w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Fc
gamma
receptor
IIIa
polymorphism
is
not
associated
with
susceptibility
to
systemic
lupus
erythematosus
in
Brazilian
patients
Marcelle
Grecco,
Viviane
Cardoso
dos
Santos,
Kaline
Medeiros
Costa
Pereira,
Luís
Eduardo
Coelho
Andrade,
Neusa
Pereira
da
Silva
∗UniversidadeFederaldeSãoPaulo(UNIFESP),DepartamentodeMedicina,DisciplinadeReumatologia,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received22September2014 Accepted15June2016
Availableonline25October2016
Keywords:
Systemiclupuserythematosus FcgammareceptorIIIa
Singlenucleotidepolymorphism Genepolymorphism
Immunogenetics
a
b
s
t
r
a
c
t
WeevaluatedthepossibleassociationbetweenFCGR3AV/F(158)polymorphismandSLE sus-ceptibilityandclinicalphenotypein305sequentiallyretrievedSLEpatientsand300healthy controlsfromthesoutheasternpartofBrazilbyallele-specificpolymerasechainreaction. OurresultsshowednoassociationbetweenFCGR3A158V/FallelesandsusceptibilitytoSLE inthisseriesofpatientsalbeittheheterozygousgenotypewasstronglyassociatedwiththe disease.
©2016PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Polimorfismo
do
receptor
Fc
gama
IIIa
não
está
associado
à
susceptibilidade
ao
lúpus
eritematoso
sistêmico
em
pacientes
brasileiros
Palavras-chave:
Lúpuseritematososistêmico ReceptorFcgamaIIIa
Polimorfismodenucleotídeoúnico Polimorfismogenético
Imunogenética
r
e
s
u
m
o
Avaliou-seapossívelassociac¸ãoentreopolimorfismoFCGR3AV/F(158)easuscetibilidade eofenótipoclínicodolúpuseritematososistêmico(LES)em305pacientescomLES admi-tidossequencialmentee300controlessaudáveisdaRegiãoSudestedoBrasilporreac¸ão emcadeiadapolimerasealelo-específica.Osresultadosdopresenteestudomostraramnão haverassociac¸ãoentreosalelosFCGR3A158V/FeasuscetibilidadeaoLESnessasériede pacientes,aindaqueogenótipoheterozigototenhasidofortementeassociadoàdoenc¸a.
©2016PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobuma licenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](N.P.Silva). http://dx.doi.org/10.1016/j.rbre.2016.07.013
Introduction
Systemic lupuserythematosus(SLE) isconsidered the pro-totype of chronic immune complex-mediated diseases. In physiologicalconditions,circulatingimmunecomplexes(IC) areremovedfromtheperipheralbloodandotherbiological fluidsbythemononuclearphagocyticsystem.1,2 InSLE,the inadequateclearanceofICmayleadtotissuedamagedueto ICtissuedepositionandoverload,whichresultsinreleaseof inflammatorymediatorsandinflammatorycellinflux.2,3The Fcgamma receptors(Fc␥R),presentinmononuclear phago-cyticcells,playanimportantroleintheclearanceofICand apoptoticcells.4,5 Inaddition, theinternalization ofnucleic acid-containingIC via Fc␥Rbyplasmacytoid dendriticcells allowsthebindingofintracellulartoll-likereceptors(TLR)and consequent activationofdownstreamcascades that culmi-nate inthe synthesis oftypeI interferon.6,7 Several single nucleotidepolymorphisms(SNPs)havebeendescribedinthe Fc␥Rencodinggenes,andsomeofthemhavefunctional con-sequences.Asexpected,someofthesepolymorphismshave beenextensivelystudiedinautoimmunediseases.5,8
Human Fc␥RIII (CD16) receptor is an extensively glyco-sylated heterogeneousproteinwithan apparentmolecular weight of 50–80kDa. FCGR3A gene codes for the Fc␥RIIIa receptorpresentinmacrophages,NKand␥␦Tcells,with low-affinityforIgG-containingIC.4,9,10TheFCGR3Agenepresents a G559T polymorphism that leads to the substitution of ValineforPhenylalanineatposition158 ofthepolypeptide chain(158V/F), reducingevenmorethereceptoraffinityfor IgG subclasses.9–11 The association between FCGR3A gene polymorphism and SLEhas been studied byseveral inves-tigators. However, conflicting results have been reported concerningthisassociationindifferentpopulations.9,10,12–16 Given this scenario, the present study aimed at investi-gating the Fc␥RIIIa 158V/F polymorphism in Brazilian SLE patientsthatareembeddedinapopulationwithmixedethnic background.
