w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
A
model
for
the
functional
assessment
of
elderly
with
myeloid
neoplasms
Ana
Lúcia
Ippolito
Carbonell
a,∗,
Renata
Maceu
Salhab
a,
Viviana
Giampaoli
b,
Maysa
Seabra
Cendoroglo
a,
Maria
de
Lourdes
Chauffaille
aaUniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil bUniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received1November2014
Accepted26December2014
Availableonline17February2015
Keywords:
Performancetests
Karnofskyperformancestatus
Aged
Leukemia,myeloid
Myelodysplastic-myeloproliferative diseases
a
b
s
t
r
a
c
t
Objective:Myeloidneoplasmsare heterogeneousdiseases thataremoreincident inthe
elderly.Thegoalsofthisstudyweretoaggregateageriatricapproachtothepatient
assess-ment,toshowtheimpactofgender,age,hemoglobinconcentrationandcomorbiditieson
the functionalityofelderlywithmyeloid neoplasmsandtobetterunderstandhowthe
instrumentsoffunctionalassessmentworkaccordingtotheaggressivenessofthedisease.
Methods:Elderlypatients (≥60 years old)with myeloidneoplasms wereassessed using
the Karnofskyscale,Eastern CooperativeOncologic Groupscale,andbasic and
instru-mentalactivitiesofdailylivingscales.Thehematopoieticcelltransplantation-comorbidity
indexassessedthecomorbidities.Amixedlogisticalregressionmodelwasfittedto
esti-mate the impactof gender,age,hemoglobinconcentrationandthe hematopoieticcell
transplantation-comorbidityindexonpatients’functionality.
Results:Eighty-twopatientswithameanageof72.8years(range:60–92years)were
evalu-ated.EightypercenthadgoodKarnofskyandEasternCooperativeOncologicGroupscales
and39%wereindependentaccordingtothedailylivingactivityscales.Allofthepatients
withpoorKarnofskyandEasternCooperativeOncologicGroupscaleswereclassifiedas
dependentbythedailylivingactivityscales.Themixedlogisticregressionmodelsshowed
thatage,gender,hemoglobinconcentrationandthecomorbidityindeximpactedonthe
dailylivingactivityscales.KarnofskyandEasternCooperativeOncologicGroupscaleswere
affectedbyhemoglobinandthecomorbidityindex.Themodelhypothesizedthehemoglobin
concentrationatwhichtherewasahigherriskofpoorKarnofskyandEasternCooperative
OncologicGroupscales.Thishemoglobinconcentrationdependedoncomorbiditiesandon
theaggressivenessofthemyeloidneoplasm.
Conclusion: Thegeriatricapproachimprovedthesensitivityandspecificityofthepatients’
assessment.HemoglobinconcentrationassociatedtotheriskofpoorKarnofskyandEastern
CooperativeOncologicGroupscalesdependedonthecomorbidityscoreandonthedisease
aggressiveness.TheKarnofskyandEasternCooperativeOncologicGroupscaleshadhigher
sensitivityinpatientswithmoreaggressivediseases.
©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published
byElsevierEditoraLtda.Allrightsreserved.
∗
Correspondingauthorat:RuaDiogodeFaria,824,04037-000SãoPaulo,SP,Brazil.
E-mailaddress:[email protected](A.L.I.Carbonell).
http://dx.doi.org/10.1016/j.bjhh.2015.02.003
1516-8484/©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.PublishedbyElsevierEditoraLtda.Allrights
Introduction
Myeloidneoplasms(MN)are agroupofheterogeneous
dis-eases that include myeloproliferative neoplasms (MPN),
myelodysplastic syndromes (MDS) and acute myeloid
leukemia (AML). All these diagnosis are more incident
andprevalentinelderlyindividuals.
