w w w . r b o . o r g . b r
Original
article
Infected
primary
knee
arthroplasty:
Risk
factors
for
surgical
treatment
failure
夽
João
Gabriel
Duarte
Paes
Pradella
a,
Miguel
Bovo
a,
Mauro
José
Costa
Salles
b,
Giselle
Burlamaqui
Klautau
c,
Osmar
Arbix
Pedro
de
Camargo
d,
Ricardo
de
Paula
Leite
Cury
e,∗aResidentPhysicianintheDepartmentofOrthopedicsandTraumatology,SchoolofMedicalSciences,SantaCasadeMisericórdiadeSão
Paulo(DOT-FCMSCP),SãoPaulo,SP,Brazil
bPhDinMedicine;AdjunctProfessorofInfectology,FCMSCP;CoordinatoroftheInfectologyClinic,SantaCasadeSãoPaulo,SãoPaulo,
SP,Brazil
cAssistantProfessorofInfectology,FCMSCP,SãoPaulo,SP,Brazil
dAdjunctProfessor,AcademicConsultantandMemberoftheKneeSurgeryGroup,DOT-FCMSCP,SãoPaulo,SP,Brazil
eLecturerandHeadoftheKneeSurgeryGroup,DOT-FCMSCP,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received13August2012
Accepted3October2012
Keywords:
Kneearthroplasty
Humans
Bacterialinfections/diagnosis
Bacterialinfections/therapy
a
b
s
t
r
a
c
t
Objective:Topresentepidemiologicaldataandriskfactorsassociatedwithsurgical
out-comes favorable or unfavorable for the treatment of infection in infected total knee
arthroplasty.
Methods:We reviewedmedicalrecordsof48 patientswhounderwent treatmentof
pri-marytotalkneearthroplastyforinfectionbetweenJanuary1994andDecember2008,in
theOrthopedicsandTraumatologyDepartmentoftheSantaCasadeMisericórdiadeSão
Paulo.Thevariablesassociatedwithfavorableoutcomeofsurgicaltreatment(debridement
andretentionorexchangearthroplastyintwodays)orunfavorable(arthrodesisordeath)
infection.
Results:Atotalof39casesofinfectionafterprimarytotalkneearthroplasty,22progressed
to17forafavorableoutcomeandunfavorableoutcome.Earlyinfections(OR:14.0,95%CI
1.5–133.2,p=0.016)anddiabetes(OR:11.3,95%CI1.4–89.3,p=0.032)wereassociatedwith
arthrodesisjointanddeathrespectively.
Conclusion:Patientswithearly infectionhada higherriskofdevelopingsurgical
proce-durewithunfavorableoutcome(arthrodesis)anddiabeticshadhigheroddsofdeathafter
infectionofprimarykneearthroplasties.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.Allrightsreserved.
夽
StudyconductedattheDepartmentofOrthopedicsandTraumatology,SchoolofMedicalSciences,SantaCasadeSãoPaulo,
Fernand-inhoSimonsenWing,SãoPaulo,SP,Brazil.Director:Prof.Dr.OsmarAvanzi.
∗ Correspondingauthorat:RuaBarataRibeiro,380,6◦andar,SãoPaulo,SP,Brazil.CEP01308-000.Tel.:+113214-5334.
E-mail:[email protected](R.d.P.L.Cury).
Artroplastia
primária
de
joelho
infectada:
fatores
de
risco
para
falha
na
terapia
cirúrgica
Palavras-chave:
Artroplastiadojoelho
Humanos Infecc¸ões
bacterianas/diagnóstico
Infecc¸õesbacterianas/terapia
r
e
s
u
m
o
Objetivo: Apresentardadosepidemiológicoseosfatoresderiscoassociadosaodesfecho
cirúrgicofavoráveloudesfavorávelparaotratamentodainfecc¸ãonaartroplastiatotalde
joelhoinfectada.
