w w w . r b o . o r g . b r
Original
Article
Importance
of
radiological
studies
by
means
of
computed
tomography
for
managing
fractures
of
the
tibial
plateau
夽
,
夽夽
Clécio
de
Lima
Lopes
a,∗,
Carlos
Antônio
da
Rocha
Cândido
Filho
b,
Thiago
Almeida
de
Lima
e
Silva
c,
Marcelo
Carvalho
Krause
Gonc¸alves
a,
Ricardo
Lyra
de
Oliveira
c,
Paulo
Rogério
Gomes
de
Lima
caInstitutoRomeuKrauseofTraumatologyandOrthopedics,Recife,PE,Brazil bKneeTreatmentCenter,Recife,PE,Brazil
cHospitalOtáviodeFreitas,Recife,PE,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30November2013 Accepted6January2014 Availableonline30October2014
Keywords:
Tibialfractures/classification Tibialfractures/radiography Computedtomography Operativesurgicalprocedures
a
b
s
t
r
a
c
t
Objectives: To evaluate the concordance among knee surgery specialists regarding the classification andsurgicaltechniqueindicated incasesoftibial plateaufracture, using conventionalradiographsandcomputedtomography.
Methods:Forty-fourpatientswithfracturesofthetibialplateaushownonradiographicand tomographicimageswereselected.Thesewereevaluatedbyspecialistsattwodifferent times,withanintervalofsevendays.Onthefirstoccasion,thespecialistsonlyhadaccess totheradiographs,whileonthesecondoccasiontheyhadaccesstobothradiographsand computedtomographyimages.Theirconcordancewasevaluatedbymeansofthekappa coefficient.
Results:TheinterobserverreliabilityoftheSchatzkerclassificationonthefirstoccasionwas 0.36andonthesecondoccasion,0.35.Thiswasconsideredtopresentlowreproducibility. Inevaluatingtheintra-observerreproducibilityofthisclassification,themeankappaindex was0.42,whichwasclassifiedasmoderate.Fromevaluatingthechoiceofsurgicalaccess, theinter-observerreliabilitywas0.55onthefirstoccasionand0.50onthesecond,whichwas consideredtopresentmoderatereproducibility.Evaluationontheimplantchosenshowed thattheinterobserverreliabilitywas0.01onthefirstoccasionand−0.06onthesecond, whichwasconsideredtobepooranddiscordant.Inevaluating theclassificationofthe threecolumns,theinter-observerreproducibilitywas0.47(p<0.0001),whichwasclassified asmoderateconcordance.
夽
Pleasecitethisarticleas:deLimaLopesC,daRochaCândidoFilhoCA,deLimaeSilvaTA,Gonc¸alvesMCK,deOliveiraRL,deLima PRG.Importânciadoestudoradiológicopormeiodetomografiacomputadorizadanomanejodasfraturasdoplatôtibial.RevBrasOrtop. 2014;49:593–601.
夽夽
WorkdevelopedattheOrthopedicsandTraumatologyService,HospitalOtáviodeFreitas,Recife,PE,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](C.deLimaLopes). http://dx.doi.org/10.1016/j.rboe.2014.10.010
Palavras-chave:
Fraturasdatíbia/classificac¸ão Fraturasdatíbia/radiografia Tomografiacomputadorizada Procedimentoscirúrgicos operatórios
Avaliaraconcordânciaentreespecialistasemcirurgiadejoelhocomrelac¸ãoàclassificac¸ão eàtécnicacirúrgicaindicadanasfraturasdoplatôtibialcomousodasradiografias conven-cionaisedatomografiacomputadorizada.
Métodos: Foramselecionados44pacientescomfraturasdeplatôtibialcomsuasimagens radiográficasetomográficas,asquaisforamavaliadasporespecialistasemdois momen-tosdistintos,comintervalodesetedias.Noprimeiromomentoosespecialistastiveram acesso apenasàsradiografiasenosegundoàsradiografiaseàsimagensdetomografia computadorizada.Aconcordânciafoiavaliadapormeiodocoeficientekappa.
Resultados: Aconfiabilidadeinterobservadorparaaclassificac¸ãodeSchatzkernoprimeiro momentofoi0,36enosegundo0,35,consideradasdebaixareprodutibilidade.Naavaliac¸ão dareprodutibilidadeintraobservadordessaclassificac¸ão,amédiadoíndicefoide0,42, classificadacomomoderada.Aavaliac¸ãodaescolhadoacessocirúrgicoteveuma confiabil-idadeinterobservador de0,55numprimeiromomentoe0,50nosegundo,consideradas de reprodutibilidademoderada.Quando avaliadooimplanteescolhido,a confiabilidade interobservadorfoide0,01noprimeiromomentoe-0,06nosegundo,consideradasruim ediscordante.Naavaliac¸ãodaclassificac¸ãodastrêscolunas,areprodutibilidade interob-servadorfoide0,47(p<0,0001),classificadacomoconcordânciamoderada.
