www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Clinical
outcome
and
patient
satisfaction
using
biodegradable
(NasoPore)
and
non-biodegradable
packing,
a
double-blind,
prospective,
randomized
study
夽
Pawel
Krzysztof
Burduk
a,∗,
Malgorzata
Wierzchowska
a,
Blazej
Grze´
skowiak
b,
Wojciech
Ka´
zmierczak
c,
Katarzyna
Wawrzyniak
daNicolausCopernicusUniversity,FacultyofMedicine,OtolaryngologyandLaryngologicalOncologyCollegiumMedicum,
Toru´n,Poland
bUniversityHospital,DepartmentofOtolaryngologyandLaryngologicalOncology,Bydgoszcz,Poland
cNicolausCopernicusUniversity,FacultyofMedicine,DepartmentofPathophysiologyofHearingandBalanceSystem,
Toru´n,Poland
dNicolausCopernicusUniversity,FacultyofMedicine,DepartmentofAnesthesiologyandIntensiveTherapyCollegiumMedicum,
Toru´n,Polônia
Received15May2015;accepted4January2016 Availableonline28March2016
KEYWORDS FESSsurgery; Biodegradable packing;
Patientsatisfaction; Mucosalhealing; Follow-up
Abstract
Introduction:Nasal packingafter endoscopicsinussurgeryisusedasastandardprocedure.
The optimumsolutionto minimizeoreliminate alldisadvantagesofthisproceduremay be accomplishedusingbiodegradablepacks.
Objective: The aimofthis study was tocompare patient satisfactionandclinical outcome
associatedwithabsorbableandnon-absorbablepackingafterFESS.
Methods:Intotal,50patientswereincludedinaprospective,double-blind,randomizedtrial.
Onesidewaspackedwithpolyurethanefoam,whiletheoppositesidewaspackedwithgauze packing.Onthe2nd,10th,and30thpostoperativeday,thepatientswerequestionedwiththe aidofavisualanalogscale.Thestandardizedquestionnairesforbleeding,nasalbreathing, feel-ingofpressure,andheadachewereused.Thepresenceofsynechiae,infection,orgranulation wasnotedandrecordedwiththevideo-endoscopy.
Results:AsignificantdifferenceaccordingtolowerpressurewasfoundintheNasoPoregroup
comparedtothecontrolsondaytenaftersurgery.TheNasoPorepackinghadlowerscoreswith respecttopostoperativenoseblockageonthe2ndand10thdays.Mucosalhealingwasbetter fortheNasoPoregroup,bothatdaytenand30comparedwiththecontrolgroup.
夽 Pleasecitethisarticleas:BurdukPK,WierzchowskaM,Grze´skowiakB,Ka´zmierczakW,WawrzyniakK.Clinicaloutcomeandpatient
satisfactionusingbiodegradable(NasoPore)andnon-biodegradablepacking,adouble-blind,prospective,randomizedstudy.BrazJ Otorhi-nolaryngol.2017;83:23---8.
∗Correspondingauthor.
E-mail:[email protected](P.K.Burduk).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.01.001
resorbabletraditionalimpregnatedgauzepacking.Intensivesalinedouchesappliedthreeto fourtimesperdayaremandatoryaftertheoperationtopreventsynechiaeformationandfluid resorptionbythepacking.
Publishedby Elsevier Editora Ltda. onbehalf ofAssociac¸˜ao Brasileira de Otorrinolaringolo-giaeCirurgiaC´ervico-Facial.ThisisanopenaccessarticleundertheCCBYlicense(http://
creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE CirurgiaFESS; Tampão biodegradável; Satisfac¸ãodo paciente; Cicatrizac¸ãoda mucosa; Seguimento
Desfechoclínicoesatisfac¸ãodopacientecomousodetampãobiodegradável (NasoPore)enãobiodegradável:estudoprospectivo,duplo-cegoerandomizado
Resumo
Introduc¸ão:Otamponamentonasalapóscirurgiasinusalendoscópicaéprocedimentoderotina.