Metódos: Foramrevisados48prontuáriosdepacientessubmetidosaotratamentoda
artro-plastiatotalprimáriadejoelhoporinfecc¸ãoentrejaneirode1994edezembrode2008no
Servic¸odeOrtopediaeTraumatologiadaSantaCasadeMisericórdiadeSãoPaulo.Foram
analisadasasvariáveisassociadasaodesfechodotratamentocirúrgicofavorável
(desbrida-mentoeretenc¸ãodaartroplastiaoutrocaemdoistempos)oudesfavorável(artrodesesou
óbito)dainfecc¸ão.
Resultados: Em39casosdeinfecc¸ãopós-artroplastiatotalprimárianojoelho,22evoluíram
paradesfecho favorável e 17 paradesfecho desfavorável. Infecc¸õesprecoces (RC:14,0,
IC95%1,5–133,2,p=0,016)ediabetes(RC:11,3,IC95%1,4–89,3,p=0,032)foramassociadasa
artrodesedaarticulac¸ãoeaoóbito,respectivamente.
Conclusão: Pacientescominfecc¸ãoprecoceapresentarammaiorriscodeevoluirpara
pro-cedimentocirúrgicocomdesfechonãofavorável(artrodese)eosdiabéticosapresentaram
maiorchancedeóbitoapósinfecc¸ãodeartroplastiasprimáriasnojoelho.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier
EditoraLtda.Todososdireitosreservados.
Introduction
Osteoarthrosis is the most prevalent joint disease among
elderly adults and it occurs because of the joint
car-tilage degeneration process. Knee arthroplasty is a
surgical technique for treating advanced
osteoarthro-sis and is being increasingly used because of its good
results regarding pain relief and reestablishment of
function. Like all surgical procedures, total knee
arthro-plasty (TKA) is subject to complications over the short or
long term, including the following: systemic and
throm-boembolic phenomena; complications that affect the
patellofemoral joint; neurovascular lesions; periprosthetic
fractures; loosening of the implanted components; and
infection.1
Amongallthecomplications,post-arthroplastyinfectionis
oneofthemostsevereandfearedtypesanditsincidencemay
range from 0.5to 23%.2,3 Post-arthroplasty knee infections
haveaneconomicimpactgreaterthan300milliondollarsper
yearinthecountriesofNorthAmerica.4
For treatment of infected TKA to be successful,
early diagnosis is fundamental, with immediate
appli-cation of therapeutic measures. Appropriate physical
examination, imaging examinations, laboratory tests
to investigate inflammatory activity and puncturing of
the affected knee may assist greatly in defining the best
management.4
Regarding the treatmentfor theinfection, several types
of surgical procedure have been described, including the
following: surgical cleaning with retention of the implant;
revision in a one-stage procedure, consisting of removal
of the implant, rigorous surgical cleaning and placement
of a new prosthesis; revision in two stages, in which
implanting the new prosthesis is postponed until a time
that some authors consider to be safer; and salvage
pro-cedures such as arthrodesis and amputation, in cases of
lackofsuccessinpreviousattempts.5 All theseprocedures
should be accompanied by appropriate antibiotic therapy
accordingtothepathogensidentifiedasresponsibleforthe
infection.6
The gold standard for treating cases of infected TKA
whenimplantremovalbecomesnecessaryistwo-stage
revi-sion. In this, intravenous antibiotics are administered for
sixweeksafterdebridement and then fillingthe joint
cav-itywithaspacercomprisingorthopediccementwithadded
antibiotic.7 The aims in applying the spacer are to
main-tain thejoint distances,occupy the emptyspacesbetween
the structuresand release high levels of antibiotic at this
site.8 The second stage is performed taking into
consid-eration the possibility of curing the infection,7 which is
confirmed through clinical reassessment and producing a
hemogramcomprisingaleukocyte countandinflammatory
marker tests such as the erythrocyte sedimentation rate
and C-reactive protein level, and joint puncture in order
to culture the synovial fluid.5 When the results from the
examinationsarewithintherangeofnormalityandthe
cul-turesarenegative,thepatientthenundergoestherevision,
which consistsremoval of the spacer and placement of a
new joint implant that is fixed using cement with added
antibiotic.5,7
Eventhough thisisacatastrophiccomplicationforTKA
patients,withhighcostsforthehealthcaresystem,few
stud-ieshaveevaluatedthefactorsassociatedwithfailureofthe
surgicalmethodsthatareusedforcuringinfectedknee
arthro-plastycases.9
Theaimofthisstudywastomakeadescriptiveanalysis
ofinfectedTKAcasesandthepossibleriskfactorsassociated
withunfavorableoutcomesfollowingsurgicaltherapyforthe
Methodology
Thiswasaretrospectivecase–controlstudyconductedbythe
KneeSurgeryGroupofthe DepartmentofOrthopedicsand
Traumatology,SantaCasadeMisericórdiadeSãoPaulo.The
populationforthisstudyconsistedofalltheindividualswho
underwentprimaryTKAbetweenJanuary1994and
Decem-ber2008,who wereidentified bymeans ofthedatabase of
theinstitution’sKneeGroup.Amongthese,onlythepatients
whopresentedsignsandsymptomsofinfectionsubsequent
toprimaryTKAwereanalyzedthroughreviewingthemedical
records.Thisstudywasapprovedbytheinstitution’sResearch
EthicsCommittee.
