. Liddell A, Lock er D. Gender and age differ ences in at t it udes t o dent al pain and dent al cont r ol.
Com m unit y Dent Oral Epidem iol 1997; 25: 314 - 8 .
12. Locker D, Shapiro D, Liddell A. Who is dent ally anxious? Concordance bet w een m easur es of dent al anx iet y . Com m unit y Dent Oral Epidem iol 1996; 24: 346- 50.
14. Pereira LHMC, Ram os DLP, Crosat o E. Ansiedade e dor em odont ologia – enfoque psicofisiopat ológico. Rev APCD 1995; 49: 285- 90.
15. Pet r y PC, Vict or a CG, Sant os I S. Adult os liv r es de cár ie: est udos de casos e cont r oles sobr e conhecim ent os, at it udes e pr át icas pr ev ent iv as. Cad Saúde Pública 2000; 16: 145- 53.
16. Rocha RG, Araúj o MAR, Soares MS, Borsat t i MA. O m edo e a ansiedade no t rat am ent o odont ológico: cont r ole at r avés de t er apêut ica m edicam ent osa, I n: Feller C, Gor ab R. At ualização na
Clínica Odont ológica. São Paulo: Ed. Ar t es Médicas; 2000. p. 387- 410.
17. Rosa AL, Fer r eir a CM. Ansiedade odont ológica: nível de ansiedade, pr evalência e com por t am ent o dos indivíduos ansiosos. RBO 1997; 54: 171- 4.
Address to correspondence
Sibele Sart i Penha
Faculdade de Odont ologia da Universidade de São Paulo Dept o de Est om at ologia - Disciplina de Clínica I nt egrada Av. Prof. Lineu Prest es, 2227 Cidade Universit ária 05508 - 900 São Paulo, SP, Brasil
E- m ail: sibsar t [email protected]
Received on 26/ 6/ 2002. Reviewed on 29/ 4/ 2003. Approved on 3/ 7/ 2003.
© 2 0 0 3 Fa cu lda de de Sa ú de Pú blica da U n iv e r sida de de Sã o Pa u lo
Ave nida D r . Ar na ldo, 7 1 5 0 1 2 4 6 - 9 0 4 Sã o Pa ulo SP Br a zil
Te l./ Fa x : + 5 5 1 1 3 0 6 8 - 0 5 3 9