Conclusão: Ousodatomografiacomputadorizadanãoapresentoumelhoriana concordân-ciainterobservadornaclassificac¸ãodeSchatzker,bemcomonãopromoveumudanc¸ano planejamentopré-operatório.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Fracturesofthetibialplateaupresentriskstoknee function-ing,sincethesearejointfracturesoftheproximalthirdofthe tibiawhereloadtransmissiontakesplace.Theyresultfrom axialcompressiveforcesthatmayormaynotbecombined withvarus orvalgusstress onthe knee joint.1 These frac-turesaccountforaround1.3%ofallfracturesandaremore common amongmale patients. This typeof injurymainly affectsyoungormiddle-agedpatientswho aresubjectedto high-energytrauma,andelderlypeoplewhoareexposedto low-energytrauma.2Thetreatmentforthesefracturesaims toachieveanatomicalreductionofthejointsurfaceand sta-bleosteosynthesis inordertoenableearlymobilization,so astopreventcomplicationssuchasjointstiffnessand post-traumaticarthrosis.3
Forthesefractures,preoperativeplanningisfundamental. The clinical history, trauma mechanism, age and associ-atedcomorbiditiesinfluencethetreatmentdecisions.Inthe physicalexamination,thesoft-tissueenvelope,neurovascular functioningandassociatedlesionsshouldbeassessedsothat theinterventionwillbeappropriate.4
Radiographicevaluationonthesefracturesinvolves four views: anteroposterior, lateral, internal oblique and exter-nal oblique (Fig. 1). Computed tomography (CT)is ofgreat valuefordeterminingthelocationandmagnitudeofthejoint depression.1
Managementofthesefracturesconsistsofusing compre-hensiveclassificationsystemsthatareeasilyreproducibleand haveprognosticvalue,therebymakingitconceptuallyeasier todefinetacticsandsurgicalaccesses.
Fig.1–Radiographicviewsfordiagnosingtibialplateaufractures:(A)anteroposterior;(B)lateral;(C)internaloblique;(D) externaloblique.1
Schatzker
Type I Fracture with lateral shearing
Type II Shearing + lateral joint depression
Type III Pure joint depression
Type IV Fracture of the medial plateau
Type V Bicondylar fracture
Type VI Bicondylar fracture extending to metaphysis
Fig.2–Schatzker’sclassification.1
medialandlateral(Fig.1).Inadditiontousingtheaxialview, theaccuracyoftheclassificationwasobtainedwiththeaidof theAPviewwith3Dreconstruction.
According to this classification, an independent joint depressionwithacorticalfractureofthecolumnisdefined asafractureofthecorrespondingcolumn.Purejoint depres-sion(SchatzkerIII)isdefinedasazero-columnfracture.The majorityoffracturesduetosimpleslateralshearingor depres-sion/shearing(SchatzkerIandII)arefracturesofonecolumn (lateralcolumn).However,whenthereisananterolateral frac-ture and a separate posterolateral joint depression with a fractureoftheposteriorcorticalbone,itisdefinedasa frac-tureoftwocolumns(lateralandposteriorcolumns).Ajoint depression in the posterior column witha fracture of the posterior corticalbone isalsodefined asa fracture ofone
Medial column Lateral column
A
O
C
B D
Posterior column
Fig.3–Three-columnclassificationproposedbyLuoetal.5: illustrationofdivisionofthetibialplateauintothree
column (posterior column), which is not included in Schatzker’sclassification.Theothertypicaltwo-column frac-tureisanteromedialwithanisolatedposteromedialfragment (fractureoftheposteriorandmedialcolumns),which tradi-tionallywasinSchatzker’stypeIV(medialcondylarfracture). Three-columnfractures are defined ashaving atleast one independentjointfragmentineachcolumn.Thecommonest three-column fracture is the traditional bicondylar type (SchatzkertypesV andVI),combinedwithanisolated pos-terolateraljointfragment.
Theobjectiveofthepresentstudywastoassessthe impor-tanceofCTformanagingfracturesofthetibialplateauand compare the classification, surgical approach and type of implantused.
Materials
and
methods
Forty-four patients with tibial plateau fractures attended between April and August 2012 were selected in a non-probabilistic consecutive manner. They all came from the orthopedicsandtraumatologyserviceofastatetrauma refer-ralhospital.Theirradiologicalexaminations(CTandsimple radiographs) were analyzed by 10 orthopedists who were membersoftheBrazilianSocietyofOrthopedicsand Trauma-tologywithexperienceofkneesurgery.Thesespecialistswere blindedandworkedindependently.
