www.jped.com.br
REVIEW
ARTICLE
Update
on
diagnosis
and
management
of
childhood
epilepsies
夽
Sameer
M.
Zuberi
∗,
Joseph
D.
Symonds
PediatricNeurosciencesResearchGroup,FraserofAllanderNeurosciencesUnit,RoyalHospitalforSickChildren,Glasgow, UnitedKingdom
Received6July2015;accepted7July2015 Availableonline4September2015
KEYWORDS
Epilepsy; Epilepsies; Diagnosis; Management; Child
Abstract
Objectives: To reviewthe currentevidence basefor the diagnosis andmanagementofthe childhoodepilepsiesandtodrawattentiontothecurrentgapsinthisevidencebase.Thefocus willbeontherapeuticaspects.CurrentInternationalLeagueAgainstEpilepsy(ILAE) terminol-ogy willbedescribedandusedthroughoutthediscussion.Thereviewwilldrawattentionto recentadvancesthathavebeenmadeinbothourunderstandingandtreatmentofthechildhood epilepsies.Potentialfuturedirectionsforresearchandtreatmentoptionswillbediscussed.
Sources: OriginalarticlesrelevanttothesubjectwereobtainedfromtheMedLinedatabase usingpertinentMeSHterms.Relevantpaperswerereadandassimilated.Citationsearchingwas used.
Summaryofthefindings: Epilepsyisamajorcauseofglobaldiseaseburden.Childhood epilep-sies are aheterogeneous group of conditions. A multi-axial diagnosticapproach shouldbe taken prior tomakingtreatment andmanagementdecisionsfor anyindividualpatient. For themajorityofpatients,successfulcontrolofseizurescanbeachievedwithasingle medica-tion.However,asignificantminoritydevelopsrefractorydisease.Epilepsysurgerycanprovide cureforacarefullyselectedgroupofthesecases.
Conclusions: Thereremainsignificantgapstheevidencebasefortreatmentinseveralareasof childhoodepilepsy.Concertedmulti-centereffortsshouldbemadetotrytoclosethesegaps. A personalizedmedicineapproachmay helptoreduce theproportion ofrefractorycasesof childhoodepilepsyinfuture.
©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:ZuberiSM,SymondsJD. Updateondiagnosisandmanagementofchildhoodepilepsies.JPediatr (RioJ). 2015;91:S67---77.
∗Correspondingauthor.
E-mail:[email protected](S.M.Zuberi).
http://dx.doi.org/10.1016/j.jped.2015.07.003
PALAVRAS-CHAVE
Epilepsia; Epilepsias; Diagnóstico; Tratamento; Infância
Atualizac¸ãosobreodiagnósticoetratamentodeepilepsiasdainfância
Resumo
Objetivos: Analisar abasede evidências atualpara odiagnóstico e tratamentodas epilep-sias da infância e chamar a atenc¸ão para as lacunas atuais nessa base de evidências. O foco será os aspectos terapêuticos. A terminologia atual da Liga Internacional contra a Epilepsia (ILAE) será descrita e utilizada na discussão. A análise chamará a atenc¸ão para os recentes avanc¸os em nosso entendimento e no tratamento das epilepsias da infância. Serão discutidas possíveis orientac¸ões futuras para as opc¸ões de pesquisa e tratamento.
Fontesdedados: Trabalhosoriginaisrelevantesparaoassuntoforamobtidosdabasededados MedLineusandotermosrelevantesdoMeSH.Ostrabalhosrelevantesforamlidoseassimilados. Foiusadapesquisadecitac¸ões.
Resumodosdados: Aepilepsiaéumadasmaiorescausasdacargaglobaldedoenc¸as.As epilep-siasdainfância representamumgrupoheterogêneodedoenc¸as.Umaabordagemmultiaxial dodiagnóstico deve serrealizada antesda tomadadedecisões detratamentode qualquer paciente individual.Namaioriados pacientes,ocontrolebem-sucedidodas crisespodeser obtido com uma única medicac¸ão. Contudo, uma minoria significativa desenvolve doenc¸a refratária.A cirurgia deepilepsiapode curarum grupocuidadosamenteselecionado desses casos.
Conclusões: Aindaexistemlacunassignificativasnabasedeevidênciasdetratamentoem diver-sasáreasdeepilepsiadainfância.Devemserenvidadosesforc¸osmulticêntricosconcertados paratentarfecharessaslacunas.Umaabordagemmédicapersonalizadapodeajudarareduzir aproporc¸ãodecasosrefratáriosdeepilepsiadainfâncianofuturo.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Epidemiology
Epilepsy is the most prevalent chronic neurological dis-ease in the world, with an estimated 65 million people affected.1 Severe epilepsy ranks as the fourth largest causeofglobaldiseaseburden.2Crudeincidenceestimates for epilepsy vary from 15 to 113 per 100,000 per year, depending on the population studied.3 The incidence of epilepsyin childhoodis morethantwicethat intheadult population.4
Definitions
Epilepsy has been conceptually defined as a disorder of the brain characterized by an enduring predisposition to generateepileptic seizures.Anepileptic seizureisa tran-sientoccurrenceofsignsand/orsymptomsduetoabnormal excessive or synchronous neuronal activity in the brain.5 To facilitate the practical application of epilepsy as a diagnosticterm,theInternational LeagueAgainstEpilepsy (ILAE)finalizedanoperationaldefinitionofepilepsyin2014 (Table 1).6 It is perhaps most helpful to conceptualize epilepsynotasasinglecondition,butasagroupof condi-tions,‘‘theepilepsies’’,reflectingtherecognitionthatthe underlyingcausesofepilepticseizuresarebothvariedand numerous,andthattheclinicalmanifestationsofabnormal
Table1 InternationalLeagueAgainstEpilepsyoperational
definitionofepilepsy2014.6
Adiseaseofthebraindefinedbyanyofthefollowing conditions
1.Atleasttwounprovoked(orreflex)seizuresoccurring >24hapart
2.Oneunprovoked(orreflex)seizureandaprobabilityof furtherseizuressimilartothegeneralrecurrencerisk(at least60%)aftertwounprovokedseizures,occurringover thenext10years
3.Diagnosisofanepilepsysyndrome
excessive or synchronous neuronal activity are heteroge-neous.
