COPI NG STRATEGI ES OF OSTOMI ZED I NDI VI DUALS
Nat alia Cam pos Bar n abe1 Magda Cr ist ina Queir oz Dell’Acqua2
Bar n abé NC, Dell’Acqu a MCQ. Copin g st rat egies of ost om ized in div idu als. Rev Lat in o- am En f er m agem 2 0 0 8
j ulho- agost o; 1 6 ( 4 ) : 7 1 2 - 9 .
This st udy aim ed at under st anding t he ex per ience of indiv iduals w it h int est inal div er sions as r egar ds coping
w it h t heir new life condit ions. The qualit at iv e appr oach w as used, inv olv ing 11 ost om ized subj ect s. The dat a
were collect ed by m eans of sem i- st ruct ured int erviews which were t aped and lat er fully t ranscribed and analyzed
according t o Cont ent Analysis as proposed by Bardin and t he Coping t heoret ical fram ework . The findings in t he
st udy were evidenced by t hree core cat egories denom inat ed: i did not choose it ; i had t o accept it and i have
t o live wit h t he ost om y. The form t o m anage t he condit ion of being ost om ized was revealed by coping st rat egies
which were based on bot h em ot ions and t he problem it self. The st udy cont ribut ed for reflect ion and applicat ion
of know ledge in assist ance pr act ice and t eaching for car e t he ost om ized.
DESCRI PTORS: ost om y ; adapt at ion, psy chological; nur sing
ESTRATEGI AS DE ENFRENTAMI ENTO ( COPI NG) EN PERSONAS OSTOMI ZADAS
El obj et iv o del est udio fue com pr ender la ex per iencia que per sonas con der iv aciones int est inales pr esent a al
enfrent ar est a nueva condición de vida. Se ut ilizó un enfoque de nat uraleza cualit at iva, con 11 suj et os est om izados.
Los dat os fueron recolect ados a t ravés de ent revist as sem iest ruct uradas, grabadas y post eriorm ent e t ranscrit as
en su t ot alidad, siendo analizadas según el Análisis de Cont enido de Bardin y el fundam ent o t eórico de Coping.
Los hallazgos del est udio fuer on en t r es cat egor ías cent r ales, denom inadas: no lo elegí; t uv e que acept ar lo y
con ( v iv o) con la est om ía. La est r at egia par a con t r olar la con dición , ser est om izado, se r ealizó a t r av és de
est r at egias par a en f r en t ar t an t o aspect os em ocion ales com o el pr oblem a en sí. El est u dio con t r ibu y ó par a
r eflex ionar y ut ilizar el conocim ient o en la pr áct ica asist encial y par a la educación en cuant o al cuidado del
en t om izad o.
DESCRI PTORES: ost om ía; adapt ación psicológica; en fer m er ía
ESTRATÉGI AS DE ENFRENTAMENTO ( COPI NG) DE PESSOAS OSTOMI ZADAS
Est e t r a b a l h o o b j et i v o u co m p r een d er a ex p er i ên ci a d e p esso a s co m d er i v a çõ es i n t est i n a i s, q u a n t o a o
en f r en t am en t o à n ov a con d ição d e v id a. Realizou - se est u d o q u alit at iv o, sen d o en t r ev ist ad os 1 1 su j eit os
ost om izados. Os dados for am colet ados por m eio de ent r evist as sem i- est r ut ur adas, gr avadas e post er ior m ent e
t ranscrit as na ínt egra e foram analisadas segundo a propost a de análise de cont eúdo de Bardin e do referencial
t eór ico de Coping . Os achados do est udo ev idenciar am - se por t r ês cat egor ias cent r ais: eu não escolhi; t iv e
que aceit ar e con( vivo) com a ost om ia. A for m a par a m anej ar a condição de est ar ost om izado r evelou- se por
est r at ég ias d e en f r en t am en t o t an t o b asead as n a em oção, com o n o p r ob lem a. O est u d o con t r ib u iu p ar a a
r eflex ão e a ut ilização do conhecim ent o na pr át ica assist encial e de ensino par a cuidar do ost om izado.
DESCRI TORES: ost om ia; adapt ação psicológica; en fer m agem
1
RN, e- m ail: nat [email protected] .br; 2 Ph.D. in Nursing, Facult y, e- m ail: m queiroz@fm b.unesp.br. Sao Paulo St at e Universit y “ Júlio de Mesquit a Filho”, Medical School at Bot ucat u, Brazil.
I NTRODUCTI ON
G
iv in g car e t o ost om ized pat ien t s r equ ir esu n d e r st a n d i n g t h e m , si n ce t h e co m p r o m i si n g o f v a r i o u s d i m e n si o n s i n t h e i r n e w l i f e co n d i t i o n i s
ev idenced by significat ions and sy m bolic ex pr essions
of a singular experience in t he healt h- disease process, w hich br ings w ays t o adapt .
The m ain idea in t his st udy aim s at showing
coping st rat egies, which are defined as a process wit h
t h e p u r p o se t o co n t r o l t h e r e q u i r e m e n t s o f t h e i n d i v i d u a l - e n v i r o n m e n t r e l a t i o n s h i p t h a t w i l l b e
designed by individuals wit h int est inal st om as in t heir
daily liv es.