Infectionsin revision knee arthroplasty procedures and
infectionsconfirmedbymeansofaswabfromsecretionsfrom
theoperativewoundand/orcasesforwhichinsufficient
infor-mationwasavailableinthemedicalrecordswereexcluded.
Thediagnosticcriteriaforinfectionassociatedwith
arthro-plasty were established in accordance with a previously
published study.10 The microbiological confirmation ofthe
infectionwasdonebymeansofculturingtwoormoretissue
samplesfromtheperiprostheticregion,andfrombonetissue
andidentificationofthepathogeninthesynovialfluid,along
withthehistopathologicaldescription.11
Allthepatientsunderwentarthrotomy,implantremoval,
placementofacementedspacer(PMMA)incorporating
van-comycin,provisionalimmobilizationusingasplintanduse
ofanorthosisor externalfixation, giventhegreat
instabil-ityoftheregion. Thestabilizationmethodwas selectedby
thesame surgeon, accordingtothe stabilitythathad been
acquiredthroughplacementofthespacer.
Amongthe variablesstudied, parametersrelatingtothe
patients were evaluated, such as: sex, age, comorbidities
(obesity, HIV, previous use of corticoids, diabetes mellitus,
arterialhypertension,rheumatoidarthritisandsmoking)and
the diagnosis that indicated the need forTKA. In relation
totheinfection,thefollowingdatawere gathered:thetime
thatelapsedbetweenthesurgeryandthediagnosisof
infec-tion (upto threemonthsafterthe surgery wasconsidered
to be early infection, from three to 24 months was
con-sidered to be intermediate infection and 24 months was
consideredtobelateinfection)12andthebacteriathatwere
isolatedfromthecultures,whichweredifferentiatedbetween
polymicrobialinfection(twoormorepathogensidentifiedin
cultures)and monobacterialinfection.Thesurgicaltherapy
wascharacterizedasrevisionarthroplasty(surgical
debride-mentwithretentionoftheprosthesisandtwo-stagerevision
ofaninfectedprosthesis)orsalvageprocedures(arthrodesis
oramputation).
Statistical
analysis
The descriptive analysis on all the characteristics studied
wasdoneusingpercentagesforthequalitativevariablesand
meansandstandarddeviationsforthequantitativevariables.
Toanalyzetheassociationsbetweentheriskfactorsandthe
successofthesurgicaltherapy,wecharacterizedtheoutcome
variableasfunctionalsurgicaltreatment(F)whenthecurefor
theinfectionwasassociatedwithdebridementandretention
oftheprosthesis,orwithconventionalrevisionarthroplastyor
useofanunconventionalendoprosthesis;orasnonfunctional
surgicaltreatment(NF)whenthecurefortheinfectionwas
associatedwithjointarthrodesisordeathassociatedwiththe
infection.Inaddition,weanalyzedtheriskfactorsassociated
withinfection-relateddeath.Forbivariateanalyses,Fisher’s
exacttestwasused,withthestatisticalsignificancelevelof
p<0.05anda95%confidenceinterval.Alltheanalyseswere
doneusingtheRstatisticalsoftware,version2.15.0.1
Results
Outofthe592patientswhounderwentprimaryTKAinthe
Department ofOrthopedics,Santa Casa de Misericórdiade
SãoPaulo,38(6.42%)evolvedwithinfection.Inaddition,ten
patientswhowereincludedinthesamplecamefromother
medicalinstitutionsandwerereferredfortreatmentatSanta
CasadeMisericórdiadeSãoPaulo.Thus,thetotalsample
eval-uatedinthisstudywas48casesofinfectedTKA.Ninepatients
(18.75%)wereexcludedfromtheanalysisbecauseofdifficulty
inidentifyingthevariablesinthemedicalfiles.