A soluc¸ão ideal para minimizar ou eliminar as desvantagens desse procedimento pode ser alcanc¸adacomousodetampõesbiodegradáveis.
Objetivo:Oobjetivodesteestudofoicompararasatisfac¸ãodopacienteeodesfechoclínico
associadosaousodetampõesabsorvíveisenãoabsorvíveisapósacirurgiafuncionaldosseios paranasais(FESS-FunctionalEndoscopicSinusSurgery).
Método: Nototal,50 pacientesforamincluídosnesteestudoprospectivo,duplo-cegoe
ran-domizado. Umdoslados foitamponadoespumade poliuretano,enquanto nooutrolado foi realizadoumtamponamentocomgaze.Nos2◦,10◦ e30◦ diasapósaoperac¸ão,ospacientes foramquestionados com aajuda deuma escala analógica visual. Foramempregados ques-tionáriospadronizadosparasangramento,respirac¸ãonasal,sensac¸ãodepressãoecefaléia.A presenc¸adesinequias,infecc¸ãoougranulac¸ãofoiregistradaporvideoendoscopia.
Resultados: Foiobservadadiferenc¸a significante,dasensac¸ãodepressão,tendosidomenor
noladotratadocomNasoPorevs.controlesno10◦ diaapósacirurgia.Otamponamentocom NasoPoreobteveescoresmaisbaixoscomrespeitoao bloqueionasalpós-operatóriono2◦ e 10◦ dias.Acicatrizac¸ãodamucosafoimelhornoladodoNasoPore,masno10◦ e30◦ dias,os resultadosforamcomparáveisaosdoladodecontrole.
Conclusão:OconfortogeraldopacienteémaiorcomousodeNasoPorevs.tamponamento
tradicionalcomgazebesuntadanãoreabsorvível.Ousovigorosodejatosdesoluc¸ãodesalina aplicadas3-4vezesaodiaéumprocedimentoobrigatórioapósacirurgia,paraevitaraformac¸ão desinequiaseparaumaabsorc¸ãonaturaldotampão.
PublicadoporElsevier EditoraLtda.emnomedeAssociac¸˜aoBrasileira de Otorrinolaringolo-giaeCirurgiaC´ervico-Facial.Este ´eumartigo OpenAccess sobumalicenc¸a CCBY(http://
creativecommons.org/licenses/by/4.0/).
Introduction
Chronic rhinosinusitis is a very common disease, and the success of treatment is dependent on effective surgery andpostoperativecare.Endoscopicsinussurgery(ESS)has becomethegold standard forthe treatmentof inflamma-tory,benignandselectedmalignantpathology.1,2Themain principlesarere-establishingventilationanddrainage with-outscarring,synechiae,andobstruction.3---5Toachievethese results,themiddlemeatusisoftenpacked.Thisprocedure should stabilize the middle turbinate, prevent synechiae formation, and act as a hemostatic agent.3---7 However, nasalpackingcouldbeasourceofpain,nasalobstruction, bleeding,anddiscomfortduringpackremoval.5,6These dis-advantagesaremostlycomparedwithnon-absorbablenasal packing.3,5---9
Recently,differentabsorbablebiomaterialshavebecome availableforuseasmiddlemeatuspackingafterfunctional endoscopicsinus surgery (FESS).3---8,10 These kind of packs donotneedtoberemovedandthereforeimprovepatient
comfort after surgery.3,4,7,8,10 The material prevents synechiaeformationandstabilizesthemiddleturbinate.It startstodissolvewithinafewdaysandcanbewashedout orsuctionedfromthenose.5,8,10
NasoPore(Polyganics --- Groningen, The Netherlands) is a biodegradable synthetic polyurethane foam, which was usedinthecurrentwork.Thepolyurethanebondsprovide strong initial compressivemechanical properties,whereas thehydrophiliccomponenttakes-upthewaterorbloodand isgraduallyfragmented.Theaimofthisstudywasto com-pare patient satisfactionand clinical outcome associated withtheabsorbableandnon-absorbablepackingafterFESS.
