FRONTOTEM PORAL DEM ENTIA WITH
SEVERE THALAM IC INVOLVEM ENT
A clin ical an d n eu ro p at h o lo g ical st u d y
M árcia Radanovic
1, Sérgio Rosemberg
2, Rogério Adas
3, St ênio C. M iranda
3,
Paulo Caramelli
4, Leonardo Caixet a
3, Ricardo Nit rini
5ABSTRACT - Frontotem p oral d em entia (FTD) is the third -lead ing cause of cortical d em entia after Alzheim er’s d isease and Lew y b od y d em entia, and is characterized b y a d em entia w here b ehavioral d isturb ances are p rom inent and ap p ear early in the course of the d isease. We rep ort the case of a 58 year-old m an affected b y d em entia w ith b ehavioral d isturb ances, in ad d ition to rig id -hyp okinetic and a low er m otor neuron synd rom e t h at w ere p resen t at lat er st ag es o f t h e illn ess. Neu ro im ag in g st u d ies sh o w ed fro n t o t em p o ral at ro p h y. Neurop atholog ical stud ies revealed intense thalam ic neuronal loss and astrocytic g liosis, as w ell as m od erate frontotem poral neuronal loss, astrocytosis and spongiform degeneration. Thalam ic degeneration has previously b een d escrib ed am ong the w id e g roup of neurop atholog ical features of FTD. The aim of the p resent stud y is to show the clinical and neurop atholog ical asp ects of thalam ic d eg eneration in FTD, along w ith its role in b ehavioral d isturb ances, a com m on find ing in this cond ition.
KEY WORDS: frontotem p oral d em entia, thalam ic d eg eneration, neurop atholog ical find ing s.
Demência frontotemporal com intenso envolvimento talâmico: estudo clínico e neuropatológico
RESUMO - Dem ência frontotem p oral (DFT) é a terceira causa d e d em ência cortical, ap ós d oença d e Alzheim er e d em encia d os corp os d e Lew y, caracterizand o-se p or ser um a sínd rom e d em encial em q ue as alterações d e com p ortam ento são p roem inentes e ap arecem p recocem ente. Descrevem os o caso d e um hom em d e 58 anos ap resentand o d em ência com exp ressiva alteração d e com p ortam ento, som ad as a sínd rom e rígid o-hip ocinética e d e n eu rô n io m o t o r in ferio r. Os exam es d e n eu ro im ag em m o st raram at ro fia fro n t o t em p o ral. O exam e neuropatológico revelou intensa perda neuronal e astrocitose talâm ica, bem com o m oderada depleção neuronal frontotem p oral, com astrocitose e d eg eneração esp ong iform e. Deg eneração talâm ica já foi d escrita entre os p ossíveis achad os neurop atológ icos na DFT. O ob jetivo d este estud o é contrib uir com um a d escrição d os asp ectos clínicos e neurop atológ icos d a d eg eneração talâm ica na DFT, b em com o seu envolvim ento nos transtornos d e com p ortam ento, tão freq üentes nesta cond ição clínica.
PALAVRAS-CHAVE: d em ência frontotem p oral, d eg eneração talâm ica, achad os neurop atológ icos.
Beh avio ral an d Co g n it ive Neu ro lo g y Un it , Dep art m en t o f Neu ro lo g y 1,3,4,5Dep art m en t o f Pat h o lo g y, 2Un iversit y o f São Pau lo Sch o o l o f
Med icine, São Paulo SP, Brazil: 1M.D., Consultant Neurolog ist, 2M.D., Associate Professor, 3M.D,4M.D., Assistant Professor, 5M.D., Associate
Pro fesso r
Received 5 May 2003, received in fin al fo rm 15 Ju ly 2003. Accep t ed 6 Au g u st 2003.
