www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Endoscopic
sinus
surgery
dissection
courses
using
a
real
simulator:
the
benefits
of
this
training
夽,夽夽
Bibiana
Fortes
∗,
Leonardo
Balsalobre,
Raimar
Weber,
Raquel
Stamm,
Aldo
Stamm,
Fernando
Oto,
Nathália
Coronel
HospitalProfessorEdmundoVasconcelos(HPEV),SãoPaulo,SP,Brazil
Received10February2014;accepted3February2015 Availableonline19October2015
KEYWORDS
Nasalcavity; Dissection; Trainingcourses
Abstract
Introduction:Endonasalsurgeriesareamongthemostcommonproceduresperformedin oto-laryngology.Duetodifficultyincadaveracquisitionandtheintrinsicrisksoftrainingresidents duringoperationsonrealpatients,nasosinusalendoscopicdissectioncoursesutilizingreal sim-ulators,suchastheSinusModelOtorhinoNeuroTrainerarebeingdevelopedasanewtechnique tofacilitatetheacquisitionofbetteranatomicalknowledgeandsurgicalskill.
Objective:ToevaluatetheefficacyofnasosinusalendoscopicdissectioncourseswiththeSinus ModelOtorhinoNeuroTrainersimulatorinthetrainingofotolaryngologysurgeons.
Methods:Aprospective,longitudinalcohortstudywasconducted with111otolaryngologists whoparticipatedinatheoreticalandpracticalcourseofendoscopicsurgerydissectionusing theSinusModelOtorhinoNeuroTrainersimulator,withapplicationofquestionnairesduringand afterthecourse.
Results:Fromthetenproceduresperformedutilizingthesimulator,theevaluationrevealed meanscoresfrom3.1to4.1(maximumof5).Seventy-sevenparticipantsansweredthe ques-tionnairesixmonthsaftertheendofthecourse.93%ofthemreportedthattheycouldperform theproceduresmoresafelyfollowingthecourse,98%reportedanimprovementintheir anatom-icalandclinicalknowledge,and85%relatedanimprovementintheirsurgicalability.Afterthe course,thenumberofendoscopicsurgeriesincreasedin40%oftherespondents.
夽 Pleasecitethisarticleas:FortesB,BalsalobreL,WeberR,StammR,StammA,OtoF,etal.Endoscopicsinussurgerydissectioncourses usingarealsimulator:thebenefitsofthistraining.BrazJOtorhinolaryngol.2016;82:26---32.
夽夽Institution:HospitalEdmundoVasconcelos,SãoPaulo,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](B.Fortes). http://dx.doi.org/10.1016/j.bjorl.2015.02.003
Conclusion: EndoscopicsinusdissectioncoursesusingtheSinusModelOtorhinoNeuroTrainer simulatorprovedtobeusefulinthetrainingofotolaryngologists.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Cavidadenasal; Dissecac¸ão; Cursosde capacitac¸ão
Cursosdedissecc¸ãodecirurgiaendoscópicanasossinusalemsimuladorreal---os benefíciosdestetreinamento
Resumo
Introduc¸ão: Cirurgias endonasais são as cirurgias mais realizadas na otorrinolaringologia. Devido àdificuldadede adquirircadáverese ao riscoinerenteem realizartreinamento em pacientesreais,cursosdedissecc¸ãoendoscópicanasossinusalemsimuladoresreais,como o sinusmodel otorhino---neurotrainer---S.I.M.O.N.T,sãouma novapropostadeaquisic¸ãode maiorconhecimentoanatômicoehabilidadescirúrgicas.
Objetivo: Avaliaraeficáciadoscursosdedissecc¸ãodecirurgiaendoscópicanasossinusalcom simuladorS.I.M.O.N.T.notreinamentodecirurgiõesotorrinolaringologistas.