Diagnosis
When considering a diagnosis of epilepsy, a multi-axial approachis recommended.7 The following axes shouldbe considered:
1. Isthediagnosisepilepsy? 2. Whataretheseizuretypes?
3. Canthediagnosisofanestablishedepilepsysyndromebe made?
Establishingwhetherthediagnosisisepilepsyor not
Accuracy of diagnosis is paramount, since a diagnosis of epilepsycanhavesignificantimplicationsforpatients,their families, and therapeutic management. However, making a diagnosis of epilepsy can be challenging, since there areanumberof paroxysmalconditionsfor whichthe clin-ical history may resemble that of an epileptic seizure, and because there is no definitive diagnostic investiga-tionfor thiscondition.Misdiagnosis ratesin epilepsyhave traditionally beenhigh. Of233 childrenreferred toa ter-tiaryepilepsycenter inDenmark, 87(39%) werefoundby expert assessment not to have epilepsy, and of these 35 (40%)hadbeenstartedonanti-epilepticdrugs(AEDs).8The mostfrequentlyobserveddifferentialdiagnoseswere non-epileptic staring spells(52.8%), psychogenic non-epileptic seizures(10.3%),syncope(3.4%),dystonia(3.4%),and para-somnias(3.4%).Misdiagnosis ofnon-epileptic events when thetrue diagnosis isepilepsyappearstobeless common. In aDutch study that included 888 children referredto a tertiarycenterwithparoxysmalevents,19/124(5.6%) chil-dren whohadbeen referred withmultiple unclearevents were given a diagnosis of epilepsy.9 Initial assessment by a practitioner with expertise and experience in epilepsy diagnosis is thought to significantly reduce misdiagnosis rates.
In many cases, the diagnosis of an epileptic or non-epilepticeventcanbebasedonanaccuratedescriptionof theepisodeorepisodesbythepatientandwitnesses,with nofurtherinvestigationsnecessary.Thewidespreaduseof smartphoneshasgreatlyfacilitatedthediagnosisof parox-ysmalevents.Wheneventsarerecurrentandthereisdoubt abouttheirnature,parentsshouldbestronglyencouraged tocapturethemonvideo.TheILAEhasbuiltupanexcellent onlineresource10whereclinicianscanviewvideoexamples ofepilepticandnon-epilepticevents.
Syncopaleventscanoftenbedifferentiatedfrom epilep-tic seizures by the patient’s description of howthey felt beforethecollapse.Typicalprodromalsymptomsofsyncope aredizziness,visualloss,nausea,sweating,andtinnitus.In allcasesorcollapse,itisadvisableofobtaina12-lead elec-trocardiogram,withparticularattentiontomeasurementof the corrected QT interval, sincecardiac arrhythmia is an importantdifferential.11
Descriptionofseizuretypes
Onceacleardescriptionoftheevent(s)hasbeenobtained, iftheyarethoughttobeepileptic,theclinicianshouldtry toclassifythe seizuretype(s).Table 2details thecurrent ILAEclassificationofseizuretypes.Generalizedseizuresare conceptualized asbeginning within,and rapidlyengaging bilateralnetworkswithinthebrain,whereasfocalseizures originatewithinnetworkslimitedtoonehemisphere.Focal seizuresmayprogresstoengagebothhemispheres,resulting in bilateral convulsive features. An electroencephalogram (EEG)isausefuladjuncttoseizuretypeclassification, par-ticularly in focal epilepsies for which focal epileptiform activitymayhelpidentifyalobarlocation.
Syndromeclassification
By analyzing the clinical details of a patient’s epilepsy, includingseizuretypes,ageofonset,andassociated comor-bidities,itmaybepossibletodiagnoseaspecific epilepsy syndrome.Manyepilepsysyndromesareassociatedwith par-ticularfindingsonEEG,thereforethisinvestigationcanbe veryhelpful inassisting syndromeclassification.Achieving a syndromic diagnosis is important, since it may inform therapeuticdecisions,furtherinvestigations,andprognosis. TheILAEwebsiteprovidesclinical andEEGfeatures of31 epilepsysyndromes.10Estimatesfortheproportionof child-hoodepilepsycasesthatcanbediagnosedwithanepilepsy syndromehaverangedbetween15.7%and37.1%,depending onthepopulationincluded.12---14Themostprevalentepilepsy syndromes of childhood appear to be benign epilepsy of childhoodwithcentro-temporalspikes(BCECTS),childhood absence epilepsy (CAE), juvenile absence epilepsy (JAE), juvenilemyoclonicepilepsy(JME),andWestsyndrome(WS). Manyoftheepilepsiesthatdonotconformtoasyndromic diagnosiscanstillbedescribedintermsofseizuretypesand etiology(Table3).
Etiology
In most epilepsies, investigation for an underlying eti-ology is warranted, regardless as to whether or not an epilepsy syndrome diagnosis has been made. The excep-tions to this rule aretypical cases of BCECTS, CAE, JAE, and JME. Although these epilepsies all have a principally geneticetiology,geneticinvestigationisnotcurrently clini-callyusefulsincemultiplesusceptibilitygenesareinvolved and there is no established correlation between genetic findingsandeither prognosis or therapeuticmanagement. These same syndromes are very rarely associated with structuralbrainabnormalities, soneuroimagingis alsonot necessary.15 In allothercasesofchildhood-onsetepilepsy, including atypical cases of the above-listed syndromes, neuroimaging is indicated. The purpose of neuroimaging is to identify any causative structural brain lesion. Some lesions,suchasneoplasms,mayrequireimmediate mana-gement, whilst others, such as focal cortical dysplasia, may prove to be surgically remediable targets further down the line. Abnormal neuroimaging is found in 50% of newchildhood-onset epilepsy in which there arefocal seizures, and in 15---20% of cases imaging studies provide usefulinformationonetiologyand/orseizurefocus.16 Mag-netic resonance imaging (MRI) is the imaging modality of choice.
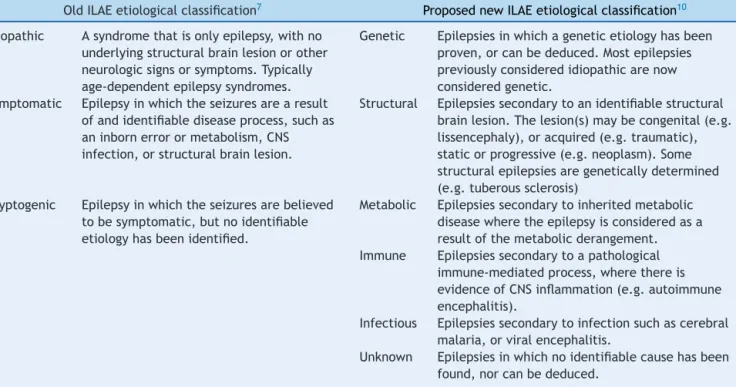
Thefirstsignificantattemptatreclassifyingthe epilep-siesinline withmodernunderstandingof thediseaseand itsmechanismswasmadebytheILAEin2010.Theprincipal changestoofficialILAEnomenclaturefocusedonetiological categorization.The terms ‘‘idiopathic,’’‘‘symptomatic,’’ and ‘‘cryptogenic’’ were replaced by the more precise terms ‘‘genetic,’’ ‘‘structural,’’ and ‘‘metabolic.’’ The inclusionof furtheretiological categories ‘‘immune’’ and ‘‘infectious’’iscurrentlyunderdiscussion(Table4).
Table2 InternationalLeagueAgainstEpilepsyclassificationofseizuretypes.