Theequipmentusedtoconductthecomplementary exam-inationson thecaseswere theSiemens VMIcompactplus 500machineandtheVisionLineLX2processorforthe sim-pleradiographsandtheGE16-channelmultislicetomograph fortheCTscans.
Photographicimageswereobtainedusingacamerawitha resolutionof5.0megapixels(iPhone4smartphone),copied into digital media (.jpg format) and displayed for each observerseparatelybymeansofaPowerPointpresentationin Office2007,onatablet(iPad2)withhigh-resolutionimages (1024×768).
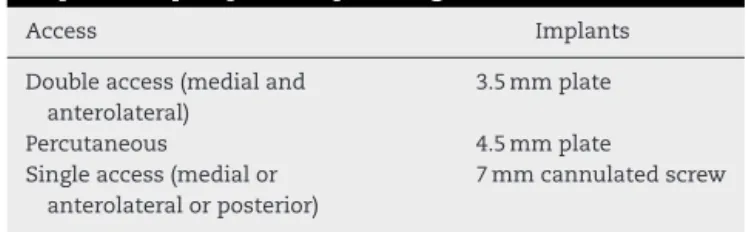
Allthespecialistshadaccesstothesameimages,without identificationofthepatients. Theseimageswereevaluated intwostages:time1andtime2,withaseven-dayinterval betweentheevaluations.Attime1,radiographicimagesof theaffectedkneeweredisplayedinanteroposterior,lateral, internaloblique andexternaloblique views.Thespecialists answeredaquestionnaireregardingtheSchatzker classifica-tionandthechoiceofaccessrouteandimplanttobeused (Table1).Attime2,inadditiontotheradiographs,CTscans wereshown.Thequestionnairewasappliedagain,withthe additionoftheclassificationofthecolumns.Attime2,the
Thedatagatheredwereprocessedinadatabasethatwas cre-atedusingtheSPSS19.0softwareforWindows,inwhichthe universalvariablesandthevariablesanalyzedwereincluded. Afterthisstage,thedatawereanalyzedusingthecoefficient. The coefficient evaluated the concordance between observersbymeansofpairedanalysis,inwhichtheproportion ofconcordancebetweentheobserverswascompared,taking intoaccountthepercentageconcordanceduetochance.The valuesrangedfrom −1(absolutediscordanceto+1(perfect concordance).5–7
This project was approved by our institution’s research ethics committee, inaccordance with Resolution 196/96of theNationalHealthCouncil(GuidelinesandRegulatoryRules forResearchInvolvingHumanBeings).Informationaboutthe studywasgiventoeachpatient,andeachpatientwasaskedto signfreeandinformedconsentstatement.Ifthepatientwas consideredtobeincapableofsigningtheform,acloserelative wasaskedtodoso.
Results
Duringthestudyperiod,44patientswereincluded:28males (64.0%)and16females(36.0%).Theirmeanagewas45.6±16.7 years,withaminimumof21andamaximumof77.However, sincetherewasgreatvariationofages,wenotedthatthemode wasinthefifthdecadeoflife.
At evaluation time 1, the interobserver reliability of Schatzker’sclassificationwas0.36,whichwasclassifiedaslow. Inevaluatingthechoiceofsurgicalaccess,theinterobserver reliability was0.55,which was moderatelyreproducible.In evaluatingthechoiceofimplantstobeused,theinterobserver reliabilitywas0.01,whichwasclassifiedaspoor(Table2).
Atevaluationtime2,theinterobserverreliabilityrelatingto Schatzker’sclassificationwas0.35,whichwasclassifiedaslow. Inevaluatingthesurgicalaccess,theinterobserverreliability was0.50,whichwasmoderatelyreproducible.Inevaluating thechoiceofimplants,theinterobserverreliabilitywas−0.06, whichwasclassifiedasdiscordant(Table3).
Therewasnostatisticallysignificantdifferenceinrelation tothemeansforinterobserverreproducibilityattimes1and2 oftheevaluationofSchatzker’sclassification(p=0.658)(Fig.4). Themeaninterobserverconcordanceattime1regarding the choiceofimplant was0.05(poor)and attime2,it was
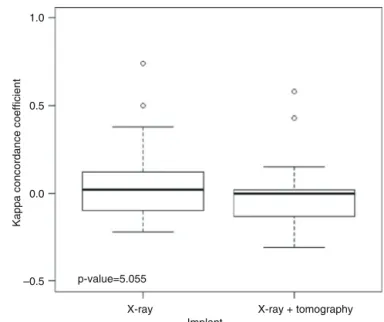
−0.03 (discordant). There was no difference in the means regardingthechoiceofimplant,inrelationtotheevaluation times(p=0.055)(Fig.5).