Dra. M árcia Radanovic - Rua Crist iano Viana 163/92 - 05411-000 São Paulo SP - Brasil. E-mail: radano@t ecw ay.com.br
Fro n t o t em p o ra l d em en t ia (FTD) rep resen t s 10-20% o f all d em en t ias (b ein g t h e t h ird -lead in g cau se o f co rt ical d em en t ia aft er Alzh eim er’s d isease an d Lew y b od y d em entia)1,2. Loss of p ersonal aw areness,
im p ulsiveness, ap athy, lack of initiative, p erseverative b e h a vio r, h yp e ro ra lit y, p ro g re ssive re d u ct io n o f sp eech an d p reserved sp at ial ab ilit ies, t o g et h er w it h fro n t o t em p o ra l a t ro p h y o n CT o r MRI sca n s a n d h yp o p erfu sio n / h yp o m et ab o lism in fro n t al, t em p o -ral and frontotem p o-ral regions in SPECT and PET
stud ies, are finstud ing s that m ake for a very p rob ab le stud iag -n o sis o f FTD. Fam ily h ist o ry is d escrib ed i-n 20-40 % o f su ch cases. A rig id -h yp o kin et ic an d lo w er m o t o r syn d ro m es h ave also b een d escrib ed in lat er st ag es of FTD3,4.
Th e Lu n d an d Man ch est er Gro u p s5 d efin ed t h ree
-Arq Neu ro p siq u iat r 2003;61(4) 931
m o n p at h o lo g ical fin d in g s in FTD are b ilat eral an d sym m et rical at ro p h y in t h e fro n t o t em p o ral reg io n s, with striatal degeneration. There m ay be a correlation b et w een t h e clin ical p resen t at io n an d t h e p red o m i-n ai-n t sit e o f at ro p h y: t h e o rb it o m ed ial fro i-n t al co rt ex is m o re affect ed in t h o se p at ien t s w it h o veract ivit y an d d isin h ib it io n , w h ile t h e d o rso lat eral fro n t al co r-t ex is m o re affecr-t ed in r-t h o se p resen r-t in g ap ar-t h y. In so m e cases, t h e st riat al d eg en erat io n is severe an d acco m p an ied b y im p o rt an t lim b ic an d n ig ral alt era-t io n s, an d era-t h is su b g ro u p o f p aera-t ien era-t s is p ro n e era-t o d e-velo p st ereo t yp ic an d rit u alist ic b eh avio r, t o g et h er with rigid - hyp okinetic synd rom e6,7. Histological
stu-d ies m ay sh o w t w o stu-d ist in ct p at t ern s: o n e w it h a se-vere lo ss o f n eu ro n s in layers III an d V, sp o n g ifo rm d eg en erat io n / m icro vacu o lat io n o f layer II an d m i-n im al g lio sis (fro i-n t al lo b e d eg ei-n erat io i-n ), ai-n d o t h er, b ein g less co m m o n , in w h ich t h ere is a severe lo ss o f cells an d g lio sis, b u t n o sp o n g ifo rm o r m icro vacu o lat io n ch an g es, w it h sw o llen n eu ro n s o r cell in -clu sio n s in so m e cases (Pick-t yp e). Th e st riat u m an d lim bic system seem to be m ore affected in the second p resen t a t io n5,8. Wh en t h e d em en t ia is a sso cia t ed
w it h m o t o r n eu ro n d isease, t h ere is a larg e lo ss o f cells, m icrovacuolation and m ild gliosis involving p re-d o m in a n t ly t h e o rb it o m ere-d ia l fro n t a l reg io n s; t h e
st riat u m an d lim b ic syst em are less affect ed , b u t se-vere n ig ra l a n d h yp o g lo ssa l d a m a g e ca n a lso b e fo u n d . Th ere is a m assive lo ss o f cells at all levels o f th e an terio r h o rn2,9.
