Rev. bras. ortop. vol.49 número4
Texto
Imagem
Documentos relacionados
Sixty synthetic femurs were tested in physiological bending, to calculate the yield and ultimate load to displacement following fixation of distal diaphysis fractures of the femur
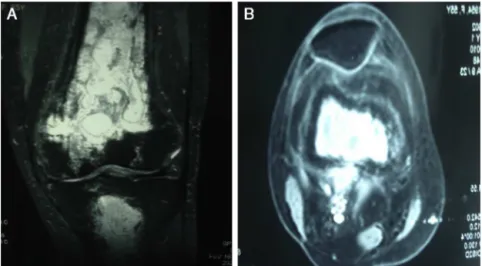
Tomographic images on coronal (A), sagittal (B) and axial (C) planes depicting intra-articular radiocarpal and distal radio-ulnar fracture of the distal end of the radius,
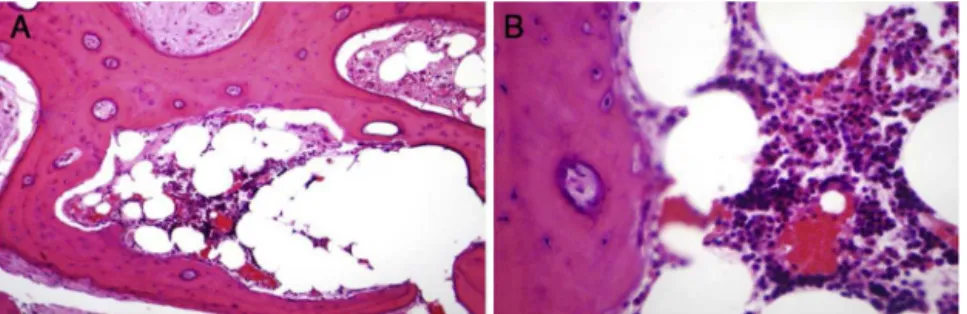
Histomorphometry of the distal femur showed a decrease in trabecular volume in the untreated group (OVX), and an increase in the two treated groups, principally in the
For the WKY phrenic nerves, a trend towards a smaller size (area and diameter) was observed from proximal to distal segments on both sides and in both genders, with no..
It was observed that in the evaluation of the graft incorporation in the proximal and distal interfaces, quality and appearance of the graft and fixation
The probability of attending school four our group of interest in this region increased by 6.5 percentage points after the expansion of the Bolsa Família program in 2007 and
ABSTRACT Molecular characterization of fall armyworm Spodoptera frugiperda resistant to Vip3Aa20 protein expressed in corn Transgenic plants containing genes from Bacillus
O objetivo do presente trabalho é apresentar a Associação Terra do Marolo (ATEM) como forma de promover o desenvolvimento local do Município de Paraguaçu- MG,