Material
and
methods
Patientsandcontrols
Peripheralbloodwasobtainedfrom305sequentiallyretrieved SLEpatientsattendingthe RheumatologyOutpatientClinic at Universidade Federal de São Paulo – UNIFESP, Brazil. All patients met at least four of the revised criteria for classification of SLEaccording to the American College of Rheumatology.17 Detailed clinical characteristics were not availableforallpatientsandonlythechartswithconsistent datawereconsideredintheanalysisoftheclinicalphenotype ofdisease.Accordingly,SystemicLupusInternational Collab-orating Clinics/American Collegeof Rheumatology-Damage Index (SLICC-DI) data was available for 167 patients. The controlgroupcomprised300healthyblooddonorswhohad nofamilyhistoryofautoimmunediseasesasassessedbya detailedquestionnaire.Thestudywasapprovedbythe Insti-tutional Ethics Committee (# 2074/07) and all participants providedwritteninformedconsent.
Ethnicclassification
LatinAmericancountriesingeneral,andBrazilinparticular, presentintenseethnicmiscegenation,mainlyattheexpense of Africanand European elements.Weadopted the ethnic classificationusedbytheGrupoLatinoamericanodeEstudio delLupus(GLADEL).18Accordingtothisclassification,the indi-vidualsortshimself regardinghisown ethnicityas wellas hisparentsandfourgrandparents.Theethnicgroupsstudied weredefinedasfollows:
a) Blackethnicity:individualinthestudy,parentsand grand-parentsclassifiedasblack.
b) Whiteethnicity:individualinthestudy,parentsand grand-parentsclassifiedaswhite.
c) Mixedethnicity:existenceofatleastonedisagreementin thelineageoftheindividualclassificationbymaternalor paternalgrandparents.
NucleicacidisolationandFCGR3Apolymorphismanalysis
GenomicDNAwasextractedfromblood samplesbysalting out,basedonthemethodologypreviouslydescribedby Laiti-nenetal.19Weexaminedthesinglenucleotidepolymorphism (SNP)G559T (rs396991) of FCGR3A (http://www.ncbi.nlm. nih.gov/gene/2214) by allele-specific PCR according to Wu etal.9withminormodifications,usingasinglesenseprimer (5′TCACATATTTACAGAATGGCAATGG3′)andtwo anti-senseprimers:5′TCTCTGAAGACACATTTCTACTCCCTA C3′forGallele;and5′TCTCTGAAGACACATTTCTACTCC CTAA3′)forTallele.The50
Lreactionmixturecontained 100ngDNA,1.2mMMgCl2,0.2mMdNTP,2.5UPlatinumTaq DNAPolymeraseand10pmolofeachallele-specificsenseand antisenseprimers.PCRstartedwithaninitialstepof5minat 95◦C,followedby35cyclesof30sat94◦C,45sat54◦C,and20s at72◦C,withafinalextensionstepof8minat72◦C.The138bp ampliconwasanalyzedbyelectrophoresisona3%agarosegel inTBE.
Researchforautoantibodies
We identified all subserologies (double-stranded DNA, Sm, RNP,SSA,SSB).WeusedindirectimmunofluorescenceforANA test and ds-DNAand Ouchterlony doublediffusionfor the autoantibodiesSm,RNP,SSA-RoandSSB-La.
Statisticalanalysis
Table1–EthnicandgenderdistributionofSLEpatientsandcontrols.
SLE Controls
Ethnicity n % n % pa
Black 12 3.9 16 5.4 0.113
White 111 36.4 130 43.3
Mixed 182 59.7 154 51.3
Gender Female Male Female Male pa
291 14 178 122 <0.001
a Chi-squaretest.