We rep o rt t h e case o f a 58 year-o ld m an affect ed b y d em en t ia, w h ich h ad evo lved o ver a fivyear p e-riod, where behavioral disturbances were prom inent. Th ere w as a p o sit ive fam ily h ist o ry fo r d em en t ia. In ad d it io n , rig id -h yp o kin et ic an d lo w er m o t o r n eu ro n syn d ro m es w ere p resen t at lat er st ag es o f t h e illn ess w hile neuroim ag ing stud ies show ed frontotem p oral atro p h y. Neu ro p ath o lo g ical stu d ies revealed in ten se t h alam ic n eu ro n al lo ss an d ast ro cyt ic g lio sis, as w ell as m o d erat e fro n t o t em p o ral n eu ro n al lo ss, ast ro cy-t o sis an d sp o n g ifo rm d eg en eracy-t io n . Th alam ic d eg e-n erat io e-n h as p revio u sly b eee-n d escrib ed am o e-n g t h e w id e g ro u p o f n eu ro p at h o lo g ical feat u res o f FTD. Th e aim o f t h e p resen t st u d y is t o sh o w t h e clin ical an d n eu ro p at h o lo g ical asp ect s o f t h alam ic d eg en e-rat io n in FTD, alo n g w it h it s ro le in b eh avio ral d is-t u rb an ces, a co m m o n fin d in g in is-t h is co n d iis-t io n .
CASE
Ou r p at ien t is a 58 year-o ld , rig h t -h an d ed , Cau casian b u sin essm a n , w it h eig h t yea rs o f sch o o lin g . At t h e a g e o f 54 h e p resen t ed ap at h y an d lack o f in t erest in h is d aily act ivit ies, w h ich in it ially h ad b een at t rib u t ed t o fin an cial p ro b lem s. A g lo b al b eh avio ral ch an g e w as o b served in t h e su b seq u en t m o n t h s. Pa ra n o id d elu sio n s o ccu rred : h e alw ays felt threatened , trying to p rotect him self from im a-g in ary at t acks b y p o lice o r ro b b ers. At t h e sam e t im e, h e d em o n st rat ed u n in h ib it ed b eh avio r, o u t o f ch aract er w it h his p revious p ersonality p rofile, such as talking to strangers in t h e st reet , u n d ressin g h im self in p u b lic p la ces, b eg g in g for m oney, for instance. His b ehavior b ecam e p rogressively less in h ib it ed an d h e w as at t en d ed b y several p sych iat ric services, receivin g an t i-p sych o t ic d ru g s w it h p art ial resp o n se. On e year resp rio r t o ad m issio n , h e d evelo resp ed a resp ro g ressive m em o ry im p airm en t t h at d isab led h im fro m co n -tinuing his p rofessional activities. Furtherm ore, he had d if-ficulty in recog nizing friend s and relatives and hyp erorality sym p t o m s w ere n o t ed . Six m o n t h s lat er, h e b eg an d ep en -d in g o n relat ives t o p erfo rm b asic -d o m est ic t asks, su ch as feed in g , d ressin g a n d b a t h in g h im self, w it h g lo b a l in -co n t in en ce o ccu rrin g t h ree m o n t h s b efo re a d m issio n . No p revio u s syst em ic o r n eu ro lo g ica l illn ess, h ist o ry o f t ra u -m a, alcohol consu-m p tion or d rug ab use w ere p resent. The p at ien t h ad an o ld er b ro t h er, w h o d ied at t h e ag e o f 53 w it h a sim ilar d em en t ia last in g fo r fo u r years.
Th e g en eral p h ysical exam in at io n w as n o rm al, w h ile t h e n eu ro lo g ical exam in at io n sh o w ed a vig il, t im e/sp ace o rien t ed p at ien t , w it h red u ced verb al flu en cy, an d p reser-ved o ral co m p reh en sio n an d exp ressio n . Also , fro n t al re-lease sig n s an d g lo b al rig id ity w ere p resen t an d d em en tial syn d ro m e w it h b eh avio ral ab n o rm alit ies p red o m in at ed .