Generalizedseizures
Generalizedtonic---clonic Bilaterallyincreasedtone,followedbysustainedbilateralrhythmiclimbjerking. Clonic Sustainedbilateralrhythmicjerking.
Absence
Typicalabsence Abruptonsetofalteredawareness.Memoryofeventsusuallyimpaired.Oraland manualautomatismsarecommon.Clonicmovementsofpartsofthefacemayoccur. Atypicalabsence Lessabruptonsetandoffsetthantypicalabsence.Maybeassociatedwithlossof
muscletone,orsubtlemyoclonicjerks.Oftenlongerthantypicalabsences.Alteration inawarenessvariable.
Myoclonicabsence Rhythmicmyoclonicjerksoftheshouldersandarmswithtonicabduction,resultingin progressiveliftingofthearmsduringtheseizure.Themyoclonicjerksaretypically bilateral,butmaybeunilateralorasymmetric.Last10---60s.Alterationinawareness variable.
Absencewitheyelidmyoclonia Absenceseizuresaccompaniedbybrief,repetitive,oftenrhythmic,fastmyoclonicjerks oftheeyelids,withsimultaneousupwarddeviationoftheeyeballsandextensionofthe head.Seizuresaretypicallyverybrief(<6sinduration)andmultipleseizuresoccurona dailybasis.Mostlyawarenessisretained.
Tonic Bilaterallyincreasedtoneofthelimbslastingsecondstoaminute.Oftenoccuroutof sleepandinrunsofvaryingintensity.Theindividualisunawareduringtheseevents. Individualsmaymakeanexpiratorysoundatonset.Maycausedropattacks. Atonic Suddenlossordiminutionofmuscletonewithoutapparentprecedingmyoclonicor
tonicfeatures.Verybrief(<2s)andmayinvolvethehead,trunk,orlimbs.
Myoclonic
Myoclonic Singleorseriesofjerks(briefmusclecontractions).Eachjerkistypicallymilliseconds induration.
Negativemyoclonus Briefcessationofbackgroundmuscletone,lastinglessthan500ms.Theresulting movementproducedcanhavetwocomponents,aninitiallossofposturecausedbythe negativemyoclonus,andasubsequentvoluntary,compensatorymovementtorestore posture.Mayoccurinisolationorinaseries.
Myoclonic---atonic Myoclonicseizurefollowedbyanatonicseizure.Sometimesaseriesofmyoclonicjerks occurspriortotheatonia.Theheadandlimbsareaffected,typicallyresultinginrapid fall.
Myoclonic---tonic Myoclonicseizurefollowedbyatonicseizure.Sometimesaclusterofmyoclonicjerks occurspriortotheincreasedtone.
Focalseizures:canbeclassifiedbyfeatures,and/orlaterality,and/orlobarlocalization
Byfeatures(clinical):oneormoretypeoffeaturemaybepresentduringanysinglefocalseizure
Aura Aurasaresubjectiveandmaybesensoryorexperiential.Asensoryaurainvolvesa sensationwithoutanobjectiveclinicalsign,whichmaybevisual,auditory,olfactory, epigastric,etc.Anexperientialaurainvolvesaffective,mnemonic,orperceptual subjectivephenomena,includingdepersonalizationandhallucinatoryevents. Motor Amotorfeatureinvolvesmotoractivityandmayconsistofanincrease(positive)or
decrease(negative)inmusclecontraction.
Autonomic Characterizedbyautonomicphenomena,whichcaninvolvecardiovascular, gastrointestinal,vasomotor,andthermoregulatoryfunctions.Examplesinclude palpitations,nausea,butterflies,hunger,chestpain,urgetourinateordefecate, goosebumps,sexualsensation,feelinghotorcold,piloerection,pallor,tachycardiaor bradycardia/asystole,flushing,pupillarychanges,andlacrimation.
Dyscognitive Involvesalteredawarenessorresponsiveness.
Byhemisphericlocalization(clinicalorelectrophysiological)
Right Indicationsofhemisphericlocalizationmaybesubtle,particularlyinseizuresthat rapidlyengagebilateralnetworks.Headturning,eyedeviation,andunilateralclonic movementsalllateralizetothecontralateralhemisphere.
Left
Bylobarlocalization(clinicalorelectrophysiological)
Table2 (Continued)
Temporal Characterizedbybehavioralarrestanddyscognitivefeatures.Automatismsandauras arecommon.
Parietal Ictalfeaturesareoftensubjective,andincludepositiveand/ornegativesensory featuressuchasparesthesia,disorientation,andcomplexvisualhallucinations. Occipital Characterizedbyvisualaura,typicallymulti-coloredshapes.
EpilepticSpasms
Suddenflexion,extensionormixedflexion-extensionofproximalandtruncalmuscles,lasting1---2s,i.e.,longerthana myoclonicjerk(whichlastsmilliseconds)butnotaslongasatonicseizure(whichlasts>2s).Spasmstypicallyoccurina series,usuallyonwakening.Subtleformsmayoccurwithonlychinmovement,grimacing,orheadnodding.Spasmsmaybe bilaterallysymmetric,asymmetric,orunilateral.
casesremainofunknowncause.17Increasesinthesensitivity andavailabilityofgenetic,biochemical,andneuroimaging testingwillresultinafallintheproportionofunknown eti-ologycasesinfuture.14Thegeneticcausesofbothmetabolic andstructuralepilepsiesarebeingincreasinglyunderstood, sotheboundariesbetweenthesecategoriesarebecoming progressively blurred. In the future, the term ‘‘genetic’’ maywellbecomeoutdated,tobereplacedbymoreprecise terminology.
Forchildreninwhomepilepsypresentsat ayoung age, orisassociatedwithdevelopmentalregressionor develop-mentalimpairment,ifnodefinitiveetiologicaldiagnosishas been madethroughneuroimaging, itisreasonable to con-sider investigation for an underlying geneticor metabolic cause.The approachto suchinvestigation willdepend on
the following: the nature of the patient’s epilepsy and associatedcomorbidities;thepopulationbackgroundofthe patientand the prevalence of specific genetic/metabolic conditions within that population; and the availability of specificdiagnostictesting locally or regionally.Identifying ametabolicetiology may havesignificant implications for treatmentapproach.
Comorbidities
The most commonly observed comorbidities in childhood epilepsyaredevelopmentalimpairments, learning disabil-ities, autism spectrum disorders (ASD), attention deficit hyperactivity disorder (ADHD), and behavioral problems.
Table3 Mostfrequentlyencounteredchildhoodepilepsysyndromes.
Epilepsysyndrome Proportionoftotal childhoodepilepsy
Ageofpresentation Descriptionofsyndrome
Westsyndrome15 2---3% 3---12months Infantilespasmswithassociated
hypsarrhythmiaonEEG.Oftensecondaryto structuralbrainlesions.Globaldevelopmental impairmentistypicallyseen.
