w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Association
of
PDCD1
polymorphism
to
systemic
lupus
erythematosus
and
rheumatoid
arthritis
susceptibility
Luisa
Matos
do
Canto
a,1,
Ticiana
Della
Justina
Farias
a,1,
Mayara
Delagnelo
Medeiros
a,
Cíntia
Callegari
Coêlho
a,
Aline
Fernanda
Rodrigues
Sereia
a,
Lia
Kubelka
Fernandes
de
Carlos
Back
a,
Filipe
Martins
de
Mello
b,
Adriana
Fontes
Zimmermann
c,
Ivânio
Alves
Pereira
c,
Ilíada
Rainha
de
Souza
a,∗aUniversidadeFederaldeSantaCatarina,DepartamentodeBiologiaCelular,EmbriologiaeGenética,Florianópolis,SC,Brazil bUniversidadedoEstadodeSãoPaulo,FaculdadedeMedicina,Servic¸odeReumatologia,SãoPaulo,SP,Brazil
cUniversidadeFederaldeSantaCatarina,HospitalUniversitário,DivisãodeReumatologia,Florianópolis,SC,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received4July2014 Accepted6May2015
Availableonline23November2015
Keywords:
Rheumatoidarthritis
Systemiclupuserythematosus Autoimmunity
PDCD1gene
PD1.3polymorphism
a
b
s
t
r
a
c
t
Objective:Thisstudyaimstoanalyzetherelationshipofprogrammedcelldeath1(PDCD1) genepolymorphism(PD1.3G/A–rs11568821)withfeaturesofsystemiclupuserythematosus (SLE)andrheumatoidarthritis(RA)inaSouthernBrazilianpopulation.
Methods:Polymerasechainreaction-restrictionfragmentlengthpolymorphism(PCR-RFLP) wasperformedin95SLEand87RApatientsand128controlgroupindividualsfromSanta Catarina,SouthernBrazil.TheHardy–Weinbergequilibrium(HWE)test,andoddsratio(OR) wereanalyzed,consideringCI95%andp≤0.05.
Results:ThePD1.3Aallelefrequencieswere0.095(SLE),0.115(RA)and0.078(controls).The genotypes ofthecontrolgroupwereinHWE,while thoseofSLEandRApatientswere not.However,wefoundnoassociationbetweenPD1.3polymorphismandtheSLEorRA susceptibility,norclinicalorepidemiologicaldata.
Conclusion: TherewasnosignificantassociationbetweenPD1.3polymorphismandSLEor RAsusceptibilityinthisSouthernBrazilianpopulation.
©2015ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Associac¸ão
entre
o
polimorfismo
do
gene
PDCD1
e
a
susceptibilidade
ao
lúpus
eritematoso
sistêmico
e
à
artrite
reumatoide
Palavras-chave:
Artritereumatoide
Lúpuseritematososistêmico
r
e
s
u
m
o
Objetivo:Esteestudotevecomoobjetivoanalisararelac¸ãoentreopolimorfismodogene
PDCD1 (Programmed cell death1)(PD1.3G/A –rs11568821)com caraterísticas dolúpus eritematososistêmico(LES)edaartritereumatoide(AR)emumapopulac¸ãodosuldoBrasil.
∗ Correspondingauthor.
E-mail:[email protected](I.R.Souza).
1 Bothoftheseauthorsequallycontribuedtothiswork.
http://dx.doi.org/10.1016/j.rbre.2015.07.008
Autoimunidade GenePDCD1
PolimorfismoPD1.3
Métodos: AtécnicadePCR-RFLP(PolymeraseChainReaction-RestrictionFragmentLenght Poly-morphism)foiutilizadaparaanalisaramostrasde95pacientescomLESe87comARe128 indivíduosdogrupocontroledeSantaCatarina,suldoBrasil.Foianalisadaa probabili-dadedeequilíbriodeHardy–Weinberg(EHW)eooddsratio(OR),considerandoumIC95%e
p≤0.05.
Resultados:AsfrequênciasalélicasPD1.3Aforamde0,095(LES),0,115(AR)e0,078(controles). OsgenótiposdogrupocontroleestavamemEHW,enquantoaquelesdospacientescomLESe ARnãoestavam.Noentanto,nãofoiencontradanenhumaassociac¸ãoentreopolimorfismo
PD1.3easusceptibilidadeaoLESouàAR,nemcomdadosclínicosouepidemiológicos.
Conclusão: Nãofoiencontradaassociac¸ãosignificativaentreopolimorfismoPD1.3ea sus-ceptibilidadeaoLESouàARnestapopulac¸ãodosuldoBrasil.