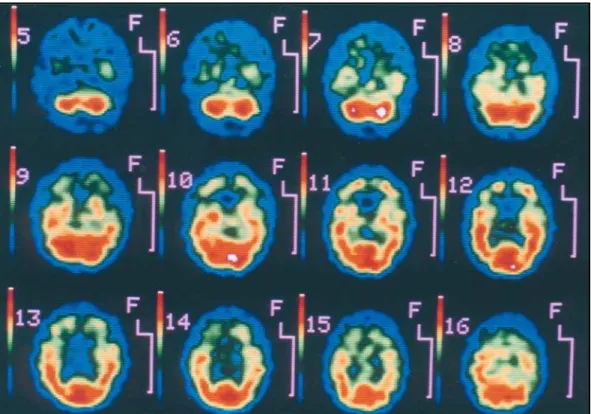
Th e sco re in t h e Min i-Men t al St at e Exam in at io n (MMSE) w as 26/30, revealin g im p airm en t in At t en t io n /Calcu lat io n (3/5), Recall (2/3) an d Co p yin g (0/1). Th e n eu ro p sych o lo -g ical exam in at io n in clu d ed t h e Mat t is Dem en t ia Rat in -g Scale (sco re: 101 / 144), an d t h e Ho o p er Visu al Org an iza-t io n , Wisco n sin Card So riza-t in g , Trail Makin g an d Ben iza-t o n Vi-su a l Ret en t io n t est s. Th e sco res o b t a in ed in t h e Ma t t is Dem en t ia Rat in g Scale sh o w ed a g reat er im p airm en t in Initiation/Perseveration (28/37), Concep tualization (20/39) an d Mem o ry (17/25). Th e o verall resu lt s d isclo sed a d eep im p a irm en t o f t h in kin g flexib ilit y, execu t ive fu n ct io n s, m em ory, visuosp atial and constructional skills. A b rain MRI scan (Fig 1) revealed p red om inant frontal cortical and sub -cortical atrop hy and ventricular enlargem ent without signs o f in t racran ial h yp ert en sio n . Brain SPECT sh o w ed h yp o -p erfu sio n in t h e fro n t al co rt ex an d su b co rt ical st ru ct u res such as the caud ate and thalam us (Fig 2). Blood tests w ere n o rm al an d sero lo g ic t est s fo r HIV an d fo r syp h ilis w ere n eg at ive. Cereb ro sp in al flu id an alysis sh o w ed n o ab n o r-m alit ies, w h ilst elect ro n eu ro r-m yo g rap h y revealed sig n s o f ch ro n ic d eg en era t io n in t h e a n t erio r h o rn cells. An a lysis of the p rion p rotein gene (b y single chain p olym erase reac-t io n ) d id n o reac-t sh o w an y m u reac-t areac-t io n .
Clinical course and neuropat hologic examinat ion
Mo n t h s a ft er a d m issio n , t h e p a t ien t d evelo p ed a p ro -g ressive lo ss o f co n t a ct w it h t h e en viro n m en t a n d a ri-g id h yp o kin et ic syn d ro m e. He w as b ed rid d en an d in a veg et a et ive set a et e in et h e fin a l set a g es o f et h e illn ess. Diset a l a m yo -t ro p h y an d fascicu la-t io n s co u ld b e seen . Th e su b jec-t d ied five ye a rs a ft e r p re se n t in g sym p t o m s, o f re sp ira t o ry co m p licat io n s.
General autopsy disclosed bilateral bronchopneum onia. The brain weighed 1,000 g. Gross evaluation of the brain showed wid ening of cereb ral sulci, m ore evid ent at the frontotem poral regions, along with ventricular dilatation a n d re la t ive sp a rin g o f su b co rt ica l st ru ct u re s (Fig 3 ). Histopathological study of the frontal cortex showed m o-derate to severe neuronal loss, with astrocytic gliosis m ore prom inent in the granular layer and spongiform changes in the outer cortical layers (II and III) (Fig 4). Marked neuronal depletion and astrocytosis were observed at the thalam us, especially in the dorsom edial nuclei (Fig 5), substantia nigra and the caudate. The im m unohistochem istry study for the detection of prion protein was negative.