Childhoodabsenceepilepsy15 2---5% 8---12years Multipleabsenceseizuresperdayinan otherwisehealthychild.Absencescan
invariablybeprovokedbyhyperventilationand areassociatedwith2.5---3.5Hzgeneralized spike-wavedischargesonEEG
Benignchildhoodepilepsywith centro-temporalspikes15
3---8% 3---14years Briefhemifacialseizuresthatmaysecondarily generalizeiftheyoccurnocturnally.EEGis characteristic,showinganormalbackground withhighamplitudesharpwavesinthe centro-temporalregions,whichareactivated bydrowsinessandsleep.98%ofchildrenare seizure-freeoffmedicationbyaged18. Juvenileabsenceepilepsy15 1---4% 8---20years Relativelyinfrequenttypicalabsenceseizures
aswellasgeneralizedconvulsiveseizuresinan otherwisenormalchildoryoungadult. Generalizedepileptiformdischargesareseen oninterictalEEG.
Juvenilemyoclonicepilepsy15 5---11% 8---25years Frequentmyoclonicseizuresthataremore prominentinthemorninginanotherwise normalchildoryoungadult.Mostpatientsalso havegeneralizedconvulsiveseizures.
Table4 InternationalLeagueAgainstEpilepsy(ILAE)etiologicalclassificationofepilepsy.
OldILAEetiologicalclassification7 ProposednewILAEetiologicalclassification10
Idiopathic Asyndromethatisonlyepilepsy,withno underlyingstructuralbrainlesionorother neurologicsignsorsymptoms.Typically age-dependentepilepsysyndromes.
Genetic Epilepsiesinwhichageneticetiologyhasbeen proven,orcanbededuced.Mostepilepsies previouslyconsideredidiopathicarenow consideredgenetic.
Symptomatic Epilepsyinwhichtheseizuresarearesult ofandidentifiablediseaseprocess,suchas aninbornerrorormetabolism,CNS infection,orstructuralbrainlesion.
Structural Epilepsiessecondarytoanidentifiablestructural brainlesion.Thelesion(s)maybecongenital(e.g. lissencephaly),oracquired(e.g.traumatic), staticorprogressive(e.g.neoplasm).Some structuralepilepsiesaregeneticallydetermined (e.g.tuberoussclerosis)
Cryptogenic Epilepsyinwhichtheseizuresarebelieved tobesymptomatic,butnoidentifiable etiologyhasbeenidentified.
Metabolic Epilepsiessecondarytoinheritedmetabolic diseasewheretheepilepsyisconsideredasa resultofthemetabolicderangement. Immune Epilepsiessecondarytoapathological
immune-mediatedprocess,wherethereis evidenceofCNSinflammation(e.g.autoimmune encephalitis).
Infectious Epilepsiessecondarytoinfectionsuchascerebral malaria,orviralencephalitis.
Unknown Epilepsiesinwhichnoidentifiablecausehasbeen found,norcanbededuced.
Giventhatepilepsyisadisorderaffectingthebrain,itdoes not come as a surprise that these comorbidities have a neurologicalbasis. Recently, genetic studies have demon-strated a significant amount of genetic overlap between epilepsyandotherneurodevelopmentaldisorders, suggest-ingthattheyallhaverelatedneurobiologicaldeterminants. Overall, it has been estimated that 80% of children with epilepsyhavecognitive,psychosocial,orexecutivefunction problems.1830%ofchildrenwithepilepsyhave developmen-tal delay,25% have languagedelay, 5---15% have ASD,and 20---30% have ADHD.19---22 Recognition and management of theseco-morbidities is essential, sincethey canoften be biggerprioritiesfor the familythantheepileptic seizures themselves.
TheroleoftheEEG
Ashighlightedabove,theEEGisausefultooltoassistthe clinicianinthe classificationof seizuretypes andepilepsy syndromes.HoweveritmustbeemphasizedthatEEGshould notbe usedasa diagnostic test for epilepsy,since ithas bothpoor specificityand sensitivity.One-third ofpatients withepilepsywillhaveacompletelynormalinterictalEEG,9 whilst5%ofchildrenwithoutepilepsywilldemonstratefrank epileptiformabnormalities.23 When thereis clinicaldoubt asto whether episodesthat areoccurring frequently are epilepticornot,video-telemetryorambulatoryEEGcanbe veryuseful, sincemost epileptic events will have an EEG correlate.
Management
Managementofchildhoodepilepsymustbeholistic,giving dueconsiderationtotheindividualneedsandexpectations ofthepatientandtheirfamily.Theconceptsof‘‘epilepsy’’
and ‘‘the epilepsies’’ are not easy to grasp, and a key role of the clinician is to help the patient and their family make sense of a condition that has traditionally been misunderstoodand stigmatized.Expert management reliesonhavingasoundknowledgeofthepharmacological treatmentoptions,includingtheirindications,interactions, and side-effect profiles. Non-pharmacological treatment options include epilepsy surgery, the ketogenic diet, and neurostimulation techniques. Non-pharmacological treat-mentmayallowsomechildrenwhoseepilepsyisrefractory to medical treatment to become seizure-free, and may substantiallyreducetheseizureburdenfor others. Manag-ing epilepsy is about more than controlling seizures, and management within a multidisciplinary team may be the optimumwaytoensurethatallofachild’sepilepsy-related needs are met.24 Such a team may include pediatricians orpediatricneurologists,neurophysiologists,psychologists, occupational therapists,physiotherapists,speechand lan-guagetherapists,specialistnurses,dieticians,radiologists, andsurgeons.
Indicationsforstartingtherapy
In the Dutch study of epilepsy in childhood, after a sin-gle unprovoked epileptic seizure, 46% of children were found tohave nofurtherseizures over a2-year follow-up period.25 Based onthishigh non-recurrencerate,coupled withgoodevidencethatearlyAEDtreatmentdoesnot influ-ence long-term seizure outcome,26 it is generally advised that treatment is notstarted following a singleseizure.27 After twounprovoked seizures, the probabilityof a third eventrangesfrom60%to90%,28andthereforeconsideration oftreatmentinitiationisreasonable.
seizure=treatment.’’ The recently adopted ILAE opera-tional definition of epilepsy(Table 1) recognizes that, in some circumstances, such as the presence of structural or metabolic etiology, the risk of recurrence after a sin-gle seizure is as high as it is after two seizures in the generalpopulation.6Conversely,certainchildhoodepilepsy syndromes, particularly BCECTS and Panayiotopoulos syn-drome,typicallyfollowacourseinwhichveryfewseizures are followed by complete remission, and it is reasonable toavoidtreatingmanychildrenwiththesesyndromeswith medication.29,30Thedecisiononwhethertostarttreatment is therefore multifacetedand must bear in mind the fol-lowing:age,syndromicdiagnosisifapplicable,etiology,and acceptabilityofafurtherseizure(whichmaybereducedif previousseizureshavebeenprolongedortraumatic).