©2015ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Autoimmunerheumaticdiseasesshareclinicalfindingsand arecausedbymultiplefactorsincluding acomplexgenetic basiscoupledwithnon-geneticfactors,whichcontributein differentdegreesforeachaffectedindividual.1Genetic
poly-morphismsofthehumangenomehavebeeninvestigatedand
newevidenceofgeneticcontributiontorheumaticdiseases
hasbeendiscovered.Amongautoimmunediseases,systemic
lupuserythematosus(SLE)andrheumatoidarthritis(RA),have beenthemaintargetsofgeneticvariationstudies,oncethey representmultisystemdisorderswithawidespectrumof clin-icalmanifestations.1,2
SLE affects mainly women ofreproductive age, and its
major characteristic is the production of autoantibodies
againstnuclearantigens,asdoublestrandedDNA(dsDNA), ribonucleoproteins(RNP)andSmith(Sm)antigen;aswellas cytoplasmic,andcell-surfaceantigens.3Theseautoantibodies
depositonseveralorganscausinginflammationandleading tosymptomsthatcouldrangefromsubtletolife-threatening. Constitutional manifestations including fever, fatigue and weightlossmayoccur,aswellasjointpainduetoarthritis, malaranddiscoidrashes,photosensitivity,andinvolvement ofthecentralandperipheralnervoussystem,kidneys,heart andlungs.1Progressionofthediseaseisindividualand
het-erogeneous,sodifferentbiomarkershavebeensoughtinorder tounveildiseasesusceptibilityanddevelopmentaswellasto guidetherapeuticdecisions.4,5
RA pathogenesis is complex and results in chronic
inflammation of joints and, in many patients, systemic
complications, such as subcutaneous nodules, pulmonary
involvementandearlyatherosclerosis,thatmaybe challeng-ingregardingtreatment.6Inordertocometobetterprognosis
and outcomes in RA, the development of biomarkersthat
allowdiseasesub-categorizationareneeded.7Sofar,serologic
factorssuchasrheumatoidfactor(RF)andanti-citrullinated proteinautoantibodies(ACPA);and theacute inflammation markerC-reactiveprotein(CRP),havehelpedclassifyingRA clinicalphenotypes.8–11Rheumatoidfactorisanautoantibody
directedagainst the Fc portion ofIgG, and correlates with theseverityofthedisease12;whereastheACPAaredirected
againstcitrullinatedproteins,andcanalsohelptopredicta moresevereanderosivedisease.13
Although the etiology of SLE and RA are not well
established,itishypothesizedthatderegulatedlymphocyte activationplayanimportantroleinthebreakdownofimmune tolerance,leadingtoautoreactivity.2,14 Involvedinthis
pro-cesses,co-stimulatorymoleculesarecriticalforthebalance betweenTcellactivationandinhibition.15Amongthose,the
programmedcelldeath1(PD-1)isshowntobeanimportant moleculeinvolvedinprofoundlossofself-toleranceleading torapidlethalityassociatedwithlymphocyteinfiltrationin many organs.16Thisproteinisexpressedonthesurfaceof
T,Bandmyeloidcells,andisamemberoftheCD28family thatbelongstotheimmunoglobulinsuperfamilyandactsas aninhibitorymoleculeon Tcells,afterinteracting withits ligandsPDL-1andPDL-2(programmedcelldeath1ligand1 and 2).17 AfterinitialactivationofTcellinteractions,
PD-1-PD-LmaylimitautoreactiveTcellproliferationandcytokine production,whereasstimulatedbyantigensthePD-1 damp-ensTcellreceptor(TCR)signaling.Theamountofexpression ofPD-1andthedegreeofinvolvementbetweenthisprotein anditsligandsregulatethethresholdofTcellactivationand the amount ofcytokines produced.18,19 PD-1-deficientmice
develop spontaneous autoimmune diseases, indicating an
essentialfunctionofPD-1inthemechanismsoftolerance.20–23
PD-1 is encoded by the PDCD1 gene, located at 2q37.3
locus.AmongtheSNPsfoundwithinthisregion,thePD1.3G/A
(rs11568821) potentially represents a functional
polymor-phism associated with the transcriptional regulation of
PD-1.24ThePD1.3AallelealtersthebindingsiteofRUNX1(or
AML1)transcriptionfactor,locatedontheintron4enhancer region,whichcouldleadtoaberrantproteinexpression, sug-gesting amechanism fortheself-tolerance breakdown.25,26
Association studies correlated the presence of the allele
PD1.3AwithSLEinMexicanandScandinavianpopulations,25
and withdiabetesmellitus1andRAinDenmarkand
Swe-denrespectively.26,27 However,somepopulationsinAsiaare
non-polymorphicforthisgenomicregion,presentingonlythe
PD1.3G allele,28–30 whichemphasizesthediversity ofallelic
frequencyamongpopulations,andsupportsthenecessityto study theassociationofthisPDCD1 polymorphisminother localities.InBrazil,threestudieshaveevaluatedthe frequen-ciesofPD1.3polymorphism.Oneinpatientswithpemphigus foliaceus (also anautoimmunedisease),31insilica-exposed
workers,32andinacohortofpatientswithChagasdisease,33
Table1–Characteristicsofsystemiclupus erythematosus(SLE)andrheumatoidarthritis(RA) patientsandcontrolsfromSouthernBrazil.
SLE patientsn
RA patientsn
Controlsn
Female(%) 92(96.84) 75(86.21) 123(96.09) Meanage(SD) 37,35(±12,16) 54.42(±13.33) 47,38(±15.04)
SD,standarddeviation.
Hence, through this study we intended to evaluate the frequencyofPD1.3polymorphisminaSouthernBrazilian pop-ulationanditsrelationshiptoSLEandRAsusceptibility.
Methods
Altogether,95SLEpatients,87RApatientsand128control sub-jectsparticipatedonthisstudy,whichwasapprovedbythe CommitteeonEthicsoftheFederalUniversityofSanta Cata-rina(UFSC)(CEP/UFSC–casenumber172/06),afterinformed consentwasobtainedfromallpatientsandcontrolssubjects. Womenmadeup96.84%ofSLEpatients,86.10%ofRApatients and 96.09%ofcontrols.Themean age ofSLEpatientswas 37.35±12.16years,ofRApatientswas54.42±13.33yearsand ofcontrol group was 47.38±15.04 years (Table 1). Patients were admittedatthe HospitalUniversitário Professor Poly-doroErnanideSãoThiago,Florianópolis,Brazil,from2007to 2009,anddiagnosedaccordingtothe1987AmericanCollege
ofRheumatologycriteria. Thecontrolgroupwascomposed
ofhealthy volunteerswithout personalorfamilyhistory of autoimmunediseases.Familial,epidemiologicalandclinical datafromindividuals wereobtainedbyquestionnairesand medicalrecords. Regarding clinical data, we evaluated SLE patient’smedicalchartrecordsofarthritis,photo-sensibility, Raynaud’sphenomenon,andnephritis,whichwerethe recur-rentclinicalmanifestationinthisgroup.ForRApatients,we consideredrheumatoidfactor(RF)positivity(>20IU/ml),and levelsofC-reactiveprotein(CRP) abovethereference value (>5mg/l)asthelaboratorialmanifestationstobeassociated withthealleles.
