rev bras hematol hemoter. 2016;38(3):190–192
w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Scientific
Comment
Comments
on:
“Clinical,
hematological
and
genetic
data
of
a
cohort
of
children
with
hemoglobin
SD”
夽
Maria
Stella
Figueiredo
∗UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
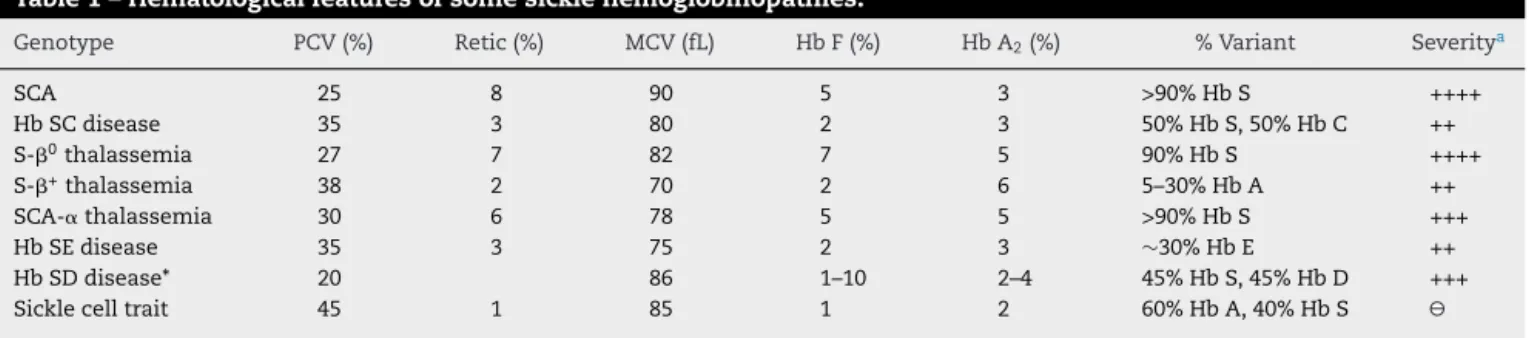
Sickle cell disease (SCD) is a group of genetic conditions relatedtothepresenceofasicklehemoglobin(HbS) muta-tion(HBB:c.20A>T).PeoplewithSCDcanbehomozygousfor Hb S or can havecompound heterozygosity for Hb S with othergenemutations.1,2SomehematologicfeaturesofSCD arelisted inTable1, butraregenotypes canalsobefound. SincetheconcentrationofHbSisapathophysiologicalfactor ofdisease severity,thepresenceoflower concentrationsof HbSduetodoubleheterozygositycandeterminephenotypic heterogeneity.1,3 However,other geneticand environmental factorscanalsohaveaneffectonthediseasephenotype.4
Studies looking for abnormal hemoglobins (Hbs) in the Brazilianpopulationhavebeenperformedsincethe1950s.5–8 However, the Brazilian Government Directive MS # 822/01 that regulates newborn screening for hemoglobinopathies, haspromotedanincreaseofdataabouthemoglobinopathies indifferentBrazilianregions.9–11Thisassociatedwiththeuse ofisoelectricfocusingelectrophoresis(IEF)andhigh-pressure liquid chromatography (HPLC) as diagnostic methods, has enabledtheidentificationofanincreasingnumberof abnor-malHbsaswellascompoundheterozygousstatesofHbS.12–14 AnexampleisapaperpublishedinthisissueoftheRevista BrasileiradeHematologiaeHemoterapiathatshowsdataon acohortofchildrenwithhemoglobinSDpattern.15
Hb D is an abnormal Hb, which migrates to the same
positionasHbSinelectrophoresisatalkalinepH,andcan beseparated fromHb S inacidpH.16–18 SeveralHb D have been described in different racial groups, but the majority presented a point mutation in codon 121 of the -globin gene,whichresultsinthesubstitutionofglutamicacid for
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.bjhh.2016.05.002.
夽
SeepaperbyRezendeetal.onpages240–6.
