w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Special
article
Primary
nodal
peripheral
T-cell
lymphomas:
diagnosis
and
therapeutic
considerations
Luis
Alberto
de
Pádua
Covas
Lage
a,
Tamara
Carvalho
dos
Santos
Cabral
a,∗,
Renata
de
Oliveira
Costa
b,
Marianne
de
Castro
Gonc¸alves
a,
Debora
Levy
a,
Maria
Cláudia
Nogueira
Zerbini
a,
Juliana
Pereira
aaFaculdadedeMedicina,UniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil bCentroUniversitárioLusíada(UNILUS),Santos,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received16September2014 Accepted10March2015 Availableonline7June2015
Keywords:
T-cellLymphoma Diseasesclassification Immunophenotyping WorldHealthOrganization Antineoplasticcombined chemotherapyprotocols
a
b
s
t
r
a
c
t
NodalperipheralT-celllymphomasareararegroupofneoplasmsderivedfrompost-thymic andactivatedTlymphocytes.AreviewofscientificarticleslistedinPubMed,Lilacs,and the Cochrane Library databaseswas performed usingthe term“peripheral T-cell lym-phomas”.AccordingtotheWorldHealthOrganizationclassificationofhematopoietictissue tumors, thisgroupofneoplasmsconsistsofperipheralT-celllymphomanototherwise specified(PTCL-NOS),angioimmunoblasticT-celllymphoma(AITL),anaplasticlargecell lymphoma-anaplastic lymphoma kinasepositive (ALCL-ALK+),anda provisional entity calledanaplasticlargecelllymphoma-anaplasticlymphomakinasenegative(ALCL-ALK−).
Because the treatmentand prognoses ofthese neoplasmsinvolve differentprinciples, it is essentialto distinguisheachone by its clinical,immunophenotypic, genetic, and molecularfeatures.Exceptforanaplasticlargecelllymphoma-anaplasticlymphomakinase positive,whichhasnoadverseinternationalprognosticindex,theprognosisofnodal periph-eralT-celllymphomasisworsethanthatofaggressiveB-celllymphomas.Chemotherapy basedonanthracyclinesprovidespooroutcomesbecausetheseneoplasmsfrequentlyhave multidrug-resistantphenotypes.Basedonthis,thecurrenttendencyistouseintensified cyclophosphamide,doxorubicin,vincristine,prednisolone(CHOP)regimenswiththe addi-tion ofnew drugs,andautologoushematopoieticstemcelltransplantation.Thispaper describestheclinicalfeaturesanddiagnosticmethods,andproposesatherapeutic algo-rithmfornodalperipheralT-celllymphomapatients.
©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthorat:RuaDr.OvídioPiresdeCampos,225,1◦andar,PAMB,sala61,CerqueiraCésar,05403-010SãoPaulo,SP,Brazil.
E-mailaddress:[email protected](T.C.d.S.Cabral).
http://dx.doi.org/10.1016/j.bjhh.2015.03.017
278
revbrashematolhemoter.2015;37(4):277–284Introduction
Non-Hodgkinlymphomas(NHLs)areaheterogeneousgroup of malignancies of the immune system, encompassing more than 40 entities with specific clinical, morphologic, immunophenotypic, and molecular characteristics. In the WesternWorld,NHLsoriginatefromBlymphocytesin85–90% ofcasesandfromlymphoidTcellsandnaturalkillercells(NK) in10–15%ofcases,whileT-celllymphomasrepresentahigher proportionofNHLcasesinAsiancountries,accountingforup to25%oftheseneoplasms.1
T-cellmalignanciesderivedfrom precursor orimmature T cells originate from leukemia-lymphoblastic T-cell lym-phoma.Otherwise, the NHLs thatoriginatefrom matureT lymphocytesorNKcellsarerecognizedasperipheralT-cell lymphomas(PTCL).Thelatterrepresent12–15%ofallNHLs and,accordingtotheWorldHealthOrganization(WHO) Clas-sificationofTumors,comprise22differententitiescategorized accordingtoclinicalpresentationasprimarynodal,primary extranodal,primarycutaneous,anddisseminatedorleukemic formsassummarizedinTable1.1–3
Thisreviewdiscussesthe mainclinical and therapeutic aspects of primary nodal PTCLs such as peripheral T-cell lymphoma not otherwise specified (PTCL-NOS), angioim-munoblastic T-cell lymphoma (AITL), anaplastic large-cell lymphoma-anaplastic lymphoma kinase (ALK) positive
Table1–WorldHealthOrganizationclassificationof
peripheralnaturalkiller(NK)/T-celllymphomas.