Whole blood samples were obtained from SLE and RA
patientsandfromcontrolsubjects.TheDNAwasextracted
usingthephenol–chloroformtechnique.34ThePD1.3A(PDCD1)
allelewasdetectedbypolymerasechainreactionrestriction fragmentlengthpolymorphism(PCR-RFLP).35ThePCR
prod-uctof180bpwas digestedbyPstI restrictionendonuclease (BioLabsInc.,NewEngland),accordingtothemanufacturer instructions.Allexperimentswereperformedwithnegative andpositiveinternalcontrolspreviouslygenotypedat Labo-ratóriodeGenéticaMolecularHumana–UFPR.Theproductof digestionwasstainedwithGelRed®solutionandsubjectedto
electrophoresisona3%agarosegel.DNAwasvisualizedwith aphotographedgeldocumentationsystem(MiniBISProDNR). Thegenotypewasclassifiedaccordingtothesizeofthe gen-eratedfragments(GG–180bp;GA–180bp,150bpand30bp;
AA–150bpand30bp).
Hardy–Weinbergequilibrium(HWE)wastestedusingthe
2 test. Alleleand genotypefrequencieswereestimatedby directcounting.Alleleandgenotypefrequencieswere com-paredbetweenpatientsandcontrolsbyFisherexacttestusing SPSS(version20.0;SPSSInc.,Chicago,IL),whichwasalsoused tocalculatetheoddsratio(OR)inordertodeterminethe asso-ciationofthePD1.3Aalleleandthestudieddiseases,aswell as its association to poorprognosis factors of SLEand RA patients. Apvalueof0.05was adoptedasthelimitof sig-nificanceforalltests.
Results
ThealleleandgenotypefrequenciesofPD1.3polymorphisms
found amongthe groups are shown in Table2. The
geno-typedistributioninthecontrolgroupwasinHWE(2(1)=2.24,
p=0.13),butthedistributionsobservedinSLEandRApatients werenot(2(1)=6.60,p=0.01forSLEand2(1)=9.02,p<0.001
forRA).Nevertheless,noassociationwasfoundregardingthe allelesorgenotypesandbothdiseases(p>0.05)(Table2).
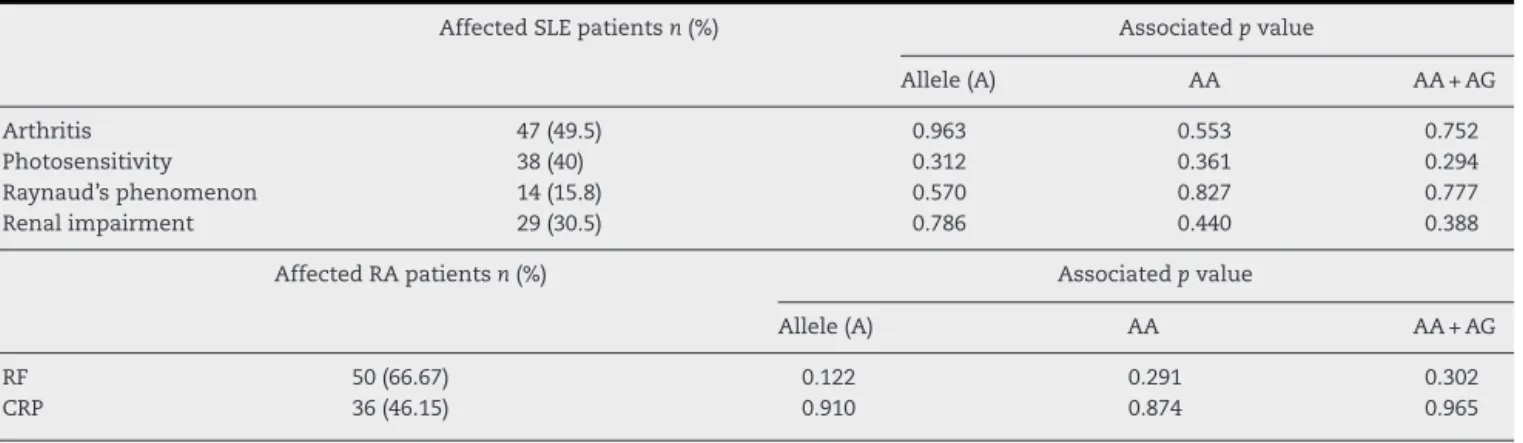
AmongSLEpatients,49.5%hadarthritis,40.0%complained of photosensitivity, 15.8% experienced the Raynaud’s phe-nomenonand30.5%presentedrenalimpairment.Association betweentheseclinicalfactorsandPD1.3allelesandgenotypes wereanalyzed,butnosignificantresultswerefound(Table3). LessthanhalfofRApatients(46.15%)presentedhighlevel ofCRP,and66.67%hadRFpositivity.However,thosefactors werenotassociatedwiththepresenceofPD1.3Aalleleeither inhomozygosisorheterozygosis(Table3).
