This work was carried out at the Speech-Language, Pathology and Audiology Course, Ribeirão Preto School of Medicine, Universidade de São Paulo – USP – Ribeirão Preto (SP), Brazil, whose fellowship was granted by the Extension Program “Ensinar com Cultura e Extensão”, from Universidade de São Paulo (USP). (1) Department of Ophthalmology, Otolaryngology and Head and Neck Surgery, Ribeirão Preto School of Medicine, Universidade de São Paulo – USP – Ribeirão Preto (SP), Brazil.
(2) Clinical Speech Therapist, Ribeirão Preto (SP), Brazil.
Conflict of interests: No
Author’s contribution: FDFS was the main researcher, elaborating the study and chronogram, researching the literature, performing data collection and analysis, and writing the article; PPM was the mentor, elaborating the study and chronogram, performing data analysis, writing and correcting the article, and submitting the study for final approval.
Correspondence address: Patrícia Pupin Mandrá. Av. Bandeirantes, 3900, Monte Alegre, Ribeirão Preto (SP), Brasil, CEP: 14049-900. E-mail: [email protected]
Received: 2/20/2013; Accepted: 8/12/2013
Users’ satisfaction with a conversation circle program in
the waiting room
Satisfação de usuários com um programa de Roda de Conversa
em sala de espera
Patrícia Pupin Mandrá1, Fernanda Diniz Faleiros Silveira2
ABSTRACT
Purpose: To investigate the satisfaction of participants with an educatio-nal program in health. Methods: Research voluntarily participants were 34 adults, 21 females and 13 males. For the collection was designed an instrument directed with responses presented in Likert scale (0-5). The data were categorized and tabulated for analysis by nonparametric statis-tics. Results: The program was evaluated as very good (VG) by 73.8% of those interviewed, the strategy of presentation as VG by 73.2%, the organization was 70.3% for VG, the language and supporting material for VG were 75.5% and 57.2% respectively, and 69.3% considered it important the content and 44% were prepared to convey knowledge.
Conclusion: It consisted to which participants were satisfied with the program, so the circles of conversation were an effective strategy capable of producing a discussion of the issues placed on the agenda and effec-tive for sensitization of the participants in their health.
Keywords: Health Promotion; Health Education; Humanization of As-sistance; Patient Satisfaction; Speech, Language and Hearing Sciences
RESUMO
Objetivo: Investigar a satisfação de participantes com um programa edu-cativo em saúde. Métodos: Participaram voluntariamente da pesquisa 34 adultos, 21 do gênero feminino e 13 do gênero masculino. Para a coleta, foi elaborado um instrumento dirigido com respostas apresentadas em escala Likert (0-5). Os dados obtidos foram categorizados e tabulados para a análise por meio de estatística não paramétrica. Resultados: A temática foi avaliada como muito boa (MB) por 73,8% dos entrevistados, a estratégia de apresentação como MB por 73,2%, a organização como MB para 70,3% e a linguagem e o material de apoio como MB para 75,5% e 57,2%, respectivamente. Sessenta e nove vírgula três por cento dos entrevistados consideraram importante o conteúdo e 44% estavam preparados para transmitir o conhecimento. Conclusão: Constatou-se que os participantes ficaram satisfeitos com o programa e que as rodas de conversa mostraram-se como uma estratégia efetivamente capaz de produzir a discussão sobre os assuntos colocados em pauta e eficaz para a sensibilização dos participantes frente a sua saúde.
INTRODUCTION
The university is a privileged site for divulgation and propa-gation of scientific knowledge, both internally and externally. Health educational actions are strategies for disseminating knowledge in the community, as well as for making faculty and students aware of the social reality in which they are in-serted. In order to fulfil its social role, the university has been conducting extension programs to articulate and integrate the education and health knowledge in benefit of the community. Health education is mainly aimed at conveying information to change the personal behaviour regarding the own health(1) and
qualify individuals so that they can act consciously towards the daily reality(2). Through educational practices, the healthcare
practitioners could divulge the scientific knowledge and act on the daily life of people(3).