By perform ing as a nurse/ professor conj oint ly
w it h a gr oup of under gr aduat e nur sing st udent s in a
specialized public service, t he Ost om ized Pat ient Care Cent er (Núcleo de Assist ência ao Ost om izado ( NAO),
w hich has assist ed ost om ized pat ient s in t he r egion
con sist in g in t h e Region al Healt h Div ision ( DI R XI )
s i n c e t h e Ce n t e r w a s e s t a b l i s h e d i n 1 9 9 4 , t h e i m p o r t a n ce o f d i a g n o si n g a n d u n d e r st a n d i n g o u r
cl i en t s’ r eq u i r em en t s w a s a ck n o w l ed g ed so a s t o
pr opose an indiv idualized int er locut ion- based for m of car e giv ing( 1).
An ost om ized p er son is on e w h o h as b een
subm it t ed t o an ost om y surgery, which is t he opening of t he abdom inal w all and of an int est inal or ur inar y
segm ent w it h t he pur pose t o div er t fecal or ur inar y t r ansit t o t he ex t er nal env ir onm ent . This sur ger y is
at t r ibut ed t o v ar ious causes, am ong w hich t he m ost f r e q u e n t a r e t r a u m a s , c o n g e n i t a l d i s e a s e s ,
i n f l a m m a t o r y d i s e a s e s , t u m o r s , a n d b o w e l a n d bladder can cer( 2 ).
I n t his st udy, int est inal rat her t han urological d iv er sion s w ill b e ap pr oach ed du e t o t h e in f er en ce
t hat different effluent s m ay result in people’s dist inct b eh av ior s.
Wh en f acin g t h e p ost op er at iv e st om a, t h e
ost om ized pat ient begins t o deal wit h t his new realit y, sh o w i n g v ar i o u s f eel i n g s, d i f f er en t an d i n d i v i d u al
behav ior s and r eact ions. The im pact of t he pr esence of ost om y d et er m in es an alt er at ion in b od y im ag e
and different react ions occur, depending on individual ch ar act er ist ics, social su ppor t f ou n d by t h e pat ien t
and on t he per cept ion of loss ex per ienced( 3).
Th e lit er at u r e an d t h e ex per ien ce in giv in g c a r e t o o s t o m a t e s s h o w t h a t s u c h i n d i v i d u a l s
experience various losses in t heir lifet im e, which m ay be real or sym bolic. They face t he loss of self- est eem ,
and t hat m ay lead t o a feeling of disrespect in face of
s o c i e t y. Th e l o s s p e r c e i v e d b y t h e i n d i v i d u a l i m m e d i a t e l y f o l l o w i n g o s t o m y i s t h a t o f t h e
ph y siological an d an at om ical fu n ct ion of defecat in g. I n t his condit ion t he ost om at e is a person who will not
sit on a t oilet , but will have t o discreet ly pour his feces an d f ace an ar t i f i ci al an u s t h at can n o l o n g er b e
con t r olled( 4 ).
Aft er surgery, t he ost om at e t hinks about how
t o r esu m e h is lif e, t h at is, h ow t o in cor p or at e h is concer ns r elat ed t o t he m or e pr act ical aspect s of his
lif e, su ch as t h e p ossib ilit y of p er f or m in g self - car e and m aint aining his previous social, int erpersonal and
leisur e act iv it ies. Addit ionally, issues concer ning t he
p u r c h a s e o f d e v i c e s , f r e q u e n c y o f m e d i c a l appoint m ent s and how t o deal wit h t he difficult ies t hat
m ay ar ise ov er t he adapt at ion per iod ar e par t of an ost om at e’s life. Ot her challenges are also added, such
as caring for t he st om a, concern about ot hers’ opinions and his sexualit y as well as concerns about his diet( 3- 4).
An ost om at e’s ex per ience gr adually changes
over t im e, and depending on t he developm ent of his disease and t he possibilit ies of adapt at ion found, t he
ost om at e dev elops copin g st r at egies w it h w h ich h e b eg in s t o d eal w it h t h e d aily p r ob lem s or ch an g es
occurring as a result of t he ost om y. To t hat end, t he person needs a personal period of t im e t o t hink about
an d ad ap t t o h i s n ew o st o m at e’s co n d i t i o n . Su ch period of t im e m ay t ake days, weeks or m ont hs, and
encouragem ent and reinforcem ent from ot her people, r elat iv es or pr of ession als par t icipat in g in t h e social
suppor t pr ov ided t o him ar e essent ial( 3).
Th e e x i s t e n c e o f Ca r e Pr o g r a m s f o r Ost om ized Pat ient s m aint ained by t he public ser v ice
lar gely con t r ibu t es t o adapt at ion , sin ce t h er e is an oppor t unit y for t he ex change of ex per iences am ong
ost om at es, t he provision of pouches and support from a group of professionals who favor learning as regards
car ing for t he st om a and r esum ing self- est eem( 3). I n f ace of t h e com plex it y of t h e t r eat m en t
and r ehabilit at ion of ost om at es, t his st udy aim ed at u n d e r st a n d i n g t h e e x p e r i e n ce o f i n d i v i d u a l s w i t h
int est inal div er sions as r egar ds coping w it h t he new life condit ion.
TH EORETI CAL AN D M ETH OD OLOGI CAL
DESI GN
Wh en b eg i n n i n g t h e co m p o si t i o n o f t h ese
t h eor et i cal p r esu p p osi t i on s, t h e co p i n g con cep t i s
int er poses bet w een him and t he ev ent per ceiv ed as
t hr eat ening in or der t o m ast er, t oler at e or r educe it s
im pact upon his physical and psychological well- being”.