DISCUSSION
Th e in it ial clin ical m an ifest at io n s o f t h is p at ien t (m arked p erso n alit y an d b eh avio ral ch an g es), t o g e-t h er w ie-t h e-t h e relae-t ive p reservae-t io n o f m em o ry an d lea rn in g fu n ct io n s, co rresp o n d t o t h e p ro g ressive co m p o rt m en t /execu t ive d ysfu n ct io n p ro file o f co g -nitive im p airm ent as d escrib ed b y Mesulam10. His
ini-t ial p erfo rm an ce in ini-t h e MMSE w as n o rm al, b u ini-t alrad y d isclo sed slig h t d ist u rb an ces in at t en t io n , m e-m ory and p raxis. The sub seq uent neurop sychological exam in at io n , h o w ever, sh o w ed a m o re w id esp read im p airm en t , w h ich p red o m in at ed in t h e execu t ive fu n ct io n s an d m em o ry. Availab le d at a fro m h ist o ry an d fro m clin ical exam in at io n , lab o rat o ry in vest ig at io n , n eu ro im ag in g sat u d ies an d at h e n eu ro p aat h o lo
Arq Neu ro p siq u iat r 2003;61(4) 933
g ical find ing s p oint to a FTD. The cortical histolog ical features includ ed neuronal loss, d iffuse astrocytosis, m o re evid en t in t h e g ran u lar layer, an d sp o n g io sis o f t h e o u t er layer (II an d III). A rem arkab le ast ro cy-t o sis a n d severe n eu ro n a l lo ss w ere fo u n d in cy-t h e t h alam u s, esp ecially in t h e d o rso m ed ial n u cleu s. A sim ilar p at t ern o f d eg en erat io n w as fo u n d in o t h er su b co rt ical st ru ct u res su ch as t h e cau d at e an d su b s-t an s-t ia n ig ra. All s-t h ese lesio n s fo llo w ed a m u ls-t ifo cal d ist rib u t io n an d are co m p at ib le w it h t h e d iag n o sis of FTD. Although the descriptions of the neuropatho-lo g ical feat u res o f FTD u su ally fo cu s o n t h e fro n t al, t em p o ral an d st riat al ab n o rm alit ies, t h alam ic d eg e-n erat io e-n w as also d escrib ed ie-n 1990 b y Ke-n o p m ae-n11
in w h a t h e t erm ed “d em en t ia la ckin g d ist in ct ive h ist o lo g y” (DLDH), a s w ell a s in o t h er st u d ies8 ,1 2.
Ho w ever, t h e p ro m in en ce o f t h e t h alam ic at ro p h y as w as fo u n d in o u r case is d ist in ct ly u n u su al.
Prim ary t h alam ic d eg en erat io n (PTD) cau sin g d e-m en t ia w as first d escrib ed in 1939 b y St ern13 in a
su b ject w h o p resen t ed severe at ro p h y o f ven t ral an -terior and dorsom edial thalam ic nuclei, and a variable d eg ree o f g lio sis in t h e cereb ral co rt ex. Mart in , in 197514, classified t h e t h alam ic d eg en erat io n s in t o :
p referen t ial t h alam ic d eg en erat io n , t h alam ic d eg e-neration associated w ith m ulti-system atrop hies and the thalam ic form of Creutzfeld tJakob d isease. Cog -n it ive alt erat io -n s i-n t h alam ic lesio -n s (t h alam ic d e-m en t ia) h ave b een w ell d o cu e-m en t ed in vascu lar an d d eg en erat ive lesio n s15-18. In t h e lat t er, t h ey m ay ap
-p ear in asso ciat io n w it h m o t o r n eu ro n d isease19 o r a
m o re d iffu se su b co rt ical at ro p h y, freq u en t ly b ein g fam ilial in ch aract er. Sin ce t h e d eg en erat ive alt erat io n s freq u en erat ly sp read erat o o erat h er su b co rerat ical serat ru cerat u -res, t h e t erm “su b co rt ical g lio sis” is also ap p lied t o su ch cases o f p ro g ressive d em en t ia asso ciat ed w it h variab le co rtical n eu ro n al lo ss an d su b co rtical / d eep w h it e m at t er g lio sis20-22.
Fig 3. Coronal sect ion of t he brain show ing w idening of sulci (especially f ront ot emporal) and vent ricular dilat at ion.