Goalsoftherapy
The ideal goal of AED therapy is cessation of epileptic seizureswithoutundesirablesideeffects.Treatingseizures isdesirable,astheyarefrighteningforfamilies;candirectly leadtomedicalcomplications,suchasinjuryoraspiration; andmayinterferewitheducation,leisure,oremployment. The term epileptic encephalopathy is used to describe epilepsies in which epileptic activity itself is believed to contributetoseverecognitiveandbehavioralimpairments aboveandbeyondwhatwouldbeexpectedfromthe under-lying pathology alone.31 Examples of epilepsies in which effective control of epileptic activity appears togo hand in handwithimproved cognitive performanceareWS and Landau---Kleffner syndrome, otherwise known as acquired epilepticaphasia.Therelativecontributionofthe underly-ingetiologyversusongoingepilepticactivity---bothclinical seizures andsubclinicalepileptiform activity seen onEEG --- to cognitive and behavioral impairment in people with epilepsywillvaryindifferentepilepsysyndromes.Evenin so-called‘‘benign’’epilepsysyndromes,manychildrenwill have specific or general cognitive impairment. The term benign is therefore likelyto disappear from the epilepsy lexiconintime.Parentsmustbeawarethatcontrollingthe seizures may not have any impacton associated learning disability.
Effectivenessoftherapy
Overall, approximately 60% of children achieve complete seizurefreedomoncetheyareestablishedona therapeu-ticdosetheirfirstAED.Itisnotcurrentlypossibletopredict reliablywhichchildrenwillrespondwelltoAEDs,although certainriskfactors,suchasageofonset<1year,structural ormetabolicetiology,developmentalimpairment,andhigh frequency ofseizures beforetreatment initiationincrease thelikelihoodthattheepilepsywillberefractory.32,33
Evidence-basedAEDtreatment
There are 26 AEDs currently licensed for treatment of epilepsyinchildhood.Amongthesemedications,theolder oneshaveattainedtheirlicensethroughlongstanding estab-lisheduse,andtheneweronesweregenerallylicensedafter
demonstratinga>50%reductioninseizurefrequencywhen usedasadd-ontherapy inrefractoryepilepsy.Meanwhile, theevidencebaseforwhichAEDtouseasfirstlinetreatment remainslimited,withveryfewstudiesmeasuringlong-term outcomes.
The choice of initial treatment should take into accountthe seizure type(s), epilepsysyndrome, age, eti-ology,comorbidities,andpotentialinteractionswithother medications.34
Generalizedorfocalseizures
The SANAD trials used randomized unblinded methodol-ogyto compare initial treatment options, with epilepsies broadly stratified into two groups: epilepsy with focal seizures(previouslytermedpartialepilepsy), andepilepsy with generalized seizures (previously termed generalized epilepsy).35,36Themeanageofsubjectswas38.3yearsinthe focalgroupand22.5yearsinthegeneralizedgroup;thus, itisdifficulttosaywhetherthefindingsarefully applica-bletochildren.Treatmentefficacywasdeterminedbythe proportionofpatientswhoachieved12-monthremission2 yearsafterrandomization.
In the focal arm of SANAD, 1721 patients were ran-domized to treatment with lamotrigine, carbamazepine, gabapentin, or topiramate. Both lamotrigine and car-bamazepine were more efficacious than gabapentin or topiramate.Lamotriginetreatmentwasassociatedwith sig-nificantlyfewersideeffectsthancarbamazepine.
In the generalized arm of SANAD, 716 patients were randomizedtotreatment withlamotrigine, topiramate or sodium valproate. Here sodium valproate was more effi-cacious than both topiramate and lamotrigine. Sodium valproatewasbettertoleratedthantopiramate,withno sig-nificantdifferenceintolerabilitybetweensodiumvalproate andlamotrigine.
Syndrome-specificAEDtreatment
VeryfewtrialsofinitialAEDtreatmenthavebeenstratified byepilepsy syndrome;therefore, treatment decisions are generallyguided by whetherfocalseizures arepresent or not.TheexceptionhereisCAE,forwhichalong-termdouble blindedtrialcomparedethosuximide,sodiumvalproate,and lamotrigineinapopulationof453children.Freedomfrom failurerates at 12 months were asfollows: ethosuximide (45%),sodiumvalproate(44%),andlamotrigine(21%).There wasstatisticallysignificantsuperiorityofethosuximideand sodiumvalproate over lamotrigine. The sodium valproate groupexperiencedthemostundesirablesideeffects,most notablyattentiondysfunction.
Ithasbeen recentlydemonstratedthatcombinedtherapy withbothvigabatrinandcorticosteroidsresultsinimproved seizureoutcomesat 12---24monthsofage whencompared withcorticosteroidtherapyalone.38
There are no other syndrome-specific AED approaches based on grade 1 or 2 clinical evidence. There are sev-eral clinical reports of patients with myoclonic seizures experiencing a deterioration in myoclonus when sodium channel-blockingmedicationsarestarted. Sodiumchannel blockers include carbamazepine, lamotrigine, and pheny-toin.TheseAEDsarethereforeoftenavoidedinsyndromes characterized by myoclonic, seizures such as JME39 and Dravetsyndrome.40
Etiology-specifictherapy
Treatingepilepsybyetiologyisanattractiveconcept,since targetingtheunderlying diseasemechanismwould appear tobeamorespecificapproach. Epilepsycanbesecondary toagreatnumberofindividuallyrareinheritedmetabolic diseases, and when specific treatment for these is initi-atedseizurecontroloftenimproves.Pyridoxinedependency and GLUT1 deficiency syndrome may present with severe epilepsythatisrefractorytoAEDtherapy,butrespondvery welltospecifictreatmentwithpyridoxineandtheketogenic diet,respectively.
Recent advances in genetic understanding of epilepsy may in future lead to the stratification of patients with epilepsy into gene-specific AED therapy, though large cohorts will berequired tobuild a strong evidence base. Promising results have been observed with everolimus treatment for patients with tuberous sclerosis,41 and stiripentoltreatmentinDravetsyndrome,asevereepileptic encephalopathywhoseonsetisininfancy,causedby muta-tionsintheSCN1Agene.42
Monitoringtherapy
Regularmonitoringofantiepilepticdruglevelsisrarely indi-cated.The bestwaytomonitor fortoxicityistokeepthe patientunderregularfollow-upandtorecommendthatthe familyseekmedicalattentioniftheynoticeanypotential side effects. AEDsare generally muchbetter tolerated if theyareintroduced atalow dose,which isincrementally titratedupwards.CheckingAEDlevelsmaybeusefulfor cer-tainmedicationswithanarrowtherapeuticwindow,suchas phenytoin,phenobarbital,andtriplebromide,andin situa-tions of treatment failure and where it is suspected that subtherapeuticlevelsmaybebeingachieved.
Refractoryepilepsy
WhenthefirstAEDdoesnotwork,howtoselectthe secondone?