Table2–FCGR3AgenotypeandalleledistributioninSLEpatientsandcontrols.
SLE Controls
Genotype n % n % pa pb
VV 35 11.5 54 18.0 0.002 0.023
FF 23 7.5 39 13.0 0.027
VF 247 81.0 207 69.0 <0.001
Allele n % n % pc
V 317 52.0 315 52.5 0.853
F 293 48.0 285 47.5
a Chi-squaretest.
b Bonferronicorrectionformultiplecomparisonsmethod.
c Chi-squaretest.
Results
There was no difference between patients and controls regardingethnicbackgrounddistribution,buttheSLEgroup hadalower frequencyofmalesascomparedtothecontrol group(Table1). However,thestatisticalanalysisperformed withineachgroupconfirmedthatneitheralleledistribution (SLEpatientsp=0.863;controlsp=1.000)norgenotype distri-bution(SLEpatientsp=0.449;controlsp=1.000),wasgender related(datanotshown).
Thepatient group had asignificantly higher proportion of heterozygous individuals (VF) than the control group (Table 2). Accordingly, the control group presented a sig-nificantly higher proportion of the homozygous FCGR3A genotypes VV (p=0.023) and FF (p=0.027). As expected, there was no difference between groups regarding the prevalence of individual alleles (p=0.853) (Table 2). The FCGR3A genotype distribution showed deviation from the Hardy Weinberg equilibrium in both, SLE and control groups.
There was no association between most clinical mani-festationsand genotypes (Table 3) withthe exception of a higherfrequencyofcentralnervoussystem (CNS) manifes-tations, observedin patients withFCGR3A VV genotype (5 patientshadpsychosis,threehad convulsionsand onehad othermanifestation).Amongthe167SLEpatientswith avail-ableSLICC/ACR-DIrecords,noassociationwasfoundbetween thisdamagescoreandanyFCGR3Agenotype(p=0.300)(Fig.1). Noassociation wasfound betweenFCGR3Agenotypes and the presence ofthe individual autoantibodies anti-dsDNA,
6.00
4.00
2.00
.00
FF VV
Genotype
SLICC-DI
VF
Fig.1–BoxplotdistributionofSLICC/ACR-DIaccordingto theFCGR3Agenotypes.Noassociationwasfoundbetween thedamagescoreandanyparticularFCGR3Agenotype (p=0.300).
anti-Sm,anti-RNP,anti-SS-A/Roandanti-SS-B/Laamongthe 305SLEpatients(Table4).
Discussion
Table3–ClinicalmanifestationsofSLEpatientsaccordingtoFCGR3Agenotype.
Manifestation(n) VV FF VF pa
n % n % n %
Skin(178) ⊕ 16 100.0 6 100.0 147 94.0 0.511
∅ 0 0.0 0 0.0 9 6.0
Oralulcers(145) ⊕ 1 6.7 0 0.0 28 22.6 0.158
∅ 14 93.3 6 100.0 96 77.4
Arthritis(178) ⊕ 16 100.0 6 100.0 138 88.5 0.244
∅ 0 0.0 0 0.0 18 11.5
Hematologic(178) ⊕ 10 62.5 5 83.3 116 74.3 0.509
∅ 6 37.5 1 16.7 40 25.7
Renal(178) ⊕ 10 62.5 2 33.3 88 56.4 0.463
∅ 6 37.5 4 66.7 68 43.6
Serositis(178) ⊕ 4 25.0 1 16.7 38 24.3 0.909
∅ 12 75.0 5 83.3 118 75.7
CNS(177) ⊕ 9 53.3 1 17.7 30 19.4 0.003
∅ 7 43.8 5 83.3 125 80.6
n,numberofpatientswithconsistentrecordsforeachclinicaltrait;CNS,centralnervoussystem;⊕,presencegenotype;∅,absencegenotype. a Chi-squaretest.
Table4–PresenceofindividualautoantibodiesinSLE patientsaccordingtotheFCGR3Agenotype.