The purpose of the health education should be guided by an educational model. Based on the traditional preventive model of health education, the practitioner theoretically would reach the proposed objectives by means of verticalised information and persuasion of individuals(4-6), assuming the principle that
adequate information should be conveyed by those who hold knowledge (i.e. the practitioner)(3). On the other hand, the
practitioners might use the radical/dialogical model, in which the effective participation of the population is assumed and individual choices, autonomy, self-management, and social responsibility on the process of health-disease-care(4,6). With
this model, individuals would be made responsible for their health problems and there would be a valorisation of the key strategies for experience exchange in order to unleash a reflec-tion. The basis for this purpose would be the joint construction of knowledge by means of educational practices, whose aim is to raise the critical awareness among individuals through idea exchanges and to respect the diversity in human relations(7,8).
The dialogic model for health education has been associated to prolonged changes in health-related habits and behaviours as the use of these principles allow the construction of new meanings on the themes being addressed(9).
With the use of a bi-directional rather than a unidirectional communication resource, one wants to have access to and democratisation of scientific knowledge for all social classes without compromising the technical precision.
One of the dialogic structures of health education descri-bed in the literature is the formation of small groups for local workshops, group dynamics, conversation circles, and collec-tive games supported by illustracollec-tive/informacollec-tive material such as pamphlets, folders, video and so on(3,6,9-11).
The informality of the conversation circle is an example of democratic learning space, which promotes inclusion of and cooperation by participants and third-parties in the construction of the educational process. In this strategy, their knowledge is taken into account for establishment of communication and critical analysis of the content addressed(9). During the
conversation circle, the practitioner (facilitator) will endeavour to promote reflection and discussion of the theme by exchan-ging and sharing problems and solutions on an interactive, horizontal and dialogic basis(11).
In order to put the conversation circle into practice, the healthcare practitioners should also worry at their stance, lan-guage supporting material, and site as all these aspects must be suitable for theoretical model, theme, and target community in terms of gender, age group, education level, occupation, and socioeconomic class. The themes must be selected based on the participants’ interests and practices in order to stimulate the initial exchange of experiences(10).
The communication process is one of the issues faced in the humanisation of the healthcare. The success involving these actions depends on the challenge of learning, recognising and negotiating with the other person who may have peculiar rights, autonomy and cultural background(12). The use of a participative
methodology creates space for discussion and construction of knowledge to be shared among the individuals taking part in the activity(13).
Evaluation of the educational practice developed is of ex-treme importance for a critical review of the program’s objec-tive, which includes the theoretical model and strategies used. Therefore, the healthcare user who participates in these actions plays a key role in rating the program at whom it is aimed.
Researchers(6) have studied the efficacy of a program
de-veloped by community healthcare agents, whose theme was speech therapy. The educational model adopted by them was the personal experience report, with data being obtained by means of both semi-structured collective interview prior to intervention and focal group technique after the intervention. The researchers concluded that an educational intervention performed on the basis of the conception of a radical educatio-nal model was shown to be efficient for addressing the issues raised by the group.
Speech therapists have developed a work with educators by planning and conducting workshops for health promotion. They concluded that such workshops stimulated discussion on the themes addressed and opportunity for participants to build knowledge and apply it in their daily practices autonomously(14).
Authors have evaluated the effectiveness of an educational process by means of speech exposure, in which the participants were encouraged to report their own interests and experiences regarding the theme as they saw an album of illustrations. At the end of the program, an easy-reading manual with illustrations was distributed in order to reinforce the themes addressed. A questionnaire was elaborated to evaluate the knowledge of the group. The results indicated that the educational process was efficient, since the knowledge on the theme had improved and therefore it was found to be an effective low-cost model that can also be used for health promotion(10).
been described elsewhere(11). Three interdisciplinary,
inter--sectoral conversation circles were conducted, involving 40 practitioners such as physicians, psychologists, nurses, social workers, administrative assistants, physiotherapists, general service operators, and others. The conversation circles had a total time of 150 minutes. During the activities, the facilitators sought to reflect and discuss on the theme with the participants. In fact, the conversation circles were shown to be a promising and effective method to promote changes in the healthcare environments, since collective work strengthened the solidary thinking as well as a new way of promoting health.
The educational action conducted by nurses and social workers aiming to make workers sensitive to the use of cigars in public areas has been evaluated. The work was based on the following strategies: a) puppet theatre; b) survey on knowledge and behaviour regarding smoking habit; c) educational quiz games on the theme; d) conversation circles with groups for informal discussion on the theme based on free expression of doubts, personal experiences and life witness; and e) lectures with video presentation and debate, including distribution of educational folders. After evaluation of the program, it was found that changes in participants were effective and that the knowledge conveyed adequately by trained practitioners was crucial for preventing health impairment, mainly the informa-tion provided, thus stimulating individuals to be aware of the changes in their lifestyle and behaviour(15).