If seizure freedom is not achieved with the first AED, the chance of attaining complete remission with a sec-ond AED is 40%.43 For every AED that is unsuccessful, the chances of achieving remission with a different AED diminishproportionately. Ultimately,one-thirdof children with epilepsy will continue to have epileptic seizures
regardless of medication.44 The ILAE has set forth a practical definition of drug-resistant epilepsy as epilepsy in which two appropriately chosen and appropriately dosed AEDs have been administered without remission of seizures.45
Choiceofsecond-lineAEDtherapyhasnoevidencebase. Thereis alsonoevidencethat polytherapyismore effica-cious than alternative monotherapy. In the first instance, most clinicianswill tryalternative monotherapy,although therewilltypicallybea periodof overlapwhilstoneAED is gradually withdrawn and another is introduced. Once two or more monotherapy approaches have been unsuc-cessful, apolytherapyapproachmay thenbe tried.When considering polytherapy, interactions between AEDs must be considered, as this may affect dosing. For example, the lamotrigine dose should be halved when adminis-tered concomitantly with sodium valporate due to the enzyme-inhibiting properties of the latter. It is generally recommendedthattheAEDregimendoesnotinclude med-ications with the same broad mechanism of action. For example,both carbamazpeineandlamotrigine aresodium channel-blockers, so one should be cautious about using thesetwosimultaneously.
WhenmultipleAEDsfailtowork
For children with refractory epilepsy withfocal seizures, surgicaltreatmentshouldbeconsidered.Inrandomized tri-als of surgery versus additional AED therapy in carefully selectedsurgical candidates,theproportionofthese chil-drenwhobecomeseizure-freeaftersurgeryissignificantly greaterthanthoserandomizedtoreceiveanadditionalAED. Comprehensivepreoperativeevaluationinvolvesa multidis-ciplinary approach to pinpoint the epileptogenic zone of thebrainastheappropriatesurgicaltarget.High-resolution neuroimaging, ictal EEG, dynamic ictal radionucelotide scan (such as single photon-emission computed tomogra-phy [SPECT]), and detailed neuropsychological evaluation areallusefultoolsinthisregard.Between30%and80%of pediatric patients achieve long-term seizure-freedom fol-lowing epilepsy surgery46; Non-resective surgical options may be used in highly specific situations. For example, interhemisphericdisconnectionmaybeusedincaseswhere seizures originating from one hemisphere are frequently generalizing.
Another alternative to further AED trials in refractory epilepsyistheketogenicdiet,whichusesahighly special-izeddiettomaintainthepresenceofketonebodiesinthe systemiccirculation.Ketonebodiesappeartohavean anti-epilepticeffect,althoughtheexactmechanismisnotwell understood.Theketogenicdietappearstobeequallyas effi-caciousasadd-onAEDtherapy.Inonestudy16%ofchildren withrefractoryepilepsybecameseizure-freeonthediet.47 Forsomefamilies,administrationoftheketogenicdietmay bechallenging.
Specificsituations
Clusters
Althoughthereisnoaccepteddefinitionofclusterseizures, it is well accepted that patients withrefractory epilepsy can go through self-limited periods of significantly wors-enedseizurecontrol.Suchperiodsareoftenprecipitatedby stress,intercurrentillness,orsleepdeprivation.Therehave beennoclinicaltrialstoinformclinicianshowbestto man-agethesesituations,butmanyhaveexperiencedthatashort courseofalong-actingbenzodiazepine,suchasclobazam, canbeeffective.
Statusepilepticus
Statusepilepticusreferstoanyseizurelastinglongerthan 30min, or multiple seizures without restitution of nor-mal conscious level between events. It may classified as convulsive, focal, autonomic, or absence. The recom-mendedfirstlinetherapyisabenzodiazepine,whichmaybe administeredrectally(diazepam),orallyornasally (midazo-lam),orintravenously(lorazepamordiazepam).Ifseizures persistdespiteonedoseofbenzodiazepine,asecond ben-zodiazepine dose may be given.49 Treatment for status epilepticus following two ineffective doses of benzodi-azepinehasnoevidencebase,andresponsestotherapymay behighlyindividual.Optionsincluderectalparaldehyde,IV phenytoin, IV phenobarbital, IV sodium valproate, and IV levetiracetam. It is recommended that children prone to episodesofstatusepilepticushavetheirpersonalized treat-mentplanskeptbothbythefamily,andbyanyemergency departmentwhere theyarelikelytobereceived.Forthe treatment of children without personalized plans, emer-gencydepartmentsshouldhavegenericprotocolsinplaceto ensurepromptmanagementandappropriatedosing.34 The differentialdiagnosisofstatusepilepticusiseasytooverlook in theheatof theemergency situation,butconsideration should begiven tothe possibility of non-epileptic status, andtoincreasedintracranialpressure,inwhichdecorticate posturingmaymimicconvulsiveactivity.Administrationofa highdosebloodpressure-loweringanticonvulsantscanhave significantadverseeffectsincasesofincreasedintracranial pressure.
Pregnancy
Forwomenofchildbearingagewithepilepsy,consideration needs tobe given tothe potential teratogenic effects of medication. The risk toan unborn fetus frompoorly con-trolled epilepsy outweighs the teratogenic risk conferred fromanyAED,butthereisnowclearevidencethatsodium valproate is significantly moreteratogenic thanthe other AEDs,with5.7---16.8% ofpregnanciesaffected. Therefore, for patients with newly diagnosed epilepsy, if they may become pregnant in the next few years, it is advisable to commence them on a medication other than sodium valproate.50
Discontinuationoftherapy
For children who have been seizure-free on medication for over 2 years on monotherapy, discontinuation of AED treatmentshouldbeconsidered,particularlyifthereisno
structuralor metabolicunderlying etiology.In children in whom AED therapy is withdrawn after 2 years of seizure freedom,70% willremainseizure-free for thesubsequent 2years.51
Suddenunexpecteddeathinepilepsyandmortality
In a Finish cohort of 245 patients with childhood-onset epilepsyfollowed-upover40years,theoverallstandardized mortality rate was calculated as 6.4/1000 patient-years, whichisapproximately1.5timesthatofthegeneral popula-tion.Thevastmajorityofdeathsoccurredinadulthood,and halfwerenotrelatedtoepilepsy.Suddenunexpecteddeath in epilepsy(SUDEP) accounted for 23/33 epilepsy-related deathsinthiscohort.Themajorriskfactorsforincreased mortalityarestructuralormetabolicetiology,frequencyof seizures,andthepresenceofnocturnalseizures.52Children withuncomplicatedepilepsydonotappeartobeatriskof SUDEP.
Future
directions
Despite major recent advances in the understanding of epilepsyetiology,andtheemergence of anumberofnew AEDs,theproportionofchildhood-onsetepilepsiesthatare refractorytotreatmenthaslargelyremainedunchanged.To addressthisissue,thereisa clearneedfor amore strati-fiedapproachtotreatment.Traditionally,stratificationhas beenbybroadseizuretype(focalorgeneralized),andonly occasionallybyepilepsysyndrome.Withtheemergenceof genetictechnologyitispossiblethatinthefuture, stratifi-cationwillbedonebygenotype.Inordertobuildauseful evidencebase,largemulticentertrailsareneeded.