∗ Correspondingauthorat:DepartamentodeOncologiaClínicaeExperimental,DisciplinadeHematologiaeHemoterapia,Universidade
FederaldeSãoPaulo(UNIFESP),RuaDrDiogodeFaria,824,3◦andar,VilaClementino,04037-002SãoPaulo,SP,Brazil. E-mailaddress:[email protected]
glutamine(HBB:c.364G>C).ThisabnormalHbisusuallycalled Hb D-Punjab or Hb D-Los Angeles, howeverit can alsobe namedHbD-NorthCarolina,HbD-Chicago,HbD-Portugal,Hb D-Cyprus,andHbD-OakRidge.19–21Theestimatedprevalence ofHbD-Punjabis0.1to0.4%inAfrican-Americans.22InBrazil, astudyofAfricandescendantsshowedasimilarprevalence.5 SometimeafterthediscoveryofHbD-Punjab,the coinher-itanceofHbD-PunjabandHbSwasidentifiedinCaucasian patientswithclinicalandhematologicalmanifestations simi-lartothoseofsicklecellanemia(SCA),becausethismutation facilitatesHb Spolymerization.23–25 Furtherclinical studies confirmedthe severityofthemanifestationsofthis associ-ationandtheneedtotreattheseindividualsasSCApatients byprescribinghydroxyureawhenindicated.21,26–29
ThereareothertypesofHbDduetodifferentpoint muta-tionsinthe-globingene,suchasHbD-Iran(HBB:c.67G>C) andHbD-Ibadan(HBB:c.263C>A).However,individualswith thesemutationshavenormalhematologicvaluesanddonot sufferfromvaso-occlusivecomplications,sincetheirredcells donotsickleunderphysiologicconditions.18,30,31
HbKorle-Bu(HbKB)orHbG-Accra(HBB:c.220G>A)isa fre-quentmutationinSub-SaharanAfrica.32,33 ThisHbhasthe same IEFmobilityasHbD-Punjabbutcanbedifferentiated byHPLC.HeterozygotesforHbKBhavenohematologic alter-ations,andindividualswithdoubleheterozygosisHbS-HbKB havenormalredcellsonbloodsmearandabenignclinical course,similartosicklecelltraitasHbKBdoesnotparticipate inthegelationofHbS.33,34
Interestingly,the HbKBmutation[beta73(E17)Asp→Asn] canoccurinadditiontotheHbSmutation[beta6(A3)Glu6Val]
http://dx.doi.org/10.1016/j.bjhh.2016.05.012
revbrashematolhemoter.2016;38(3):190–192
191
Table1–Hematologicalfeaturesofsomesicklehemoglobinopathies.
Genotype PCV(%) Retic(%) MCV(fL) HbF(%) HbA2(%) %Variant Severitya
SCA 25 8 90 5 3 >90%HbS ++++
HbSCdisease 35 3 80 2 3 50%HbS,50%HbC ++
S-0thalassemia 27 7 82 7 5 90%HbS ++++
S-+thalassemia 38 2 70 2 6 5–30%HbA ++
SCA-␣thalassemia 30 6 78 5 5 >90%HbS +++
HbSEdisease 35 3 75 2 3 ∼30%HbE ++
HbSDdisease* 20 86 1–10 2–4 45%HbS,45%HbD +++
Sicklecelltrait 45 1 85 1 2 60%HbA,40%HbS
SCA:sicklecellanemia;PCV:packedcellvolume;Retic:reticulocytecount;MCV:meancellvolume;Hb:Hemoglobin.
a Severityofdiseaseratedfrommostsevere(++++)toabsenceofclinicalevents( )includescomplicationsrelatedtosicklevaso-occlusionand
hemolysis.
Tablemodifiedfrom1with*dataobtainedfrom21,27,32.
inthesamebetaglobinchain.Inthiscase,thisHbwitha dou-blemutationistermedHbC-Harlem(orHb C-Georgetown) (HBB:c.20A>T,HBB:c.220G>A),becauseitmigratestothe posi-tionofHbCincelluloseacetateelectrophoresisatalkalinepH. IndividualsheterozygousforHbC-Harlemareasymptomatic, butthecoinheritanceofHbSandHbC-Harlemhasclinical manifestationssimilartoSCA.20,32,35
ResearchersfromIndiaandtheMiddleEastarethemain authorsofthefewpapersaboutHbSD-Punjab;thereareless datapublishedabouttheassociationHbS-HbKB.21,27–29,34,36–41 BystudyingtwodifferentgroupsofpatientswithHbSD pat-terns,specificallyHbSD-PunjabandHbS-HbKB,Rezendeetal. notonlypublishedimportantclinicaldataaboutthe coinher-itanceoftworareHbbutalsopointedouttheimportanceof thisdifferentialdiagnosis.15
Conflicts
of
interest
Theauthordeclaresnoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. SteinbergMH.Sicklecellanemia,thefirstmoleculardisease: overviewofmolecularetiology,pathophysiology,and therapeuticapproaches.SciWorldJ.2008;8:1295–324.