Table2–AlleleandgenotypefrequenciesofPD1.3polymorphismobservedinsystemiclupuserythematosus(SLE)and rheumatoidarthritis(RA)patientsandcontrols.Hardy–Weinbergequilibrium(HWE)valuesforgenotypicdistribution, andassociationanalysisbetweenthediseasesandthePD1.3(G/A)polymorphisminsamplesofpatientsandunaffected controlsubjectsoftheBrazilianpopulationwerecalculated.
SLE pvalue RA pvalue Controlsn=128
n=95 n=87
AlleleG 0.905 (Ref.) 0.885 (Ref.) 0.922
AlleleA 0.095 0.661 0.115 0.364 0.078
GG 0.842 (Ref.) 0.816 (Ref.) 0.859
GA 0.126 0.940 0.138 0.715 0.125
AA 0.032 0.755 0.046 0.206 0.016
HWE(pvalue) 2(1)=6.60(0.010) 2(1)=9.02(<0.001) 2(1)=2.24(0.130)
Table3–Clinicalfeaturespresentinsystemiclupuserythematosus(SLE)andrheumatoidarthritis(RA)patients,and theirassociationtoPD1.3polymorphism.
AffectedSLEpatientsn(%) Associatedpvalue
Allele(A) AA AA+AG
Arthritis 47(49.5) 0.963 0.553 0.752
Photosensitivity 38(40) 0.312 0.361 0.294
Raynaud’sphenomenon 14(15.8) 0.570 0.827 0.777
Renalimpairment 29(30.5) 0.786 0.440 0.388
AffectedRApatientsn(%) Associatedpvalue
Allele(A) AA AA+AG
RF 50(66.67) 0.122 0.291 0.302
CRP 36(46.15) 0.910 0.874 0.965
RF,rheumatoidfactor;CRP,C-reactiveprotein.
Discussion
ForthefirsttimeinBrazil,PDCD1genewasconsidereda candi-dateforsusceptibilitytosystemiclupuserythematosus(SLE) andtorheumatoid arthritis(RA). Associationsbetweenthe SNPPD1.3Aandclinicalandlaboratorialmanifestationswere tested,findingnostatisticallysignificantresults.
OncegenotypefrequenciesofSLEandRApatientswere notinHardy–Weinbergequilibrium(Table3),divergingfrom thecontrolgroup,aputativeassociationwiththesediseases wasinvestigated.ThefrequencyofAAgenotypewasverylow inallgroups(0.032inSLE,0.046inRAand0.016incontrols)as shownbyothercase–controlstudiesindifferentpopulations, whereAAfrequencieswereallbelow0.05.31,33,35–44One
Ira-niancohort,however,hasshownAAgenotypefrequenciesof 0.20incontrolsand0.44inpatientswithColorectalCancer (CCR),revealingaswell,an associationbetweenthis geno-typeandCCR(p=0.0005).45InBrazil,thefrequencyoftheAA
genotypewas alsolowaccordingtothreedifferentcohorts
involving patients with Chagas disease (0.03 and 0.01 in
controls),33pemphigusfoliaceus(0.007and0.01incontrols),31
andreaching0%inagroupofsilica-exposedworkers(0.03in controls).32Interestingly,somepopulationscarrythe minor
allele,but nohomozygous descriptionwas found, present-ingonlyGGandAGindividuals.Yet,theanalyzedgenotypes showednostatisticallysignificantORvaluewhenconsidering theriskofdevelopingSLEorRAinourstudy.35,46–48
AssociationsofthePD1.3Aalleletodiseasedevelopment
have been increasingly investigated, not only in SLE and
RA patients,25,26,28,29,35–37,46,49–55 but also in other
autoim-muneand chronicinflammatorydiseases suchasDiabetes
Mellitus type I (T1D),27,38,42 Graves and Addison disease,39
Ankylosing spondylitis,44 and Myasthenia Gravis,41 as well
asinotherconditionsasCCR,45andsilicaexposedworkers
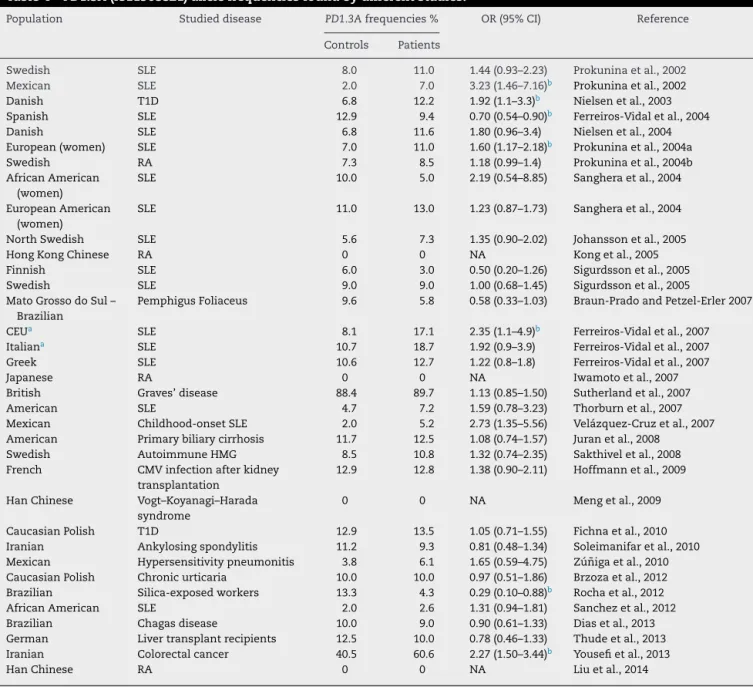
(Table4).32ThePD1.3Aallelefrequencyhighlydiffersamong
populationsworldwide,threeChinesestudiesrelatedtoRA
andVogt–Koyanagi–HaradaSyndromefoundnoallele
varia-tion intheir population,28,30,55 whichwas alsoobserved in
Japaninasimilarstudy.29Europeanstudiesshowthe
pres-enceofthePD1.3polymorphism,yetassociationtodiseases variesamongstudies.AnassociationofPD1.3AtoSLEwas
demonstrated by Prokunina et al.25,26 in European women
andMexicans,andbyFerreiros-Vidaletal.51inSLEpatients
from Germany,Czech Republic and Hungary. Nevertheless,
Ferreiros-Vidal et al. have previously shown a reversal of patternsinaSpanishcohort,withdecreasedriskofSLE devel-opmentinPD1.3Acarriers.50RApatientswerealsogenotyped
forPDCD1rs11568821polymorphismbyfewgroups,28,29,36,55
andasmentionedpreviously,ChineseandJapanesecohorts carriedsolelythePD1.3Gallele.ASwedishstudywastheonly onetopresentdataonRAandrs11568821polymorphism,but associationbetweenthediseaseandalleleorgenotypeswas notdemonstrated.36Nonetheless,thesamegroupshowedan
associationofPD1.3AandRApatientsnegativeforRF.Inthe presentstudywecouldnotfindanyassociationbetweenRF positivityorhighlevelsofCRPandtheallelesorgenotypes investigated.