This group of diseases includes from indolent entities
suchaspolycythemiaveraandessential thrombocythemia,
toaggressive diseases,suchas AMLand MDS with excess
ofblasts.Chronicmyeloidleukemiaand myelofibrosishave
somerisktoevolveaggressively.1
ThemanagementofolderindividualswithMNtakesinto
account characteristics related to the patient and to the
disease.2–6Thechronologicalage,theperformancestatus(PS)
andthecomorbidityscorearepatient-relatedvariablesthat
areconsideredduringtreatmentdecisionmakingofelderly
individuals.7–9
The PS assessment is carried out using the Karnofsky
PerformanceScale10(KPS)orbytheEasternCooperative
Onco-logicGroup11(ECOG)scale.However,overthelastthirtyyears,
severalstudieshavedemonstratedthelowsensitivityofthese
instruments to evaluatefunction inolder individuals with
cancer.12–14Thus,ithasbeenrecommendedtoaggregate
geri-atrictoolstothePSassessment.
The major clinical challenge in the management of all
myeloidneoplasmsisthetreatmentofAMLinolderpatients.
Depending on the clinical and functional reserve of the
patient,thetherapeuticapproachmaybeexcessivelytoxic.2
Thus,itisveryhelpfultodistinguishtheimpactoftheaging
processseparatedfromtheimpactofthedisease.15
Theobjectivesofthisstudyweretoassessthe
functional-ityofelderlypatientswithMNaggregatingthebasicactivity16
(ADL)andinstrumentalactivity17(IADL)ofdailylivingscales
totheKPSandECOGandtoevaluatetheimpactofgender,
age,hemoglobin(Hb)concentrationandcomorbidityscoreon
thefunctionalityofthesepatients.Athirdobjective wasto
designamodeltoshowhow functionalassessment
instru-mentsworkinrespecttotheaggressivenessofthedisease.
Methods
Elderlypatients(≥60yearsold)withMNfollowedatthe
Hema-tologicOutpatientClinicoftheUniversidadeFederaldeSão
Paulo,(UNIFESP)wereincludedinthisstudy.
Diagnoseswere basedontheWorld HealthOrganization
(WHO)Classification oftumors ofhematopoietic and
lym-phoid tissues18 using the analysis ofperipheral blood and
bonemarrowsmears,thehistologyofbonemarrowbiopsy,
andimmunophenotypic,cytogeneticandmolecularstudies.
The patient’s functional evaluation was performed by
a hematologist just before the clinical consultation and
included PS assessedemploying the KPS and ECOG scales
andfunctionalstatuswiththeADLandIADLscales.
Comor-biditieswere evaluatedaccording tothehematopoieticcell
transplantation-comorbidityindex(HCT-CI)developedby
Sor-rorin2005.19
The Hb concentration was measured by an automated
technique employing a multichannel hematology analyzer
(CELL-DYN Ruby, Abbott Diagnostic Division)using a blood
sampletakenbeforetheconsultation.
Patientswithtransfusionpositivestatusreceivedredblood
cells priortothedeterminationoftheHb concentrationin
the monthpreceding thefunctional assessment. The
deci-siontotransfusewasbasedonthedropinHbanditsrelated
symptoms.Demographicandclinicaldatawereobtainedfrom
medicalrecords.
ThestudywasapprovedbyResearchEthicsCommitteeof
UNIFESP(#0262/10) andtheprocedures undertakenwerein
accordancewiththeDeclarationofHelsinkiof1975,revised
in2008.20Allpatientssignedinformedconsentforms.
Statisticalanalysis
Analyses ofmeans ofage and Hb concentrationwere
per-formed using Student’st test or ANOVA with Tukey’s test.
Thefrequenciesofcategoricalvariableswereevaluatedwith
Fisher’sexacttest.
Twomixedlogisticregressionmodelswerefittedtoassess
theimpactofgender,age,HCT-CIandHbconcentrationonPS,
dichotomizedasgood(KPS≥80%andECOG<2)orpoor,and
onfunctionalstatus,asindependentordependent(needhelp
inatleastonedailytask).
Generally,mixedmodelsconsidertheinformation
hierar-chicallystructuredattheunitandclusterlevels.Thesecluster
levelsresultfromagroupingprocessoutlinedby
character-istics shared bythe units. Moreover,in mixed models the
assumptionofindependenceisviolated,because thereisa
correlationbetweentheunitsthatbelongtothesamecluster.