Autoantibody Genotype pa
VV(n=35) FF(n=23) VF(n=247)
+ % + % + %
Anti-dsDNA 12 34.3 8 34.8 72 29.1 0.832
Anti-Sm 8 22.9 6 26.1 37 15.0 0.231
Anti-RNP 15 42.9 8 34.8 73 29.6 0.267 Anti-SS-A/Ro 8 22.9 10 43.5 74 30.0 0.243 Anti-SS-B/La 0 0 3 13.0 25 10.1 0.122
a Chi-squaretest.
distributionofFCGR3A158V/FallelesbetweenSLEandhealthy controls.Interestingly,SLEpatientsdidshowasignificantly higher frequency of the heterozygous 158V/F genotype. In addition, therewasa higherfrequencyofthe VV homozy-gousgenotypeinpatientswithahistoryofCNSinvolvement. Otherclinicaltraitsanddiseaseseveritywerenotassociated withFCGR3Apolymorphisminthisseries.Accordingtoour results,theFCGR3Agenotype distributiondidnotobeythe HardyWeinbergequilibrium.Onepossibleexplanationforthis observationistheexistenceofgenecopynumbervariation,a majorcauseofdeviationofHardy–Weinbergequilibrium.20In fact,recentstudieshaveshownthatFc␥receptorgenesmay presentcopy numbervariation,including FCGR3A,FCGR3B, andFCGR2Cgenes.21,22
Willcocksandcolleaguesfoundanassociationbetweenlow FCGR3BgenecopynumberandSLEinCaucasians,however thisassociationwasnotseeninChineseSLEpatientsin gen-eralorwhenSLEpatientswithlupusnephritiswereanalyzed separately.23 InanotherstudywiththeChinesepopulation, Zhouandcolleaguesfoundanassociationbetweenincreased FCGR3Agenecopynumber(3or4)andthepresenceof anti-glomerularbasementmembraneantibody.24
ItisknownthattheFCGR3A158Valleleencodesforahigher affinityreceptorthanthe158Fallele.9,10Consistentwiththe role playedbyFc␥RIIIainimmune complexclearance, it is
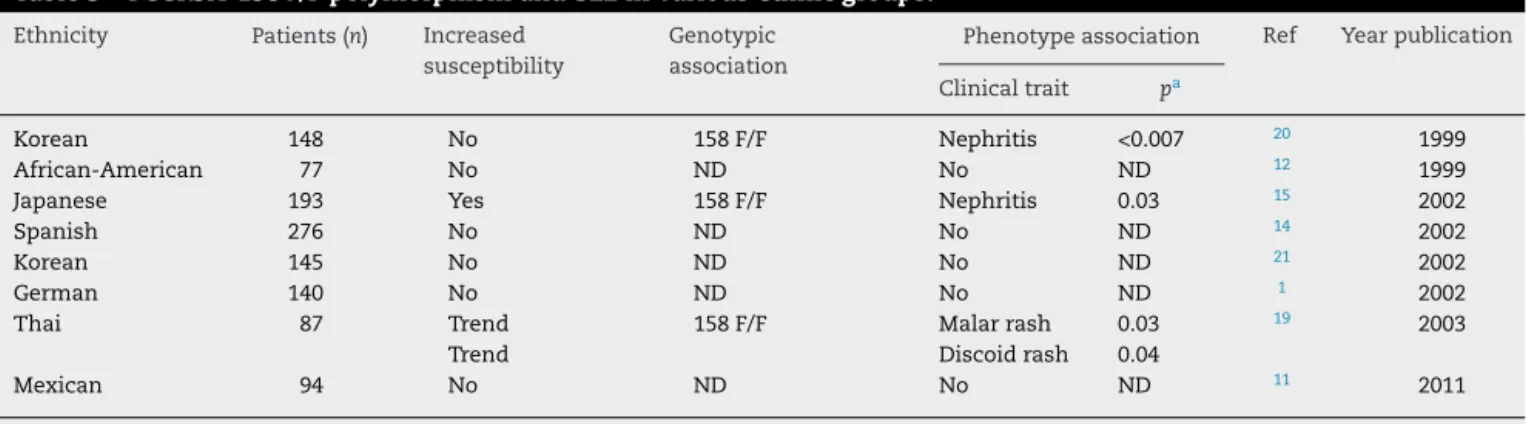
conceivablethatthedecreasedbindingcapacityofthe158F allelewould beassociatedwithimmunecomplex-mediated diseases.Infact,anincreasedsusceptibilitytoSLEinFCGR3A 158F/Findividualshasbeenreportedinsomeethnicgroups.3 However,the literatureiscontroversialregardingthis asso-ciation. Among Japanese, homozygosis for the 158F allele contributed to SLEsusceptibility,15 but in the Thai popula-tion,onlyatendencytoassociationwasfoundbetweentheFF genotypeandSLEsusceptibility.25Noassociationwasfound between the 158V/F polymorphism and SLE in Spanish,14 African-American,12 andMexicanindividuals.11 InKoreans, according toSalmon et al.,26 homozygosis forthe F allele constituted arisk factor forlupus nephritis,incontrast to theresultsofLeeandcolleagues,whofoundnoassociation betweenthispolymorphismandSLEinthisethnicgroup.27In theGermanpopulation,althoughtheFc␥RIIIapolymorphism didnotconfersusceptibilitytoSLE,thepresenceoftheFallele was associatedwithclinicalmanifestations,prognosis, and courseofdisease(Table5).1