According t o aut hors coping is defined as “ t he set of
cognit ive and behav ioral effor t s int ended t o m ast er,
reduce or t olerat e int ernal or ext ernal dem ands which
t h r eat en or su r pass an in div idu al’s r esou r ces” ; t h is
r esponse is called “ coping st r at egy ”( 5- 6).
Wit h respect t o t he coping funct ions classified
t h e m i n t o t w o d i v i si o n s: p r o b l e m - so l v i n g co p i n g
st r at eg ies an d em ot ion - f ocu sed cop in g st r at eg ies.
Pr o b l e m - s o l v i n g c o p i n g r e f e r s t o t h e e f f o r t s t o
m anage or change pr oblem s or also t o im pr ov e t he
r elat ion sh ip b et w een p eop le an d t h e en v ir on m en t .
These are st rat egies t hat are referred t o as adapt ive,
w hich ar e m or e closely r elat ed t o r ealit y and t o t he
p ossib ilit y of r em ov in g or m in im izin g t h e st r essf u l
source. Em ot ion- focused coping st rat egies involve t he
at t em pt t o r eplace or r egulat e t he em ot ional im pact
of st r ess on t h e in div idu al. Th ey m ain ly st em f r om
defensiv e pr ocesses w hich cause indiv iduals t o av oid
conscious confront at ion wit h t he t hreat ening realit y( 6).
This was a qualit at ive st udy perform ed at t he
Ost om ized Pat ient Care Cent er (Núcleo de Assist ência
a o O s t o m i z a d o ( N A O )) i n c o n n e c t i o n w i t h t h e
Co l o p r o ct o l o g y Ou t p a t i e n t Un i t o f t h e Un i v e r si t y
Hospit al Gast r osu r ger y Depar t m en t of t h e Bot u cat u
School of Medicine - UNESP.
Eleven subj ect s w it h int est inal diver sion w ho
had pr ev iously agr eed t o par t icipat e in inv est igat ion
w e r e e v a l u a t e d i n t h e s t u d y. Th e s a m p l e w a s
com p osed u n t il d at a w er e sat u r at ed , accor d in g t o
sy st em s dev eloped in qualit at iv e r esear ch.
The pr oj ect w as subm it t ed t o and appr ov ed
o f b y t h e Et h i cs a n d Resea r ch Co m m i t t ee o f t h e
Bot ucat u School of Medicine – UNESP ( OF.119/
2006-CEP) , and t he individuals agreed t o part icipat e in t he
st udy by signing an I nfor m ed Consent For m .
Th e dat a w er e collect ed by sem i- st r u ct u r ed
int er v iew s, t ape- r ecor ded and lat er fully t r anscr ibed
by t he r esear cher.
I nit ially, t he individual and social cont ext s of
t h e su b j ect s in v olv ed in t h e st u d y w er e id en t if ied
accor ding t o t he follow ing dat a: age, sex, educat ion,
p r of ession / occu p at ion , r eason f or ost om y, t im e of
ost om y, t em p or ar y or d ef in it iv e ost om y. Nex t , t h e
guiding quest ions below w er e applied:
- When were you t old about t he ost om y, and how did
you feel about it ?
- Tell m e about w hat it w as like in you hom e, about
you and t he st om a.
- What were t he difficult ies at t he beginning, and what
are t he difficult ies t oday st em m ing from t he fact t hat
y ou ar e an ost om at e?
- What social r oles do y ou play t oday ? What is y our
ev er y day life lik e?
- How do face t he problem t oday?
The dat a w er e obt ained by m eans of sem
i-st r u ct u r ed i n t er v i ew s, a n d a n a l y zed a cco r d i n g t o
c o n t e n t a n a l y s i s , w h i c h i s d e f i n e d a s “ A s e t o f
c o m m u n i c a t i o n a n a l y s i s t e c h n i q u e s a i m i n g a t
o b t a i n i n g , b y m ea n s o f sy st em a t i c a n d o b j ect i v e
p r o c e d u r e s f o r d e s c r i p t i o n o f m e ss a g e co n t e n t ,
in dicat or s ( qu an t it at iv e or n ot ) w h ich w ill allow t h e
in f er en ce of k n ow ledge r elat ed t o t h e con dit ion s of
pr oduct ion/ r epr oduct ion of such m essages”. Cont ent
analysis works on words and t heir m eanings, seeking
t o learn what is behind t he analyzed words, “ ... it is a
sear ch f or ot h er r ealit ies t h r ou gh ( it alicized by t h e
aut hor ) of t he m essages”( 7).
The coping t heor et ical fr am ew or k as w ell as
st udies by ost om y expert s w ere used t o analyze and
discuss t he dat a( 6).
RESULTS AND DI SCUSSI ON
Am ong t he 1 1 pat ient s fr om t he Ost om ized
Pa t i e n t Ce n t e r ( N A O) w h o w e r e i n t e r v i e w e d , 7
( 63.63% ) were fem ales, and 4 ( 36.36% ) were m ales.
Ther e w er e 4 ( 36.36% ) pat ient s in t he age r ange of
50 t o 59 years old, and t he ot hers were dist ribut ed in
t he following age ranges: 2 ( 18.18% ) were 30 t o 39
years old, 2 ( 18.18% ) were 40 t o 49, and 3 ( 27.27% )
were 60 t o 69.
As r egar ds edu cat ion , 8 ( 7 2 . 7 2 % ) pat ien t s
had not graduat ed from elem ent ary school, 1 ( 9.09% )
was illit erat e, 1 ( 9.09% ) had not com plet ed high school,
a n d 1 ( 9 . 0 9 % ) w a s a h i g h - s c h o o l g r a d u a t e .