Conclusion
Childhood-onsetepilepsiesareaheterogeneousgroupof dis-orderswitha widevariety of causes andan equally wide varietyofpresentations.The majorityof patientsachieve seizurefreedomwithtreatmentonasingleAED,whichmust bechosen appropriately.Successfulmanagementneedsto beunderscoredbyastructuredapproachtodiagnosis,which shouldtakeamulti-axialapproach.Recentadvancesinthe understandingofepilepsyetiologyandpathophysiologyhave resulted in a reconceptualization of the classification of epilepsies.Despitethescientificadvances,anddespitethe developmentofanumberofnewAEDs,asignificant treat-mentgapstillexists, witha proportionof patientshaving refractory disease. For some carefully selected patients, epilepsy surgery can lead to remission, but successful surgerymustbeunderpinnedbycomprehensivepre-surgical evaluation.Apersonalizedmedicalapproachusingstratified treatmentschemesmayhelptodeliverbetteroutcomesin future.Inordertoachievethis,globaleffortsmustbemade toestablisharobustevidencebase.
Conflicts
of
interest
References
1.ThurmanDJ,BeghiE,BegleyCE,BergAT,BuchhalterJR,Ding D,etal.Standardsforepidemiologicstudiesandsurveillance ofepilepsy.Epilepsia.2011;52:2---26.
2.SalomonJA,VosT,HoganDR,GagnonM,NaghaviM,MokdadA, etal.Commonvaluesinassessinghealthoutcomesfromdisease andinjury:disabilityweightsmeasurementstudyfortheGlobal BurdenofDiseaseStudy2010.Lancet.2012;380:2129---43. 3.Banerjee PN,FilippiD,Allen HauserW.The descriptive
epi-demiology of epilepsy --- a review. Epilepsy Res. 2009;85: 31---45.
4.Kotsopoulos IA, van Merode T, Kessels FG, de Krom MC, Knottnerus JA. Systematic reviewand meta-analysis of inci-dencestudiesofepilepsyandunprovokedseizures.Epilepsia. 2002;43:1402---9.
5.FisherRS,vanEmdeBoasW,BlumeW,ElgerC,GentonP,Lee P,etal.Epilepticseizuresandepilepsy:definitionsproposedby theInternationalLeagueAgainstEpilepsy(ILAE)andthe Inter-nationalBureauforEpilepsy(IBE).Epilepsia.2005;46:470---2. 6.FisherRS,AcevedoC,ArzimanoglouA,BogaczA,CrossJH,Elger
CE,etal.ILAEofficialreport:apracticalclinicaldefinitionof epilepsy.Epilepsia.2014;55:475---82.
7.EngelJJr,InternationalLeagueAgainstEpilepsy(ILAE).A pro-poseddiagnosticschemeforpeoplewithepilepticseizuresand withepilepsy:reportoftheILAETaskForceonClassification andTerminology.Epilepsia.2001;42:796---803.
8.UldallP,AlvingJ,HansenLK,KibaekM,BuchholtJ.The misdi-agnosisofepilepsyinchildrenadmittedtoatertiaryepilepsy centre with paroxysmal events. Arch Dis Child. 2006;91: 219---21.
9.StroinkH,vanDonselaarCA,GeertsAT,PetersAC,BrouwerOF, ArtsWF.Theaccuracyofthediagnosisofparoxysmaleventsin children.Neurology.2003;60:979---82.
10.InternationalLeagueAgainstEpilepsy.Epilepsydiagnosis;2015. Available from: https://www.epilepsydiagnosis.org/ [cited 17.04.15].
11.IkizMA,CetinII,EkiciF,GüvenA,De˘gerliyurtA,KöseG. Pedi-atric syncope: is detailed medical history the key point for differentialdiagnosis?PediatrEmergCare.2014;30:331---4.
12.KhooTB.Classificationofchildhoodepilepsiesinatertiary pedi-atricneurologyclinicusingacustomizedclassificationscheme fromtheinternationalleagueagainstepilepsy2010report.J ChildNeurol.2013;28:56---9.
13.OkaE,OhtsukaY,YoshinagaH,MurakamiN,KobayashiK,Ogino T.Prevalenceofchildhoodepilepsyanddistributionof epilep-ticsyndromes:apopulation-basedsurveyinOkayama,Japan. Epilepsia.2006;47:626---30.
14.WirrellEC,GrossardtBR,Wong-KisielLC,NickelsKC.Incidence andclassificationofnew-onsetepilepsyandepilepsysyndromes inchildreninOlmstedCounty,Minnesotafrom1980to2004:a population-basedstudy.EpilepsyRes.2011;95:110---8.
15.BeghiM,BeghiE,CornaggiaCM,GobbiG.Idiopathicgeneralized epilepsiesofadolescence.Epilepsia.2006;47:107---10.
16.GaillardWD,ChironC,CrossJH,HarveyAS,KuznieckyR, Hertz-PannierL,etal.Guidelinesforimaginginfantsandchildrenwith recent-onsetepilepsy.Epilepsia.2009;50:2147---53.
17.Helbig I,Scheffer IE,Mulley JC,Berkovic SF. Navigatingthe channelsandbeyond:unravellingthegeneticsoftheepilepsies. LancetNeurol.2008;7:231---45.
18.Høie B, Sommerfelt K, Waaler PE, Alsaker FD, SkeidsvollH, MykletunA.Thecombinedburdenofcognitive,executive func-tion, and psychosocialproblems in childrenwithepilepsy: a population-basedstudy.DevMedChildNeurol.2008;50:530---6.
19.Baca CB, Vickrey BG, Caplan R, Vassar SD, Berg AT. Psychi-atricandmedicalcomorbidityandqualityoflifeoutcomesin childhood-onsetepilepsy.Pediatrics.2011;128:e1532---43.
20.MatsuoM,MaedaT,SasakiK,IshiiK,HamasakiY.Frequent asso-ciationofautismspectrumdisorderinpatientswithchildhood onsetepilepsy.BrainDev.2010;32:759---63.
21.BergAT,PlioplysS,TuchmanR.Riskandcorrelatesofautism spectrumdisorderinchildrenwithepilepsy:acommunity-based study.JChildNeurol.2011;26:540---7.
22.HermannB,JonesJ,DabbsK,AllenCA,ShethR,FineJ,etal. Thefrequency, complicationsand aetiologyof ADHDin new onsetpaediatricepilepsy.Brain.2007;130:3135---48.
23.OkuboY,MatsuuraM,AsaiT,AsaiK,KatoM,KojimaT,etal. EpileptiformEEGdischargesin healthychildren:prevalence, emotionaland behavioralcorrelates, and geneticinfluences. Epilepsia.1994;35:832---41.