Primarycutaneouslymphomas
MycosisfungoidesandSézarysyndrome
PrimarycutaneousCD30+T-celllymphoproliferativedisease
-Primarycutaneousanaplasticlarge-celllymphoma(C-ALCL) -Lymphomatoidpapulosis(LYP)
PrimarycutaneousperipheralT-celllymphomas(PTCLs) -Gama-deltaT-celllymphoma
-CD8+aggressiveepidermotropiccytotoxic
-CD4+small-medium
NodalperipheralT-celllymphomas(PTCL)
PeripheralT-celllymphomanototherwisespecified(PTCL-NOS) AngioimmunoblasticT-celllymphoma(AITL)
Anaplasticlarge-celllymphoma(ALCL)anaplasticlymphomakinase (ALK)positive
Anaplasticlarge-celllymphoma(ALCL)ALKnegative(provisional)
ExtranodalperipheralT-celllymphomas
ExtranodalNK-T-celllymphoma,nasaltype Enteropathy-associatedT-celllymphoma(EATL) HepatosplenicT-celllymphoma(HSTL)
Subcutaneouspanniculitis-likeT-celllymphoma(SPTCL)
Epstein–Barrvirus(EBV)-positiveT-celllymphoproliferativechildhood disorders
-EBV-positiveT-celllymphoproliferativechildhooddisease -Hydroavacciniforme-like
Widespreadorleukemic
T-cellprolymphocyticleukemia(T-PLL)
T-celllargegranularlymphocyticleukemia(T-LGL)
ChroniclymphoproliferativedisordersofNKcells(provisional) AggressiveNK-cellleukemia
AdultT-cellleukemia/lymphoma
(ALCL-ALK+),andanaplasticlarge-celllymphoma-ALK
nega-tive(ALCL-ALK−).
Methods
AsystematicliteraturesearchusingPubMed,Lilacs(Literatura Latino-AmericanaedoCaribeemCiênciasdaSaúde),andthe Cochrane Library databases was conductedto identify sci-entific papersrelated tothe search term “peripheral T-cell lymphomas”. Onlypapersfocusedonhumansubjectswere included.
Clinicalandepidemiologicalaspects
PTCL-NOSarerepresentedbynodalorextranodalT-cell lym-phomasnototherwisecategorizedasanyspecificentityinthe currentWHOclassification.Thesetumorsrepresent60–70% ofall PTCLs,and 5–7% ofallNHLs. Theyoccur more com-monlyinadultswithamedianageof60years andhavea slightmalepredominance.4–6Althoughlymphnode
involve-mentpredominatesinthemajorityofcases,theselymphomas often disseminate to the bone marrow, liver, spleen, and otherextranodalsitessuchastheskinandlung.Theyrarely havealeukemicpresentation.5,6Patientsoftenpresentwith
unfavorable clinical characteristics including B symptoms, elevatedlactatedehydrogenase(LDH)levels,hightumor bur-den,advanceddisease(StageIIIorIV),andpoorperformance status.5,6
The AITL subtype is characterizedby a specific clinical syndromeandpolymorphicinfiltrateinvolvinglymphnodes, withproliferation ofhigh endothelialvenulesinatree-like patternandirregularproliferationoffolliculardendriticcells (FDC)withpredominantlyperivasculardistribution.AITL rep-resentsthesecondmostcommonsubtypeofPTCL(15–20%of cases)withitsprevalenceonlybeingexceededbyPTCL-NOS.It occursmostcommonlyinelderlypatients(aged60–65years), withaslightmalepredominance.7
Typical casesof AITL show acute or subacute systemic features that maymimic drugreactions or systemic infec-tions. Clinically, AITL presents as small and generalized lymphadenopathy, hepatosplenomegaly, and constitutional symptoms. Maculopapularrashoccursin50%ofcasesand paraneoplastic manifestations such as arthritis, vasculitis, serous effusions, and neurological manifestations are not uncommon. Laboratory featuresincludeeosinophilia, poly-clonal hypergammaglobulinemia, elevated serum LDH and erythrocyte sedimentation rate (ESR), as well as circulat-ing autoantibodies(cryoagglutinins,cryoglobulins, immune complexes, positivedirectCoombstest)andparaneoplastic phenomenaofanimmunenature(hemolyticanemia, leuko-cytoclasticvasculitis,rheumatoidarthritis,andautoimmune thyroiddisease).1,4,7
ALCL isaPTCLcharacterizedbylargepolymorphic lym-phoidCD30+ cellswithabundantcytoplasmand
horseshoe-orkidney-shapednuclei.Thethreerecognizedsubtypes are ALCL-ALK+, ALCL-ALK−, and primary cutaneous anaplastic
lymphoma.8 ALCL-ALK+ predominatesinyounger patients,
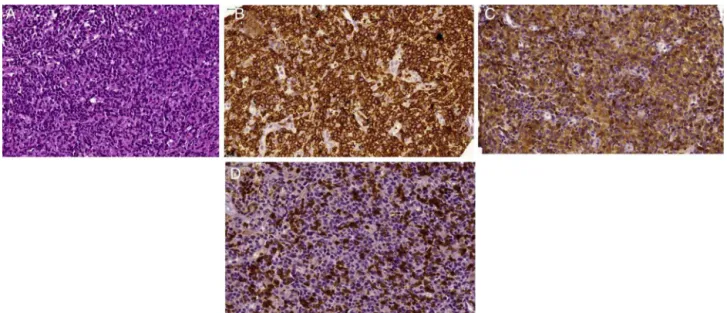
pre-Figure1–MorphologicaspectsofPeripheralT-celllymphomanototherwisespecified(PTCL-NOS).(A)Diffuseproliferation ofatypicalmediumsizedlymphoidcells.Notesomeintermingledeosinophils[hematoxylinandeosin(H&E)-stained section].(B)DiffuseexpressionofCD3bytheneoplasticlymphoidcells.(C)ThesecellsalsoexpressCD4.(D)CD7antigenis onlypartiallyexpressedbyneoplasticTcells.