2. SteinbergMH,SebastianiP.Geneticmodifiersofsicklecell disease.AmJHematol.2012;87(8):795–803.
3. SteinbergMH.Geneticetiologiesforphenotypicdiversityin sicklecellanemia.SciWorldJ.2009;9:46–67.
4. SerjeantGR.Thenaturalhistoryofsicklecelldisease.Cold SpringHarbPerspectMed.2013;3(10):a011783.
5. TondoCV,SalzanoFM.AbnormalhemoglobinsinaBrazilian Negropopulation.AmJHumGenet.1962;14:401–9.
6. SalzanoFM,TondoCV.HemoglobintypesinBrazilian populations.Hemoglobin.1982;6(1):85–97.
7. ZagoMA,CostaFF.Hereditaryhaemoglobindisordersin Brazil.TransRSocTropMedHyg.1985;79(3):385–8.
8. ZagoMA.Hemoglobinopathies:prevalenceandvariability. RevPaulMed.1986;104(6):300–4.
9. PaixaoMC,CunhaFerrazMH,JanuarioJN,VianaMB,LimaJM. ReliabilityofisoelectrofocusingforthedetectionofHbS,Hb C,andHBDinapioneeringpopulation-basedprogramof newbornscreeninginBrazil.Hemoglobin.2001;25(3):297–303.
10.RamalhoAS,MagnaLA,dePaiva-e-SilvaRB.Government DirectiveMS#822/01:uniqueaspectsofhemoglobinopathies forpublichealthinBrazil.CadSaudePublica.
2003;19(4):1195–9.
11.LoboCL,BallasSK,DomingosAC,MouraPG,doNascimento EM,CardosoGP,etal.Newbornscreeningprogramfor hemoglobinopathiesinRiodeJaneiro,Brazil.PediatrBlood Cancer.2014;61(1):34–9.
12.SilvaMR,SendinSM,PimentelFS,Velloso-RodriguesC, RomanhaAJ,VianaMB.HbStanleyville-II
[alpha78(EF7)Asn→Lys(alpha2);HbA2:c.237C>A]:incidence
of1:11,500inanewbornscreeningprograminBrazil. Hemoglobin.2012;36(4):388–94.
13.SilvaMR,SendinSM,AraujoIC,PimentelFS,VianaMB. Clinicalandmolecularcharacterizationofhemoglobin Maputo[beta47(CD6)Asp>TyrHBB:c.142G>T]andG-Ferrara [beta57(E1)Asn>LysHBB:c.174C>A]inanewbornscreening inBrazil.IntJLabHematol.2013;35(6):e1–4.
14.BelisarioAR,SalesRR,SilvaCM,Velloso-RodriguesC,Viana MB.ThenaturalhistoryofHbS/hereditarypersistenceof fetalhemoglobinin13childrenfromthestateofMinas Gerais,Brazil.Hemoglobin.2016;40(3):215–9.
15.RezendePV,CostaKS,DominguesJuniorJC,SilveiraPB, BelisarioAR,SilvaCM,etal.Clinical,hematologicaland geneticdatainacohortofchildrenwiththehemoglobinSD pattern.RevBrasHematolHemoter.2016;38(3):240–6.
16.ItanoHA.Athirdabnormalhemoglobinassociatedwith hereditaryhemolyticanemia.ProcNatlAcadSciUSA. 1951;37(12):775–84.
17.LehmannH.ThreevarietiesofhumanhaemoglobinD. Nature.1958;182(4639):852–4.
18.TorresLdeS,OkumuraJV,SilvaDG,Bonini-DomingosCR. HemoglobinD-Punjab:origin,distributionandlaboratory diagnosis.RevBrasHematolHemoter.2015;37(2):120–6.
19.BaglioniC.Abnormalhumanhaemoglobins.VII.Chemical studiesonhaemoglobinD.BiochimBiophysActa. 1962;59:437–49.
20.KinneyTR,WareRE.Compoundheterozygousstates.In: EmburySH,HebbelRP,MohandasN,SteinbergMH,editors. SicklecelldiseaseBasicprinciplesandclinicalpractice.1st ed.NewYork:RavenPress;1994.p.437–51.
