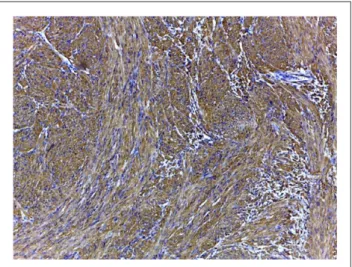
Fibrosarcoma of the urinary bladder in a cat
Texto
Imagem

Documentos relacionados
Na interface do WebGlobulus não há possiblidade de calcular o valor do Site Index de cada parcela de amostragem ou até mesmo outras parcelas em qualquer zona
O âmbito de actuação do Conselho Superior do Ministério Público, perante esta estrutura organizativa, está limitado, pelas próprias competências do Procurador-Geral da
The objective of this work is to evaluate the simulation of the time course of soil temperature through daily and annual cycles in two types of soil at six depths 2, 4, 6, 8, 16 and
However the magnitude and variability observed in the three curves (average and the seasonal values) of the absorption coefficient are significantly different if summer and
OnabotulinumtoxinA 100 U signi fi cantly improves all idiopathic overactive bladder symptoms and quality of life in patients with overactive bladder and urinary incontinence:
In the case of transurethral resections of the urinary bladder, no significant difference (p = 0.238) was found in the average postopera- tive length of stay of patients who were
Aim: To investigate the histopathologic changes in native bladder and gastrointesti- nal segment, the relation between histopathologic changes, type of operation and the period
The study evaluated 79 consecutive female patients with lower urinary tract symptoms (LUTS), including signs of overactive bladder syndrome (OAB), stress (SUI) and mixed