dominance.Extranodalinvolvementisfrequent,and50%of casesarediagnosedatanadvancedstage(IIIor IV)and in patientswithBsymptoms.Themostcommonlyinvolvedsites includetheskin,subcutaneoustissue,bone,lung,andliver. Bonemarrowinvolvementoccursin10–30%ofcases,butthe leukemic phase isunusual and occurs more frequently in thesmall-cellmorphologicalvariant.Itrarelypresentswith gastrointestinal and central nervous system involvement. Despite the advanced stage involving multiple extranodal sites,mostpatientspresentwithlow-riskorlow-intermediate riskdisease accordingtotheInternationalPrognosticIndex (IPI),sinceperformance statusis frequently preservedand most patients are younger, with normal LDH levels at diagnosis.4,9
ALCL-ALK−ismorphologicallyindistinctfromALCL-ALK+,
butdoesnotshowchromosomaltranslocationsinvolvingthe
ALKgeneorexpressionoftheALKprotein.Thedisease pre-dominatesintheelderly; extranodalinvolvementoccurs in uptohalfofcasesandisusuallydiagnosedinpatientswith advancedstagediseasewhohaveBsymptomsandaggressive disease.Recently,anunusualvariantassociatedwith pros-theticbreastimplantsthathasanindolentbehaviorhasbeen described.8–10
Histopathologicalandmoleculardiagnosticcriteria
Anexcisional tumorbiopsyis essentialforcorrect diagno-sis.Needlebiopsyguidedbyimagingisnotrecommended.1It
shouldbehighlightedthatforthecorrectdiagnosisand classi-ficationofPTCL,histopathologicalanalysisbyanexperienced hematopathologistusingalargesamplewithaconsiderable amountoftissuethatallowsvisualizationofthebroadpattern oflymphnodeinfiltrationisnecessary,aswellasapplyinga wideimmunohistochemicalpanel.
InPTCL-NOS,thecompromisedlymphnodeshows para-corticalordiffuseinfiltrationwithlossofthenormallymph node architecturalpattern.Althoughlargetumorcells pre-dominate, a few cases exhibit small neoplastic cells. The morphologicspectrumvariesfrommonotonousto pleomor-phic cells with an excess of mitotic cells (Figure 1). The WHO classificationrecognizes histologicalvariantssuchas lymphoepitheliodlymphoma(Lennertlymphoma),follicular, and T-like zone. Phenotypically, it exhibits aberrant anti-gen expression characterized by a lack of T-cell markers suchasCD5andCD7.MostcasesexpresstheCD4antigen, although some others may be CD8+, particularly the
lym-phoepitheliodvariant. About 30%ofPTCL-NOS expressthe CD30 marker, but the phenotypic profile and morphologic aspect allow it to be distinguished from ALCL-ALK− since
thelatterexpressesepithelialmembraneantigens(EMA)and contains cytotoxicgranules.Distinguishingitfrom classical Hodgkin’slymphoma(HL)canbeachievedbyobservingthe expressionofCD15,PAX-5,andEpstein–Barrvirus(EBV).Also, PTCL-NOS present witha highproliferative rate,withKi67 higherthan70%,andstrongandhomogeneousexpressionof CD3.1,4,11CasesofPTCLCD30+/ALK−withnohistologic
simi-laritytoclassicALCLshouldbecategorizedasPTCL-NOS.1A
monoclonalrearrangementoftheT-cellreceptor(TCR)geneis usuallyseeninPTCL-NOSbypolymerasechainreaction(PCR); acytogeneticabnormalitywithcomplexkaryotypeistherule. Inthesubtypewithafolliculargrowthpattern,itiscommonto observetherecurrentaberrationt(5;9)(q33;q22)thatproduces theoncogenicproteinITK-SYK.11
280
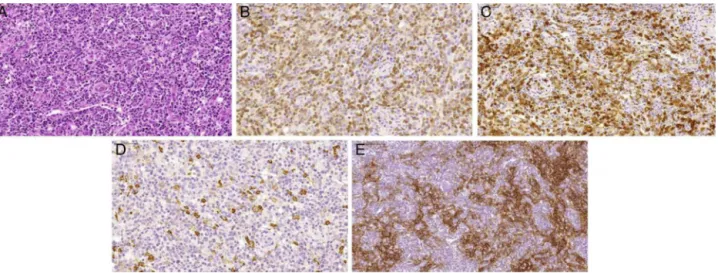
revbrashematolhemoter.2015;37(4):277–284Figure2–MorphologicaspectsofangioimmunoblasticT-celllymphoma.(A)Proliferationofsmalltomediumsized lymphoidcellswithmildatypiasurroundingprominenthighendothelialvenules.Occasionallargecellsareobserved,as wellassomeplasmocytes(H&E-stainedsection).(B)ThemajorityofneoplasticlymphoidcellsexpressmembraneCD3.(C) NeoplasticlymphoidcellsalsoexpressCD10.(D)CD20antibodyhighlightsthelargeBimmunoblasts.(E)Folliculardendritic cellmeshworkexpansionsurroundinghighendothelialvenulesisevidentwithCD21immunostain.