Amongthe39patientsstudied,34(87.18%)werefemaleand
five(12.82%)weremale.Theagerangewasfrom41to89years,
withameanof69.7years(SD±10.0years).Themeanlength
oftimebetweenthesurgeryandthediagnosingofinfection
was70.4weeks(SD±15.3).Therightkneewasaffectedin20
patients(51.28%)andtheleftkneein19(48.72%).
Thediseasethatledtotheindicationofarthroplastywas
primarykneearthrosisin29patients(74.35%)andthecases
ofsecondarykneearthrosiswereconsequent tothe
follow-ing:rheumatoidarthritisintwo(5.12%),asepticosteonecrosis
of the femurdue tocorticoid use in two(5.12%), sequelae
ofsepticarthritisinone(2.56%),synovialchondromatosisin
one(2.56%),ligamentinjuryinone(2.56%)andpost-fracture
sequelaeinthekneeregion(includingthedistalfemurand
proximaltibia,whichaffectthejointarea)inthree(7.68%).
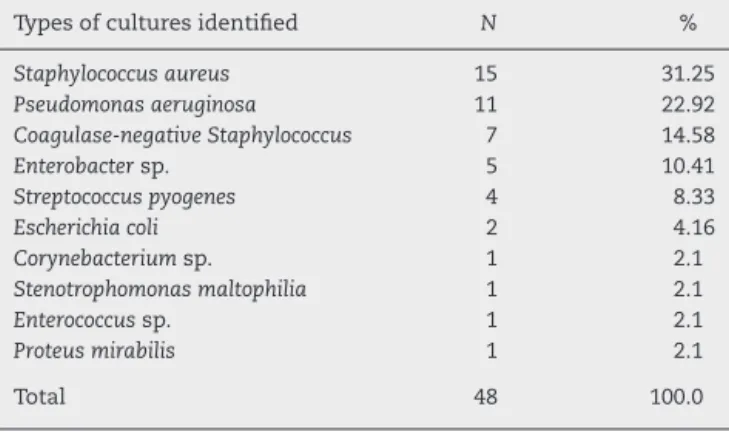
Theinfectiousagentsidentifiedwere:Staphylococcusaureus
(31.2%); Pseudomonas aeruginosa (22.9%), coagulase-negative
Staphylococcus (14.5%), Enterococcus sp (2.1%), Enterobacter
(10.4%),Streptococcuspyogenes(8.3%),Escherichiacoli(4.1%),
Pro-teus mirabilis (2.1%), Stenotrophomonas maltophilia (2.1%) and
Corynebacterium sp (2.1%) (Table 1). Seven infections were
polymicrobial(17.94%)and32weremonomicrobial(82.06%).
Regarding the presence of comorbidities, 31 patients
(79.48%) presentedsystemicarterialhypertensionand nine
(23.07%)presenteddiabetes(typesIorII).Diabetesand
arte-rial hypertension occurred in association in eight patients
(20.51%);two(5.12%)saidthattheyweresmokers; andtwo
(5.12%)presentedrheumatoidarthritis.Fivepatients(12.82%)
didnothaveanycomorbidities(Table2).
Accordingtothetimethathadelapsedfromthesurgery
to the appearance ofsigns and symptoms ofinfection, 19
patientspresentedearlyinfection (48.72%),eighthad
inter-mediateinfection(20.52%)and12hadlateinfection(30.76%).