Methods
Studydesign
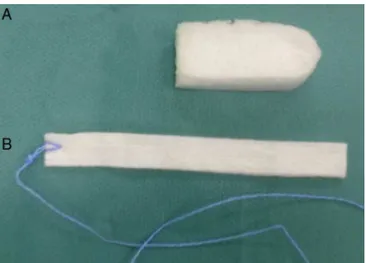
Figure1 NasoPore(A)andgauzestrip(B)packing.
surgerywhiletheoppositesidewasfilledwithpacking com-posedoftraditionalimpregnatedgauzestrip.Thisstudywas approvedbytheBioethicsCommitteeoftheNicolaus Coper-nicusUniversity(KB326/2013)andwritteninformedconsent wasobtainedfromallparticipants.
A total of 50 patients wereincluded from the Dep.of OtolaryngologyandLaryngologicalOncology.Themeanage was 47.5 years (±9.8); 22 female and 28 male patients wereincluded. The inclusioncriteriawerechronic rhinos-inusitis (CRS) with or without nasal polyps according to theEPOSguidelines11 andsymmetricalpathologybetween the nasal cavities based on computed tomography (CT) scan.12 Thestudyincluded38patientswithCRSwithnasal polypsand12 withoutnasalpolyps.The exclusioncriteria wereseptoplasty, turbinate surgery, or knownintolerance topolyurethane. In each case, bilateral surgery was per-formed to the same extent. The research was approved by the local ethics committee and informedconsent was obtained before the study. The patients were computer-randomizedtopackingtheright orleftsidewithNasoPore andtheothersidewithgauzestrip.Inallcases,the pack-ing was placed in the middle meatus at the end of the surgery.
Surgery
The surgery was performed under general anesthesia by one surgeon. To minimize bleeding and optimize the surgicalfield,theprocedureusedpremedicationwith cloni-dineandtotalintravenous anesthesia(TIVA),asdescribed previously.13 Preoperatively, all of the patients received intravenousantibiotics(cefuroxime1.5g).Attheendofthe surgery, the surgeon wasinformed by the nurseof which side to use the NasoPore, which was randomly assigned. The opposite side was packed with non-resorbable gauze strip pack. Standard 4cm NasoPore and 4cm long gauze strip withan ointment(Fig.1) wereused.The procedure utilized2gOxycortointment(1gcontains310mgof hydro-cortisoneand30mgofoxytetracycline,aswellasthebase --- Jelfa,Poland). The patientsand the observerwere not informedofwhichsidehadreceivedtheNasoPoreorgauze
packing. Table
On the 2nd, 10th, and 30th postoperative day, a physi-cian other than the operating surgeon questioned the patientswiththeaidofavisualanalogscale(VAS)and per-formed nasalendoscopy. The non-absorbablepacking was removedonthe10thdayaftersurgery.Thedatacollection wasanalogous to comparable studies, using standardized questionnaires for each side for the following parame-ters: bleeding, nasal breathing, feeling of pressure, and headache.5,6,10,14 The parameters were determined using a VAS withpossible values ranging from 0 (nosymptoms) to 10 (maximum symptoms). The presence of synechiae, infection,granulation,orre-epithelializationwasnotedand recorded with the video-endoscopy on both sides on the 10thand30thdayaftersurgery.Afterdischarge,allpatients usedanantibiotic(clarithromycin,1000mgdailyfor10days, nasal steroids (fluticasone furoate) once daily, and nasal salinedouchesuptothreetofourtimesdaily).