Table4andFig.6showthedegreeofintraobserver
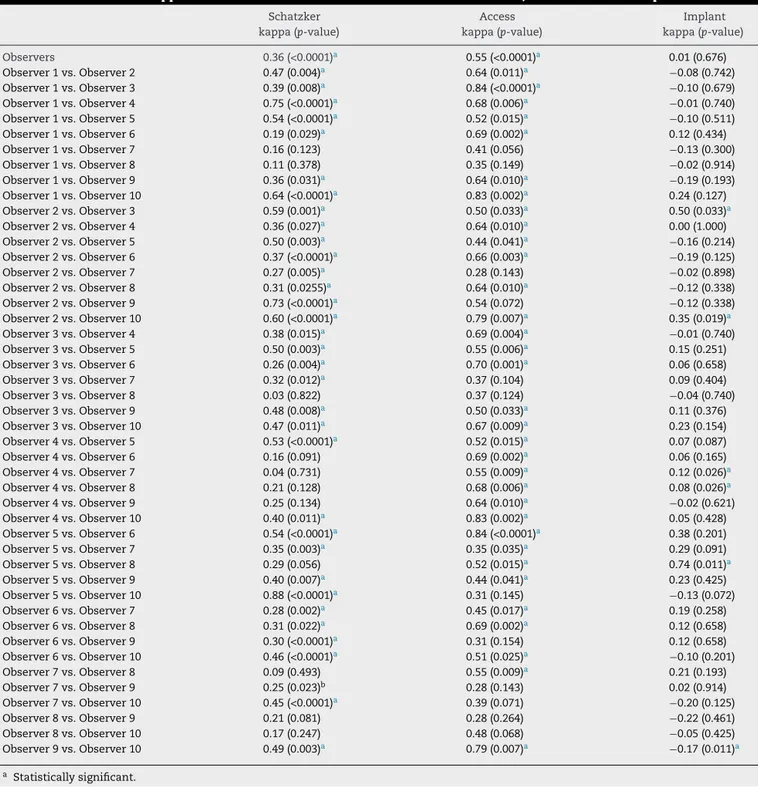
Table2–Interobserverkappaindexattime1inrelationtoSchatzker’sclassification,accessrouteandimplant.
Schatzker Access Implant
kappa(p-value) kappa(p-value) kappa(p-value)
Observers 0.36(<0.0001)a 0.55(<0.0001)a 0.01(0.676)
Observer1vs.Observer2 0.47(0.004)a 0.64(0.011)a −0.08(0.742) Observer1vs.Observer3 0.39(0.008)a 0.84(<0.0001)a −0.10(0.679) Observer1vs.Observer4 0.75(<0.0001)a 0.68(0.006)a −0.01(0.740) Observer1vs.Observer5 0.54(<0.0001)a 0.52(0.015)a −0.10(0.511) Observer1vs.Observer6 0.19(0.029)a 0.69(0.002)a 0.12(0.434) Observer1vs.Observer7 0.16(0.123) 0.41(0.056) −0.13(0.300) Observer1vs.Observer8 0.11(0.378) 0.35(0.149) −0.02(0.914) Observer1vs.Observer9 0.36(0.031)a 0.64(0.010)a −0.19(0.193) Observer1vs.Observer10 0.64(<0.0001)a 0.83(0.002)a 0.24(0.127) Observer2vs.Observer3 0.59(0.001)a 0.50(0.033)a 0.50(0.033)a Observer2vs.Observer4 0.36(0.027)a 0.64(0.010)a 0.00(1.000) Observer2vs.Observer5 0.50(0.003)a 0.44(0.041)a −0.16(0.214) Observer2vs.Observer6 0.37(<0.0001)a 0.66(0.003)a −0.19(0.125) Observer2vs.Observer7 0.27(0.005)a 0.28(0.143) −0.02(0.898) Observer2vs.Observer8 0.31(0.0255)a 0.64(0.010)a −0.12(0.338) Observer2vs.Observer9 0.73(<0.0001)a 0.54(0.072) −0.12(0.338) Observer2vs.Observer10 0.60(<0.0001)a 0.79(0.007)a 0.35(0.019)a Observer3vs.Observer4 0.38(0.015)a 0.69(0.004)a −0.01(0.740) Observer3vs.Observer5 0.50(0.003)a 0.55(0.006)a 0.15(0.251) Observer3vs.Observer6 0.26(0.004)a 0.70(0.001)a 0.06(0.658) Observer3vs.Observer7 0.32(0.012)a 0.37(0.104) 0.09(0.404) Observer3vs.Observer8 0.03(0.822) 0.37(0.124) −0.04(0.740) Observer3vs.Observer9 0.48(0.008)a 0.50(0.033)a 0.11(0.376) Observer3vs.Observer10 0.47(0.011)a 0.67(0.009)a 0.23(0.154) Observer4vs.Observer5 0.53(<0.0001)a 0.52(0.015)a 0.07(0.087) Observer4vs.Observer6 0.16(0.091) 0.69(0.002)a 0.06(0.165) Observer4vs.Observer7 0.04(0.731) 0.55(0.009)a 0.12(0.026)a Observer4vs.Observer8 0.21(0.128) 