Th e t h alam u s h as m assive co n n ect io n s w it h t h e fro n t al lo b es, t h e lim b ic syst em an d t h e act ivat in g ret icu lar fo rm at io n o f t h e b rain st em , an d t h ese co n -n ect io -n s are d irect ly relat ed t o t h e m ech a-n ism s o f b eh avio ral co n tro l, em o tio n s an d m em o ry. Th alam ic nuclei are p art of the three frontal-sub cortical circuits t h at o rig in at e in t h e p refro n t al co rt ex an d w h ich are relat ed t o b eh avio ral an d co g n it ive fu n ct io n s. Th e d o rso m ed ial (p arvicellu lar an d m u lt ifo rm d ivisio n s) an d an t ero ven t ral n u clei are in sert ed in t h e d o rso la-t eral p refro n la-t al circu ila-t , w h ich is relala-t ed la-t o execu la-t ive functions and m otor p rogram m ing. The m agnocellu-lar d ivision of the d orsom ed ial and the anteroventral nuclei are also p art of the lateral orb itofrontal circuit, t h e in ju ry o f w h ich lead s t o p erso n alit y ch an g es an d m o o d alt erat io n s, esp ecially irrit ab ilit y (fo r t h is rea-so n , t h e an t ero ven t ral an d d o rrea-so m ed ial n u clei are u su ally referred t o as t h e “lim b ic t h alam u s”). So m e sp ecific reg io n s o f t h e d o rso m ed ial n u cleu s b elo n g t o t h e an t erio r cin g u lat e circu it w h ere lesio n s o f t h is circu it are asso ciat ed w it h ap at h y an d akin et ic m u -t ism23,24. Th e t h alam o fro n t al t ract s o rig in at e in t h e
anterior and m edial nuclei of the thalam us, and som e st u d ies h ave d escrib ed a p ict u re t h at very m u ch re-sem b les a “fro n t al syn d ro m e” in p at ien t s w it h sm all in farct s in vo lvin g t h ese t ract s. Th e an t erio r n u cleu s is also co n n ect ed w it h t h e m am m ilary b o d ies (via t h e m am m illo t h alam ic t ract ), p layin g an im p o rt an t role in the production of em otions and m em ory func-t io n s16,25. Th ese n eu ro an at o m ical p ecu liarit ies m ay
reflect in t h e clin ical p ict u re o f FTD: t h o se p at ien t s in w h o m a relat ive sp arin g o f t h e t h alam u s o ccu rs,
m ay in it ially h ave a “d isin h ib it ed ” fro n t al syn d ro m e, b u t as t h e d isease evo lves t o a m o re severe p at h o lo -g ical sta-g e, the involvem ent of the b asal -g an-g lia and t h e t h alam ic n u clei (as p resen t ed in t h is case) can usually b e correlated with an “ap athetic” frontal syn-d ro m e syn-d u e t o t h e im p o rt an t ro le o f t h ese st ru ct u res in at t en t io n an d aw aren ess26.
In co n clu sio n , t h alam ic d eg en erat io n , esp ecially w h en in vo lvin g t h e d o rso m ed ial n u cleu s, m ay b e in -cluded in the spectrum of neuropathological findings fo r FTD an d m ay co n t rib u t e t o in t en sifyin g t h e b e-h avio ral d ist u rb an ces alread y fo u n d in t e-h ese cases.
Acknow ledgements - We are ind eb ted to Dr. Françoise Gray fo r p erfo rm in g t h e im m u n o h ist o ch em ical st u d y fo r d et ect io n o f p rio n p ro t ein s an d t o Dr. David S. Kn o p m an fo r h is co m m en t s an d in fo rm at io n t h at h elp ed t o sh arp en t h e d iscu ssio n .
REFERENCES
1. Gustafson L. Clinical picture of frontal lobe degeneration of non-Alzheimer type. Dementia 1993;4:143-148.
2. Jackson M, Lowe J. The new neuropathology of degenerative frontotemporal dementias. Acta Neuropathol 1996;91:127-134. 3. Mendez MF, Cherrier M, Perryman KM, Pachana N, Miller BL,
Cummings JL. Fronto-temporal dementia versus Alzheimer’s disease: differential cognitive features. Neurology 1996;47:1189-1194. 4. Miller BL, Ikonte C, Ponton M, et al. A study on the Lund-Manchester
research criteria for frontotemporal dementia: clinical and single-photon emission CT correlations. Neurology 1997;48:937-942.