Statisticalanalysis
Statistical analysis was performed with Statistica soft-ware,v.10.(StatSoftInc.)Theparameterswerecompared usingthe Wilcoxon signed rank test, McNemara test, and Shapiro---Wilk’stest. The level of significance wasdefined asp<0.05.The study population wascalculatedfor error inherentinatestresult.Thepoweranalysisofthe investi-gationgroupwas80%.
Fiftypatientswererandomizedand100sinuscavitieswere treated. Theabsorbable packingwasputin 27right sides and23leftsidesofthenasalcavities.Thenon-absorbable packingwasputaccordinglyin23rightand27leftsidesof thenasalcavities.Forty-ninepatientscompletedthestudy. This wasduetoone patientrefusing toattend follow-up, ashefeltwell.TheVASresultsforpressure,noseblockage, headache,and nasal painare shown in Table1. A signifi-cant differenceaccording topressure wasfound between the NasoPore and control sides on day 10 after surgery (p<0.04).Thepatientsreportedlowerfillingofnose pres-sureontheNasoPoreside.Nodifferenceswereobservedon the2ndand30thdayspost-surgery.The NasoPorepacking hadlowerscoreswithrespecttopostoperativenose block-age(4.26vs.4.73,p<0.04)onthe2ndand10thdays(1.81
vs. 2.29, p<0.02; Table 1). The results were significant. However,therewasnosignificanceonthe30thday(0.45vs. 0.68,ns).Nevertheless,slightlylowerscoresforheadache andnasalpainwererecordedfor theNasoPoregroup dur-ingthefollow-upvisits,buttheresultswerenotsignificant
(Table1).
Assessmentofbleedingonpackingremovaldemonstrated nodifferences.Minimalbleedingwithout anyfuture inter-ventionwasobservedforonecaseineachgroup.
Forty-nine subjects returned for the assessment of mucosal healing on the 10th and 30th days after opera-tion.Endoscopicobservationsofwoundhealingaftersurgery revealedbloodcrusting,edematousswelling,and epithelial-ization.Mucosalhealing(re-epithelialization)wasbetterfor
Table2 Resultsofsynechiae,infection,andre-epithelizationbetweengroups.
Synechiae Infection Re-epithelization
N C p N C p N C p
Day2
n=50
--- --- --- --- --- --- --- ---
---Day10
n=49
0 0 ns 0 0 ns 68.1% 32.7% <0.001
Day30
n=49
3 2 ns 0 1 ns 95.7% 90.2% <0.06
N,Nasopore;C,Control;ns,notsignificant;n,numberofpatients.
theNasoPoregroup,bothondaytenand30,comparedwith thecontrolgroup(p<0.001,p<0.06).At 10thdaythe re-epithalization in studygroup was68.1% andreached over 95.7% at 30th day. The endoscopic viewat 10th day was very satisfactory compared to control group, where only 32.7%oftheoperatedfieldshowedepithelization.Inboth groupsatthe30thday,there-epithelizationlevelwasover 90%, pointing to complete healing. Nevertheless, the re-epithelializationinthecontrolgroupachievedasatisfactory levelonthe30thday(90.2%).Inthisstudy,synechiae for-mationwasobservedinthreeoftheNasoPoregroupandtwo ofthecontrolgroup(Fig.2).Nosignificancewasobserved
(Table2).Inonecaseofnon-absorbablepacking,onthe30th
dayoffollow-up,infectionwithmucopurulentdischargewas found.
Resorptionoftheabsorbablepackingwasfluentinmost cases(Fig.2).Inthreecases,someremnantsofthedressing onthe10thdaywerenoted,whichcouldresultinsynechiae formationinthelatefollow-up(Fig.2).Inthesecases,the patientsdidnotadheretotherecommendationofregular (threetofourtimesperday)nasaldouches.