In a project carried out by both healthcare service workers and community radio professionals, several workshops (13 meetings lasting four hours) were created in order to discuss, reflect and create joint actions on the health theme. Academic texts, poems, songs, soap-opera creation and paintings were used to address the themes. The facilitators were worried about avoiding that the workshops were linearly and unidirectionally created, thus giving priority to the participants’ experiences and interpretations. The final evaluation was made by means of a questionnaire on the workshops, including supporting material and knowledge incorporation. After data analysis, one concluded that the methodology met the objective, since the participants were involved and partnerships were developed among them during the project(5).
Assuming that there must be a knowledge exchange betwe-en university and local community through extbetwe-ension actions(16),
a social-educational program focusing on the speech therapy healthcare was implemented and developed in the waiting room of the Integrated Rehabilitation Centre of the State Hospital of Ribeirão Preto (CIRHER) during the year of 2011.
Considering that one of the indicators of healthcare quality is the evaluation of the user’s satisfaction regarding the heal-thcare actions, as established by the Unified Health System (SUS) and in accordance with the health education perspective adopted, and assuming that such an evaluation should be a constant monitoring process of the health educational practi-ces(17), it becomes necessary to know the participants’ opinions
about goal fulfilment, content, material, dynamics, strategies, and interpersonal relations during the program. According to a study(17), the result on the efficacy of the program was the basis
for discussion between proponents and managers regarding the re-dimensioning and/or improvement of the actions and stra-tegies adopted to meet specific needs of the healthcares users. Validation of the data obtained from evaluation will depend on how one intends to use the results(17).
Therefore, the objective of this study was to assess the participants’ satisfaction with a health educational program developed by means of conversation circles in the waiting room.
METHODS
The present study was approved by the local human research committee of Clinic Hospital of the Ribeirão Preto, Ribeirão Preto Medical School, University of São Paulo (CEP HC FMRP USP), according to protocol number 8802/2010.
A total of 34 people participated in the study, being 21 female and 13 male. All the participants were users and/or caretakers attending the CIRHER during April to June 2011 who were in the waiting room and accepted to take part in the University Extension Program called “Conversation Circle: Strategy to Promote Speech Therapy Healthcare”. The parti-cipants were selected by verbal invitation before presentation of the study’s and program’s objectives and signing of an informed consent form.
The best date and time for development of the conversation circles were chosen based on a survey of the profile of all in-dividuals attending the CIRHER in different days and times. During the appointments, the participants were asked to say their age, gender, medical speciality, and if they were health-care users or health-caretakers and if they were interested in taking part in future conversation circles, including suggestions about the theme. After the survey, it was decided that the activities would be conducted on Fridays in the morning. The program was divulged by means of posters placed on the walls of the waiting room and other healthcare sectors in the CIRHER. One week before the beginning of the activities, verbal invitation was followed up by presentation of the study’s and program’s objectives to be achieved together with the users and/or care-takers present in the waiting room at a previously determined time for the conversation circles.
person. At the end of each conversation circle, the participants were given a questionnaire for evaluation of their satisfaction, in which suggestion for other themes could be indicated. Eight conversation circles were conducted during the program. Themes, goals, strategies and materials used in each of the conversation circles are listed in Table 1.
The educational material used during the conversation circles was elaborated based on bibliographical references and related official sites (World Health Organization, Ministry of Health, and Federal Council of Speech, Language and Hearing Sciences).
An instrument (directive questionnaire) was elaborated to evaluate the participants’ satisfaction, which consisted of instructions, identification, and 10 questions on theme-related content, strategies and didactic material used during the conver-sation circles. A 5-point Likert scale together with illustrations was used as follows: “Very Poor” (VP), “Poor” (P), “Regular” (R), “Good” (G), and ‘Very Good” (VG).
At the end of each conversation circle, the participants were invited to answer the questionnaire individually and to sign a free informed consent form.
For data analysis, the questionnaires were read and sepa-rated by conversation circle and the resulting data were cate-gorised and tabulated by using non-parametric statistics. All
the results were organised into Excel tables and then absolute and relative frequencies of the answers were calculated. Next, the data were interpreted and statistically analysed from the following categories: content, material and importance.
One should emphasise that the program was part of an Extension Culture Project elaborated by a professor-master and carried out by a fourth-year undergraduate student in Speech, Language and Hearing Sciences under supervisor, and there was a previous two-month period so that the student could be theoretically and technically prepared to act.