In our study the heterozygousgenotype (VF)was more prevalentinSLEpatients,andasexpectedthiscausedno dif-ference inthe allelicdistribution between SLEand control groups. Thereasonforahigherfrequencyofthe heterozy-gous 158V/F genotype in SLE patients is not readily clear. Itcouldberelatedtocopynumbervariationand itmaybe hypothesizedthatanintermediateaffinitystateinthepool ofFc␥RIIIareceptors,asprovidedbythecoexistenceofhigh avidity(158V)andlowavidity(158F)FCGR3Avariants,would setanimmunecomplex-clearancescenariofavorabletothe developmentofimmunecomplex-mediateddiseasesinthis ethnic set-up. Experimental data are required to test this hypothesis.
Table5–FCGR3A-158V/FpolymorphismandSLEinvariousethnicgroups.
Ethnicity Patients(n) Increased susceptibility
Genotypic association
Phenotypeassociation Ref Yearpublication
Clinicaltrait pa
Korean 148 No 158F/F Nephritis <0.007 20 1999
African-American 77 No ND No ND 12 1999
Japanese 193 Yes 158F/F Nephritis 0.03 15 2002
Spanish 276 No ND No ND 14 2002
Korean 145 No ND No ND 21 2002
German 140 No ND No ND 1 2002
Thai 87 Trend 158F/F Malarrash 0.03 19 2003
Trend Discoidrash 0.04
Mexican 94 No ND No ND 11 2011
ND,notdetermined. a Chi-squaretest.
WithrespecttoSLEclinicalmanifestations,Wuand col-leaguesfoundthattherewasastrongassociationbetweenthe FFgenotypeandlupusnephritisinAmericansfromdiverse geneticbackground,9 similarlytowhatwasobservedinthe KoreanpopulationbySalmonetal.,in1999.26However,even in Americans with varied genetic background the role of FCGR3Apolymorphism inSLEphenotypeisnotclear,since Alarcon and colleagues found that homozygosis forthe V allele(FCGR3A*GG) wasasignificant predictor ofend-stage renaldiseaseamongSLEpatientswithkidneydisease.28The association ofthe 158Fallele with lupusnephritis9,26 and theassociationoftheVallelewithend-stagerenaldisease28 suggestthat otherstillunknownfactors mayinfluencethe development and outcome of renal manifestations inSLE. Association between the VV genotype and history of CNS involvementhasnotbeenreportedbyotherauthors.This orig-inalfindingisintriguing,butoneshouldkeepinmindthat, duetothelownumberofhomozygousVVSLEpatientsinthe presentseries,thisassociationmustberegardedas prelimi-nary.
In conclusion, this original analysis of FCGR3A 158V/F polymorphism inBrazilianSLE patientsshowed no associ-ation between any ofthe alleles and susceptibility toSLE, but disclosed a remarkably higher frequency of the het-erozygous158V/Fgenotype inSLEpatients ascomparedto healthycontrols.Inaddition,wehavenotconfirmedthe pre-viouslyreportedassociationbetweenthe158Falleleandlupus nephritisin ourseries, but wedidfind anintriguing asso-ciationbetweenthe158Valleleandcentralnervoussystem involvement.Thepresentfindingssupporttheimpactofthe genetic variability ofthe Fc␥receptors in general and the Fc␥RIIIainparticularonthesusceptibilityandphenotypeof systemiclupuserythematosus.Ourpreliminaryresults war-rantfurtherstudiestoconfirmandinvestigatetheroleofthe family ofFc␥ receptorsinthe pathophysiologyofsystemic lupuserythematosus.
Funding
This study was supported by grant 2008/50213-2 from Fundac¸ão de Amparo à Pesquisa do Estado de São Paulo
(FAPESP).MarcelleGreccowassupportedbyCoordenac¸ãode Aperfeic¸oamentodePessoaldeNívelSuperior(CAPES).Luís Eduardo Coelho Andrade receives a grant (#476356/2008-3) from the Brazilian Council for Research and Development (CNPq)agency.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.MangerK,ReppR,JansenM,GeisselbrechtM,WassmuthR, WesterdaalNA,etal.FcgammareceptorIIa,IIIa,andIIIb polymorphismsinGermanpatientswithsystemiclupus erythematosus:associationwithclinicalsymptoms.Ann RheumDis.2002;61:786–92.
2.SalmonJE.Abnormalitiesinimmunecomplexclearanceand Fcreceptorfunction.In:WallaceDJ,HahnBH,editors.Dubois’ lupuserythematosus.7thed.Philadelphia:Lippincott Williams&Wilkins;2007.p.191–213.
3.LiX,PtacekTS,BrownEE,EdbergJC.Fcgammareceptors: structure,functionandroleasgeneticriskfactorsinSLE. GenesImmun.2009;10:380–9.
4.GessnerJE,HeikenH,TammA,SchmidtRE.TheIgGFc receptorfamily.AnnHematol.1998;76:231–48. 5.TakaiT.Rolesofreceptorsinautoimmunity.NatRev
Immunol.2002;2:580–92.
6.PascualV,FarkasL,BanchereauJ.Systemiclupus
erythematosus:allroadsleadtotypeIinterferons.CurrOpin Immunol.2006;18:676–82.
7.WiedemanAE,SanterDM,YanW,MiescherS,KäsermannF, ElkonKB.Contrastingmechanismsofinterferon-␣inhibition byintravenousimmunoglobulinafterinductionbyimmune complexesversusToll-likereceptoragonists.Arthritis Rheum.2013;65:2713–23.
8.BournazosS,WoofJM,HartSP,DransfieldI.Functionaland clinicalconsequencesofFcreceptorpolymorphicandcopy numbervariants.ClinExpImmunol.2009;157:244–54. 9.WuJ,EdbergJC,RedechaPB,BansalV,GuyrePM,ColemanK,
etal.AnovelpolymorphismofFcgammaRIIIa(CD16)alters receptorfunctionandpredisposestoautoimmunedisease.J ClinInvest.1997;100:1059–70.
bindingofIgGbynaturalkillercellFcgammaRIIIa, independentlyoftheFcgammaRIIIa-48L/R/Hphenotype. Blood.1997;90:1109–14.
11.Brambila-TapiaAJ,Gámez-NavaJI,González-LópezL, Sandoval-RamírezL,Medína-DíazJ,MaldonadoM,etal. FCGR3AV(176)polymorphismforsystemiclupus erythematosussusceptibilityinMexicanpopulation. RheumatolInt.2011;31:1065–8.
12.OhM,PetriMA,KimNA,SullivanKE.Frequencyofthe Fc␥RIIIA-158FalleleinAfricanAmericanpatientswith systemiclupuserythematosus.JRheumatol.1999;26: 1486–9.