5. Brun A, Englund E, Gustafson L, et al. Clinical and neuropathological criteria for frontotemporal dementia the Lund and Manchester Groups. J Neurol Neurosurg Psychiatry. 1994;57:416-418.
6. Neary D, Snowden J. Fronto-temporal dementia: nosology, neuropsychology, and neuropathology. Brain Cogn 1996;31:176-187. 7. Caixeta L, Nitrini R. Clinical subtypes of frontotemporal dementia. Arq
Arq Neu ro p siq u iat r 2003;61(4) 935
8. Mann DM, South PW, Snowden JS, Neary D. Dementia of frontal lobe type: neuropathology and immunohistochemistry. J Neurol Neurosurg Psychiatry 1993;56:605-614.
9. Neary D, Snowden JS, Mann DMA, Northen B, Goulding PJ, McDermott N. Frontal lobe dementia and motor neuron disease. J Neurol Neurosurg Psychiatry 1990;53:23-32.
10. Mesulam M-M. Behavioral Neuroanatomy. In Mesulam M-M (ed). Principles of behavioral and cognitive neurology.2.Ed. New York: Oxford Univ Press, 2000:1-120.
11. Knopman DS, Mastri AR, Frey WH, Rustan T. Dementia lacking distinctive histologic features: a common non-Alzheimer degenerative dementia. Neurology 1990;40:251-256.
12. Mann DM, South PW. The topographic distribution of brain atrophy in frontal lobe dementia. Acta Neuropathol (Berl) 1993;85:334-340. 13. Stern K. Severe dementia associated with bilateral symmetrical
degeneration of the thalamus. Brain 1939;62:157-171.
14. Martin JJ. Thalamic degenerations. In Vinken PJ, Bruyn GW (eds). Handbook of clinical neurology, vol. 21. Amsterdam: North-Holland, 1975:587-604.
15. Martin JJ. Thalamic syndromes. In Vinken PJ, Bruyn GW (eds). Handbook of clinical neurology. vol. 2. Amsterdam: North-Holland, 1969:469-496.
16. Kalashnikova LA, Gulevskaya TS, Kashina EM. Disorders of higher mental function due to single infarctions in the thalamus and in the area of the thalamofrontal tracts. Neurosci Behav Physiol 1999;29:397-403. 17. Kornfeld M, Seelinger DF. Pure thalamic dementia with a single focus of
spongiform change in cerebral cortex. Clin Neuropathol 1994;13:77-81.
18. Krolak-Salmon P, Montavont A, Hermier M, Milliery M, Vighetto A. Thalamic venous infarction as a cause of subacute dementia. Neurology 2002;58:1689-1691.
19. Deymeer F, Smith TW, DeGirolani U, Drachman DA. Thalamic dementia and motor neuron disease. Neurology 1989;39:58-61. 20. Moossy J, Martinez AJ, Hanin I, Rao G, Yonas H, Boller F. Thalamic
subcortical gliosis with dementia. Arch Neurol 1987;44:510-513. 21. Verity MA, Wechsler AF. Progressive subcortical gliosis of Neumann:
a clinicopathologic study of two cases with review. Arch Gerontol Geriatr 1987;6:245-261.
22. Lanska DJ, Markesbery WR, Cochran E, Bennett D, Lanska MJ, Cohen M. Late-onset sporadic progressive subcortical gliosis. J Neurol Sci 1998;157:143-147.
23. Barbas H, Ghashghaei HT, Rempel-Clower NL, Xiao D. Anatomic basis of functional specialization in prefrontal cortices in primates. In Grafman J (ed). Handbook of neuropsychology vol. 7 2.Ed., Amsterdam: Elsevier, 2002:1-27. 24. McPherson S, Cummings JL. The frontal lobes and frontal-subcortical circuits in neuropsychiatric disorders. In Grafman J (ed). Handbook of neuropsychology vol. 7 2.Ed., Amsterdam: Elsevier, 2002:99-116. 25. Amaral DG. Functional organization of perception and movement. In
Kandel ER, Schwartz JH, Jessell TM (eds). Principles of neural science. 4.Ed. New York: McGraw-Hill, 2000:337-348.