Discussion
The most important considerations after FESS operations arepatientcomfort,minimizingbleeding,reductionof dis-comfortassociatedwithnasalpacking,andpropermucosal healing. As the non-resorbable (removable) nasal packing can beveryunpleasant,the differenttypes of resorbable packinghavebeeninvestigated.4---6,8,10 Someauthorsdonot supportthe useof nasalpacking at all.6,8,10,15 Conversely, middlemeatalpackinghaspreventedlateralizationof the middleturbinate,synechiaeformation,andbleeding.4,6,7,10 Usingsomeabsorbablematerials,themucosalhealing pro-cesscouldbemoreeffectiveandfaster.3,4Insomecases,the absorbablematerials couldalsobe associatedwithslower healingandsynechiaeformation. Thisisprobablybecause of the possibility of osteogenesis initiation.5 One of the newly developedbiodegradable nasalpackingmaterials is thepolyurethanefoam NasoPore,whichisusedafterFESS operations.5,10Thismaterialcouldalsobeimpregnatedwith steroidsorantibioticstoreducethepost-operative discom-fortandachievebetterclinicaloutcomes.16,17
The aim of this study wasto compare the efficacy of a biodegradable nasal packing (NasoPore) with a tradi-tionalgauzestrippackingimpregnatedwithointment(2gof
oxytetracyclineandhydrocortisone).Theointmentwasused topreventtheadherenceofthepackingtothemucosa.
Thepost-operativefeelingofpressurewashigherinthe controlgroupthanontheNasoPoreside.Onpost-operative daystwoand30,thisobservationwasnotstatistically signif-icant.Ondayten,thefeelingofpressurewasgreateronthe controlside,resultinginasignificantdifference(p<0.04). Intheauthors’opinion,thiswascausedbyresorptionofthe NasoPore,and by stable gauze strip packing and the for-mationof blood clotsaround the gauzematerial. Patient comfortappears tobe improved by the resorbable pack-ing. The same observations have been reportedby other authors.4,5,10
Parametersincludingnoseblockage,headache,andnasal painweregenerallylowerfortheNasoPoregroupthanthe controlgroup.Ondayten,astatisticallysignificant reduc-tionofnose blockage(p<0.02)intheNasoPoregroupwas observed. This was caused by resorption of the packing withlessdebridement in themiddle meatuscompared to high secretion and edema mediated by the gauze pack-ing on the other side. However, although there were no statisticallysignificantdifferencesfortheobserved param-etersduringthefollow-up,patientcomfortappearedtobe muchbetterintheNasoPoregroup.Thesameobservations weremadebyotherauthorscomparingtheusageof differ-entresorbableandnon-resorbablepackingmaterials.3,5,6,10 The study has demonstrated that NasoPore does not sig-nificantlyreduce therisk of post-operativebleeding. The sameresultswereobservedfor otherresorbableand non-resorbablenasalpackingmaterials.5---7,9,10
thatremovingthenon-absorbablepackingcouldcauselocal mucosalbleedingandaprolongedphaseofbloodcrusting, whichdelaysepithelialization.Nevertheless,thedifference almostdisappearedbythelatefollow-upvisit(p<0.06).The sameresultswereobservedbyShoman.5
Overall, theNasoPorepacking resultsin better patient comfortandabetterhealingprocessafterFESSsurgery.
Conclusion
UsingaresorbableNasoPorepackingafterFESS,thefeeling ofpressure andnose blockage inthe earlypost-operative periodweresignificantlyreduced.Theoverallpatient com-fort was higher compared to non-resorbable traditional gauzestrip packing.The wound healing wasbetter when using NasoPore, but future investigations are required. Intensivesaline douches,threetofourtimesper day, are mandatoryaftertheoperationtopreventsynechiae forma-tionandfluidresorptionbythepacking.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
This work was presented at 25th Congress of the Euro-peanRhinologicSocietyand33rdInternationalSymposium onInfectionandAllergyoftheNoseCongress,June22---26, 2014,Amsterdam,TheNetherlands.