0.68(0.006)a 0.08(0.026)a Observer4vs.Observer9 0.25(0.134) 0.64(0.010)a −0.02(0.621) Observer4vs.Observer10 0.40(0.011)a 0.83(0.002)a 0.05(0.428) Observer5vs.Observer6 0.54(<0.0001)a 0.84(<0.0001)a 0.38(0.201) Observer5vs.Observer7 0.35(0.003)a 0.35(0.035)a 0.29(0.091) Observer5vs.Observer8 0.29(0.056) 0.52(0.015)a 0.74(0.011)a Observer5vs.Observer9 0.40(0.007)a 0.44(0.041)a 0.23(0.425) Observer5vs.Observer10 0.88(<0.0001)a 0.31(0.145) −0.13(0.072) Observer6vs.Observer7 0.28(0.002)a 0.45(0.017)a 0.19(0.258) Observer6vs.Observer8 0.31(0.022)a 0.69(0.002)a 0.12(0.658) Observer6vs.Observer9 0.30(<0.0001)a 0.31(0.154) 0.12(0.658) Observer6vs.Observer10 0.46(<0.0001)a 0.51(0.025)a −0.10(0.201) Observer7vs.Observer8 0.09(0.493) 0.55(0.009)a 0.21(0.193) Observer7vs.Observer9 0.25(0.023)b 0.28(0.143) 0.02(0.914) Observer7vs.Observer10 0.45(<0.0001)a 0.39(0.071) −0.20(0.125) Observer8vs.Observer9 0.21(0.081) 0.28(0.264) −0.22(0.461) Observer8vs.Observer10 0.17(0.247) 0.48(0.068) −0.05(0.425) Observer9vs.Observer10 0.49(0.003)a 0.79(0.007)a −0.17(0.011)a
a Statisticallysignificant.
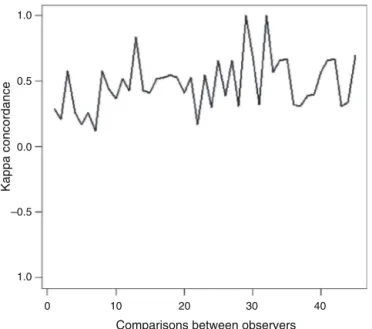
In evaluating the three-column classification, the inter-observer reproducibility was 0.47 (p<0.0001), which was classifiedasmoderate(Table5andFig.7).
ThemeanSchatzkerconcordancewas0.36(low)andthe three-columnconcordancewas0.48(moderate).Themean concordancewasgreater inthethree-column classification thanintheSchatzkerclassificationattime2(p=0.003)(Fig.8).
Discussion
ControversyregardingroutineuseofCTscansandtheideal classificationmethodfortibialplateaufracturescontinuesin
the literature.Thisaroused ourinterest inconducting this study.
The Brazilian National Health System (SUS) provides healthcare fora largepercentage ofthis country’s popula-tion.High-complexityexaminationssuchasCTandmagnetic resonancearenotroutinelyavailableatsomeservices.Their highcost,alongwithaccessdifficulties,thusplacesvalueon conductingstudiesontheuseoftheseexaminations.