Table1–Pathogensidentifiedinintraoperativeissue cultures.
Typesofculturesidentified N %
Staphylococcusaureus 15 31.25
Pseudomonasaeruginosa 11 22.92
Coagulase-negativeStaphylococcus 7 14.58
Enterobactersp. 5 10.41
Streptococcuspyogenes 4 8.33
Escherichiacoli 2 4.16
Corynebacteriumsp. 1 2.1
Stenotrophomonasmaltophilia 1 2.1
Enterococcussp. 1 2.1
Proteusmirabilis 1 2.1
Total 48 100.0
Inrelationtotherapyfortheinfectedarthroplastycases,
arevision prosthesisimplantedintwo stageswas used in
20patients(51.3%),anonconventionalendoprosthesisinone
(2.6%), arthrodesis in 12 (30.7%) and chronic suppression
antibiotictherapy inone (2.6%). Infection-associated death occurredinthecasesoffivepatients(12.8%).
Inrelationtotheanalysisonriskfactorsassociatedwith thetherapeuticoutcome,i.e.failure(NF)orsuccess(F)ofthe surgicalprocedureassociatedwiththecurefortheinfection intheprimaryTKA,weobservedthatvariablessuchasage, sex,presenceofprimaryorsecondary arthrosis, identifica-tionofbacteriaincultures,monomicrobialorpolymicrobial infections,presenceorabsenceofStaphylococcusaureus, iden-tificationofpathogensinmorethanonetissuesampleand
presenceof comorbidities did notdemonstrate any
statis-ticallysignificantassociation withthe outcomes described.
However, in the cases of infection diagnosed up to three
months after the surgery (early period), there was a
sta-tisticallysignificantassociationwithnonfunctionalsurgical treatment(NF)(OR:14.0;95%CI:1.5–133.2;p=0.016)(Table3).
Analysisonthevariablesassociatedwithdeathsecondary
toinfectionshowedthatonlythepatientswithdiabetes
mel-litushadastatisticallysignificantassociationwithdeath(OR:
11.3;95%CI:1.4–89.3;p=0.032).
Table2–Distributionoftypesofcomorbidities presentedbypatients(someofthempresentedmore thanonetypeofcomorbidity).
Typesofcomorbidity N %
Arterialhypertension 31 54.4
Diabetes 9 15.8
Rheumatoidarthritis 2 3.5
Smoking 2 3.5
Stroke 1 1.8
Arrhythmia 1 1.8
Corticoiduse 1 1.8
Alcoholabuse 1 1.8
Liverdisease 1 1.8
Heartfailure 1 1.8
Obesity 1 1.8
Livertransplantation 1 1.8
Total 55 100.0
Discussion
Itisnowknownthatthenumberoftotalarthroplasty proce-duresperformedhasbeenincreasingrapidlyyearbyyear.It hasbeenestimatedthatbetween2005and2030,thenumberof TKAproceduresperformedintheUnitedStatesisexpectedto increasebyupto673%andreachthelevelof3.48million pro-ceduresperyear.6,13Improvementoftheoperativetechniques
andasepsisprocedures,anduseofpreoperativeantibiotics,
hasreducedtheriskofinfectioninprimaryprostheses.14,15
However,evenwiththesechanges,theincreaseinthe
num-berofprocedureshasgeneratedever-greaternumbersofcases
ofinfectionthatrequiresurgicaltreatment.15 Theinfection
ratesinpreviousstudiesrangedfrom1%to5%forinfections
inprimaryarthroplastycases.16AtSantaCasadeMisericórdia
deSãoPaulo,whichisteachinghospitalthatattendspatients
withintheBrazilianNationalHealthSystem(SUS),the
infec-tionrateafterprimarykneearthroplastywasassessedas6.4%
overtheperiodfrom1994to2008.Thisfigureprobablyreflects
surgicaltreatmentsforpatientswithcomorbiditiessuchas
diabetesmellitus,infectionsofgreaterseverity(suchasthose
thatoccurduringtheearlyperiod,i.e.uptothreemonthsafter
thesurgery)andpolymicrobialinfectioncausedbypathogens
presenting greater bacterial resistance. Ong et al.17
evalu-atedthe riskfactors forinfection inacohort consistingof
a largenumber ofindividualswho underwent primary hip
arthroplastyandconcludedthatinoperationsperformedin
medicalinstitutionswithpublicattendance(Medicare),
pres-ence ofcomorbidities,male sexand prolonged durationof
surgeryinfluencedtheinfectionrates.