Con cer n in g occu p at ion , 3 ( 2 7 . 2 7 % ) p at ien t s w er e
housew ives, 3 ( 27.27% ) r epor t ed t o no longer w or k,
2 ( 18.18% ) were ret ired, and t he ot hers had different
occu p at ion s.
I n 7 ( 63.63% ) of t he subj ect s, t he reason for
ost om y w as bow el cancer, and 4 ( 36. 36% ) r epor t ed
ot her causes: Cr ohn’s Disease, Ulcer at ive Rect ocolit is
+ I nt est inal Tuber culosis, I nt est inal Ulcer and Sacral
Ulcer due t o occupat ional accident s. The ost om y t im e
subjects and from 7 to 10 years in 4 (36.36% ). As regards
the type of stom a, 7 (63.63% ) presented a definitive stom a
and 4 (36.36% ) had a tem porary stom a.
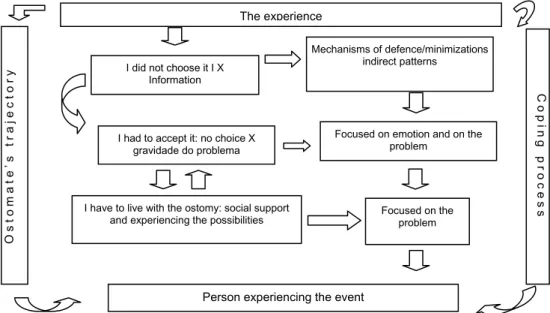
Th e co m p o si t i o n o f t h i s a n a l y t i ca l u n i t i s
r ep r esen t ed b y t h r ee cat eg or ies w h ich em er g ed in
t h e st u dy an d ar e pr esen t ed in Figu r e 1 , descr ibed
a s: I d i d n o t ch o o se i t – co n si st i n g o f t w o su b
-cat egor ies nam ed The dat e w hen infor m at ion about
t h e o s t o m y w a s g i v e n w a s r e m a r k a b l e a n d
C
o
p
i
ng
proce
ss
Ost
o
m
a
t
e
’s
trajec
to
ry
The experience
I did not choose it I X Information
I had to accept it: no choice X gravidade do problema
I have to live with the ostomy: social support and experiencing the possibilities
Person experiencing the event
Mechanisms of defence/minimizations indirect patterns
Focused on emotion and on the problem
Focused on the problem
I n a d e q u a c y i n t h e w a y t o g i v e t h e i n f o r m a t i o n
concerning t he need for ost om y; I had t o accept it –
co n si st i n g o f t w o su b - ca t e g o r i e s: I t i s a cce p t e d
because t here is no ot her opt ion and Acknowledgm ent
of t he severit y of t he problem helps wit h accept ance,
and from cat egory I have t o live wit h t he st om a t here
em er ged t he follow ing sub- cat egor ies: Being helped
t o handle t he pouch, and Everyday act ivit ies t ake place
w h en ev er possible.
Figur e 1 - Mov em ent of m eaning appr ehended, accor ding t o t he ost om at es’ ex per ience
1st Cat egory – I did not choose it
When t alking t o t he pat ient s, it was observed
t hat t hey did not have a choice as regards having t he
ost om y. And even w hen t hey w er e infor m ed about it
pr ior t o t he surgery, t hey did not hav e a m om ent t o
st op an d t h in k abou t t h eir ow n w ish es eit h er, sin ce
t he sit uat ion was put t o t hem in t he condit ion t hat “ no
m or e w ait ing w as r ecom m ended”. Also, a phy
sician-pat ient int eract ion t hat would allow for anot her choice
w as not clear.
Sub- cat egor y - The dat e w hen inform at ion about t he
ost om y w as giv en w as r em ar k able
A v er y n ot iceable aspect in t h e ost om at es’
st at em en t s w as t h e m em or y ev ok ed w h ich allow ed
f or accu r acy con cer n in g t h e d at e w h en t h ey w er e
infor m ed about t he per for m ance of t he ost om y, t hus
sh ow in g t h at it w as a r em ar k able m om en t in t h eir
liv es. . . Ah , it w as on May 1 3 , 2 0 0 5 . . . I w as t h er e in t h e
gast roent erology depart m ent , and t hen t hey t old m e t hat I had t o
be operat ed...and had t he t hing put on on May 18. E2
... Ah, it w as one m ont h before having t he surgery, on
March 7. He t old m e t hat I was going t o be operat ed and t hat I
m ay have t o use t he pouch. E3
From t he first m om ent when t he pat ient hears
about ost om y, t here are react ions t hat break all race,
color, age, cult ur e, r eligion and sex bar r ier s, for cing
h i m t o b e g i n a d e e p p e r so n a l ch a n g e . W h e n a n
indiv idual becom es ost om ized, he does not only lose
a par t of his body, but he also changes his est het ic
confor m it y and loses his capacit y or com pet ence t o
con t r ol h is f ecal an d / or u r in ar y w ast e elim in at ion .
Th er ef or e, alt h ou gh t h e st om a is som et h in g t h at is
added t o t he subj ect , it r epr esent s a v iolat ion and a
loss of cont inence, body front iers, a part of one’s self,
confidence, dignit y, independence, for m s of life and
pr ev ious r oles( 8- 9).