Observer1vs.Observer9 0.49(<0.0001)a 0.49(0.058) −0.14(0.462) Observer1vs.Observer10 0.22(0.192) 0.61(0.044)a −0.21(0.132) Observer2vs.Observer3 0.40(0.004)a 0.21(0.477) −0.24(0.111) Observer2vs.Observer4 0.48(0.006)a 0.49(0.058) −0.01(0.740) Observer2vs.Observer5 0.71(<0.0001)a 0.50(0.049)a 0.00(0.740) Observer2vs.Observer6 0.19(0.017)a 0.53(0.019)a 0.02(0.621) Observer2vs.Observer7 0.27(0.046)a 0.38(0.201) 0.05(0.251) Observer2vs.Observer8 0.43(<0.0001)a 0.49(0.058) 0.00(1.000) Observer2vs.Observer9 0.61(<0.0001)a 0.49(0.058) −0.18(0.120) Observer2vs.Observer10 0.60(0.001)a 0.61(0.044)a 0.58(0.002)a Observer3vs.Observer4 0.42(0.003)a 0.49(0.058) −0.04(0.338) Observer3vs.Observer5 0.52(<0.00001)a 0.50(0.049)a −0.08(0.251) Observer3vs.Observer6 0.27(0.016)a 0.37(0.099) −0.01(0.887) Observer3vs.Observer7 0.38(0.011)a 0.38(0.201) −0.03(0.740) Observer3vs.Observer8 0.44(0.001)a 0.49(0.058) 0.00(1.000) Observer3vs.Observer9 0.66(<0.0001)a 0.49(0.058) 0.43(0.033)a Observer3vs.Observer10 0.52(<0.0001)a 0.21(0.477) −0.15(0.266) Observer4vs.Observer5 0.49(0.005)a 0.67(0.008)a 0.09(0.064) Observer4vs.Observer6 0.26(0.022)a 0.55(0.011)a −0.12(0.073) Observer4vs.Observer7 0.28(0.043)a 0.35(0.125) −0.13(0.441) Observer4vs.Observer8 0.32(0.019)a 1.00(<0.0001)a 0.00(1.000) Observer4vs.Observer9 0.29(0.057) 1.00(<0.0001)a 0.13(0.137) Observer4vs.Observer10 0.50(0.003)a 0.49(0.058) −0.06(0.402) Observer5vs.Observer6 0.27(0.005)a 0.41(0.074) −0.14(0.621) Observer5vs.Observer7 0.36(0.009)a 0.33(0.156) −0.08(0.251) Observer5vs.Observer8 0.29(0.049)a 0.67(0.008)a 0.00(1.000) Observer5vs.Observer9 0.63(<0.0001)a 0.67(0.008)a −0.08(0.165) Observer5vs.Observer10 0.59(0.002)a 0.67(0.008)a 0.01(0.740) Observer6vs.Observer7 0.39(<0.0001)a 0.20(0.338) 0.13(0.154) Observer6vs.Observer8 0.09(0.480)a 0.55(0.011)a 0.00(1.000) Observer6vs.Observer9 0.27(0.015)a 0.55(0.011)a −0.17(0.038)a Observer6vs.Observer10 0.36(0.001)a 0.53(0.019)a 0.02(0.621) Observer7vs.Observer8 0.10(0.371) 0.35(0.125) 0.00(1.000) Observer7vs.Observer9 0.31(0.020)a 0.35(0.125) −0.24(0.106) Observer7vs.Observer10 0.37(0.006)a −0.04(0.898) 0.15(0.087) Observer8vs.Observer9 0.33(0.015)a 1.00(<0.0001)a 0.00(1.000) Observer8vs.Observer10 0.40(0.013)a 0.49(0.058) 0.00(1.000) Observer9vs.Observer10 0.28(0.077) 0.49(0.058) −0.18(0.183)
a Statisticallysignificant.
Intheresultsfromourstudy,Schatzker’sclassification pre-sentedalowrateofgeneralinterobserverreproducibility,both attime1,whenonlyradiographswereanalyzed,andattime2, whenradiographsandCTscanswereanalyzed.Inevaluating theintraobserverreproducibility,theresultfoundcomprised moderatemeanconcordance.
In a study involving 50 cases of tibial plateau fracture, Charalambous et al.9 observed that Schatzker’s classifi-cation presented highly variable intra- and interobserver reproducibility. They concluded that these results should be taken into consideration, so that surgeons would use this classification for guiding treatments and determining prognoses.
Waltonetal.10comparedtheSchatzkerandAOGroup clas-sificationsandconcludedthattheAOwasmorereproducible. Theyalsoobservedthatthetwoclassificationswereoriginally basedonradiographicstudies.Thisfactormayhaveinterfered withtheresultsfromourstudy,giventhatwealsousedCT images.
AccordingtoBrunneretal.,11Schatzker’sclassification pre-sented good intra- and interobserver reproducibility when performedwiththeaidofCT.
1.0
0.5
0.0
–0.5
X-ray X-ray + tomography
Schatzker
Kappa concordance coefficient
Fig.4–Boxplotofinterobserverreproducibilityof Schatzker’sclassificationinrelationtothetwoevaluation times.