RESULTS
Thirty-four adults, 21 female and 13 male, have participated voluntarily in the study. All of them were attending the CIRHER during April to June 2011. During the program, eight conver-sation circles were conducted in the waiting room. Because it was a conversation circle program (open group) with volunteers, it was found a variation in the number of participants, that is, five ones with mean age of 43 years old.
The participants in the fourth conversation circle (n=6) did not accept to take part in the study and they did not answer the questionnaire. Therefore, Table 2 lists the results obtained from the evaluation of seven conversation circles.
Table 1. Theme developed during the conversation circles
Conversation circle
Theme Goal Strategy Supporting material
1 Speech Therapy/Presentation a) To establish confidence relationship and dialogic interaction between users and mediator
b) To introduce the speech therapist
Chat between mediator and participants
Folder/video
2 Health a) To reflect on general health and quality of life
Mediated dialogic activity Posters/Pamphlets/ Video
3 Speech a) To reflect on care and prevention regarding vocal alterations
Mediated dialogic activity Fo l d e r “ Vo i c e c a m p a i g n 2011”/Video
4 Elderly health a) To reflect on the elderly health and speech/hearing changes
Mediated dialogic activity Folders/video
5 Smoking a) To reflect on the relationship between smoking and speech/ hearing changes
Mediated dialogic activity Pamphlets/Video
6 Communication relationship speaker x listener
a)To reflect on the speaker x listener relationship
Mediated dialogic activity ”String dynamics”
Pamphlets/Video
7 Communication a) To reflect on for ms of communication and possible changes
Mediated dialogic activity Pamphlets/Video
8 Stuttering/finish a) To reflect on stuttering and its manifestations. End of the program
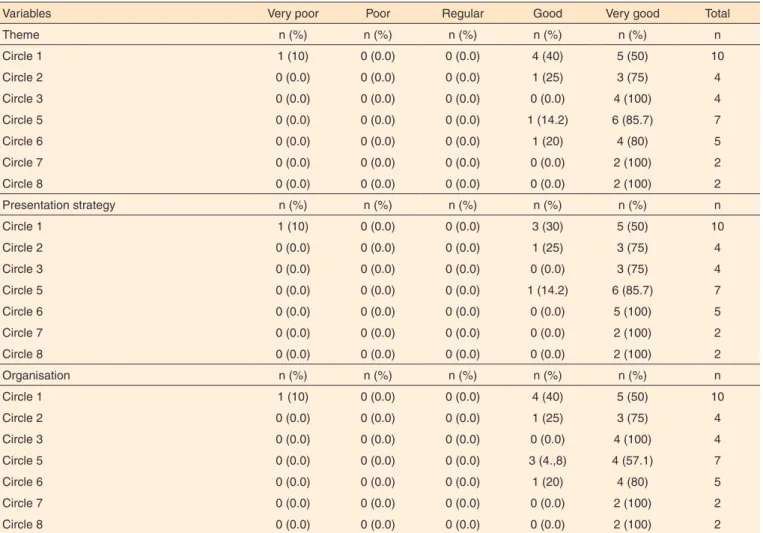
It was found that the participants evaluated the theme as being satisfactory, with 24.75% of them evaluating it as “G” and 73.8% as “VG”, whereas strategy and organisation were considered as “VG”, respectively, 73.2% and 70.3%. The results on satisfaction with content, strategy and organisation were listed in Table 3.
The oral language (vocabulary) used by the researcher was evaluated as being satisfactory (VG) by 75.7% of the partici-pants and the supporting material (i.e. video, folders, pamphlets,
banner and panel) was considered very good by 57.2%. Folders and digital videos were selected, whereas pamphlets, banners and panel were printed based on institutional documents according to themes previously proposed by the users in the waiting room (Table 4).
With regard to the questions “How important was the con-versation circle to you” and “Are you capable to conveying the knowledge acquired here”, 69.3% and 44% of the participants considered them as VG (Table 5).