Su b - cat eg or y – I n ad eq u acy in in f or m in g ab ou t t h e
o st o m y
A n o t h e r n o t e w o r t h y a s p e c t i s h o w t h e
healt hcar e pr ofessional infor m s t he pat ient about t he
at t it ude t hat lack s suppor t and incr eases t he im pact
and r esponses fr om t hese people:. . .When I w as t o be
operat ed, t he doct or t old m e t hat it was necessary t o operat e, and
t hat I m ight not go back t o norm al, he t old m e! Then, I was
operat ed, and he said: look, t here’s som et hing, t he t hing is you
will have t o use t he pouch forever, t here’s no way t o go back t o
norm al E4.
The way t o t alk about t he diagnosis, t he rit uals
u sed t o in for m t h e pat ien t , t h e pr ofession al- pat ien t
con t ex t in w h ich t h e diagn osis in f or m at ion is giv en
are aspect s t hat influence t he responses t o t he disease
and t reat m ent( 10- 11).
I n t h i s ca t eg o r y, I d i d n o t ch o o se i t, t h e
defen se m ech an ism s t h at w er e com pat ible w it h t h e
b eg in n in g of t h e ex p er ien ce w er e m ad e ex p licit in
conv er gence w it h t he sub- cat egor ies.
Alt hough t he discourses revealed, t hrough t he
recording unit s, a serious and risky borderline sit uat ion
which im posed a surgery as an ext raordinary m easure
for t he m om ent , t hese individuals were st ill conscious,
aware and in cont rol of t hem selves prior t o t he surgical
procedure. And t his did not guarant ee t hem t he right
t o a decision, not even t he right t o deciding whet her
or not t o be an ost om at e. I t seem ed t o us t hat t he
p r i n ci p l e o f a l t er i t y w a s n o t g u a r a n t eed t o t h ese
p eop le.
Th e co n t act w i t h t h i s si t u at i o n sh o w s t h e
m an ag em en t of st r ess m ain ly b y in d ir ect p at t er n s,
f or alt h ou gh t h er e w as “ con sen t ”, a copin g m et h od
d e n o m i n a t e d a s d i r e ct p a t t e r n co u l d h a v e b e e n
considered by relat ing it t o t he use of abilit ies in order
t o solve t he problem ; concret ely t he process had only
been init iat ed, since t he condit ion of being ost om ized
w a s g o i n g t o b e g i n . I n d i r e ct p a t t e r n s w h i ch a r e
com pat ible w it h t he necessar y t im e t o adj ust t o t he
unsolvable sit uat ion w ere, t herefore, applicable. Such
palliat ive coping st rat egy aim s at gaining t im e for t he
individual t o be able t o access direct coping( 6).
Hence, in face of t his period in one’s life and
accor ding t o t he cont r ibut ion, each indiv idual has a
charact erist ic repert oire of defense m echanism s when
facing anxiet y- gener at ing conflict ive sit uat ions. These
ar e t o pr ot ect t he indiv idual “ against sit uat ions t hat
h e p er cei v es as d an g er o u s” an d t h r eat en i n g . Th e
f o l l o w i n g a r e ci t e d a s e x a m p l e s o f su ch d e f e n se
m echanism s: denial, w it hdr aw al, r eact ion for m at ion,
i n t r o j ect i o n , r ep r essi o n , r a t i o n a l i za t i o n , i so l a t i o n ,
r e g r e s s i o n , c o n v e r s i o n , p r o j e c t i o n , e t c . Ot h e r
unconsciously used defense m echanism s ar e apat hy,
sl e e p y w i t h d r a w a l , se l e ct i v e i n a t t e n t i v e n e ss a n d
concern. I n t his coping process, t he init ial experience w a s a n t i c i p a t e d b y t h e m a r k o f i m m a t u r e a n d
unconscious m echanism s w hich w ere com pat ible w it h t h ese su b j ect s’ r eso u r ces an d p o ssi b i l i t i es i n t h i s
ex per ien ce( 1 2 ).
Pr o c e e d i n g t o t h e s e c o n d c a t e g o r y, t h e
m ov em ent pr int ed in t his ex per ience is per ceiv ed.
2nd Cat egory – I had t o accept it
Dur ing t he int er v iew s, it w as obser v ed t hat t h e su b j ect s d i d n o t h av e an o t h er escap e i n t h i s
dilem m at ic sit uat ion, t hus having t o, som ehow, accept
t he condit ion of being ost om ized.
Sub- cat egory- I t is accept ed because t here is no ot her op t ion
A r e m a r k a b l e a sp e ct w a s t h e r e si g n a t i o n
cont ained in t he st at em ent s. There was also evidence
of t he beginning of coping in m ot ion t o be focused on t h e pr oblem . Man y in div idu als accept ed t h e ost om y
because t hey had no ot her opt ion, em phasizing t hat ev en t h ou gh it w as dif f icu lt t o liv e w it h t h e pou ch ,
t hey w ere alive and no longer felt t hat t hey w ere ill, su f f er in g pain or f acin g t h e possibilit y of im m in en t
d eat h . So m e st at em en t s al so sh o w ed a l o o k i n t o r ealit y, for t he sev er it y of t heir pr oblem led t hem t o
t he follow ing feelings.