withatree-likepatternofendothelialvenulesandirregular proliferationofFDC.Bimmunoblastsareusuallypresentin theparacorticalregionandmaymimicHL(Figure2). Neoplas-ticcellsexpressapatternoffollicularThelpercellssuchas CD3+,CD4+,CD10+,BCL-6+,CXCL13+,PD1+,andICOS+ cells.
Indeed,vascularexpansioncanbedemonstratedby immuno-histochemistryforCD31andCD34.Irregularproliferationof FDCcanbedefinedbyCD21,CD23,andCD35stainingthat areoftenfoundwithvessels. TheB-cell-associated antigen markers,suchasCD20andCD79a,mayshowimmunoblasts intheinterfollicularareas.ThesecellsareinfectedbyEBVand are Reed-Sternberg-like cells mimicking classical HL.7,11–14
MostoftheAITLcasescontainamonoclonalpopulationofT cells.ThepresenceofBlymphocyteclonescanbedetected inup to 30% ofcases and the EBV genome isdetected in nearly100%.Karyotypicaberrationsoccurin70–80%ofcases, mainlytrisomyofchromosome3and5,andanadditionalX chromosome.11,15
AlthoughALCL-ALK+ presentswithabroad
morphologi-calspectrum,allcasescontainavariableproportionofcells witheccentricnuclei(kidney-likeorhorseshoe-shaped)with aneosinophilicperinuclearareacorrespondingtotheGolgi, and abundant cytoplasm; these cells are called ‘hallmark cells’.Themorphologicalfindings ofthisdisease varyfrom small to very large malignant cells (Figure 3). In addition, fivedistinctmorphologicalpatternsarerecognizedincluding classical,lymphohistiocytic,small-cell,‘Hodgkin-like’variant, andmixedpattern.9,11Theclassicalvariantsrepresent60–70%
ofallcasesandtheirmalignantcellsarealmostexclusively largeandsometimesReed-Sternberg-like. Whenthe lymph node architecture ispartially compromised, the cells grow withinsinusoidsandmay simulatemetastatictumors.The cellphenotypeexhibitsdiffusepositivityforCD30and some-timespresentsasa‘perinucleardot’thatcorrespondstoGolgi. ExpressionoftheCD2antigeniscommon,butCD45RO,CD5,
and CD7are usuallynegative.Mostpatientspresentwitha CD4+/CD8−phenotypeand showco-expressionofcytotoxic
antigenssuchasgranzyme B,TIA-1,perforinand theEMA antigen.4,9,11 Most casesof ALCL-ALK+ have t(2;5)(p23;q35),
resultinginthehybridproductNPM1-ALK.Inthesecases,the ALKproteincanbefoundinboththecytoplasmandnucleus. About90%oftheselymphomashaveaclonalrearrangement of the TCR gene. Inaddition to the classict(2;5), avariant chromosometranslocationinvolvingtheALKgeneandother geneslocatedonchromosomes1,2,3,17,19,22,andXmay occur. Themorphologicalandphenotypic aspectsof ALCL-ALK− cases are identical to those observed in ALCL-ALK+
cases.4,11,16
Prognosticfactors
DifferentstudieshaveshownthatthephenotypeofT-cell lym-phomascanbeeffectivelystratifiedusingtheIPI.17,18However,
aPrognosticIndexforT-cellLymphomas(PIT)wasdeveloped inanattempttoproducemoreaccurateprognosticindicators. Thisprognosticindexidentifiedfourriskfactors;age,serum LDH,performancestatus,andhistopathologicalinvolvement of the bone marrow. Patients were stratified into four risk groupswith0,1,2,ormorethan2riskfactorswithoverall survival(OS)of62%;53%,33%,and18%foreachriskgroup, respectively.19
AnotherindexisthemodifiedPrognosticIndexforT-cell Lymphoma (mPIT),whichincorporatesabiological variable (Ki67expression)andclinicalaspectssuchasage,LDH,and performancestatus.ThemPITdistinguishesthreedifferent riskgroups:goodriskprognosis,intermediaterisk,andpoor risk.20TheInternationalPeripheralT-cellLymphomaProject
Figure3–Morphologicaspectsofanaplasticlargecelllymphoma-anaplasticlymphomakinase(ALK)positive.(A)Diffuse proliferationoflarge,highlyatypicalcells,withprominentpleomorphism(H&E-stainedsection).Somehallmarkcellscan beobserved;theypresentlargemultilobulated‘horseshoe-like’nuclei.Neoplasticcellsshowdiffuseexpressionof(B)CD30; (C)CD43;(D)epithelialmembraneantigensand(E)ALK-1.Inthiscase,ALK-1positivitypresentexclusivecytoplasmic pattern.