Table 2. Characterisation of the participants in the conversation circles
Absolute frequency (n)
Conversation circles 1 2 3 4 5 6 7 8 Total
Participants 10 4 4 6 7 5 2 2 40
Gender
Female 4 3 3 NA 4 3 2 2 21
Male 6 1 1 3 2 0 0 13
Age
Minimum 28 28 60.5 NA 63.3 47.7 46 46
Average 53.4 45.5 52 NA 50 29 36 36
Maximum 65 63 69 NA 74 65 56 56
Note: NA = no answer
Table 3. Participants’ satisfaction with content, strategy and organisation
Variables Very poor Poor Regular Good Very good Total
Theme n (%) n (%) n (%) n (%) n (%) n
Circle 1 1 (10) 0 (0.0) 0 (0.0) 4 (40) 5 (50) 10
Circle 2 0 (0.0) 0 (0.0) 0 (0.0) 1 (25) 3 (75) 4
Circle 3 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 4 (100) 4
Circle 5 0 (0.0) 0 (0.0) 0 (0.0) 1 (14.2) 6 (85.7) 7
Circle 6 0 (0.0) 0 (0.0) 0 (0.0) 1 (20) 4 (80) 5
Circle 7 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 2 (100) 2
Circle 8 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 2 (100) 2
Presentation strategy n (%) n (%) n (%) n (%) n (%) n
Circle 1 1 (10) 0 (0.0) 0 (0.0) 3 (30) 5 (50) 10
Circle 2 0 (0.0) 0 (0.0) 0 (0.0) 1 (25) 3 (75) 4
Circle 3 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 3 (75) 4
Circle 5 0 (0.0) 0 (0.0) 0 (0.0) 1 (14.2) 6 (85.7) 7
Circle 6 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 5 (100) 5
Circle 7 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 2 (100) 2
Circle 8 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 2 (100) 2
Organisation n (%) n (%) n (%) n (%) n (%) n
Circle 1 1 (10) 0 (0.0) 0 (0.0) 4 (40) 5 (50) 10
Circle 2 0 (0.0) 0 (0.0) 0 (0.0) 1 (25) 3 (75) 4
Circle 3 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 4 (100) 4
Circle 5 0 (0.0) 0 (0.0) 0 (0.0) 3 (4.,8) 4 (57.1) 7
Circle 6 0 (0.0) 0 (0.0) 0 (0.0) 1 (20) 4 (80) 5
Circle 7 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 2 (100) 2
DISCUSSION
The general objective of the extension program was to make the participants sensitive to the general and speech health. The strategy used for the development of the program matches the dialogic model for health education, whose aim is to work in groups in order to promote the development of critical awa-reness through idea exchange(6). The choice for conversation
circles was guided by the premise that healthcare practitioners and users need to establish a dialogic relationship based on hearing, respect, and valorisation of experiences, histories and
views of each person(10,17), and that health education is a process
capable of developing reflection and critical awareness among people regarding the causes of their health problems by means of dialogue(8).
The conversation circles lasted between 20 and 40 minutes, ranging in terms of number of participants, about 5 per circle, whose mean age ranged from 29 to 53 years old (Table 2). This variation might be explained by the fact that the number of people in the waiting room was different every day and because they might have refused to take part in the group. One also emphasises that the activities developed in the waiting room
Table 4. Participants’ satisfaction with language and material
Variables Very poor Poor Regular Good Very good Total
Language n (%) n (%) n (%) n (%) n (%) n
Circle 1 1 (10) 0 (0.0) 1 (10) 1 (10) 7 (70) 10
Circle 2 0 (0.0) 0 (0.0) 0 (0.0) 5 (50) 5 (50) 4
Circle 3 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 4 (100) 4
Circle 5 0 (0.0) 0 (0.0) 0 (0.0) 1 (14.2) 6 (85.7) 7
Circle 6 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 5 (100) 5
Circle 7 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 2 (100) 2
Circle 8 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 2 (100) 2
Supporting material n (%) n (%) n (%) n (%) n (%) n
Circle 1 0 (0.0) 0 (0.0) 0 (0.0) 5 (50) 4 (40) 10
Circle 2 0 (0.0) 0 (0.0) 0 (0.0) 1 (25) 3 (75) 4
Circle 3 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 4 (100) 4
Circle 5 0 (0.0) 0 (0.0) 0 (0.0) 2 (28.5) 3 (42.8) 7
Circle 6 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 5 (100) 5
Circle 7 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 2 (100) 2
Circle 8 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 2 (100) 2
Table 5. Participants’ satisfaction with the importance of the conversation circle and knowledge convey
Variables Very poor Poor Regular Good Very good Total
Importance n (%) n (%) n (%) n (%) n (%) n
Circle 1 0 (0.0) 0 (0.0) 0 (0.0) 2(20) 5 (50) 10
Circle 2 0 (0.0) 0 (0.0) 0 (0.0) 1 (25) 3 (75) 4
Circle 3 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 3 (75) 4
Circle 5 0 (0.0) 0 (0.0) 0 (0.0) 1 (14.2) 4 (57.1) 7
Circle 6 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 5 (100) 5
Circle 7 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 2 (100) 2
Circle 8 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 2 (100) 2
Knowledge convey n (%) n (%) n (%) n (%) n (%) n
Circle 1 0 (0.0) 0 (0.0) 3 (30) 3 (30) 1 (10) 10