Método: Estudodecoortecontemporâneolongitudinalcom111otorrinolaringologistasque par-ticiparamdecursoteórico---práticodedissecc¸ãoendoscópicanasossinusalemsimuladorreal S.I.M.O.N.T.,comaplicac¸ãodequestionáriosduranteeapósarealizac¸ãodocurso.
Resultados: Dosdezprocedimentosrealizadosnosimulador,aavaliac¸ãoapontouparamédias denotasquevariaramde3,1a4,1(máximode5).Setentaeseteparticipantesresponderama avaliac¸ão6mesesapósocurso.Declararamquehouveaumentodaseguranc¸aapósocurso,93% dosmesmos;98%disseramteraumentadooconhecimentoanátomo-clinicoe85%declararam umaumentodahabilidadecirúrgica.Quarentaporcentoaumentaramonúmerodecirurgias endonasaisapósocurso.
Conclusão:Cursos de dissecc¸ão de cirurgia endonasais com simulador real S.I.M.O.N.T. mostraramserúteisparaotreinamentodeotorrinolaringologistas.
©2015Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Endonasalsurgeriesareamongthemostperformedsurgeries inotolaryngology.Theyareconsideredthestandardof treat-mentofseveralsinusandnasalcavitypathologies.1,2Dueto theirimportance,residenttrainingisaconstantconcernin medicalresidencyservices.Themanipulationofanatomical structuresandsurgicalinstrumentsduringtheprocedureis challengingforinexperiencedsurgeons,duetothecomplex anatomyofintranasalregionandtheintimaterelationship withvitalstructures,suchasthebrain,carotidartery,and orbitcomponents.1---5
Currently, most training in endonasal surgery is con-ducted in the operating room on realpatients under the supervisionofmoreexperiencedsurgeons.2,4---6Since approx-imately5---10%ofendonasalsurgeriesdevelopcomplications andsincethelearningcurveforperformingsurgical proce-duresonrealpatientsmayaddanadditionalrisk,itwould be idealto minimize this risk as muchas possible. Thus, activities in dissection labs or in simulators, in addition to theoretical and practical courses of dissection, should beperformedandencouraged.However,thedevelopment of such laboratories has some challenges, including eth-ical, legal, financial and technical problems that hinder the acquisition of cadavers or animal models; therefore
thesurgicaltrainingprocessinotolaryngologyis gradually movingtowardtotheuseofsurgicalsimulators.2,4---7
Surgicalsimulatorscanbedividedintotwotypes:virtual simulatorsandrealanatomicalmodels.3Virtualsimulators arebasedoninteractivecomputerprograms,i.e.,theyuse virtual reality elements and mechanisms of direct inter-actionwithusers.3---5Conversely, theSinus ModelOtorhino NeuroTrainer(S.I.M.O.N.T.),arealanatomicalmodel,was created from images of anatomical structures, computed tomography,and endoscopic anatomical dissection videos ofcadavers,providingtraining,bydissection,ofendoscopic nasosinusalsurgery.3,4,8
Inthisservice,thesimulatoradoptedfortrainingduring theotolaryngologists’trainingcoursesistheS.I.M.O.N.T.,a realsimulator.
Training courses in nasosinusal surgery on cadavers provide unequivocal benefit to surgeons,9 but studies demonstratingequivalentresults incourseswithreal sim-ulatorsarestillneeded.
Objective
usingtheS.I.M.O.N.T.simulatortotrainotolaryngology sur-geons.
Methods
This research was conducted through a study of a longi-tudinal contemporary cohort. Three questionnaires were applied to otolaryngologists who took part in practical trainingcoursesinendoscopicnasosinusalsurgerywiththe simulatorintheyears2011and2012.Thecoursefeatures theoreticallecturesonanatomyaswellassurgicaland dis-sectiontechniqueconceptsinamodel.