SLEpatientswerealsoinquiredaboutclinical manifesta-tions asarthritis,photosensitivity, Raynaud’sphenomenon,
and renal involvement. However, we found no association
between PD1.3 alleles or genotypes and these
manifesta-tions.Thorburnetal.53evaluatedtheroleoffourPDCD1SNPs
(PD1.1A,PD1.3A,PD1.5TandPD1.6A)andSLEnephritis, arthri-tis, antiphospholipid antibody (APA), and double-stranded DNApositivity,findingnoassociationofPD1.3Aalleleandits associatedhaplotypeandanyclinicalphenotype.The occur-renceofAPAinSLEpatientswasalsoanalyzedbySanghera et al.35 unraveling a protection of PD1.3A carriers against
APA inboth SLE(OR=0.57; 95% CI:0.32–1.01) and controls (OR=0.40; 95% CI:0.19–0.82). Prokunina et al.,26 Johansson
etal.,37andNielsenetal.49evaluatedrenalmanifestationsin
SLEpatients.Thefirstandsecondstudiesshowedan associa-tionbetweenthePD1.3Aalleleandrenaldisordersinpatients withSLEfromSweden(OR=2.6;95%CI:1.4–4.8,andOR=2.62; 95%CI:1.28–5.35,respectively);andthethirdonedidnotfind anassociationoflupusnephropathyandtheminoralleleof
PD1.3.AsforRA,neitherRFnorCRPwasassociatedtoPD1.3A
allele presenceeither in homozygosis or heterozygosis, as opposedtowhatwasfoundbyProkuninaetal.26
Table4–PD1.3A(rs11568821)allelefrequenciesfoundbydifferentstudies.
Population Studieddisease PD1.3Afrequencies% OR(95%CI) Reference
Controls Patients
Swedish SLE 8.0 11.0 1.44(0.93–2.23) Prokuninaetal.,2002
Mexican SLE 2.0 7.0 3.23(1.46–7.16)b Prokuninaetal.,2002
Danish T1D 6.8 12.2 1.92(1.1–3.3)b Nielsenetal.,2003
Spanish SLE 12.9 9.4 0.70(0.54–0.90)b Ferreiros-Vidaletal.,2004
Danish SLE 6.8 11.6 1.80(0.96–3.4) Nielsenetal.,2004
European(women) SLE 7.0 11.0 1.60(1.17–2.18)b Prokuninaetal.,2004a
Swedish RA 7.3 8.5 1.18(0.99–1.4) Prokuninaetal.,2004b
AfricanAmerican (women)
SLE 10.0 5.0 2.19(0.54–8.85) Sangheraetal.,2004
EuropeanAmerican (women)
SLE 11.0 13.0 1.23(0.87–1.73) Sangheraetal.,2004
NorthSwedish SLE 5.6 7.3 1.35(0.90–2.02) Johanssonetal.,2005
HongKongChinese RA 0 0 NA Kongetal.,2005
Finnish SLE 6.0 3.0 0.50(0.20–1.26) Sigurdssonetal.,2005
Swedish SLE 9.0 9.0 1.00(0.68–1.45) Sigurdssonetal.,2005
MatoGrossodoSul– Brazilian
PemphigusFoliaceus 9.6 5.8 0.58(0.33–1.03) Braun-PradoandPetzel-Erler2007
CEUa SLE 8.1 17.1 2.35(1.1–4.9)b Ferreiros-Vidaletal.,2007
Italiana SLE 10.7 18.7 1.92(0.9–3.9) Ferreiros-Vidaletal.,2007
Greek SLE 10.6 12.7 1.22(0.8–1.8) Ferreiros-Vidaletal.,2007
Japanese RA 0 0 NA Iwamotoetal.,2007
British Graves’disease 88.4 89.7 1.13(0.85–1.50) Sutherlandetal.,2007
American SLE 4.7 7.2 1.59(0.78–3.23) Thorburnetal.,2007
Mexican Childhood-onsetSLE 2.0 5.2 2.73(1.35–5.56) Velázquez-Cruzetal.,2007 American Primarybiliarycirrhosis 11.7 12.5 1.08(0.74–1.57) Juranetal.,2008
Swedish AutoimmuneHMG 8.5 10.8 1.32(0.74–2.35) Sakthiveletal.,2008 French CMVinfectionafterkidney
transplantation
12.9 12.8 1.38(0.90–2.11) Hoffmannetal.,2009
HanChinese Vogt–Koyanagi–Harada syndrome
0 0 NA Mengetal.,2009
CaucasianPolish T1D 12.9 13.5 1.05(0.71–1.55) Fichnaetal.,2010
Iranian Ankylosingspondylitis 11.2 9.3 0.81(0.48–1.34) Soleimanifaretal.,2010 Mexican Hypersensitivitypneumonitis 3.8 6.1 1.65(0.59–4.75) Zú ˜nigaetal.,2010 CaucasianPolish Chronicurticaria 10.0 10.0 0.97(0.51–1.86) Brzozaetal.,2012 Brazilian Silica-exposedworkers 13.3 4.3 0.29(0.10–0.88)b Rochaetal.,2012