The studies in the literature on the concordance and reproducibilityofSchatzker’sclassificationstillpresentvery divergentresultsbut,asalsoobservedinourstudy,mostof themhavecharacterizedthisclassificationsystemashaving poortomoderatereproducibility.9,13–15
In some studies, CT has not changed the reproducibil-ity of Schatzker’s classification in relation to conventional radiographs,14 as also shown in our results. In other studies, this examination has become important for this evaluation.11,12
Martijn et al.13 evaluated the impact of CT on inter and intraobserver concordance, in comparison with plain radiographs,foroperativeplanningandforSchatzker’s classi-ficationoftibialplateaufractures.Theyconcludedthatusing CT in addition to plain radiographs did not improve the
p-value=5.055 –0.5
0.0 0.5 1.0
X-ray X-ray + tomography Implant
Kappa concordance coefficient
Fig.5–Boxplotoftheinterobserverkappaconcordance relatingtochoiceofimplant.
Table4–Interobserverkappaindexatbothtimesin
relationtoSchatzker’sclassification,accessrouteand
implant.
Time1vs. Time2
Schatzker Access Implant
kappa(p-value) kappa(p-value) kappa(p-value)
Observer1 0.35(0.044)a 0.36(0.128) 0.36(0.128) Observer2 0.85(<0.0001)a 0.35(0.125) −0.04(0.707) Observer3 0.39(0.012)a 0.50(0.049)a 0.67(0.011)a Observer4 0.28(0.075) 0.83(0.002)a 0.15(0.464) Observer5 0.49(0.005)a 0.26(0.202) −0.16(0.521) Observer6 0.28(0.043)a 0.44(0.037)a 0.12(0.658) Observer7 0.28(0.071) 0.02(0.944) 0.11(0.573) Observer8 0.31(0.037)a 0.48(0.067) 0.00(1.000) Observer9 0.38(0.017)a 0.79(0.007)a −0.04(0.658) Observer10 0.62(<0.0001)a 0.49(0.058) −0.10(0.512)
a Statisticallysignificant.
Table5–Interobserverreproducibilityinrelationtothree-columnclassification.
Observers kappa(p-value) Observers kappa(p-value) Observers kappa(p-value)
1×2 0.29(0.118) 2×9 0.52(0.022)a 5×6 0.32(0.131)
1×3 0.21(0.249) 2×10 0.53(0.011)a 5×7 1.00(<0.0001)a 1×4 0.58(0.003)a 3×4 0.55(0.011)a 5×8 0.57(0.023)a 1×5 0.26(0.145) 3×5 0.53(0.009)a 5×9 0.66(0.002)a 1×6 0.17(0.394) 3×6 0.41(0.064) 5×10 0.67(0.001)a 1×7 0.26(0.145) 3×7 0.53(0.009)a 6×7 0.32(0.131) 1×8 0.12(0.460) 3×8 0.17(0.478) 6×8 0.31(0.154) 1×9 0.58(0.003)a 3×9 0.55(0.011)a 6×9 0.39(0.079) 1×10 0.44(0.028)a 3×10 0.30(0.129) 6×10 0.40(0.064) 2×3 0.37(0.104) 4×5 0.66(0.002)a 7×8 0.57(0.023)a 2×4 0.52(0.022)a 4×6 0.39(0.079) 7×9 0.66(0.001)a 2×5 0.43(0.064) 4×7 0.66(0.002)a 7×10 0.67(0.001)a 2×6 0.84(<0.0001)a 4×8 0.31(0.154) 8×9 0.31(0.154) 2×7 0.43(0.064) 4×9 1.00(<0.0001)a 8×10 0.34(0.066) 2×8 0.41(0.108) 4×10 0.70(0.001)a 9×10 0.70(0.001)a
Observers
2 4 6 8 10
–1.0 –0.5
Concordance coefficient
Schatzker
Access management Implant management
Fig.6–Interobserverconcordancecoefficientrelatingto Schatzker’sclassificationandthechoiceofaccessrouteand implant.
intra-andinterobserverreproducibilityofSchatzker’s classi-fication,andthatitsroutineapplicationwasquestionable.
IncontrasttoWickyetal.16andMarkhardtetal.,17whose studies confirmed that CT showed tibial plateau fractures moreaccuratelyandenabledgreaterprecisionofpreoperative planning,therewasnostatisticallysignificantchangein rela-tiontooperativeplanninginthepresentstudyafterviewing theCT.
Luo etal.5 proposed using athree-column classification fortibialplateaufracturesthatencompassedlesionpatterns thatwouldbedifficulttoclassifywiththemethodscurrently used.Fractures withposteriorfragmentsare notenvisaged inSchatzker’sclassification,whichmay makeit difficultto
1.0
0.5
0.0
–0.5
1.0
10 20 30 40
0
Comparisons between observers
Kappa concordance
Fig.7–Interobserverkappaconcordanceofthe three-columnclassification.