... Ah, I ’m resigned, you know , it ’s as t hey said: You
are alive, operat ed, if you didn’t have t hat , you m ight not be able
t o be here t oday! . E1
... I was suffering a lot , it hurt a lot , and now I don’t
feel anyt hing else, t hank God I ’m fine, I j ust have t o be resigned,
you know... I ’m peaceful; I j ust have t o resign, don’t I ? What can
I do? You m ust n’t get desperat e; you m ust hold your head up and
face it ! E2
Gast roint est inal physiological alt erat ions, care f or t h e pou ch an d dif f icu lt ies t o deal w it h t h e n ew
sit uat ion led ost om at es t o pict ure t heir lim it at ions and changes t hat t ook place in t heir daily lives( 3)
.
Su b- cat egor y – Ack n ow ledgm en t of t h e sev er it y of
t he pr oblem helps w it h accept ance
An i m p o r t a n t e m e r g i n g q u e st i o n w a s t h e
not ion of t he severit y of t he problem experienced by t h e in d iv id u al, w h ich en ab led b et t er accep t an ce of
bein g ost om ized.
... I was feeling bad, you know, and t he doct ors said
day, I went t o see a specialist in m y t own, and he said: ‘Your
problem can be cured, but not here! You have t o go som ewhere
else’ ... I was resigned... I t hink t hat 4 years aft er m y surgery,
t his area was it ching, and I lift ed m y blouse... I saw t he lit t le
scrat ch... t hen I t hought : My God, I w as ent irely open, w asn’t I ?
... but I was never desperat e. I faced it ! I t hink t hat t his has
helped m e a lot , you know. E7
A l t h o u g h t h e y s h o w e d c o m m o n
ch ar act er ist ics, t h e ost om at es h ad t h eir ow n n eeds
and r esponses. Hence, t he r eact ion t o t he pr oblem s
cau sed by t h e st om a is r elat ed t o each in div idu al’s
per sonal condit ions as w ell as t o ex t er nal v ar iat ions,
such as t he qualit y of fam ily, financial and care support
r eceiv ed dur ing all phases of t he sur gical t r eat m ent
t hat generat ed t he st om a( 11- 12).
Var ious aut hor s and pr ofessional ex per ience
sh ow t h at in d iv id u als oscillat e b et w een cop in g an d
giv in g u p. Copin g, gen er ally act iv e, m ay oppose t o
non- coping. This is what was observed in m ost cases
an d p ar t icu lar ly at t h e b eg in n in g of each case as
occur r ing in t his st udy. Never t heless, aft er t he init ial
shock and each person’s peculiar durat ion, t he coping
pr ocess begins( 12- 13).
I n t his st udy, t he st rat egies used focused on
t he described em ot ion from t he at t em pt t o replace or
r egu lat e em ot ion al st r ess st em m in g f r om def en siv e
p r o cesses, w h i ch m ak es p eo p l e av o i d co n sci o u sl y
confront ing t he realit y from t he t hreat . But t here were
also ot h er pr oblem - cen t er ed st r at egies w it h ef f or t s
t o m a n a g e , a d m i n i s t r a t e o r s o m e h o w c h a n g e
problem s or im prove t he relat ionship bet w een people
and t he env ir onm ent . They focused on r ealit y, in an
at t em pt t o rem ove or at t enuat e t he st ressing source.
I n fact , t here was a choice of alt ernat ives and act ion( 6).
Such fact could be evidenced in t he cat egories
a n d s u b c a t e g o r i e s s h o w n , a n d i t c o u l d a l s o b e
observed in t he m ovem ent expressed in t he cat egory
below , w h er e lif e w as per ceiv ed as a possibilit y t o
find form s t o cope w it h sit uat ions.
3rd Cat egory – I have t o live wit h t he ost om y
I t was shown t hat t he ost om at es do not live
wit h t he st om a in t he sense of having chosen it , but
r at her t hat t hey endur e it . The pot ent ial t o liv e and
en d u r e is r ecov er ed , t h u s ad d in g m ean in g t o t h is
r eal i t y. Th er ef o r e, t h e st o m a i s n o t p ar t o f t h ese
indiv iduals’ life pr oj ect , but in t his r ealit y, t hey hav e
been led t o change t heir life habit s and t o reconsider
t heir w ishes and possibilit ies.
Sub- cat egor y – Being helped t o handle t he pouch
So m e i n d i v i d u a l s r e p o r t e d t o h a v e b e e n
h elped w it h h an dlin g t h e pou ch du e t o dif f icu lt y in
doing so, but as t im e passed, m ost of t he undert ook
self- car e. The st at em ent s r epor t t his ex per ience:
... At t he beginning, I was afraid t o t ouch it , like t his, t o
clean it ... Then I would go t o t he healt h care unit . I kept doing it
for one m ont h aft er t he surgery. I gradually got used t o it ...E3
... I handle it m yself. At t he beginning a nurse did it ;
he was m y neighbor. But t hen I realized t hat I no longer needed
it , and now I do it m yself! E6
S u b - c a t e g o r y – Ev e r y d a y a c t i v i t i e s t a k e p l a c e
w h en ev er p ossib le
The cont inuit y of daily act iv it y per for m ance
and t he search for alt ernat ives t o be able t o perform
ot her desired act ions were observed in som e report s:
... I go out as I used t o. I com e here by m yself; I drive;
I drive m y wife t o t he doct or’s; I drive m y granddaught er: I look
aft er m y gr andson. I do t he sam e t hings at hom e; I dr iv e,
anyt hing, I find t hings t o do at hom e. I j ust can’t m ake physical
effort s; t he doct or t old m e not t o, so I don’t lift heavy t hings!
And if I have t o do anyt hing, I do it sit t ing down. E5
.... We have t o look for alt ernat ives as far as possible.