13.SeligmanVA,SuarezC,LumR,IndaSE,LinD,LiH,etal.The FcgammareceptorIIIA-158Falleleisamajorriskfactorfor thedevelopmentoflupusnephritisamongCaucasiansbut notnon-Caucasians.ArthritisRheum.2001;44:618–25. 14.González-EscribanoMF,AguilarF,Sánchez-RománJ,
Nú ˜nez-RoldánA.FcgammaRIIA,FcgammaRIIIAand FcgammaRIIIBpolymorphismsinSpanishpatientswith systemiclupuserythematosus.EurJImmunogenet. 2002;29:301–6.
15.KyogokuC,DijstelbloemHM,TsuchiyaN,HattaY,KatoH, YamaguchiA,etal.Fcgammareceptorgenepolymorphisms inJapanesepatientswithsystemiclupuserythematosus: contributionofFCGR2Btogeneticsusceptibility.Arthritis Rheum.2002;46:1242–54.
16.ChuZT,TsuchiyaN,KyogokuC,OhashiJ,QianYP,XuSB,etal. AssociationofFcgammareceptorIIbpolymorphismwith susceptibilitytosystemiclupuserythematosusinChinese:a commonsusceptibilitygeneintheAsianpopulations.Tissue Antigens.2004;63:21–7.
17.HochbergMC.UpdatingtheAmericancollegeof rheumatologyrevisedcriteriafortheclassificationof systemiclupuserythematosus.ArthritisRheum. 1997;40:1725.
18.LaitinenJ,SamarutJ,HölttäE.Anontoxicandversatile proteinsalting-outmethodforisolationofDNA. Biotechniques.1994;17:316,318,320–2.
19.SiriboonritU,TsuchiyaN,SirikongM,KyogokuC, BejrachandraS,SuthipinittharmP,etal.Associationof
FcgammareceptorIIbandIIIbpolymorphismswith susceptibilitytosystemiclupuserythematosusinThais. TissueAntigens.2003;61:374–83.
20.SalmonJE,NgS,YooDH,KimTH,KimSY,SongGG.Altered distributionofFcgammareceptorIIIAallelesinacohortof Koreanpatientswithlupusnephritis.ArthritisRheum. 1999;42:818–9.
21.LeeEB,LeeYJ,BaekHJ,KangSW,ChungES,ShinCH,etal. FcgammareceptorIIIApolymorphisminKoreanpatientswith systemiclupuserythematosus.RheumatolInt.2002;21:222–6. 22.LeeS,KasifS,WengZ,CantorCR.Quantitativeanalysisof
singlenucleotidepolymorphismswithincopynumber variation.PLoSOne.2008;3:e3906.
23.SchaschlH,AitmanTJ,VyseTJ.Copynumbervariationinthe humangenomeanditsimplicationinautoimmunity.Clin ExpImmunol.2009;156:12–6.
24.BreunisWB,vanMirreE,BruinM,GeisslerJ,deBoerM,Peters M,etal.CopynumbervariationoftheactivatingFCGR2C genepredisposestoidiopathicthrombocytopenicpurpura. Blood.2008;111:1029–38.
25.WillcocksLC,LyonsPA,ClatworthyMR,RobinsonJI,YangW, NewlandSA,etal.CopynumberofFCGR3B,whichis associatedwithsystemiclupuserythematosus,correlates withproteinexpressionandimmunecomplexuptake.JExp Med.2008;205:1573–82.
26.ZhouXJ,LvJC,BuDF,YuL,YangYR,ZhaoJ,etal.Copy numbervariationofFCGR3AratherthanFCGR3BandFCGR2B isassociatedwithsusceptibilitytoanti-GBMdisease.Int Immunol.2010;22:45–51.
27.AlarcónGS,McGwinGJr,PetriM,Ramsey-GoldmanR,Fessler BJ,ViláLM,etal.Timetorenaldiseaseandend-stagerenal diseaseinPROFILE:amultiethniclupuscohort.PLoSMed. 2006;3:e396.
28.Pons-EstelBA,CatoggioLJ,CardielMH,SorianoER,Gentiletti S,VillaAR,etal.,onbehalfoftheGrupoLatinoamericanode EstudiodelLupus(GLADEL).TheGLADELmultinationalLatin Americanprospectiveinceptioncohortof1,214patientswith systemiclupuserythematosus:ethnicanddisease