–0.5 p-value=0.003
Kappa concordance coefficient
Schatzker Three columns
Fig.8–Boxplotofinterobserverkappaconcordanceofthe Schatzkerandthree-columnclassifications.
diagnosethemandplanoperations.Inouranalysis,wefound that there was moderate interobserver concordancein the three-columnclassification.Thisclassificationmaybea use-fuloptioninmanagingtibialplateaufractures.
BecauseCTisunavailableinsomeservicesandbecauseof thehighcostofthisexaminationandthehighexposureto radiationthatisinvolved,thereisaneedfornewstudiesto clarifytherealvalueofCTinclassifyingandmanagingtibial plateaufractures.
Studieswithlargersamplesandbroaderapproachesneed tobedevelopedsothatroutineuseofCTandthepresent clas-sificationsystemsformanagingtibialplateaufracturescanbe judgedmoremeaningfully.
Conclusion
UseofCTdidnotgiverisetogreaterconcordancebetween theevaluatorsregardingSchatzker’sclassification.Nordidit contributetowardschangesinpreoperativeplanningin com-parisonwithradiographs.
Thethree-columnclassificationpresentedmoderate inter-observer concordance and might be a useful option in approachestowardstibialplateaufractures.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.KfuriJúniorM,FogagnoloF,BitarRC,FreitasRL,SalimRO,
PaccolaCAJ.Fraturasdoplanaltotibial–Artigode
atualizac¸ão.RevBrasOrtop.2009;44(6):468–74.
2.ThomasCH,AthanasiovA,WullschlegerM,SchuetzM.
Currentconceptsintibialplateaufractures.ActaChirOrthop
3. TscherneH,LobenhofferP.Tibialplateaufractures.
Managementandexpectedresults.ClinOrthopRelatRes.
1993;(292):87–100.
4. MustonenAO,KoskinenSK,KiuruMJ.Acutekneetrauma:
analysisofmultidetectorcomputedtomographyfindingsand
comparisonwithconventionalradiography.ActaRadiol.
2005;46(8):866–74.
5. LuoCF,SunH,ZhangB,ZengBF.Three-columnfixationfor
complextibialplateaufractures.JOrthopTrauma.
2010;24(11):683–92.
6. CohenJ.Acoefficientofagreementfornominalscales.Ed
PsycholMeas.1960;20:37–46.
7. CongerAJ.IntegrationandgeneralisationofKappasfor
multipleraters.PsycholBull.1980;88:322–8.
8. AlbuquerqueRP,GiordanoV,PallotinoA.Análiseda
reprodutibilidadedasclassificac¸õesdasfraturasdoplatô
tibial.RevBrasOrtop.2009;44(3):225–9.
9. CharalambousCP,TryfonidisM,AlviF,MoranM,FangC,
SamarajiR,etal.Inter-andintra-observervariationofthe
SchatzkerandAO/OTAclassificationsoftibialplateau
fracturesandaproposalofanewclassificationsystem.AnnR
CollSurgEngl.2007;89(4):400–4.
10.WaltonNP,HarishS,RobertsC,BlundellC.AOorSchatzker?
Howreliableisclassificationoftibialplateaufractures?Arch
OrthopTraumaSurg.2003;123(8):396–8.
11.BrunnerA,HorisbergerM,UlmarB,HoffmannA,BabstR.
Classificationsystemsfortibialplateaufractures;does
computedtomographyscanningimprovetheirreliability?
Injury.2010;41(2):173–8.
12.RafiiM,LamontJG,FiroozniaH.Tibialplateaufractures:CT
evaluationandclassification.CritRevDiagnImaging.
1987;27(2):91–112.
13.MartijnAJ,HollaM,BiertJ,KampenA.ThevalueofaCTscan
comparedtoplainradiographsfortheclassificationand
treatmentplanintibialplateaufractures.EmergRadiol.
2011;18:279–83.
14.MaripuriSN,RaoP,Manoj-ThomasA,MohantyK.The
classificationssystemsfortibialplateaufractures:how
reliablearethey?Injury.2008;39(10):1216–21.
15.MandarinoM,PessoaA,GuimarãesJA.Avaliac¸ãoda
reprodutibilidadedaclassificac¸ãodeSchatzkerparaas
fraturasdoplanaltotibial.RevInto.2004;2(2):11–8.
16.WickyS,BlaserPF,BlancCH,LeyvrazPF,SchnyderP,MeuliRA.
ComparisonbetweenstandardradiographyandspiralCT
with3Dreconstructionintheevaluation,classificationand
managementoftibialplateaufractures.EurRadiol.
2000;10(8):1227–32.
17.MarkhardtBK,GrossJM,MonuJU.Schatzkerclassificationof
tibialplateaufractures:useofCTandMRimagingimproves