I t hink it ’s sad not t o be able t o go t o church because going t o
religious services on Sundays is m y dut y as a Christ ian. I have
found an alt ernat ive: whenever I go, I sit near t he pipe organ, t he
choir! ( laught er) ... I j ust keep looking for alt ernat ives! E11
Funct ional possibilit ies aft er beginning t o use
t h e pou ch ar e associat ed w it h t h e det er m in at ion of
per spect iv es by t he pat ient him self and encour aging
social int er act ions( 3, 14).
I n t he cat egory I have t o live wit h t he st om a,
co n t a ct w i t h r e a l i t y a n d l i f e w a s o b se r v e d , a n d
alt hough it was not t hese individuals’ choice, t his realit y
a sp ect o f f er ed t h em t h e p o ssi b i l i t y t o i m p l em en t
pr oblem - solv ing coping st r at egies. The pr oblem w as
n ot solv ed du e t o t h e im possibilit y im posed by t h e
condit ion of being ill, but t he relat ionship wit h healt h
car e ser v ice w as in t en sified an d t h e lim it s t o t h ese
in d iv id u als’ liv es w er e d em ar cat ed . Th e b eh av ior s
w er e su bt le, bu t t h ey en abled t h e assu m pt ion t h at
t her e w er e pr oblem solv ing st r at egies.
Th e cop in g con cep t is cor r ob or at ed in t h is
st udy by t he evidence of t he occurrence of a dynam ic
pr ocess w hich changed accor ding t o ev aluat ions and
r e- ev alu at ion s t h at w er e con t in u ou sly per for m ed by
The ost om at es’ t r aj ect or ies w er e ev inced by
t h ese in d iv id u als’ ex p er ien ce of g oin g t h r ou g h t h e
coping process, is not a behavior consist ing of a single
dim ension. Nev er t heless, it consist s of a w ide r ange
of k n ow n beh av ior s an d per cept ion s, dist r ibu t ed in
v ar iou s lev els w h ich com pr ise, in t h e last in st an ce,
t heir coping repert oire, wit h a wide spect rum of opt ions
sh ow in g t h eir ow n r elev an ce, sin ce t h ese w er e t h e
elect ed f or m s f or copin g. Each in div idu al pr esen t ed
h i s p e cu l i a r r e so u r ce s, w h i ch co n si st e d o f t h e i r
e x p e r i e n c e s a n d i n f l u e n c e d t h e i r p e r s o n a l
r espon ses( 1 5 ).
FI NAL REMARKS
Th e set of copin g m odes u sed t o deal w it h
t he various st ressors relat ed t o t he condit ion of being
ost om ized , in clu d in g a lar g e n u m b er of r esp on ses,
w as sh ow n by t h e w ealt h of elem en t s con t ain ed in
t he int er v iew s.
Th e b e g i n n i n g o f t h e e v e n t w a s w e l l
d e m a r c a t e d b y d e f e n s e m e c h a n i s m s , w h e r e
m inim izat ion and relat ivizat ion st rat egies wit h indirect
pat t er n s w er e pr esen t ed in t h e in t er v iew s, sh ow in g
ev idence of t he difficult ex per ience and of t he init ial
im pact . Th e f or m s of copin g w it h an d bein g in t h e
pr ocess w hich enabled indiv iduals t o go ahead w hile
f aci n g su ch ad v er si t y ar e t h e co n f i r m at i o n o f t h e
r ealit y st ill per ceiv ed under t his condit ion.
At t h is m om en t , “ I d id n ot ch oose it ” w as
st at ed and r ev ealed by feelings of fear and difficult y
and discour ses such as “ t her e’s no ot her w ay ”. The
n om in at ion of t h e disease an d of t h e dev ice w h ich
w ould be par t of t his per son w er e ex pr essed in t he
int er v iew s as “ t hat t hing, st uff, I had it on” and t he
m em or y of t h e ex act dat e w h en on e w as in f or m ed
a b o u t t h e o st o m y r e f l e ct e d t h e i n t e n si t y o f t h i s
ex p er i en ce.
The w ay chosen by t he doct or t o infor m t he
p at ien t also seem ed t o sh ow a lack of con d it ion s,
p er so n al an d i n st i t u t i o n al u n p r ep ar ed n ess, w h er e
t hese people could be offered t he opt ion t o have t heir
w ill g u ar an t eed w it h su p p or t f or t h e im p act t o b e
su f f er ed .
I n t his synt hesis, cat egories “ I had t o accept
i t ” a n d “ I h a v e t o l i v e w i t h t h e o s t o m y ” a r e
dist inguished, since t hat w as w her e t he coex ist ence
of p r ob lem solv in g cop in g st r at eg ies an d em ot ion
-focused coping st r at egies w er e show n in t he coping
process by subt le behaviors. The revealed experience
o f p eo p l e l i v i n g w i t h o st o m y w a s p r esen t ed i n a
beaut iful m ov em ent and it s m eanings, w it h a not ion
of lim it s t o one’s realit y, alt hough wit h int ense life in
t his process of becom ing ill and coping wit h it .
For t his reason, it is expect ed t hat t he findings
st em m ing from t he result s in t his st udy can cont ribut e
t o reflect ion and knowledge applicat ion by care giving
an d t each in g pr ofession als w or k in g w it h ost om at es.