Amongthepatientswithadiagnosisofearlyinfection,it
wasobservedthattheriskofanonfunctionalsurgicaloutcome
fromtreatinginfectionswas14timesgreaterthaninthecases
ofintermediateandlateinfection.Thediabeticspresenteda
higherriskofdeath,possiblyassociatedwiththecomplexity
andextentoftheinfection.Lafferetal.18demonstratedthat
patientswithinfectedkneearthroplastydiagnosedduringthe
intermediate phase presenteda higher rateof unfavorable
outcomes,probablybecauseoflatediagnosisoftheinfection.
Althoughwithoutstatisticalsignificance,possiblyrelated
tothesmallnumberofinfectedindividualsinthefinalsample,
thepatientsofmoreadvancedageandmalesexwithdiabetes
presentedgreaterriskofnonfunctionalevolutioninthe
sur-gicaltreatment.InfectionscausedbyStaphylococcusaureusin
individualswithsecondaryarthrosispresentedgreaterriskof
death.Galatetal.9analyzedtheriskfactorsforearly
complica-tionsoftheoperativewoundinmorethan17,000individuals
who underwent primaryTKA and foundthat thepresence
of diabetes mellitus had a statistically significant
associa-tionwiththeriskofinfection.Infectionsinkneearthroplasty
casescausedbyS.aureus,andparticularlyoxacillin-resistantS.
aureus,hasalreadybeencorrelatedwithunfavorableevolution
inotherpublishedpapers.19
Themean ageof the patientsevaluated was 69.4 years
and among those of advanced age (over 80 years), there
wasanonsignificantassociationwithnonfunctionalevolution
from surgicaltherapy, possiblyrelatedtothe smallsample
size (odds ratio=2.2). In a retrospective cohort of infected
Table3–Riskfactorsassociatedwiththerapeuticfailureorsuccessintreatinginfectedtotalkneearthroplastycases.
Characteristics Result Total p-Valuea Oddsratio
Therapeutic successN=22
(%)
Therapeutic failureN=17
(%)
N=39 (%) Estimate 95%CIc
Age
41–59years 3(60.0) 2(40.00) 5 12.8 0.927 (ref)b
60–69years 7(58.33) 5(41.67) 12 30.8 1.1 0.1 – 9
70–79years 10(58.82) 7(41.18) 17 43.6 1 0.1 – 8
80–89years 2(40.0) 3(60.00) 5 12.8 2.2 0.2 – 28.3
Sex
Female 20(60.60) 13(39.40) 33 84.6 0.374 (ref)b
Male 2(33.33) 4(66.67) 6 15.4 3.1 0.5 – 19.3
Diagnosis
Primary 15(51.72) 14(48.28) 29 74.4 0.464 (ref)b
Secondary 7(70.0) 3(30.0) 10 25.6 0.5 0.1 – 2.1
Time
Early 8(36.36) 14(63.64) 22 56.4 0.016* 14 1.5 – 133.2
Intermediate 8(88.89) 1(11.11) 9 23.1 (ref)b
Late 6(75.00) 2(25.00) 8 20.5 2.7 0.2 – 36.8
Numberofcomorbidities
0 3(50.00) 3(50.00) 6 15.4 0.738 (ref)b
1 14(60.87) 9(39.13) 23 59 0.6 0.1 – 3.9
2ormore 5(50.00) 5(50.00) 10 25.6 1 0.1 – 7.6
Hypertension
No 5(62.5) 3(37.5) 8 20.5 1 (ref)b
Yes 17(54.83) 14(45.17) 31 79.5 1.4 0.3 – 6.8
Diabetic
No 20(62.5) 12(37.5) 32 82.1 0.206 (ref)b
Yes 2(28.57) 5(71.43) 7 18 4.2 0.7 – 24.9
Total 22(56.41) 17(43.59) 39 100
a ResultfromFisher’sexacttest. b Referencegroup.
c 95%confidenceinterval.