References
1.GotlibT,Osuch-WójcikiewiczE,Held-ZiółkowskaM,Ku´zmi´nska M,NiemczykK. Endoscopictransnasal managementof sinon-sal malignancies-our initial experience. Videosurg Miniinv. 2014;9:131---7.
2.GotlibT,KrzeskiA,Held-ZiółkowskaM,NiemczykK.Endoscopic transnasalmanagementofinvertedpapillomainvolvingfrontal sinuses.VideosurgMiniinv.2012;7:299---303.
3.Franklin JH, Wright ED. Randomized, controlled, study of absorbablenasalpackingonoutcomesofsurgicaltreatmentof rhinosinusitiswithpolyposis.AmJRhinol.2007;21:214---7.
4.Berlucchi M, Castelnuovo P, Vincenzi A, Morra B, Pasquini E. Endoscopic outcomes of resorbable nasal packing after
tiverandomizedcontrolledstudy.EurArch Otorhinolaryngol. 2008;266:839---45.
5.Shoman N, Gheriani H, Flamer D, Javer A. Prospective, double-blind,randomizedtrialevaluatingpatientsatisfaction, bleeding, and wound healing using biodegradable synthetic polyurethanefoam (NasoPore)as a middlemeatal spacer in functionalendoscopicsinussurgery.JOtolaryngolHeadNeck Surg.2009;38:112---8.
6.LeunigA, BetzCS,SiedekV,Kastl KG. CMCpackingin func-tionalendoscopicsinussurgery:doesitaffectpatientcomfort? Rhinology.2009;47:36---40.
7.AryaAK,ButtO,NigamA.Double-blindrandomisedcontrolled trialcomparingMerocelwithRapidRhinonasalpacksafter rou-tinenasalsurgery.Rhinology.2003;41:241---3.
8.WormaldPJ,BoustredRN,LeT,HawkeL,SacksR.Aprospective single-blindrandomizedcontrolledstudyofuseofhyaluronic acidnasalpacksinpatientsafterendoscopicsinussurgery.Am JRhinol.2006;20:7---10.
9.Bugten V, Nordgard S, Skogvoll E, Steinsvag S. Effects of nonabsorbablepackingin middlemeatusaftersinus surgery. Laryngoscope.2006;116:83---8.
10.KastlKG,ReichertM,ScheithauerMO,SommerF,KisserU,Braun T,etal.PatientcomfortfollowingFESSandNasopore® pack-ing,adoubleblind,prospective,randomizedtrail.Rhinology. 2014;52:60---5.
11.FokkensWJ,LundVJ, MullolJ, BachertC,AlobidI,Barrody F,etal.EPOS2012:Europeanpositionpaperonrhinosinusitis andnasalpolyps2012.Asummaryforotorhinolaryngologists. Rhinology.2012;50:1---12.
12.LundVJ,KennedyDW.Stagingforrhinosinusitis.Otolaryngology HeadNeckSurg.1997;117:S35---40.
13.WawrzyniakK,BurdukPK,CywinskiJB,KuszaK,Kazmierczak W.Improved qualityofsurgicalfieldduringendoscopic sinus surgeryafterclonidinepremedication---apilotstudy.IntForum AllergyRhinol.2014;4:542---7.
14.Kastl KG, Betz CS, Siedek V, Leunig A. Control of bleeding following functional endoscopic sinus surgery using car-boxymethylatedcellulosepacking.EurArchOtorhinolaryngol. 2009;266:1239---43.
15.MoJ, Han DH,Shin H, Cha W, Chang MY,Jin HR. No pack-ing versus packing after endoscopic sinus surgery: pursuit of patients’ comfort after surgery. Am J Rhinol. 2008;22: 525---8.
16.MoreY,WillenS,CatalanoP.Managementofearlynasal polypo-sisusingasteroid-impregnatednasaldressing.IntForumAllergy Rhinol.2011;1:401---4.