Iron status predicts treatment failure and mortality in tuberculosis patients: a prospective cohort study from Dar es Salaam, Tanzania.
Texto
Imagem
Documentos relacionados
Considerando o passado recente da restrição ao tabagismo em Portugal (2008) e dado que a FPCE-UP foi considerada livre de fumo dois anos antes, foram propostos os seguintes
Taking into account these considerations, in this study we evaluated the repercussions of iron supplementation and restriction, as well as iron restriction followed by an
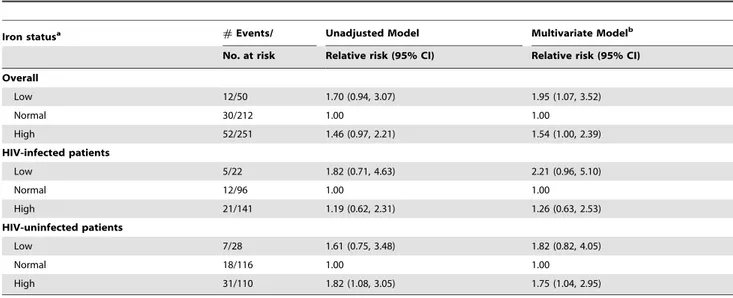
Conclusion: In this population, iron metabolism alterations were associated with a higher rate of adverse events and higher ferritin levels constituted an independent
Although we could only perform subgroup meta-analysis of serum ferritin and hair iron levels but not peripheral serum iron or serum transferrin levels because of an insufficient
In relation to iron nutriture, an increase in the cellular iron stocks through administration of iron- dextran led to higher mortality in mice infected with
Iron plays an important role in the pathology of several diseases. In previous studies we showed that higher iron levels in hosts were related to higher parasitemia and mortality.
(12) studied disacchari- dase levels and cell proliferation in the small intestine of rats with iron-deficiency anemia and observed that the animals fed an iron- deficient
Hereditary hemochromatosis is a disorder of iron metabolism charac- terized by increased iron intake and progressive storage and is related to mutations in the HFE gene..