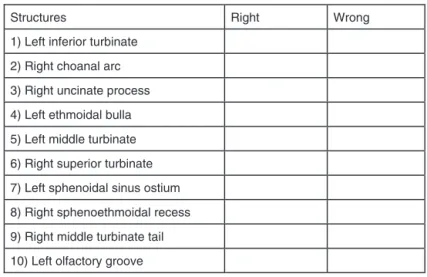
The first questionnaire (Fig. 1) was applied after the theoreticallecturesandbeforedissectionwithS.I.M.O.N.T. simulatorandaimedtothe basic knowledgeof endonasal anatomy of participants, by identifying ten anatomical structures.
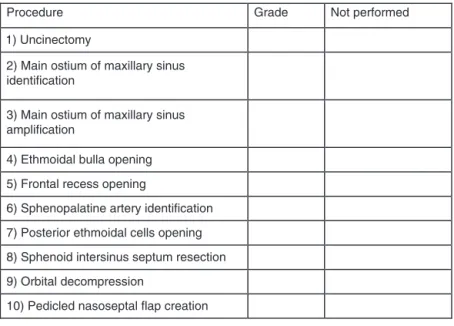
The second questionnaire (Fig.2)aimed toassess how closely the dissection in the model approximated reality, andwasappliedafterdissectionand theoreticallectures. Participants were required toassign grades (from 1 to5) comparingtenproceduresperformed employingendonasal surgeryinahumanbeingorinacadavertothesame proce-dure performed during dissectionof the S.I.M.O.N.T.;the subjects assigned a value of 0 when the procedure was not performed, 1 when the procedure was considered as completelydifferent,2forverydifferent,3forsomewhat similar,4 for very similar,and 5 for a completely similar procedure.
Thethirdandfinalquestionnaire(Fig.3)wasobtainedby telephoneorbye-mailatleastsixmonthsafterthecourse, toassesstheimpactofthetrainingwiththesimulatorinthe participant’smedicalpractice.
Participantswere dividedinto twogroups accordingto the surgical experience at the time of dissection with theS.I.M.O.N.T.GroupA(moreexperiencedtrainees) con-sisted of surgeons who performed at least one endonasal surgeryperweekandthosewhoperformedonceortwicea month.GroupB(lessexperiencedtrainees)comprised par-ticipants whoperformed less than onesurgery permonth andthose whoneverhadperformedanendonasalsurgery.
Results
Thestudyinvolvedtheparticipationof111surgeons.Sixty (54.1%)oftheseparticipantswereotolaryngologyresidents; 51(45.9%)otolaryngologistswhohadalreadygraduatedwith ameanof5.9yearsofpracticeinthespecialty,rangingfrom oneto23years.Fifty-onesurgeons(45.9%)whoperformed endonasalsurgerymorethanonceperweekand36(32.4%) whoperformed thesurgerytwotothreetimespermonth were classified as Group A. The other 18 (16.2%) partici-pantswhoperformedlessthanonemonthlyprocedureand six(5.4%)whohadneverperformedendonasalsurgerywere classifiedasGroupB.
Questionnaire1
The meanof thecorrectlyidentified anatomicalstructure for Group A was 88.4%, and for Group Bwas 86.2%. The anatomicalstructures mostcommonly mis-identified were the superior turbinate, olfactory groove, and sphenoeth-moidalrecess(Table1).
Name: ___________________________________________Age:______________
otorhinolaryngologi cal your
finish you
did
When training?
________________________________
Frequency of FESS:
( ) ≥ 1 per week ( ) 1-2 times per month ( ) ≤ 1 per month ( ) never
Point the structures below:
Structures Right Wrong
1) Left inferior turbinate
2) Right choanal arc
3) Right uncinate process
4) Left ethmoidal bulla
5) Left middle turbinate
6) Right superior turbinate
7) Left sphenoidal sinus ostium
8) Right sphenoethmoidal recess
9) Right middle turbinate tail
10) Left olfactory groove
___________________________________________________________ Name:
Age:______
Compare the procedures below performed in the S.I.M.O.N.T. model with the same
procedure in the conventional surgery.
1 – completely different
2 – very different
3 – a bit similar
4 – very similar
5 – completely similar
Procedure Grade Not performed
1) Uncinectomy
2) Main ostium of maxillary sinus identification
3) Main ostium of maxillary sinus amplification
4) Ethmoidal bulla opening
5) Frontal recess opening
6) Sphenopalatine artery identification
7) Posterior ethmoidal cells opening
8) Sphenoid intersinus septum resection
9) Orbital decompression
10) Pedicled nasoseptal flap creation
Figure2 Questionnaire2.
Questionnaire2
Of the ten procedures that were performed in the simu-lator, the evaluation of surgeons resulted in mean scores ranging from3.1 to4.1 (minimum of 1 and maximum of 5).Proceduresthat receivedthe lowestscoreswere pedi-cled nasoseptal flap creation (mean score 3.1), frontal recess opening (mean score 3.6), and posterior ethmoid bulla opening (meanscore 3.6). The procedures less per-formedwereresectionoftheintersinusalsphenoidseptum, orbital decompression, and pedicled nasoseptal flap cre-ation(Fig.4).
Questionnaire3
Ofthe 111initial participants, 77answered the question-naireatleastsixmonthsaftercompletingthecourse.Table2
demonstratesthepercentagesofeachresponse.
The last question of the questionnaire refers to the frequency of surgeries after the course. In thirty partici-pants(38.9%) thenumberof surgeriesincreased, whilein 47(61.1%)frequencyofsurgerymaintainedthesame.When stratifiedintoGroupA(moreexperienced)andGroupB(less experienced),Fig. 5shows an increase of 6%in the more experiencedgroup.
Discussion
S.I.M.O.N.T.presentsmanyadvantageswhencomparedwith animalorcadavericmodels,orwithvirtualsimulators:there isnoneedofaspecialplaceortechniqueforitsstorage;it iseasilycleanedafteruse;itusesthesamesurgical instru-mentsasusedinpractice;ithasthecapabilitytosimulate andrepresentdifferentdiseases;itlacksthebiologicalrisks inherentintraditionaldissectionsoffreshcadavers;andit can be used to dissect and train in almost any available space.Thisanatomicalmodelallowstrainingfornumerous proceduresduringthedissectioncourses.3,4,8,10,11
Name:______________________________________________________________
Age: __________
1. After you have participated in course, do you think you have acquired more security
in order to perform FESS?
( ) Yes ( ) No
2. Do you think the course helped you to acquire more anatomic-surgical knowledge?
( ) Yes ( ) No
3. Do you think is necessary to perform the course again?
( ) Yes ( ) No
4. Would you recommend the course to another person?
( ) Yes ( ) No
5. Did the course contribute to your surgical abilities?
( ) Yes ( ) No
6. How often do you perform FESS?
( ) 2-3 times per week ( ) > once a week
( ) 1-2 times per month
( ) <1-2 times per month
( ) never
Figure3 Questionnaire3.
This study aimed to evaluate the S.I.M.O.N.T. simula-torindissectioncoursesofendoscopicnasosinusalsurgery, becauseitisdifficultinBraziltoobtaincadaversfor achiev-ingsuchtraining.ThisisthefirstBrazilianstudyevaluating theroleofthesecoursesinarealsimulatorinascenarioof otolaryngologisttraining.
The first part of the study, involving Questionnaire 1, applied after theoretical lectures on anatomy and surgi-cal technique and prior to dissection, showed that both Group A and Group B, achieved a high rate of correct identificationofanatomicalstructures.This suggeststhat, in additionto thesimilarity between the anatomyof the
Table 1 Percentiles of correct answers about anatomic
structures.
Structures Group1(87) Group2(24)
n(%) n(%)
Leftinferiorturbinate 87(100%) 24(100%) Rightchoanalarc 81(93.1%) 24(100%) Rightuncinateprocess 70(80.5%) 18(75%) Leftethmoidalbulla 84(96.6%) 22(91.6%) Leftmiddleturbinate 86(98.9%) 23(95.3%) Rightsuperiorturbinate 64(73.6%) 13(54.2%) Leftsphenoidalsinus
ostium
79(90.8%) 21(87.5%)
Rightsphenoethmoidal recess
67(77%) 20(83.3%)
Rightmiddleturbinate tail
85(97.7%) 24(100%)
Leftolfactorygroove 66(75.9%) 18(75%)
Median 88.41% 86.19%
S.I.M.O.N.T. simulator and the human anatomy (Fig. 2), therewas alsoconsolidation of informationregarding the anatomical knowledgeprovided in thetheoretical part of the course. Thus, the need for theoretical classes in dis-section courses can be inferred.12 With regard to those structureswith highererror rate: right superior turbinate (RST), left olfactory groove (LOG), and right sphenoeth-moidalrecess(RSER),theinstructorsofthecourse(surgeons withextensiveexperience)wereaskedtoconductan inves-tigation on this result. As to RST, it was found that this structurewaslocatedmoreinferiorlythanwhereitisusually found inthebody.RegardingLOGandRSER, itisbelieved thatthereasonfor thelowpercentageof successmaybe
Table2 PercentagesofanswersfromQuestionnaire3.
Questions Yes No
. . . haveacquiredmore securityinorderto performFESS?
72(93.5%) 5(6.5%)
. . . haveacquiredmore anatomic-surgical knowledge?
76(98.7%) 1(1.3%)
. . . isnecessaryto performthecourse again?
33(42.8%) 44(57.2%)
. . . wouldyou
recommendthecourse toanotherperson?
75(97.4%) 2(2.6%)
. . .contributetoyour surgicalabilities?
PNFC
OD
SISR
PECO
SAI
FRO
EBO
MOMSA
MOMSI
UNCI
0 1 2 3 4 5
Figure4 Meangradesattributedtotheprocedures.PNFC,pediclednasoseptalflapcreation;OD,orbitaldecompression;SISR,
sphenoidintersinusseptum resection;PECO,posterior ethmoidal cellsopening; SAI,sphenopalatinearteryidentification;FRO, frontalrecessopening;EBO,ethmoidalbullaopening;MOMSA,mainostiumofmaxillarysinusamplification;MOMSI,mainostiumof maxillarysinusidentification;UNCI,uncinectomy.
61 (86%)
16 (14%)
71 (92%)
6 (8%)
Group A Group B
Figure5 Numberofsurgeons before andafter S.I.M.O.N.T
dissectioncourse,accordingtoexperiencegroups.
duetoalackofknowledgeorexperienceonthepartofthe participants.
Themeangradesoftheproceduresperformedinthe sim-ulator(Questionnaire2)rangedfrom3.1to4.1,foratotal of 5 points, suggesting that a dissection course using the S.I.M.O.N.T.allows goodtraining, and is comparableto a courseofdissectioninacadaver.
Pediclednasoseptalflapcreation(PNFC),frontalrecess opening (FROp), and posterior ethmoidal cell opening (PECBp) procedures obtained the lowest scores, probably because these are considered technically more complex, are not common, and also take longer toperform. Simi-lar findings weredescribed in cadaver dissection courses, where the surgeries involving the posterior ethmoid, the sphenoid, and thefrontal sinus were elected asthemost difficultprocedurestobecarriedout.12 Thissituationwas alsoconfirmed in astudy publishedby theotolaryngology departmentoftheJohnsHopkinsHospital,wherethe expec-tation of residents at the end of their training was only
toacquireconfidenceinperformingmaxillaryantrostomies andanteriorethmoidectomies.13
TheresultsinTable2showasignificantincreaseinsafety, anatomicalandsurgicalknowledge,andsurgicalskillafter thecourse;thus,itcanbeconcludedthattraininginareal simulatorissatisfactoryandeffective,especiallywhen aug-mentedbytheoreticalinstruction.About43%ofparticipants reportedthattheyfelttheneed totakethecourseagain, suggestingthatevenaftercompletionoftraining,the acqui-sitionofknowledgeisagreatchallenge;andthatmaybeonly acourse is notenough toprovide confidence tothe sur-geon.Yet 97% of otolaryngologists would recommend the course,reinforcingthepurposesoftheendoscopic nasosi-nusalsurgerydissectioncourse.
Finally,afterthecourse,whenparticipantswereasked iftherewasan increasein thenumberof theirsurgeries, about 40%answered affirmatively; andwhen thesubjects werestratifiedbyexperiencegroup,therewasanincrease from86%to92%inthegroupofthemostexperienced sur-geons, and consequently a decrease in those considered lessexperienced.Thissupportstheideathatsurgeonswere puttingintopracticethe knowledgeandskills acquired in thecourse, increasing their frequency of surgeries.Thus, despitethegoodresultsobservedinthisstudy,aconstant improvementin the qualityof anatomy and of the mate-rialusedinthesimulatorshouldbemaintained,inorderto optimallycorrespondtoacadavericexperience.
Conclusion
It was demonstrated that nasosinusal endoscopic surgical dissectioncourseswith theS.I.M.O.N.T., areal simulator, areuseful andbeneficialforthetrainingandqualification ofotolaryngologysurgeons.
Conflicts
of
interest
References
1.McFerranDJ,GrantHR,IngramsDR,FifeDG.Endoscopicsinus surgery:arejuniordoctorsbeingproperlytrained?AnnRColl SurgEngl.1998;80:359---63.
2.Arora H, Uribe J, Ralph W, Zeltsan M, Cuellar H, Gallagher A,etal.Assessmentofconstructorvalidityoftheendoscopic sinus surgery simulator. Arch Otolaryngol Head Neck Surg. 2005;131:217---21.
3.NogueiraJF,CruzDN.Modelosreaisesimuladoresvirtuaisem otorrinolaringologia: revisão de literatura. Braz J Otorhino-laryngol.2010;76:129---35.
4.Filho FV,CoelhoG, CavalheiroS, LyraM,Zymberg ST. Qual-ityassessmentofanewsurgicalsimulatorforneuroendoscopic training.NeurosurgFocus.2011;30:1---6.
5.FriedMP,SatavaS,WeghorstS,GallagherA,SasakiC,RossD, etal.Theuseofsurgicalsimulatorstoreduceerrors.In: Hen-riksenK,BattlesJB,MarksES,LewinDI,editors.Advancesin patientsafety:fromresearchtoimplementation,vol.4.2005. p.165---77.Rockville.
6.GlaserAY, HallCB, Uribe SJ,FriedMP.The effects of previ-ouslyacquiredskillson sinussurgerysimulatorperformance. OtolaryngolHeadNeckSurg.2005;133:525---30.
7.Edmond CV Jr. Impact of the endoscopic sinus surgical simulator on operating room performance. Laryngoscope. 2002;112:1148---58.
8.NogueiraJF, StammAC,LyraM,BalieiroFO,Leão FS. Build-inga realendoscopic sinus and skull-basesurgery simulator. OtolaryngolHeadNeckSurg.2008;139:727---8.
9.GurrA,HansenS,MinoviA,ProbstG,DazertS.Therelevance ofanatomicalcoursesinENT-education.Laryngorhinootologie. 2009;88:789---92.
10.Zymberg S, Guimarães Filho FV, Lyra M. Neuroendoscopic training:presentationofanewrealsimulator.MinimInvas Neu-rosurg.2010;53:44---6.
11.StammA,NogueiraJF,LyraM.Feasibilityofballoonin endo-scopic sinus surgery simulator. Otolaryngol Head Neck Surg. 2009;140:320---3.
12.BraunT,BetzCS,LedderoseGJ,HavelM,StelterK,KuhnelT, etal. Endoscopic sinus surgerytrainingcourses: benefitand problems---amulticentreevaluationtosystematicallyimprove surgicaltraining.Rhinology.2012;50:246---54.