AfricanAmerican SLE 2.0 2.6 1.31(0.94–1.81) Sanchezetal.,2012
Brazilian Chagasdisease 10.0 9.0 0.90(0.61–1.33) Diasetal.,2013
German Livertransplantrecipients 12.5 10.0 0.78(0.46–1.33) Thudeetal.,2013 Iranian Colorectalcancer 40.5 60.6 2.27(1.50–3.44)b Yousefietal.,2013
HanChinese RA 0 0 NA Liuetal.,2014
OR,oddsratio;CI,confidenceinterval;SLE,systemiclupuserythematosus;RA,rheumatoidarthritis;T1D,type1diabetes;NA,notavailable; HMG,humanmyastheniagravis.
a CollectionsofsamplesfromGermany,theCzechR.andHungaryweregroupedasCEU;collectionsfromMilan,RomeandNapleswere
groupedasItaly;collectionsfromGreecewereconsideredbytheirown(aspresentedbyFerreiros-Vidaletal.51). b p<0.05statisticallysignificant.
Funding
Thisstudy was supportedby the National Councilfor Sci-entificandTechnologicalDevelopment(CNPq),Coordination
ofImprovementofHigherEducationPersonnel(CAPES)and
FoundationtoSupportScientificResearchoftheStateofSanta Catarina(FAPESC-Fundac¸ãodeAmparoàPesquisaeInovac¸ão doEstadodeSantaCatarina).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Theauthors wishtothankespeciallythe patientsfortheir cooperationandpatience,andallcolleaguesthatcontributed to thiswork directly or indirectly. Wealsoappreciated the kindnessofDr.MariaLuizaPetzel-Erler,headofLaboratório deGenéticaMolecularHumana–UFPR,forsharingtheir geno-typecontrols.
r
e
f
e
r
e
n
c
e
s
2. Wahren-HerleniusM,DörnerT.Immunopathogenic mechanismsofsystemicautoimmunedisease.Lancet. 2013;382:819–31.
3. GrammatikosAP,TsokosGC.Immunodeficiencyand autoimmunity:lessonsfromsystemiclupuserythematosus. TrendsMolMed.2012;18:101–8.
4. AhearnJM,LiuC-C,KaoAH,ManziS.Biomarkersforsystemic lupuserythematosus.TranslRes.2012;159:326–42.
5. MurphyG,LisnevskaiaL,IsenbergD.Systemiclupus erythematosusandotherautoimmunerheumaticdiseases: challengestotreatment.Lancet.2013;382:809–18.
6. KlareskogL,CatrinaAI,PagetS.Rheumatoidarthritis.Lancet. 2009;373:659–72.
7. BaxM,vanHeemstJ,HuizingaTWJ,ToesREM.Geneticsof rheumatoidarthritis:whathavewelearned?
Immunogenetics.2011;63:459–66.
8. daMotaLMH,dosSantosNetoLL,BurlingameR,MénardHA, LaurindoIMM.Laboratorycharacteristicsofacohortof patientswithearlyrheumatoidarthritis.RevBrasReumatol. 2010;50:375–88.
9. RhodesB,FürnrohrBG,VyseTJ.C-reactiveproteinin rheumatology:biologyandgenetics.NatRevRheumatol. 2011;7:282–9.
10.NielsenS,BojesenS.Elevatedrheumatoidfactorandlong termriskofrheumatoidarthritis:aprospectivecohortstudy. BMJBrMed.2012;5244:1–9.
11.GoldmanK,GertelS,AmitalH.Anti-citrullinatedpeptide antibodiesismorethananaccuratetoolfordiagnosisof rheumatoidarthritis.IsrMedAssocJ.2013;15:516–9.
12.Habash-BseisoDE,YaleSH,GlurichI,GoldbergJW.Serologic testinginconnectivetissuediseases.ClinMedRes. 2005;3:190–3.
13.vanGaalenFA,Linn-RaskerSP,vanVenrooijWJ,deJongBA, BreedveldFC,VerweijCL,etal.Autoantibodiestocyclic citrullinatedpeptidespredictprogressiontorheumatoid arthritisinpatientswithundifferentiatedarthritis:a prospectivecohortstudy.ArthritisRheum.2004;50:709–15.
14.deSouzaAWS,MesquitaJúniorD,AraújoJAP,CatelanTTT, CruvinelWDM,AndradeLEC,etal.Immunesystem.PartIII: Thedelicatebalanceoftheimmunesystembetween toleranceandautoimmunity.RevBrasReumatol. 2010;50:665–79.