I t is also expect ed t hat t hey can:
I dent ify, in t he light of t he coping fram ework,
t he coping st rat egies used by ost om at es at a cert ain
m o m en t , u n d er st a n d i n g t h a t i t i s a n ex p er i en t i a l
p r o cess; m ed i at e r el at i o n sh i p s am o n g o st o m at es,
f a m i l y m e m b e r s o r si g n i f i ca n t p e r so n s w i t h t h e
pur pose t o est ablish int er locut ion so as t o r ecognize
av ailable r esou r ces, t h u s pr ov idin g su ppor t t o su ch
p at ien t s; p r ov id e car e t o ost om at es b y p er ceiv in g
t h em as people bein gs in t h e cou r se of t h eir liv es,
where t echnical knowledge is im port ant , and alt hough
t hey m ight not be st om at her apist s, t hey w ill be able
t o t ake hold of t heoret ical and part icularly of hum
an-in t er act ion elem en t s w h ich w ill gu ar an t ee t h e car
e-giv in g pr ocess.
REFERENCES
1 . Pai v a MCMS, Fon seca EC, Pessu t o J, Del l ’Acq u a MCQ.
Or g an i zação d e u m n ú cl eo d e assi st ên ci a a o st o m i zad o s
( N A O ) . I n : A n a i s d o 4 6 º Co n g r e s s o B r a s i l e i r o d e
Enferm agem ; 1994 out ubro 484- 5; Port o Alegre: Aben; 1994.
2. Gem elli LMG, Zago MMF. A int er pr et ação do cuidado com
o ost om izado na visão do enferm eiro: um est udo de caso. Rev
Lat in o am En f er m ag em 2 0 0 2 j an eir o f ev er eir o; 1 0 ( 1 ) : 3 4
-4 0 .
3 . S o n o b e H M , B a r i c h e l l o E, Z a g o M M F. A v i s ã o d o
colost om izado sobre o uso da bolsa de colost om ia. Rev Bras
Can cer ol 2 0 0 2 j u lh o- ag ost o- set em b r o; 4 8 ( 3 ) : 3 4 1 - 8 .
4 . Tr en t in i M, Pach eco MAB, Mar t in s ML, Silva DMG, Far ias
SR, Du ar t e R, et al. Viv en do com u m est om a: u m est u do
pr elim in ar. Rev Gaú ch a En fer m 1 9 9 2 j u lh o; 1 3 ( 2 ) : 2 2 - 3 .
5. Lazarus RS, Launier S. St ress relat ed t ransact ion bet w een
p e r s o n a n d t h e e n v i r o n m e n t . I n : D e r v i n LA, Le w i s M.
Per spect ives in int er nat ional psychology. New Yor k : Plenum ;
1 9 7 8 . p . 2 8 7 - 3 2 7 .
6. Lazarus RS, Folkm an S. St ress, appraisal and coping. New
Yor k : Spr in ger Pu blish in g; 1 9 8 4 .
7. Bar din L. Análise de cont eúdo. Lisboa: Edição 70; 1977.
8 . O l i v e i r a D V D , N a k a n o TTY. Re i n s e r ç ã o s o c i a l d o
o st o m i zad o . I n : San t o s VLCG, Cesar et t i I UR. Assi st ên ci a
9. Santos VLCG, Sawaia BB. A bolsa na mediação “estar ostomizado”
– “ est ar profissional” : análise de um a est rat égia pedagógica.
Rev Latino-am Enferm agem 2000 julho; 8(3): 40-50.
1 0 . Mar u y am a SAT, Zag o MMF. O p r ocesso d e ad oecer d o
port ador de colost om ia por câncer. Rev Lat ino- am Enferm agem
2 0 0 5 m ar ço- ab r i l ; 1 3 ( 2 ) : 2 1 6 - 2 2 .
1 1 . Cesar et t i I UR, San t os VLCG, Filippin MJ, Lim a SRS. O
cuidar de Enferm agem na t raj et ória do ost om izado: pré e t rans
e p ó s - o p e r a t ó r i o s . I n : S a n t o s V LCG, Ce s a r e t t i I U R.
Assist ên cia em Est om at er apia. São Pau lo: At h en eu ; 2 0 0 5 .
p . 1 1 3 - 3 1 .
12. Kaplan HI , Sadock BJ, Caner o R, Gr ebb JA. Com pêndio
d e Psi q u i a t r i a : ci ên ci a s d o co m p o r t a m en t o e p si q u i a t r i a
Recebido em : 12.9.2007 Aprovado em : 2.7.2008
clín ica. 7 ª ed. Por t o Alegr e: Ar t es Médicas; 1 9 9 7 .
1 3 . Pe t u c o V M . A b o l s a o u a m o r t e : e s t r a t é g i a s d e
enfr ent am ent o ut ilizadas pelos ost om izados de Passo Fundo/
RS [ disser t ação] São Paulo: Faculdade de Saúde Pública da
USP; 1 9 9 8 .
14. Sim m ons KL, Sm it h JA, Bobb KA, Liles LLM. Adj ust m ent
t o colost om y : st om a accep t an ce, st om a car e selt - ef f icacy
and int er per sonal r elat ionships. Jour nal of Adv anced Nur sing
2 0 0 7 d ecem b er ; 6 0 ( 6 ) : 6 2 7 - 3 5 .
15. Souza MC, Cerezet t i CRN, Souza Jr AHS, Nahas P,
Habr-Gam a A, Neder M, et al. Mu dan ças n a im agem cor por al e
a l t e r a çõ e s p si co l ó g i ca s e m p a ci e n t e s co l o st o m i za d o s e