24.GoldsteinJ,PlioplysS,ZelkoF,MassS,CornsC,BlaufussR,etal. Multidisciplinaryapproachtochildhoodepilepsy:exploringthe scientificrationaleandpracticalaspectsofimplementation.J ChildNeurol.2004;19:362---78.
25.StroinkH,BrouwerOF,ArtsWF,GeertsAT,PetersAC,van Donse-laarCA.Thefirstunprovoked,untreatedseizureinchildhood: ahospitalbasedstudyoftheaccuracyofthediagnosis,rate ofrecurrence,andlongtermoutcomeafterrecurrence.Dutch studyofepilepsyinchildhood.JNeurolNeurosurgPsychiatry. 1998;64:595---600.
26.CamfieldP,CamfieldC,SmithS,DooleyJ,SmithE.Long-term outcomeisunchangedbyantiepilepticdrugtreatmentaftera firstseizure:a 15-year follow-upfrom a randomizedtrialin childhood.Epilepsia.2002;43:662---3.
27.Hirtz D,Berg A, Bettis D,Camfield C,Camfield P,Crumrine P,et al. Practiceparameter: treatmentof the child with a firstunprovokedseizure:reportoftheQualityStandards Sub-committee of the American Academy of Neurology and the PracticeCommitteeoftheChildNeurologySociety.Neurology. 2003;60:166---75.
28.HauserWA,RichSS,LeeJR,AnnegersJF,AndersonVE.Riskof recurrentseizuresaftertwounprovokedseizures.NEnglJMed. 1998;338:429---34.
29.OguniH.Treatmentofbenignfocalepilepsiesinchildren:when andhowshouldbetreated?BrainDev.2011;33:207---12.
30.ArtsWF,GeertsAT.Whentostartdrugtreatmentforchildhood epilepsy:theclinical-epidemiologicalevidence.EurJPaediatr Neurol.2009;13:93---101.
31.Berg AT, Berkovic SF, Brodie MJ, Buchhalter J, Cross JH, vanEmde Boas W, et al. Revised terminology and concepts for organization of seizures and epilepsies: report of the ILAECommissiononClassificationandTerminology,2005---2009. Epilepsia.2010;51:676---85.
32.BergAT,ShinnarS,LevySR,TestaFM,Smith-RapaportS, Beck-ermanB.Earlydevelopmentofintractableepilepsyinchildren: aprospectivestudy.Neurology.2001;56:1445---52.
33.SillanpääM,SchmidtD.Earlyseizurefrequencyandaetiology predictlong-termmedicaloutcomeinchildhood-onsetepilepsy. Brain.2009;132:989---98.
34.NiceGuideline137.Theepilepsies:thediagnosisand manage-mentoftheepilepsiesin adultsand childreninprimaryand secondarycare.London: NationalInstitute of Clinical Excel-lence;2012,January(revisedDecember2013).Availablefrom:
http://www.nice.org.uk/guidance/cg137[cited21.04.15]. 35.MarsonAG,Al-KharusiAM,AlwaidhM,AppletonR,BakerGA,
Chadwick DW, et al. The SANAD study of effectiveness of carbamazepine, gabapentin, lamotrigine, oxcarbazepine, or topiramatefortreatmentofpartialepilepsy:anunblinded ran-domisedcontrolledtrial.Lancet.2007;369:1000---15.
37.LuxAL, Edwards SW, Hancock E, Johnson AL, Kennedy CR, Newton RW, et al. The United Kingdom Infantile Spasms Study(UKISS) comparinghormone treatmentwith vigabatrin ondevelopmentalandepilepsyoutcomestoage14months:a multicentrerandomisedtrial.LancetNeurol.2005;4:712---7.
38.O’CallaghanFJ.UKISStrial,preliminaryresults.In:Presented attheBritishPaediatricNeurologyAssociationAnnualMeeting. 2015.
39.CrespelA, Genton P,Berramdane M, Coubes P, Monicard C, Baldy-MoulinierM,etal.Lamotrigineassociatedwith exacerba-tionordenovomyoclonusinidiopathicgeneralizedepilepsies. Neurology.2005;65:762---4.
40.BrunklausA,DorrisL,EllisR,ReaveyE,LeeE,ForbesG,etal. TheclinicalutilityofanSCN1Ageneticdiagnosisin infantile-onsetepilepsy.DevMedChildNeurol.2013;55:154---61.
41.Krueger DA, Care MM, Holland K, Agricola K, Tudor C, Mangeshkar P, et al. Everolimus for subependymal giant-cell astrocytomas in tuberous sclerosis. N Engl J Med. 2010;363:1801---11.
42.ChironC,Marchand MC,Tran A,Rey E,d’AthisP,VincentJ, etal.Stiripentolinseveremyoclonicepilepsyininfancy:a ran-domisedplacebo-controlledsyndrome-dedicatedtrial.STICLO studygroup.Lancet.2000;356:1638---42.
43.Camfield PR, Camfield CS, Gordon K, Dooley JM. If a first antiepileptic drug fails to control a child’s epilepsy, what are the chances of success with the next drug? J Pediatr. 1997;131:821---4.
44.BergAT,LevySR,TestaFM,D’SouzaR.Remissionofepilepsy aftertwodrug failuresinchildren: a prospectivestudy.Ann Neurol.2009;65:510---9.
45.KwanP,ArzimanoglouA, BergAT,BrodieMJ,AllenHauserW, MathernG,etal.Definitionofdrugresistantepilepsy:consensus proposalbytheadhoctaskforceoftheILAECommissionon TherapeuticStrategies.Epilepsia.2010;51:1069---77.
46.Jobst BC, Cascino GD. Resective epilepsy surgery for drug-resistantfocalepilepsy:areview.JAMA.2015;313:285---93.
47.MackayMT,Bicknell-RoyleJ,NationJ,HumphreyM,HarveyAS. Theketogenicdietinrefractorychildhoodepilepsy.JPaediatr ChildHealth.2005;41:353---7.
48.EnglotDJ,Chang EF,AugusteKI.Vagusnervestimulation for epilepsy:ameta-analysisofefficacyandpredictorsofresponse. JNeurosurg.2011;115:1248---55.
49.CapovillaG,BeccariaF,BeghiE,MinicucciF,SartoriS,Vecchi M.Treatmentofconvulsivestatusepilepticusinchildhood: rec-ommendationsoftheItalianLeagueAgainstEpilepsy.Epilepsia. 2013;54:23---34.
50.WlodarczykBJ,PalaciosAM,GeorgeTM,FinnellRH. Antiepilep-tic drugs and pregnancy outcomes. Am J Med Genet A. 2012;158A:2071---90.
51.ShinnarS,BergAT,MoshéSL,KangH,O’DellC,AlemanyM,etal. Discontinuingantiepilepticdrugsinchildrenwithepilepsy: a prospectivestudy.AnnNeurol.1994;35:534---45.