∗ 5%significancelevel(p-valuep<0.05).
maintenanceoftheprosthesis,themeanagewasalsohigh
(74years).20
Out of the 39 patients evaluated in our study, 56.4%
presentedearly infection. Intermediate and late infections
occurred in 23.1% and 20.5%, respectively. Early infections
generallyresultfromperioperativecontaminationcausedby
pathogenic agents such as Staphylococcus aureus or
Gram-negativebacilli,whichproduceacutemanifestationssuchas
localpain,erythema,edemaandheatintheoperativewound,
infectedhematomasandfever.Lateinfectionsmaybeginwith
symptomsofsepsisandgenerallyresultfromhematogenic
disseminationofdistantfoci.6,12,21,22
Staphylococcussp.wasidentifiedin45%ofthecases,and
Staphylococcusaureusin32%.Byrenetal.19evaluatedinfections
subsequenttoarthroplastyproceduresandfound
Staphylococ-cusaureusin42%ofthecases.Marculescuetal.20diagnosedan
infectionrateduetoStaphylococcusaureusof32%,i.e.afigure
similartowhatwefound.
In our sample, 12.8% evolved to death, which was a
high number in comparison with Carvalho Junior et al.,23
who found a death rate of 2.5% out of 120 primary
knee arthroplasty cases. However, Morrey et al.24 found a
death rate of 7% out of 501 unilateral knee arthroplasty
cases.
Amongourpatients,37%evolvedtosalvagesurgical
pro-cedures (nonfunctional), which was a higher number with
this outcomethan foundbyD’Eliaetal.,25 who foundthat
only6.9%oftheir patients showedthis,between 2003and
2004.Itisimportanttoemphasizethatrevisionarthroplasty
totreat infectionswas notsocommonly performedinour
institution inthe 1990s,whichresultedinalarger number
ofarthrodesisproceduresinthepast.From1994to2001,20
caseswereevaluatedduetoinfection.Ofthese,eight(40%)
underwentarthrodesis.Ontheotherhand,from2002to2008,
therewere19cases,ofwhichfour(21%)underwent
arthrode-sis.
Conclusion
Patientswithearlyinfectionpresentedgreaterriskof
evolv-ingtowardsurgicalprocedureswithnonfunctionaloutcomes
(arthrodesis)anddiabeticspresentedagreaterchanceofdeath
Conflicts
of
interest
Theauthorsdeclarethattherewerenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. ChoiHR,vonKnochF,ZurakowskiD,NelsonSB,MalchauH. Canimplantretentionberecommendedfortreatmentof infectedTKA?ClinOrthopRelatRes.2011;469:961–9.
2. MulveyTJ,ThornhillTS.Infectedtotalkneearthroplasty.In: InsallJN,ScottWN,editors.Surgeryoftheknee.NewYork: ChurchillLivingston;2001.p.1875–95.
3. IveyFM,HicksCA,CalhounJH,MaderJT.Treatmentoptions forinfectedkneearthroplasties.RevInfectDis.
1990;12:468–78.
4. LetaifOB,FrucchiR,D’EliaCO,DemangeMK,Albuquerque RFM,RezendeMU,PecoraJR,HernandezAJ,CamanhoGL. Comparac¸ãofuncionalentrerevisãodeartroplastiadejoelho sépticaeasséptica.ActaOrtopBras.2009;17:159–61.
5. LeonhardtMC,D’EliaCO,SantosALG,LimaANLM,PécoraJR, CamanhoGL.Revisãodaartroplastiatotaldejoelhoemdois tempos:ovalordaculturaobtidaporbiópsiaartroscópica. ActaOrtopBras.2006;14:226–8.
6. SalesMJP.Novosconceitosnotratamentodasinfecc¸ões associadasaprótesesarticularesortopédicas.Prática Hospitalar.2008;X:1–4.