Circle 2 0 (0.0) 0 (0.0) 0 (0.0) 1 (25) 3 (75) 4
Circle 3 0 (0.0) 0 (0.0) 1 (25) 0 (0.0) 2 (50) 4
Circle 5 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 4 (57.1) 7
Circle 6 0 (0.0) 0 (0.0) 0 (0.0) 2 (40) 3 (60) 5
Circle 7 0 (0.0) 0 (0.0) 0 (0.0) 1 (50) 1 (50) 2
should be flexible and the practitioner (facilitator) must be prepared to deal with the diversity of individuals in the group and to make those who are present to adhere the group, thus legitimating the principles of autonomy, self-management, and co-responsibility for health(4,6,11,12,15).
One can indicate the following aspects or factors hypothe-tically associated with the refusal to participate in the conver-sation circles: lack of interest about the theme, spending the waiting time with other activities (e.g. reading, watching TV, talking to others, etc.), lack of clear information on how to participate in the program, lack of personal interest in acquiring knowledge, or even the site where the conversation circle oc-curs, in our case, the waiting room – an ample, noisy and busy space. Another explanation would be the sporadic occurrence of this type of action during the healthcare service and the absence of strategies for this aim, since there is a free demand of users, which may restrict the scope of educational actions(2).
It is not possible to conclude about what contributes to their acceptance or refusal to take part in the conversation circle. For some similar programs, it is suggested that the users present in the waiting room and who refused the invitation should be asked about the reasons for doing so. This information would be crucial for re-structuring the program as strategies to stimulate the target population to participate could be included.
Every health educational program should be evaluated by the participants so that its idealisers can analyse the effective-ness of the strategy adopted. The results obtained in the present work (Table 3) show that the theme addressed was satisfactory. As predicted by the bi-directional and democratic method, it should be emphasised that the contents were defined in con-junction with the users who were present in the waiting room, and at the end of each conversation circle, the participants could give suggestions on new themes(5,6,10,11,15). One considers that
the model adopted here was satisfactory in meeting the goals to construct and convey health knowledge on a participative basis, taking into account autonomy, experience and previous knowledge of each participant(5,6,8,12).
The educational materials (both elaborated and institu-tional) were used for supporting the discussion process, and it was found that the participants were satisfied with them. There was worry about selecting and elaborating materials that addressed the theme in a simple, clear, and contextualised way suitable for the cultural and social-economic level of the participants(4,6,8). The language used by the facilitator was also
target of evaluation, and again it was found that the partici-pants were satisfied (Table 4). The literature states that only a well-prepared practitioner can conduct a group dialogue and allow access to elaborated information(6). Therefore, the student
accounting for the project was previously prepared(15) so that
she could establish a symmetric and democratic relationship with the group while enabling idea exchange, reflection, and discussion on an interactive and dialogic basis, thus privile-ging the individual experience(10-12). The use of technical and
scientific terms was minimised, in an attempt to shorten the gap between academic language and community without losing the theoretical foundation(4). All the above-mentioned cares were
taken in order to enable communication barriers to be broken down, thus creating a more democratic space for construction of knowledge(11,13). In programs like this, the practitioner will
always play the role of humanising the relationships, which requires social commitment as well as technical and scientific competency in her/his area.
According to the results listed in Table 3, both strategy and organisation of the program were evaluated as satisfactory by the majority of the participants, suggesting that conversa-tion circle is a resource capable of producing discussion on themes scheduled and of making the participants sensitive to their health, showing to be a promising and effective scenario for changes in the healthcare environments(10). In fact, the
practitioner is expected to be flexible in order to deal with the dynamism imposed by the situation, since there are many variables in symmetric and democratic relations involving the voluntary participation(11,13). It is certain that strategies like
this should be included in the institutional health education planning and incorporated into the healthcare service routine on a continuous basis(11,13).
During the conversation circles, the participants had the opportunity to opine, share life experiences and ideas. In fact, those were very productive moments that stimulated them to build their own knowledge and be responsible for viewing themselves as important, giving the group the opportunity to deepen into healthcare and speech therapy issues. However, strategies encouraging people to take part in this type of activity on a voluntary rather than obligatory basis should be thought, which would stimulate the population to manage and account for their own health.
It is necessary to offer the users a space so that they can express their opinions on the service provided. Therefore, des-pite some limitations, the present instrument was found to be pertinent as it enabled the researcher to reflect on the difficulties related to method and implementation of the educational prac-tice. The program should be continuously evaluated with a qua-litative instrument as the space offered for user’s manifestation might be increased. A self-assessment instrument should also be included, since only the participants were accounted for the success of the program. However, it is a challenge to assess all the factors involved in the educational practice because several players take part in the process and situations are dynamic and often unpredictable, even for the scientific method.
CONCLUSION
REFERENCES
1. Berbel DB, Rigolin CCD. Educação e promoção da saúde no Brasil através de
Campanhas públicas. Revista Brasileira de Ciência, Tecnologia e Sociedade. 2011;1(2):25-38.
2. Lima RT, Barros JC, Melo MRA, Sousa MG. Educação em saúde e nutrição em João Pessoa, Paraíba. Rev Nutr. 2000;13(1):29-36. 3. Gilvan FF. Educação em saúde em grupo: olhar da enfermeira e do
usuário hipertenso [dissertação]. Fortaleza: Universidade Estadual do Ceará; 2011. 174p.
4. Bizzo MLG. Difusão científica, comunicação e saúde. Cad Saúde Pública. 2002;18(1):307-14.
5. Matos MR, Meneguetti lC, Gomes ALZ. Uma experiência em comunicação e saúde. Interface. 2009;13(31):437-47.
6. Brites LS, Souza, APR, Lessa, AH. Fonoaudiólogo e agente comunitário de saúde: uma experiência educativa. Rev Soc Bras Fonoaudiol. 2008;13(3):258-66.
7. Silva CMC, Meneghim MC, Pereira AC, Mialhe FL. Educação em saúde: uma reflexão histórica de suas práticas. Ciênc Saúde Coletiva. 2010;15(5):2539-50.
8. Alves GG, Aerts D. As práticas educativas em saúde e a Estratégia Saúde da Família. Ciênc Saúde Coletiva. 2011;16(1):319-25. 9. Figueiredo MFS, Rodrigues-Neto JF, Leite MTS. Modelos
aplicados às atividades de educação em saúde. Rev Bras Enferm. 2010;63(1):117-21.
10. Ribeiro PJ, Aguiar LAK, Toledo CF, Barros SMO, Borges DR.
Programa educativo em esquistossomose: modelo de abordagem metodológica. Rev Saúde Pública. 2004;38(3):415-21.
11. Gomes AMA, Sampaio JJC, Carvalho MGB, Nations MK, Alves MSCF. Código dos direitos e deveres da pessoa hospitalizada no SUS: o cotidiano hospitalar na roda de conversa. Interface. 2008;12(27):773-82.
12. Deslandes SF, Mitre RMA. Processo comunicativo e humanização em saúde. Interface. 2009;13(supl.1):641-9.
13. Jeolás LS, Ferrari RAP. Oficinas de prevenção em um serviço de saúde para adolescentes: espaço de reflexão e de conhecimento compartilhado. Ciênc Saúde Coletiva. 2003;8(2):611-20.
14. Mendonça JA, Lemos SMA. Promoção da saúde e ações f o n o a u d i o l ó g i c a s e m e d u c a ç ã o i n f a n t i l . R ev C E FAC . 2011;13(6):1017-30.
15. Custódio IL. Ações de educação em saúde no controle do tabagismo nos ambientes de trabalho. In: 61º Congresso Brasileiro de Enfermagem; 2009. dez 07-10. Fortaleza. Congresso Brasileiro de Enfermagem; Fortaleza: 2009.
16. Braga TMS, Oliveira JP. Salas de espera espaços com potencial para ações que integrem a educação e a saúde. In: Marcolino J, Zaboroski AP, Oliveira JPO. Perspectivas atuais em fonoaudiologia: refletindo sobre ações na comunidade. São José do Campos: Pulso, 2010. cap. 8.