15.ThangaveluG,SmolarchukC,AndersonCC.Co-inhibitory molecules:Controllingtheeffectorsorcontrollingthe controllers?SelfNonself.2010;1:77–88.
16.ThangaveluG,ParkmanJC,EwenCL,UwieraRRE,BaldwinTA, AndersonCC.Programmeddeath-1isrequiredforsystemic self-toleranceinnewlygeneratedTcellsduringthe establishmentofimmunehomeostasis.JAutoimmun. 2011;36:301–12.
17.KronerA,MehlingM,HemmerB,RieckmannP,ToykaKV, MäurerM,etal.PD-1polymorphismisassociatedwith diseaseprogressioninmultiplesclerosis.AnnNeurol. 2005;58:50–7.
18.SharpeAH,WherryEJ,AhmedR,FreemanGJ.Thefunctionof programmedcelldeath1anditsligandsinregulating autoimmunityandinfection.NatImmunol.2007;8:239–45.
19.WeiF,ZhongS,MaZ,KongH,MedvecA,AhmedR,etal. StrengthofPD-1signalingdifferentiallyaffectsT-celleffector functions.ProcNatlAcadSciUSA.2013;110:E2480–9.
20.NishimuraH,MinatoN,NakanoT,HonjoT.Immunological studiesonPD-1deficientmice:implicationofPD-1asa negativeregulatorforBcellresponses.IntImmunol. 1998;10:1563–72.
21.NishimuraH,NoseM,HiaiH,MinatoN,HonjoT. Developmentoflupus-likeautoimmunediseasesby disruptionofthePD-1geneencodinganITIMmotif-carrying immunoreceptor.Immunity.1999;11:141–51.
22.NishimuraH,HonjoT.PD-1:aninhibitoryimmunoreceptor involvedinperipheraltolerance.TrendsImmunol. 2001;22:265–8.
23.ZhangJ,BraunMY.PD-1deletionrestoressusceptibilityto experimentalautoimmuneencephalomyelitisin
miR-155-deficientmice.IntImmunol.2014;28:1–9.
24.BertsiasGK,NakouM,ChoulakiC,RaptopoulouA,
PapadimitrakiE,GoulielmosG,etal.Genetic,immunologic, andimmunohistochemicalanalysisoftheprogrammeddeath 1/programmeddeathligand1pathwayinhumansystemic lupuserythematosus.ArthritisRheum.2009;60:207–18.
25.ProkuninaL,Castillejo-LópezC,ObergF,GunnarssonI,BergL, MagnussonV,etal.AregulatorypolymorphisminPDCD1is associatedwithsusceptibilitytosystemiclupus
erythematosusinhumans.NatGenet.2002;32:666–9.
26.ProkuninaL,GunnarssonI,SturfeltG,TruedssonL,Seligman VA,OlsonJL,etal.Thesystemiclupus
erythematosus-associatedPDCD1polymorphismPD1.3Ain lupusnephritis.ArthritisRheum.2004;50:327–8.
27.NielsenC,HansenD,HusbyS,JacobsenBB,LillevangST. Associationofaputativeregulatorypolymorphisminthe
PD-1genewithsusceptibilitytotype1diabetes.Tissue Antigens.2003;62:492–7.
28.KongEK-P,Prokunina-OlssonL,WongWH-S,LauC-S,Chan T-M,Alarcón-RiquelmeM,etal.AnewhaplotypeofPDCD1is associatedwithrheumatoidarthritisinHongKongChinese. ArthritisRheum.2005;52:1058–62.
29.IwamotoT,IkariK,InoueE,ToyamaY,HaraM,YamanakaH, etal.FailuretoconfirmassociationbetweenPDCD1
polymorphismsandrheumatoidarthritisinaJapanese population.JHumGenet.2007;52:557–60.
30.MengQ,LiuX,YangP,HouS,DuL,ZhouH,etal.PDCD1gene mayprotectagainstextraocularmanifestationsinChinese HanpatientswithVogt–Koyanagi–Haradasyndrome.MolVis. 2009;15:386–92.
31.Braum-PradoK,Petzl-ErlerML.Programmedcelldeath1gene (PDCD1)polymorphismandpemphigusfoliaceus(fogo selvagem)diseasesusceptibility.GenetMolBiol. 2007;321:314–21.
32.RochaMC,SantosLMB,BagatinE,CohenTervaertJW, DamoiseauxJGMC,LidoAV,etal.Geneticpolymorphismsand surfaceexpressionofCTLA-4andPD-1onTcellsof
silica-exposedworkers.IntJHygEnvironHealth. 2012;215:562–9.
33.DiasFC,MedinaTDS,Mendes-JuniorCT,DantasRO,Pissetti CW,RodriguesJuniorV,etal.Polymorphicsitesatthe immunoregulatoryCTLA-4geneareassociatedwithchronic Chagasdiseaseanditsclinicalmanifestations.PLOSONE. 2013;8:e78367.
34.SambrookJ,RusselDW.Molecularcloning:alaboratory manual.3rded.NewYork:ColdSpringHarborLaboratory Press;2001.
35.SangheraDK,ManziS,BontempoF,NestlerodeC,Kamboh MI.RoleofanintronicpolymorphisminthePDCD1genewith theriskofsporadicsystemiclupuserythematosusandthe occurrenceofantiphospholipidantibodies.HumGenet. 2004;115:393–8.