21.ItaliaK,UpadhyeD,DabkeP,KanganeH,ColacoS,SawantP, etal.ClinicalandhematologicalpresentationamongIndian patientswithcommonhemoglobinvariants.ClinChimActa. 2014;431:46–51.
22.ChernoffAI.OntheprevalenceofhemoglobinDinthe AmericanNegro.Blood.1956;11(10):907–9.
192
revbrashematolhemoter.2016;38(3):190–19224.AdachiK,KimJ,BallasS,SurreyS,AsakuraT.Facilitationof HbSpolymerizationbythesubstitutionofGluforGlnatbeta 121.JBiolChem.1988;263(12):5607–10.
25.SteinbergMH.Compoundheterozygousandothersickle hemoglobinopathies.In:SteinbergMH,ForgetBG,HiggsDR, NagelRL,editors.Disordersofhemoglobingenetics, pathophysiology,andclinicalmanagement.1sted. Cambridge:CambridgeUniversityPress;2001.p.786–810.
26.VillanuevaH,KurilS,KrajewskiJ,SedrakA.Pulmonary thromboembolisminachildwithsicklecellhemoglobinD diseaseinthesettingofacutechestsyndrome.CaseRep Pediatr.2013;2013:875683.
27.OberoiS,DasR,TrehanA,AhluwaliaJ,BansalD,MalhotraP, etal.HbSD-Punjab:clinicalandhematologicalprofileofa rarehemoglobinopathy.JPediatrHematolOncol.
2014;36(3):e140–4.
28.PatelS,PurohitP,MashonRS,DehuryS,MeherS,SahooS, etal.Theeffectofhydroxyureaoncompoundheterozygotes forsicklecell-hemoglobinD-Punjab–asinglecentre experienceineasternIndia.PediatrBloodCancer. 2014;61(8):1341–6.
29.IyerS,SakhareS,SenguptaC,VelumaniA.
HemoglobinopathyinIndia.ClinChimActa.2015;444:229–33.
30.SerjeantB,MyerscoughE,SerjeantGR,HiggsDR,Moo-Penn WF.Sicklecell-hemoglobinDIran:benignsicklecell syndrome.Hemoglobin.1982;6(1):57–9.
31.Watson-WilliamsEJ,BealeD,IrvineD,LehmannH.Anew haemoglobin,DIbadan(Beta-87Threonine–Lysine), producingnosickle-cellhaemoglobinDdiseasewith haemoglobinS.Nature.1965;205:1273–6.
32.RandolphTR.Hemoglobinopathies(structuraldefectsin hemoglobin).In:KeohaneE,SmithS,WalengaJ,editors.
Rodak’shematology:clinicalprinciplesandapplications.5th ed.StLouis:Elsevier;2016.p.426–53.
33.RoperoP,VillegasA,GonzalezFA.HemoglobinKorle-Bu [beta73(E17)Asp→Asn].FirstcasesdescribedinSpain.Med
Clin.2004;123(7):260–1.
34.AklPS,KutlarF,PatelN,SalisburyCL,LaneP,YoungAN. CompoundheterozygosityforhemoglobinS
[beta6(A3)Glu6Val]andhemoglobinKorle-Bu [beta73(E17)Asp73Asn].LabHematol.2009;15(3):20–4.
35.SteinbergMH,ChuiDH.HbCdisorders.Blood. 2013;122(22):3698.
36.MondalSK,MandalS.Prevalenceofthalassemiaand hemoglobinopathyineasternIndia:a10-year
high-performanceliquidchromatographystudyof119,336 cases.AsianJTransfusSci.2016;10(1):105–10.
37.JiskootPM,HalseyC,RiversR,BainBJ,WilkinsBS.Unusual splenicsinusoidalironoverloadinsicklecell/haemoglobin D-Punjabdisease.JClinPathol.2004;57(5):539–40.
38.RahimiZ.Geneticepidemiology,hematologicalandclinical featuresofhemoglobinopathiesinIran.BiomedResInt. 2013;2013:803487.
39.WajcmanH,MoradkhaniK.Abnormalhaemoglobins: detectionandcharacterization.IndianJMedRes. 2011;134:538–46.
40.AdekileA,Mullah-AliA,AkarNA.Doeselevatedhemoglobin FmodulatethephenotypeinHbSD-LosAngeles?Acta Haematol.2010;123(3):135–9.