Therapeutic
considerations
Conventional multidrug regimens used for aggressive B cell NHL such as CHOP are routinely considered for PTCL treatment.However,theoutcomeswithanthracycline-based regimens have been disappointing in patients with ALCL-ALK+ with lowrisk IPI.21–23 Theworseoutcome ofPTCL is
theresultofmanyadverse factorssuchashigh expression of P-glycoprotein, which is associated with the anthracy-cline resistancephenotype (MDR phenotype).3 Usually, the
overall response rate is low and there is a high rate of early death during first-line treatment. Relapses are com-monandoftenoccurinthefirst twoyears aftertreatment. Because of the lack of more effective treatment for PTCL that is not ALK positive, the CHOP regimen remains the mostcommonlyusedfirst-linetherapyforthese malignan-cies.Several studies demonstrated complete response (CR) rates of 50% and OS at 5 years of 30% with the CHOP regimen.23
Thesedisappointingresultsledtotheinvestigationofnew therapeuticstrategiessuchasintensifiedchemotherapyand alternativeprotocolssuchashigh-dosetherapyfollowedby rescuewithautologoushematopoieticstemcell transplanta-tion(aHSCT).Althoughtheresultsbetweendifferentstudies werediscordant,anintensifiedCHOPregimenwiththe addi-tionofetoposidehasshownbetterprogression-freesurvival (PFS),especiallyinunder60-year-oldpatientswithfavorable riskfactors.23–25
Althoughspontaneous remissions have been described, AITL often presents with an aggressive clinical course. Occasionally, asymptomatic patients may be observed or treated with corticosteroids or immunomodulators and antiangiogenicdrugssuchascyclosporine,thalidomide,and bevacizumab.Ingeneral,patientswithAITL requiring ther-apyshouldbeallocatedtoclinicalstudies.Ofthose,CHOPor
fludarabineandcyclophosphamide(FC)regimenshavebeen usedthemostoften.7,22,23
On the other hand, patients with ALCL-ALK+ without
adverse IPI risk factors have very chemosensitive disease that responds with comparable or superior outcomes to diffuse large B cell lymphoma (DLBCL) when treated with anthracycline-based therapy. Several studies have demon-strated overall responserate (ORR) of 90% withCHOP and 5-year OS of70–80%.ALCL-ALK− and ALCL-ALK+ high risk
groupshaveanintermediateprognosisbetweenALCL-ALK+
withoutadverseriskfactorsandPTCL-NOS,witha5-yearOS of49%forALCL-ALK−and19%forPTCL-NOS.Currently,the
management of these patients is similar to those positive forthe variantALKwith lowIPI,but because the outcome isworse, the same approachusedforPTCL-NOS is recom-mended, withintensificationof CHOP byadding etoposide orallocatingpatientstoclinicaltrialsorconsolidationwith aHSCT.6,16,22,23
Usually,thetherapeuticapproachtoPTCLdoesnotinvolve irradiation,whichisreservedforbulkydisease(tumorgreater than10cm)oraresidualmassafterchemotherapy.However, there isinsufficientevidence ofclinical benefitsusing this approach.ManygroupshaveevaluatedtheroleofaHSCTin PTCLthatisnotALKpositiveforfirstCRorpartialresponse (PR).Althoughcontroversial,outsideoftheclinicaltrial set-tingpatientswithAITL,ALCL-ALK−andPTCL-NOSshouldbe
treatedwithCHOP-liketherapyandconsolidatedwithaHSCT afterthefirstCRorPR.22,23,26–29
282
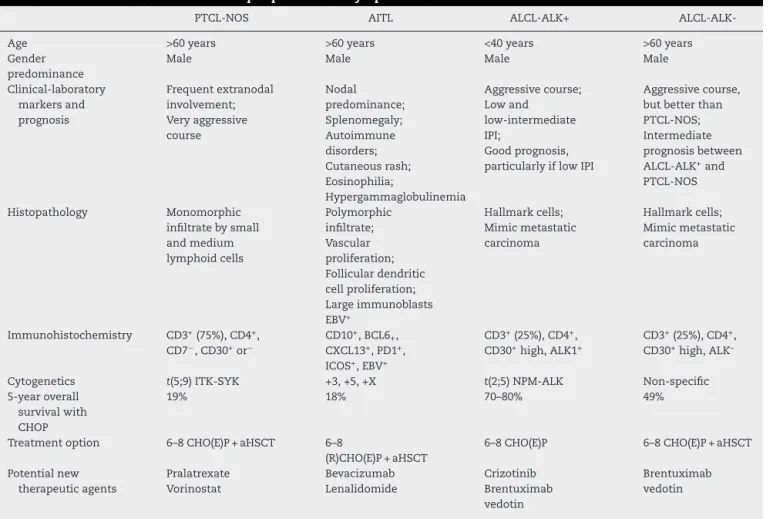
revbrashematolhemoter.2015;37(4):277–284Table2–MaincharacteristicsofnodalperipheralT-celllymphomas.
PTCL-NOS AITL ALCL-ALK+
ALCL-ALK-Age Gender predominance >60years Male >60years Male <40years Male >60years Male Clinical-laboratory markersand prognosis Frequentextranodal involvement; Veryaggressive course Nodal predominance; Splenomegaly; Autoimmune disorders; Cutaneousrash; Eosinophilia; Hypergammaglobulinemia Aggressivecourse; Lowand low-intermediate IPI; Goodprognosis, particularlyiflowIPI
Aggressivecourse, butbetterthan PTCL-NOS; Intermediate prognosisbetween ALCL-ALK+and
PTCL-NOS
Histopathology Monomorphic infiltratebysmall andmedium lymphoidcells Polymorphic infiltrate; Vascular proliferation; Folliculardendritic cellproliferation; Largeimmunoblasts EBV+ Hallmarkcells; Mimicmetastatic carcinoma Hallmarkcells; Mimicmetastatic carcinoma
Immunohistochemistry CD3+(75%),CD4+,
CD7−,CD30+or−
CD10+,BCL6 +,
CXCL13+,PD1+,
ICOS+,EBV+
CD3+(25%),CD4+,
CD30+high,ALK1+
CD3+(25%),CD4+,
CD30+high,ALK–
Cytogenetics t(5;9)ITK-SYK +3,+5,+X t(2;5)NPM-ALK Non-specific 5-yearoverall
survivalwith CHOP
19% 18% 70–80% 49%
Treatmentoption 6–8CHO(E)P+aHSCT 6–8
(R)CHO(E)P+aHSCT
6–8CHO(E)P 6–8CHO(E)P+aHSCT
Potentialnew therapeuticagents Pralatrexate Vorinostat Bevacizumab Lenalidomide Crizotinib Brentuximab vedotin Brentuximab vedotin
PTCL-NOS:peripheralT-celllymphomanototherwisespecified;AITL:angioimmunoblasticT-celllymphoma;ALCL-ALK+:anaplasticlargecell
lymphoma-anaplasticlymphomakinasepositive;ALCL-ALK−:anaplasticlargecelllymphoma-anaplasticlymphomakinasenegative;IPI:
Inter-nationalPrognosticIndex;EBV:Epstein–Barrvirus;CHO(E)P:cyclophosphamide,doxorubicin,vincristine,prednisolone;aHSCT:autologous hematopoieticstemcelltransplantation.
For many patients with PTCL, the available treatment strategies are ineffective and new therapies should be explored.Gemcitabineisanucleosideanalogthatovercomes the p-glycoprotein system. Bendamustine and antifolate agents such as pralatrexate are being tested in these lymphomas.32,33Therapywithmonoclonalantibodiessuchas
brentuximabvedotin(antiCD30),alemtuzumab(antiCD52), andzanolimumab(antiCD4)havealsobeenevaluated.
ForthesubgroupofPTCLpatientswhosetumorsexpress theCD30antigen,particularlysystemicALCLandCD30+
PTCL-NOS, brentuximab vedotin has emerged as an interesting therapy.Theantibody-drugconjugatecombinesamonoclonal antibodydirectedagainstCD30withapotentantimicrotubule agentnamed monomethylauristatin E (MMAE). CD30is an idealtherapeutic target because of its strong and uniform expressioninanaplasticlymphoma.Afterbindingtoits tar-getmolecule,brentuximabvedotinisinternalizedandMMAE is cleaved from the antibody molecule, exerting its action through inhibitionof microtubuleformation. In a phaseII multicenter trial of brentuximab vedotin in relapsed and refractoryALCL,theoverallresponseratewas86%,withaCR rateof53%.Significantadverseeventswereperipheral neu-ropathy,lungtoxicity,neutropenia,andthrombocytopenia.34
Anothernewinterestingdrugforthetreatmentofthese neoplasms is alisertib (MLN8237). This drug is a selective inhibitor of Aurora A kinase (AAK), and shows preclinical activity in PTCL cell lines and patient samples. Recently, Friedberg et al. reported the interim results of a phase II clinicaltrialofalisertibinpatientswithaggressiveBand T-cellNHL.ORRforthewholestudy populationwas32%,but whendividedbysubtype,patientswithPTCLhadanORRof 57%.35
A betterunderstanding ofthe pathophysiology ofthese tumors is allowing the use of targeted therapies, such as the ALK inhibitorcrizotinib, modulatorsofepigenetic phe-nomenon drugs able to restore the transcriptional status oftumorsuppressorgenes(histonedeacetylaseinhibitors), andimmunomodulatingagentsthathavegreaterantitumor activityinAITL.Diseaseprogressionisassociatedwithmore dysregulation of the immune system than tumor growth phenomena.31,36–40
Conclusion
Primary nodal peripheral T-cell lymphomas comprise a heterogeneousgroupofneoplasms arisingfrom the prolif-erationofactivatedlymphoidT-cells.Clinical,morphologic, immunophenotypic,genetic,andmolecularcriteriaareused to classify these neoplasms, which are frequently difficult to diagnose. Correct identification of each entity is criti-caltoestablishappropriatetherapeuticinterventions,which currently still offer poor response rates. Intensification of treatmentusingnewdrugsorspecificmonoclonal antibod-ies, as well as HSCT, may change this reality in the near future.Morestudiesarenecessarytodefinethebesttreatment approachfortheseentities.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. JaffeES,NicolaeA,PittalugaS.PeripheralT-cellNK-cell lymphomasintheWHOclassification:pearlsandpitfalls. ModPathol.2013;26Suppl.1:71–87.
2. JaffeES.PathobiologyofperipheralT-celllymphomas. HematolAmSocHematolEducProg.2006:317–22.
3. VoseJ,ArmitageJ,WeisenburgerD.Internationalperipheral T-cellandnaturalkillerlymphomastudy:pathologyfindings andclinicaloutcomes.JClinOncol.2008;26(25):4124–30.
4. DoganA,FeldmanAF.T-andNK-celllymphomaupdate. DiagnHistopathol.2009;16(2):99–110.
5. RizviMA,EvensAM,TallmanMS,NelsonBP,RosenST.T-cell non-Hodgkinlymphoma.Blood.2006;107(4):1255–64.
6. TangT,TayK,QuekR,TaoM,TanSY,TanL,etal.Peripheral T-celllymphoma:reviewandupdatesofcurrent
managementstrategies.AdvHematol.2010;2010:624040.
7. LevalL,GisselbrechtC,GaulardP.Advancesinthe understandingandmanagementofangioimmunoblastic T-celllymphoma.BrJHaematol.2010;148(5):673–89.
8. MedeirosLJ,Elenitoba-JohnsonKS.Anaplasticlargecell lymphoma.AmJClinPathol.2007;127(5):707–22.
9. FornariA,PivaR,ChiarleR,NoveroD,InghiramiG.Anaplastic largecelllymphoma:oneormoreentitiesamongT-cell lymphoma.HematolOncol.2009;27(4):161–70.
10.TenBergeRL,OudejansJJ,OssenkoppeleGJ,MeijerCJ. ALK-negativesystemicanaplasticlargecelllymphoma: differentialdiagnosticandprognosticaspects–areview.J Pathol.2003;200(1):4–15.
11.SwerdlowSH,CampoE,HarrisNL,JaffeES,PileriSA,SteinH, etal.WorldHealthOrganizationclassification:tumorsof hematopoieticandlymphoidtissues.Lyon:IARCPress;2008.
12.AttygalleAD,KyriakouC,DupuisJ,GroggKL,DissTC, WotherspoonAC,etal.Histologicevolutionof angioimmunoblasticT-celllymphomainconsecutive biopsies:clinicalcorrelationandinsightsintonaturalhistory anddiseaseprogression.AmJSurgPathol.2007;31(7):1077–88.
13.AttygalleAD,ChuangSS,DissTC,DuMQ,IsaacsonPG,Dogan A.DistinguishingangioimmunoblasticT-celllymphoma, unspecified,usingmorphology,immunophenotypeand moleculargenetics.Histopathology.2007;50(4):498–508.
14.KonstantinouK,YamamotoK,IshibashiF,MizoguchiY, KurataM,NakagawaY,etal.Angiogenicmediatorsofthe angiopoietinsystemarehighlyexpressedbyCD10-positive
lymphomacellsinangioimmunoblasticT-celllymphoma.BrJ Haematol.2009;144(5):696–704.
15.NelsonM,HorsmanDE,WeisenburgerDD,GascoyneRD,Dave BJ,LoberizaFR,etal.Cytogeneticabnormalitiesandclinical correlationsinperipheralT-celllymphoma.BrJHaematol. 2008;141(4):461–9.
16.FerreriAJ,GoviS,PileriSA,SavageKJ.Anaplasticlargecell lymphomaALK-positive.CritRevOncolHematol. 2012;83(2):293–302.
17.Gutiérrez-GarcíaG1,García-HerreraA,CardesaT,MartínezA, VillamorN,GhitaG,etal.Comparisonoffourprognostic scoresinperipheralT-celllymphoma.AnnOncol. 2011;22(2):397–404.
18.López-GuillermoA,CidJ,SalarA,LópezA,MontalbánC, CastrilloJM,etal.PeripheralT-celllymphomas:initial features,naturalhistory,andprognosticfactorsinaseriesof 174patientsdiagnosedaccordingtotheREALclassification. AnnOncol.1998;9(8):849–55.
19.GallaminiA,StelitanoC,CalviR,BelleiM,MatteiD,VitoloU, etal.PeripheralT-celllymphomaunspecified(PTCL-U):anew prognosticmodelfromaretrospectivemulticentricclinical study.Blood.2004;103(7):2474–9.
20.WentP,AgostinelliC,GallaminiA,PiccalugaPP,AscaniS, SabattiniE,etal.MarkerexpressioninperipheralT-cell lymphoma:aproposedclinical-pathologicprognosticscore.J ClinOrthod.2006;24(16):2472–9.