36.ProkuninaL,PadyukovL,BennetA,deFaireU,WimanB, PrinceJ,etal.AssociationofthePD-1.3AalleleofthePDCD1
geneinpatientswithrheumatoidarthritisnegativefor rheumatoidfactorandthesharedepitope.ArthritisRheum. 2004;50:1770–3.
37.JohanssonM,ArlestigL,MöllerB,Rantapää-DahlqvistS. AssociationofaPDCD1polymorphismwithrenal
manifestationsinsystemiclupuserythematosus.Arthritis Rheum.2005;52:1665–9.
cannotbeexcludedfromhavingeffectsintype1diabetes. BMCMedGenet.2007;8:71.
39.SutherlandA,DaviesJ,OwenCJ,VaikkakaraS,WalkerC, CheethamTD,etal.Genomicpolymorphismatthe interferon-inducedhelicase(IFIH1)locuscontributesto Graves’diseasesusceptibility.JClinEndocrinolMetab. 2007;92:3338–41.
40.JuranBD,AtkinsonEJ,SchlichtEM,FridleyBL,PetersenGM, LazaridisKN.Interactingallelesofthecoinhibitory
immunoreceptorgenescytotoxicT-lymphocyteantigen4and programmedcell-death1influenceriskandfeaturesof primarybiliarycirrhosis.Hepatology.2008;47:563–70.
41.SakthivelP,RamanujamR,WangXB,PirskanenR,LefvertAK. Programmeddeath-1:fromgenetoproteininautoimmune humanmyastheniagravis.JNeuroimmunol.2008;193:149–55.
42.HoffmannTW,HalimiJ-M,BüchlerM,Velge-RousselF, GoudeauA,Al-NajjarA,etal.Associationbetweena polymorphisminthehumanprogrammeddeath-1(PD-1) geneandcytomegalovirusinfectionafterkidney transplantation.JMedGenet.2010;47:54–8.
43.FichnaM,ZurawekM,Januszkiewicz-LewandowskaD,Fichna P,NowakJ.PTPN22,PDCD1andCYP27B1polymorphismsand susceptibilitytotype1diabetesinPolishpatients.IntJ Immunogenet.2010;37:367–72.
44.SoleimanifarN,AmirzargarAA,MahmoudiM,Pourfathollah AA,AziziE,JamshidiAR,etal.Studyofprogrammedcell death1(PDCD1)genepolymorphismsinIranianpatientswith ankylosingspondylitis.Inflammation.2011;34:707–12.
45.YousefiA,KarimiM.PD-1genepolymorphismsinIranian patientswithcolorectalcancer.LabMed.2013;44:241–4.
46.Velázquez-CruzR,OrozcoL,Espinosa-RosalesF,
Carre ˜no-ManjarrezR,Solís-VallejoE,López-LaraND,etal. AssociationofPDCD1polymorphismswithchildhood-onset systemiclupuserythematosus.EurJHumGenet.
2007;15:336–41.
47.Zú ˜nigaJ,Torres-GarcíaD,JimenezL,Ramírez-MartínezG, Juárez-NicolásF,MujicaF,etal.PDCD1genepolymorphisms indifferentMexicanethnicgroupsandtheirroleinthe susceptibilitytohypersensitivitypneumonitis.ClinBiochem. 2010;43:929–31.
48.BrzozaZ,GrzeszczakW,TrautsoltW,MoczulskiD.Lackof associationofprogrammedcelldeath1gene(PDCD1) polymorphismswithsusceptibilitytochronicurticariain patientswithpositiveautologousserumskintest.JInvestig AllergolClinImmunol.2012;22:432–6.
49.NielsenC,LaustrupH,VossA,JunkerP,HusbyS,LillevangST. AputativeregulatorypolymorphisminPD-1isassociated withnephropathyinapopulation-basedcohortofsystemic lupuserythematosuspatients.Lupus.2004;13:
510–6.
50.Ferreiros-VidalI,Gomez-ReinoJJ,BarrosF,CarracedoA, CarreiraP,Gonzalez-EscribanoF,etal.AssociationofPDCD1
withsusceptibilitytosystemiclupuserythematosus: evidenceofpopulation-specificeffects.ArthritisRheum. 2004;50:2590–7.
51.Ferreiros-VidalI,D’AlfonsoS,PapasteriadesC,SkopouliFN, MarchiniM,ScorzaR,etal.Biasinassociationstudiesof systemiclupuserythematosussusceptibilitydueto
geographicalvariationinthefrequencyofaprogrammedcell death1polymorphismacrossEurope.GenesImmun. 2007;8:138–46.
52.SigurdssonS,NordmarkG,GöringHH,LindroosK,WimanAC, SturfeltG,etal.Polymorphismsinthetyrosinekinase2and interferonregulatoryfactor5genesareassociatedwith systemiclupuserythematosus.AmJHumGenet. 2005;76:528–37.
53.ThorburnC,Prokunina-OlssonL.AssociationofPDCD1
geneticvariationwithriskandclinicalmanifestationsof systemiclupuserythematosusinamultiethniccohort. Genes.2007;8:279–87.
54.SánchezE,ComeauME,FreedmanBI,KellyJA,KaufmanKM, LangefeldCD,etal.Identificationofnovelgenetic
susceptibilitylociinAfricanAmericanlupuspatientsina candidategeneassociationstudy.ArthritisRheum. 2011;63:3493–501.
55.LiuC,JiangJ,GaoL,HuX,WangF,ShenY,etal.Apromoter regionpolymorphisminPDCD-1geneisassociatedwithrisk ofrheumatoidarthritisintheHanChinesepopulationof southeasternChina.IntJGenomics.2014;2014: