www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Objective
assessment
of
surgical
technique
in
rotation
and
nasal
projection
variation
夽
,
夽夽
Marina
Serrato
Coelho
Fagundes
∗,
Ana
Tereza
Moreira,
Elizabeth
Mila
Tambara,
Sérgio
Bernardo
Tenório,
Rogério
de
Fraga,
Rogerio
Hamerschmidt
SurgicalClinic,UniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil
Received26March2014;accepted30January2015 Availableonline10December2015
KEYWORDS
Rhinoplasty; Measures; Suturetechniques
Abstract
Introduction:In rhinoplasty, facialesthetic analysis is critical for proper surgicalplanning. Parameterssuchasrotationandnasalprojectionshouldberoutinelyevaluated.Fewstudies haveobjectivelyassessedchangesinfacialanglespostoperatively.
Objective: Toevaluatetheeffectivenessofmedialintercruralsuturesandofrotationofthe nasal tipontheincrease ofrotation andnasalprojection inCaucasianpatientsundergoing primaryrhinoplasty.
Methods:Aprospectivestudycarriedoutbetween2011and2013,with27patientstreatedwith primaryrhinoplastywithabasictechniquebythesamesurgeon,withmedialintercruralsutures androtationofthenasaltip.Rotationandnasalprojectionweremeasuredfromphotographs obtainedpreoperativelyandafter12months.
Results:All27patientscompletedthestudy.Themeanagewas27.1years.Therewasamean increaseof8.4◦intherotation---astatisticallysignificantvalue.Therewasnosignificantchange
intheprojection.
Conclusion: Themedialintercrural andnasaltiprotationsuturesareeffectiveinincreasing nasalrotationinCaucasianpatientsundergoingrhinoplasty.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:FagundesMSC,MoreiraAT,TambaraEM,TenórioSB,deFragaR,HamerschmidtR.Objectiveassessmentof
surgicaltechniqueinrotationandnasalprojectionvariation.BrazJOtorhinolaryngol.2016;82:47---55.
夽夽Institution:PostgraduatePrograminSurgicalClinic,HospitaldeClínicasdaUniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil.
∗Correspondingauthor.
E-mail:[email protected](M.S.C.Fagundes). http://dx.doi.org/10.1016/j.bjorl.2015.11.003
PALAVRAS-CHAVE
Rinoplastia; Medidas;
Técnicasdesutura
Avaliac¸ãoobjetivadatécnicacirúrgicanavariac¸ãodarotac¸ãoeprojec¸ãonasal
Resumo
Introduc¸ão:Narinoplastia,aanáliseestéticafacialéessencialparaumplanejamentocirúrgico adequado.Parâmetroscomorotac¸ãoeprojec¸ãonasaldevemserrotineiramenteavaliados.Há poucosestudosqueavaliemobjetivamenteasmudanc¸asnosângulosfaciaisnopós-operatório. Objetivo:Avaliar aeficácia das suturasintercrura mediais e derotac¸ãoda pontanasal no aumento da rotac¸ão e projec¸ão nasal em pacientes caucasianos submetidos à rinoplastia primária.
Método: Estudoprospectivorealizadoentre2011e2013,com27pacientessubmetidosà rino-plastiaprimária técnicabásica,pelomesmo cirurgião,comsuturasintercrura mediaisede rotac¸ão da pontanasal. Mediu-se a rotac¸ão e a projec¸ão nasal a partir de fotografias no pré-operatórioe12mesesapós.
Resultados: Todosos27 pacientescompletaram o estudo.A idade médiafoi de 27,1anos. Houveaumentomédiode8,4◦narotac¸ão,comsignificânciaestatística.Nãohouvealterac¸ão
significativanaprojec¸ão.
Conclusão:Assuturasintercruramediaisederotac¸ãodapontanasalsãoeficazesnoaumento darotac¸ãonasalempacientescaucasianossubmetidosàrinoplastia.
©2015Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Rhinoplastyisoneofthemostchallengingcosmetic surger-iesoftheface.Thesurgeonmustcombinethecorrectionof functional changeswith his/hersense of beauty and har-mony, taking into account the patient’s wishes.1 A facial
estheticanalysisis essential in thiscontext, inwhich the nasal anthropometric measurements should be assessed and,fromthem,asurgicalplanshouldbecreatedsothatthe desiredresultscanbeachieved.Currently,theparameters usedinfacialestheticsurgeriesarebasedonthestudyof PowellandHumphreys.2Theseauthorsformulatedsuitable
relationsbetweenfaceandnose,definingfacialangles. Nasalptosisandalackoftipprojectionrepresentalarge portionofthecomplaintsofpatients,andcanreach72%.3,4
In assessing nasalptosis, one shouldobserve the rotation ofthenasaltipthroughthenasolabialangle.This angleis obtainedbytheangularinclinationofcolumellaatthepoint whereitmeetsalinetangenttotheupperlip.Anasolabial angleisdeemedoptimalwhenitfallsbetween90◦and105◦
inmenand105◦and120◦inwomen.5
Theprojectionofthenasaltipisthedistanceatwhich thenasaltipprotrudesfromtheface.Itis measuredbya ratio.There arevarious methods of evaluatingthis ratio, amongthemtheGoodemethod.Thismethodisperformed bymeasuringthelineperpendiculartothetippointtothe lineofthefacialplanedividedbythenasionlinetothetip point.Itisrecommendedthatthisvaluefalls intherange of0.55---0.6.6
Several approaches andtechniques canbe usedin the managementof rotationandnasaltipprojectionchanges. The literature contains descriptions of open and closed (endonasal)techniques,andtheuseofgraftsandsutures. Theendonasaltechniqueproducesthesameresultsofthe open technique, though withless damage to the support mechanismsofthenasaltip.
Thenasalsupportmechanismsaredividedintomajorand minor mechanisms.Major mechanisms includethe fibrous ligament of the cephalic rim of the alar cartilage to the caudalrim of upperlateralcartilage; theshape,size and strength of medial and lateral crura, and the fibrous lig-ament from the medial crus to the caudal rim of the quadrangularcartilage.Theminorsupportmechanismsare the cartilaginous dorsumof the septum,the membranous septum, nasal spine, the interdomal ligament, sesamoid complexes of lowerlateral cartilages, ligaments between thelowerlateralcartilages,andskin/softtissues.6
Coupled with the knowledge of nasal support mecha-nisms,knowledgeoftheirdynamicsalsois important.The ideathatachange inrotationandprojectionofthenasal tip couldoccur due tochanges in medialor lateralcrura wasfirstdescribedin1960,asthetripodconcept.7In1969,
Andersondescribedthistheory,inwhichthelateralcrusof eachlowerlateralcartilageandthetwomedialcruraform atripod.Therefore,twolegsof thistripodareformed by thelateralcrura,andthethirdlegisformedbythemedial cruraandcolumella.Inthiscase,bychangingthelengthand positionofeachleg,thepositioningofthenasaltipwillbe impacted.5,8Adamsonextendedthistheoryandproposeda
M-arcmodel,inwhichthemedialandlateralcruraare con-sideredaspartofanarcofdefinedlength,alsotakinginto accountthedistancebetweenthedomus.7,8Thesetheories
arecomplementary,andareessentialwhenplanninganasal surgery.
The use of nasal sutures is becoming an increasingly popular option, is easy to learn and has a low risk of complications. In the literature, studies that objectively evaluate the changes in facial angles postoperativelyare scarce.5 In ourstudy,preoperatively,and12 monthsafter
increasingandmaintainingtheprojectionandnasaltip rota-tion.Thesesuturesaremodificationsofpreviouslydescribed techniques.9
Themedialintercruralsuturewasoriginallydescribedas atechniquetoincrease boththe projectionand the rota-tionofthenosetip.The nasaltiprotationsuturehasalso been described, withthegoalof increasinghead rotation andpromotingaslightretractionofcolumella.9
This study aims to evaluate measures of rotation and nasal tip projection with the use of medial intercrural andnasaltiprotationsuturesatthetwelfthpostoperative monthfollowingprimaryendonasalrhinoplasty.
Methods
This study was approved by the ethics committee of the institution(003/2012-06).
Datacollectionwasperformed prospectivelyfrom Jan-uary2011toDecember2013bytheresearcher.
Twenty-seven patients were selected in a study of a contemporarylongitudinalcohort.Patientsincludedinthe study had noses with predominantly Caucasian features complaining of little rotation and/or nasal projection. Exclusion criteria: patients who had undergone previous rhinoplasty, andthoseagedunder18.Prior tosurgery, all patientssignedafreeandinformedconsentformapproved bytheethicscommittee.Nopatientwaslosttofollow-up.
Theselectedpatientsunderwentabasictechnique rhino-plasty (Table 1) performed by the same surgeon, with application of medial intercrural and nasal tip rotation sutures. The septocolumellar suture, to close the access incision,wascarriedoutatthesamelevel.
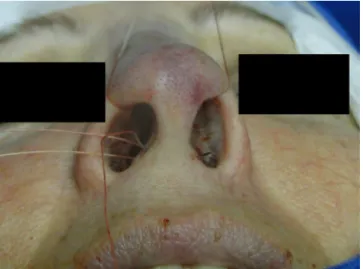
The medialintercruralsutureisperformedwithaclear Nylon4.0filamentaftercolumellarpocketdetachment,as shown in the figures below. The 5mm curved needle is passedabovetheinsideofthebaseofthecolumellarpocket towardtheexternalregion(Fig.1),where,bythesameexit orifice,theneedlepassesthroughthecolumellaandexits at thesame levelonthe oppositeside (Fig.2).Using the sameorifice,theneedlereturnstotheinsideofthepocket, wherethreeapproximationknotsaretied(Figs.3---5).Then, thisstitchispassedthroughseptalcartilage,inapoint5mm posteriortoitscaudalrim,endingwiththreeknots(Fig.6). Thesutureisburiedinthemucosa,withoutinvolvementof thisstructure.Intheoriginaldescription,theapproximation knotsarenotperformed.
Table 1 Basic technique for rhinoplasty. Steps of basic techniqueforrhinoplasty.
Basictechniqueforrhinoplasty
Septocolumellarandintercartilaginousincision Resectionofmembranousseptum
Detachmentofthenasaldorsumandperiosteum Upperlateralcartilagessplitting
Humpremoval Lateralfracture
Dissectionofcolumellarpocket Sutures
Source:Author.
Figure1 Intercruralmedialsuture.Step1---passagewitha 5mmcurvedneedleabovethebaseofcolumellarpockettothe externalaspect.
Figure2 Intercruralmedialsuture.Step2---usingthesame exitorifice,theneedletraversesthecolumellaandexitsatthe samelevelontheoppositeside.
Figure4 Intercruralmedialsuture.Step4---passageofthe needletothesidewherethesuturebegan.
Figure5 Intercruralmedialsuture.Step5---tyingthree fixa-tionknots.
Figure6 Intercruralmedialsuture.Step6---passingthepoint throughseptalcartilage,5mmposteriortothecaudalrim.
In the cephalic rotation suture, which is applied at a distance of 5mm below the columellar apex, the needle ispassed fromthe pockettotheexternal region(Fig.7), returningthrough the same hole tothe opposite side, at thesamelevel(Fig.8),where,throughthesamehole,the
Figure7 Nasal tiprotationsuture.Step 1---5mmbelowthe apexofthecolumella,theneedleispassedfromthepocketto theexternalaspect.
Figure8 Nasaltiprotationsuture.Step2---theneedlereturns throughthesameorificetotheoppositeside,atthesamelevel.
needlereturnstothepocket(Fig.9);insequence,thesuture istrespassedatapoint5mmbehindandbelowthe nasosep-tal angle, ending with three knots (Fig. 10). The suture is buried inthe mucosa, alsowithout involvement of this structure.
Figure9 Nasaltiprotationsuture.Step3---throughthesame orifice,theneedlereturnstothepocket.
Figure10 Nasaltiprotationsuture.Step4---theneedleis trespassed5mmbehindandbelowthenasoseptalangle.
Figure11 Nasolabialangle.Analysisofnasalrotation.
Figure12 Nasalprojection.Analysisofnasalprojection.
Figure 13 Preoperative. Nasal measures in preoperative period.
Astatistical analysiswascarriedout.Foradescription ofquantitative variables,mean, median,minimum value, maximumvalueandstandarddeviationstatisticsweretaken intoaccount.Forevaluationofvariables’normality condi-tion, Shapiro---Wilk test was considered. For assessment of whether or not a difference between time points of assessment(preandpost)existed,inrelationtothe varia-bles of interest, the Student’s t-test for paired samples wasapplied. p-Values <0.05 were considered statistically significant.
Results
Thesampleusedinthisstudyconsistedof27people, includ-ing9males(33.3%)and18females(67.7%).
Figure14 Postoperative.Nasalmeasuresinlate postopera-tiveperiod.
alternativehypothesisofdifferentmeanangles.Nasal rota-tionshowedastatisticallysignificantincrease(Table2).
We tested the null hypothesis of equal mean projec-tionsinbothassessmenttimepoints(preandpost) versus the alternative hypothesis of different mean projections. Therewerenostatisticallysignificantchangeswithrespect tonasalprojection(Table3).
Discussion
Inrecentyears,techniquesusedinrhinoplastyhavechanged frommoreinvasiveprocedureswithremovalofstructures,
Figure 15 Preoperative. Nasal measures in preoperative period.
Figure 16 Postoperative. Nasal measures in postoperative period.
tomore conservativeprocedures focused onrepositioning and structuring of existing tissues. This occurred mainly becauseofthedevelopmentoflatecomplicationsresulting fromnasalhealing,thatsometimescausedchangesinnasal formandfunction.10,11
The incorporation of the measures planned in the immediate pre-operative period is a major challenge in rhinoplasty. When planning the optimal approach during surgerythesurgeonshouldanticipatethehealingforcesand takeintoaccountthesupportmechanismsofthenasaltip.1
Therhinoplastyshouldfocusonproperlevelsof stabil-ity,symmetry,rotationandprojectionthatwillresistnose
Figure 18 Postoperative. Nasal measures in postoperative period.
healingforces,withmaintenanceofsatisfactorylong-term results.Aninappropriateresectionofcartilageandtheuse of grafts and sutures can lead to nasal tip deformities, includingptosis,alarcollapse,retraction,andpinching.8
Several techniques aredescribed for the treatment of nasaltipptosis,includingsurgicalproceduresandminimally invasiveactions,suchastheapplicationofbotulinumtoxin. Thesurgicalaccesscanbecarriedoutthroughanendonasal approach,oranexternaltechnique.3Openrhinoplastyhas
risksinherenttotheprocedure,suchasgreaterdamageto nasalsupportmechanismsandthefrequentneedfor multi-plegrafts,whichcarryariskofmigrationandexposureof thegraft,especiallyinthin-skinnedpatients.10
The literature describes numerous maneuvers to cor-rect noses with little rotation and projection, including
cephalic resection of upper lateral cartilage, sliding of lateralcrus,tongue-in-groove,grafts,andmembranous sep-tumresection.8
Zuliani3usestheopenrhinoplastyassociatedwithlower
toupperlateralcartilagesuspension(LUCS)incasesofnasal ptosis;24patientschangedtheirnasolabialanglefrom83.4◦
preoperativelyto102.3◦oneyearaftersurgery.When
com-pared to the use of sutures presented in this study, the techniquereportedbyZulianihasshownamoresignificant increaseinnasalrotation,butwithamoreaggressive tech-niquethatrequiredanexternalaccess.
Inaretrospectivestudyof62patientsundergoing exter-nalrhinoplasty,IngelsandOrhan5concludedthatsixmonths
aftersurgery,theuseofthecolumellarpostincreasedthe rotationandprojectionofthenasaltip,aneffectwhichis accentuatedbyremovingthecephalicportionoftheupper lateralcartilages.Thisincreasewasnotmeasured,andboth thesampleandthetechniquewerenotstandardized.
The tongue-in-groove technique gives good results in patientsundergoingrhinoplasty, withlittlerotationofthe nasaltip,but withaproperprojection.8The resultswere
evaluatedsubjectively,preventingcomparisonsandfuture standardizations.
Patrocínio12evaluated20patientswhounderwent
rhino-plastywiththeuseofa‘‘lateralcrurasteal’’techniqueto increasenasalrotationinthelatepostoperativeperiod,with ameanincreaseof20◦ inthelatepostoperativeperiod,a
statisticallysignificantoutcome.
The columellar post is a rectangular autologous graft that is fixed between the medial crura, with the aim to support and maintain the projection and rotation of the nasal tip. This structure is routinely used when per-forming an open technique, due to the inherent injury of the support mechanisms, but may also be used in endonasalapproaches.13Toriumi11describedtheimportance
ofsuturingthecaudalseptuminthemedialcrura (tongue-and-groove)tostabilizethenasalbase,inassociationwith the use of the columellar post. Combined witha higher degreeofinjuryofstructuresforachievingaccess,thereare stillcomplicationsresultingfromtheuseofthegraft.The
Table2 Descriptivestatisticalanalysisofnasalrotation.
Timing Nr.ofcases Mean Median Minimum Maximum Standard deviation
p-Valuea
Pre 27 96.8 96.6 77.4 111.6 9.2
Post 27 105.2 106.6 85.1 122.1 8.3
Post-pre 27 8.4 8.7 −7.4 23.0 6.8 <0.001
a Student’st-testforpairedsamples;p<0.05.
Table3 Descriptivestatisticalanalysisofnasalprojection.
Timing Nr.ofcases Mean Median Minimum Maximum Standard deviation
p-Valuea
Pre 27 0.69 0.69 0.49 0.85 0.09
Post 27 0.67 0.66 0.55 0.85 0.07
Post-pre 27 −0.02 −0.02 −0.20 0.16 0.08 0.184
complicationsencounteredwiththeuseofgraftsincludea badposition,displacement, induration,resorption,visible irregularities,extrusion,infection,atrophy,andsofttissue deformities.14,15
The use of the horizontal columellarpost proposed by Margulis4waseffectiveinstabilizingthenasaltipinpatients
withsevereptosis atthe tip.The use ofshell-typegrafts increasesnasal projection;however, thisoptionshouldbe avoidedinpatientswiththinskin,duetotheriskofexposure andextrusion.11 Thistypeofgraftshouldbecamouflaged,
especiallyinpatientswiththinskin. Theuse ofsutures is veryadvantageousforthesepatients, becausethereis no markingontheoverlyingskin.
In 2011, Cingi14 described the triple suture of
carti-lage,amodificationofthetongue-in-groovetechnique,with the use of figure-of-eight sutures --- a technique that did not exhibit complications and had very good subjective results.This techniqueimproves therotationof thenasal tip,presentsagradualadjustmentandallowsthecorrection ofanexcessivecolumella.Theauthorsdidnotstandardize theirmeasures,complicatingcomparisonswithother tech-niques.
For endonasal correction of hypoprojected tips, vari-oustechniqueshavebeendescribedbyPastorek16including
interdomalsuture,useofacolumellarpost, pre-maxillary graftsandanextendedcolumellargraft,allwithsatisfactory results.
The original description of sutures used in this study wasmade by Guyron17 in 1998; this authordescribed the
sutureat thebase ofmedialcruraandsofttissueremoval between the crura, as well as the use of U-sutures for bringingthefeettogether,assumingthatthecorrectionof hypoprojection should involve medial crura, according to thetripodmodel.6Inthisstudy,initiallythreeapproximation
knotswereappliedtoachieveabettercolumellarcontour, withafinalestheticeffectsimilartothatachievedbythe techniqueofcolumellarpost placement,in additiontoan associationwiththesutureofrotationofthenasaltip.This technique differs from the usual septocolumellar suture, sinceitallowsgreatermedialcrurastabilization,combined withthepossibilityofgreaterunevennessofheightbetween stitches,without affectingtheoverlying mucosa,sinceall thesuturesandknotsremainburied.
Inan objectivestudy oftheendonasalrhinoplasty con-ductedbyPasinato,2theauthormeasuredtheangles,both
in preoperative and in early postoperative periods, and reportedan increaseof8.6◦ for thenasolabial angleafter
theprocedure.Therewasneithercomparisonwiththe tech-niqueperformed,norstandardizationamongpatients.
The nasal techniques using sutures to increase rota-tion and nasal tip projection have enjoyed an increase in popularity, appearing as an option in both open and endonasalrhinoplasty.3Thesetechniques havepredictable
and controlled results, and they meet the most current principlesof rhinoplasty---conservationof structureswith non-destructive techniques.3,10 Many surgeons agree that
reversible, non-destructive, and structure-repositioning techniques should beused in preference to more aggres-sive techniques and of an indiscriminate use of grafts.7
Remodeling and positioning of structures can be accom-plished throughsutures, without an unnecessary sacrifice ofstructures.7,15
The medial intercrural suture can both increase or decrease nosal tip projection, depending on where the suture is anchored tothe nasal septum.9 Patients with a
nasal base lacking adequate structure are more likely to exhibithypoprojectedandhyporotatednoses.Stabilization ofthenasalbase mayassistinincreasingnasalprojection and rotation, and in maintaining an increased nasolabial angle. Nasal base stabilization is an essential step in the long-termmaintenanceofnasaltipposition.11Inthisstudy,
adistanceof5mmposteriortothecaudalseptumwas stan-dardized, although theheightwasnot,and theanchoring point was appliedat the samelevel of the medialcrural suture,whichmayhaveresultedintheabsenceofsignificant changesinnasalprojection.Ifthesutureisanchoredinthe nasalspinearea,therewillbeapotentialforreductionof projectionandalsoofnasalrotation.Inthisstudy,thereis alsothepotentialfor alack ofchange innasalprojection because of a beta error froman insufficient sample size. Wedidnotobservetheslightretractioninitiallydescribed byBehmand,Ghavani,andGuyuron,9probablybecausethe
firstsuturefortheapproximationofthemedialcruradoes notallowtheseptumtoexceedthislimitduringknot anchor-inginthesequenceofthestitch---aprocedurenotdescribed intheoriginaltechnique.Adecreaseoflobuleandcolumella alsooccurs.
The nasal tip rotation suture, as the name implies, increases the cephalic rotation of the nasal tip and can also result in columellar narrowing. A slight flattening of thecolumellacanalsooccur.9
Theeffectsofthesuturesareinfluencedbythedegreeof theirtightening,thethicknessofthecartilage,theamount ofsubcutaneoustissueandthethicknessoftheskin.9There
are numerous techniques described to increase the rota-tion and projection of the nasal tip; however, there are fewobjectivereportsaftersurgery,especiallylongterm,to allowonetoquantifytheeffectivenessofthesetechniques.5
Thishindersfuturecomparativestudiesandtheselectionof the optimal technique for each patient,according to the resulttobeachieved.
Modificationsoccurringin termsof tiprotationmaybe real, in which the nose tip position is changed, or illu-sory,throughchangesinthedorsum,columella,andinthe contourofthetipitself.11
In additionto the cartilaginous---osseous structure, the appearanceofnasaltipalsodependsonsubcutaneous tis-sue. In the case of weak cartilage, with thick skin and abundantsubcutaneoustissue,theresultsareusuallypoor. Itshouldbenotedthatthelowerlateralcartilagesarethe mainsupportingstructuresofthenasaltip.Therefore,any excess,deficiencyorchangeinthesecartilageswilldirectly affecttheoverlyingshapeoftheskin.9
Thelong-termresultsaremorepredictableandreliable withthe use of precisely positionedsutures, and withan understandingoftheirinteractionwiththenasaltipwhether they are used alone or in combination.15 These sutures
thatthe tighteningof theknots is acriticalstep,andfor bestresults it shouldbedone gradually. In thisstudy,we observedonecaseofcolumellainfection,whichresponded promptlytooralantibiotics.
Inthisstudy,therewasnocombineduseofthesesutures withotherstitches,becauseofitsmainobjective;however, thiscanbedoneandhasbeenwidelyusedinrecentyears, withquitesafeandpredictableresults.9Itisworthnoting
thatthisis anon-comparativestudy,andthatfuture stud-iescanbeperformedtocomparethistechniquewithother procedures,perhapsfacilitatingandmorepreciselytailoring thesurgicaltechniquetobeused,dependingonthespecific gainforthepatientandavoidingtheuseofmoreaggressive techniques (whenthere isnoneed), and of lesseffective techniquesinnosesrequiringmoresignificantchanges.
The sutures are considered indispensable for a refine-mentofthenasaltipsurgery.18
Conclusion
Thisstudy denomstratedthatmedialintercruralandnasal tiprotationsuturesareeffectiveinincreasingthenasolabial angle inCaucasian patientsundergoingprimaryendonasal rhinoplasty.Thesuturesdidnothaveasignificanteffecton nasalprojection.
Conflicts
of
interests
Theauthorsdeclarenoconflictsofinterest.
References
1.DobratzEJ,TranV,HilgerPA.Comparisonoftechniquesusedto supportthenasaltipandtheirlong-termeffectsontipposition. ArchFacialPlastSurg.2010;12:172---9.
2.PasinatoR, Mocellin M, Arantes M, Coelho MS,Dalligna DP, Soccol A. Pre and post operative facial angles in patients
submitted to rhinoplasty. Arq Int Otorrinolaringol. 2008;1: 393---6.
3.ZulianiGF,SilverWE.Analysisofnasalptosiscorrectionusing lowerlateraltoupperlateralcartilagesuspension.ArchFacial PlastSurg.2001;13:26---30.
4.MargulisA,HarelM.Managementofseveretipptosisinclosed rhinoplasty:thehorizontal columellarstrut.JPlastReconstr AesthSurg.2007;60:400---6.
5.IngelsK,OrhanKS.Measurementofpreoperativeand postop-erativenasaltipprojectionandrotation.ArchFacialPlastSurg. 2006;8:411---5.
6.Robinson S, Thornton M. Nasal tip projection: nuances in understanding,assessment,andmodification.FacialPlastSurg. 2001;2:158---65.
7.TasmanA,LohulsP.Controloftiprotation.FacialPlastSurg. 2012;28:243---50.
8.FriedmanO,KochCA,SmithWR.Functionalsupportofthenasal tip.FacialPlastSurg.2012;28:225---30.
9.BehmandRA,GhavaniA,GuyuronB.Nasaltipsutures.PartII: Theinterplays.PlastReconstrSurg.2003;112:1130---45. 10.Perkins S,Patel A.Endonasal suturetechniques intip
rhino-plasty.FacialPlastSurgClinNorthAm.2009;17:41---54. 11.ToriumiDM.Structureapproachinrhinoplasty.FacialPlastSurg
ClinNorthAm.2002;10:1---21.
12.PatrocínioLG,PatrocínioTG,BarretoDM,SubhanYS,Patrocínio JA.Evaluationoflateralcruralstealinnasaltipsurgery.JAMA FacialPlastSurg.2014;16:400---4.
13.AnsariK.Graftsandimplantsinrhinoplasty---techniquesand long-term results. Oper Tech Otolaryngol Head Neck Surg. 2008;19:42---58.
14.CingiC,SonguM.Triplecartilagecombiningsuturetechnique inrhinoplasty.AmJRhinolAllergy.2011;25:429---31.
15.BehmandRA,GhavaniA,GuyuronB.Nasaltipsutures.PartI: Theevolution.PlastReconstrSurg.2003;112:125---9.
16.Pastorek N, Ham J. The underprojecting nasal tip: an endonasalapproach.FacialPlastSurgClinNorthAm.2004;12: 93---106.
17.GuyuronB.Footplatesofthemedialcrura.PlastReconstrSurg. 1998;101:1359.