21.VoseJ.InternationalperipheralT-celllymphoma(PTCL) clinicalandpathologyreviewproject:pooroutcomeby prognosticindicesandlackofefficacywithanthracyclines. Blood.2005;106.Abstract811a.
22.ArmitageJO.TheaggressiveperipheralT-celllymphomas: 2012updateondiagnosis,riskstratificationand
management.AmJHematol.2012;87(5):511–9.
23.DeardenCE,JohnsonR,PettengellR,DevereuxS,Cwynarski K,WhittakerS,etal.Guidelinesforthemanagementof matureT-cellandNK-cellneoplasms(excludingcutaneous T-celllymphomas).BrJHaematol.2011;153(4):451–85.
24.KarakasT,BergmannL,StutteHJ,JägerE,KnuthA,
WeidmannE,etal.PeripheralT-celllymphomasrespondwell tovincristine,adriamycin,cyclophosphamide,prednisone andetoposide(VACPE)andhaveasimilaroutcomeashigh gradeB-celllymphomas.LeukLymphoma.1996;24(1–2):121–9.
25.SchmitzN,TrümperL,ZiepertM,NickelsenM,HoAD, MetznerB,etal.TreatmentandprognosisofmatureT-cell andNK-celllymphoma:ananalysisofpatientswithT-cell lymphomatreatedinstudiesoftheGermanHigh-Grade Non-Hodgkin’sLymphomaStudyGroup.Blood. 2010;116(18):3418–25.
26.EyreTA,CollinsGP.Currenttreatmentandfutureprospects forperipheralT-celllymphoma.DrugsToday(Barc). 2013;49(10):631–46.
27.YinJ,WeiJ,XuJH,XiaoY,ZhangYC.Autologousstemcell transplantationasthefirstlinetreatmentforperipheral T-celllymphoma:resultsofacomprehensivemeta-analysis. ActaHaematol.2014;131(2):114–25.
28.d’AmoreF,RelanderT,LauritzsenGF,JantunenE,HagbergH, AndersonH,etal.Upfrontautologousstemcell
transplantationinperipheralT-celllymphoma:NGL-T-01.J ClinOrthod.2012;30(25):3093–9.
29.YaredJ,KimballA.Theroleofhighdosechemotherapyand autologousstemcelltransplantationinperipheralT-cell lymphoma:areviewoftheliteratureandnewperspectives. CancerTreatRev.2013;39(1):51–9.
30.SavageKJ.PeripheralT-cellLymphomas.BloodRev. 2007;21(4):201–16.
31.FossFM.TreatmentstrategiesforperipheralT-cell
lymphomas.BestPractResClinHaematol.2013;26(1):43–56.
284
revbrashematolhemoter.2015;37(4):277–284T-celllymphomapatients:evaluationofthelong-term outcome.AnnOncol.2010;21(4):860–3.
33.BergmanAM,PinedoHM,TalianidisI,VeermanG,LovesWJ, vanderWiltCL,etal.Increasedsensivitytogemcitabineof p-glycoproteinandmultidrugresistance-associated protein-overexpressinghumancancercelllines.BrJCancer. 2003;88(12):1963–70.
34.ProB,AdvaniR,BriceP,BartlettNL,RosenblattJD,IllidgeT, etal.Brentuximabvedotin(SGN-35)inpatientswithrelapsed orrefractorysystemicanaplasticlarge-celllymphoma: resultsofaphaseIIstudy.JClinOrthod.2012;30(18):2190–6.
35.FriedbergJ,MahadevanD,JungJ,PerskyD,LossosI,DanaeeH, etal.PhaseIItrialofalisertib(MLN8237),aninvestigational, potentinhibitorofauroraAkinase(AAK),inpatientswith aggressiveB-andT-cellnon-Hodgkinlymphoma.In:ASH AnnualMeetingAbstracts,vol.118.2011.p.95.
36.DeardenCE.Roleofsingleagentanaloguesintherapyof peripheralT-celllymphomas.SeminHematol.2006;432 Suppl.2:S22–6.
37.O’ConnorOA,ProB,Pinter-BrownL,BartlettN,PopplewellL, CoiffierB,etal.Pralatrexateinpatientswithrelapsedor refractoryperipheralT-celllymphoma:resultsfromthe pivotalPROPELstudy.JClinOrthod.2011;29(9): 1182–9.
38.MarchiE,BongeroDC,KalacM,ScottoL,O’ConnorOA.The combinationofhistonedeacetylaseinhibitorsand hypomethylatingagentsexhibitsmarkedsynergyin preclinicalmodelsofT-celllymphomas.Blood(ASHAnnu MeetAbstract).2013;116(21):3937.
39.PierkarzR,WrightJ,FryeR,AllenSL,JoskeD,KirschbaumM, etal.Finalresultsofaphase2NCImulticenterstudyof romidepsininpatientswithrelapsedperipheralT-cell lymphoma(PTCL).Blood(ASHAnnuMeetAbstr). 2009;114(22):1657.