7. WhitesideLA,PeppersM,NayfehTA,RoyME.
Methicillin-resistantStaphylococcusaureusinTKAtreatedwith revisionanddirectintra-articularantibioticinfusion.Clin OrthopRelatRes.2011;469:26–33.
8. BoothJrRE,LotkePA.Theresultsofspacerblocktechniquein revisionofinfectedtotalkneearthroplasty.ClinOrthopRelat Res.1989:57–60.
9. GalatDD,McGovernSC,LarsonDR,HarringtonJR,Hanssen AD,ClarkeHD.Surgicaltreatmentofearlywound
complicationsfollowingprimarytotalkneearthroplasty.J BoneJointSurgAm.2009;91:48–54.
10.SiaIG,BerbariEF,KarchmerAW.Prostheticjointinfections. InfectDisClinNorthAm.2005;19:885–914.
11.EspositoS,LeoneS,BassettiM,BorrèS,LeonciniF,MeaniE, etal.BoneJointInfectionsCommitteefortheItalianSociety ofInfectiousTropicalDiseases(Simit).Italianguidelinesfor thediagnosisandinfectiousdiseasemanagementof osteomyelitisandprostheticjointinfectionsinadults. Infection.2009;37:478–96.
12.ZimmerliW,TrampuzA,OchsnerPE.Prosthetic-joint infections.NEnglJMed.2004;351:1645–54.
13.WidmerAF,FreiR,RajacicZ,ZimmerliW.Correlation betweeninvivoandinvitroefficacyofantimicrobialagents againstforeignbodyinfections.JInfectDis.1990;162: 96–102.
14.HuoMH,GilbertNF,ParviziJ.What’snewintotalhip arthroplasty.JBoneJointSurgAm.2007;89:1874–85.
15.HsiehPH,LeeMS,HsuKY,ChangYH,ShihHN,UengSW. Gram-negativeprostheticjointinfections:riskfactorsand outcomeoftreatment.ClinInfectDis.2009;1–49:1036–43.
16.MortazaviSM,SchwartzenbergerJ,AustinMS,PurtillJJ, ParviziJ.Revisiontotalkneearthroplastyinfection:incidence andpredictors.ClinOrthopRelatRes.2010;468:2052–9.
17.OngKL,KurtzSM,LauE,BozicKJ,BerryDJ,ParviziJ.Prosthetic jointinfectionriskaftertotalhiparthroplastyintheMedicare population.JArthroplasty.2009;246Suppl:105–9.
18.LafferRR,GraberP,OchsnerPE,ZimmerliW.Outcomeof prostheticknee-associatedinfection:evaluationof40 consecutiveepisodesatasinglecentre.ClinMicrobiolInfect. 2006;12:433–9.
19.ByrenI,BejonP,AtkinsBL,AngusB,MastersS,
McLardy-SmithP,etal.Onehundredandtwelveinfected arthroplastiestreatedwithDair(debridement,antibiotics, andimplantretention):antibioticdurationandoutcome.J AntimicrobChemother.2009;63:1264–71.
20.MarculescuCE,BerbariEF,HanssenAD,SteckelbergJM, HarmsenSW,MandrekarJN,etal.Outcomeofprostheticjoint infectionstreatedwithdebridementandretentionof components.ClinInfectDis.2006;42:471–8,15.
21.TrampuzA,WidmerAF.Infectionsassociatedwith orthopedicimplants.CurrOpinInfectDis.2006;19:349–56.
22.WidmerAF.Newdevelopmentsindiagnosisandtreatmentof infectioninorthopedicimplants.ClinInfectDis.2001;1–33 Suppl2:S94–106.
23.CarvalhoJuniorLH,CastroCAC,Gonc¸alvesMBJ,Rodrigues LCM,LopesFL,CunhaFVP.Complicac¸õesdecurtoprazoda artroplastiatotaldojoelho:avaliac¸ãode120casos.RevBras Ortop.2006;41:162–6.
24.MorreyBF,AdamsRA,IlstrupDM,BryanRS.Complications andmortalityassociatedwithbilateralorunilateraltotal kneearthroplasty.JBoneJointSurgAm.1987;69:484–8.