Randomeffectsareincludedonconsideringthisfact.
Mixed models incorporate these random effects and
estimatethemforeachgroup.Therefore,thegroupsare
repre-sentedbyrandomeffectsandthevariabilityacrossthegroups
isdescribedbytheinterceptortheslopevariability.Themixed
modelbelongstogeneralizedlinearmixedmodels(MLGM),
whichisanextensionofgeneralizedlinearmodels(GLM).21,22
StatisticalanalysiswasperformedusingRstatistics(v2.15)
andtheStatisticalPackagefortheSocialSciences(SPSS–v18).
Results
Eighty-twopatients,40menand42women,withameanage
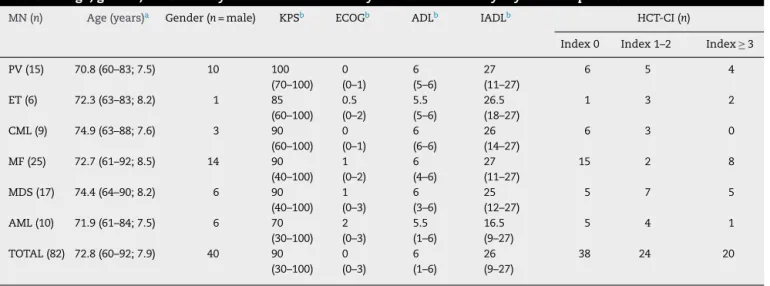
of72.8yearsold(range:60–92years),wereevaluated.Table1
showsthedescriptivestatisticsofthedemographicdata,
func-tionalityscoresandcomorbidityindices.
Ofthe fifteen patients withpolycythemiavera (PV) and
six with essential thrombocythemia (ET), 73% and 50%
wereJAKV617Fpositive,respectively.Ninetypercentofthese
patientsweretakinghydroxycarbamidetocontrolthedisease.
Alltheninepatientswhohadchronicmyeloidleukemia
(CML)wereinthechronicphase;sevenweretakingimatinib
mesylateandfourwereinmolecularremission.
Nine out of25 patientswith myelofibrosis (MF)were in
the sclerotic phase, two inblastic transformation and the
remaining14wereinthecellularphase.Elevenpatientswere
Table1–Age,gender,functionalityscoresandcomorbidityindicesstratifiedbymyeloidneoplasm.
MN(n) Age(years)a Gender(n=male) KPSb ECOGb ADLb IADLb HCT-CI(n)
Index0 Index1–2 Index≥3
PV(15) 70.8(60–83;7.5) 10 100 (70–100)
0 (0–1)
6 (5–6)
27 (11–27)
6 5 4
ET(6) 72.3(63–83;8.2) 1 85 (60–100)
0.5 (0–2)
5.5 (5–6)
26.5 (18–27)
1 3 2
CML(9) 74.9(63–88;7.6) 3 90 (60–100)
0 (0–1)
6 (6–6)
26 (14–27)
6 3 0
MF(25) 72.7(61–92;8.5) 14 90 (40–100)
1 (0–2)
6 (4–6)
27 (11–27)
15 2 8
MDS(17) 74.4(64–90;8.2) 6 90 (40–100)
1 (0–3)
6 (3–6)
25 (12–27)
5 7 5
AML(10) 71.9(61–84;7.5) 6 70 (30–100)
2 (0–3)
5.5 (1–6)
16.5 (9–27)
5 4 1
TOTAL(82) 72.8(60–92;7.9) 40 90 (30–100)
0 (0–3)
6 (1–6)
26 (9–27)
38 24 20
MN:myeloidneoplasm; PV:polycythemiavera;ET:essentialthrombocythemia;CML:chronicmyeloidleukemia;MF:myelofibrosis;MDS: myelodysplasticsyndromes;AML:acutemyeloidleukemia;KPS:Karnofskyperformancescale;ECOG:EasternCooperativeOncologyGroup scale;ADL:basicactivitiesofdailylivingscale;IADL:instrumentalactivitiesofdailylivingscale;HCT-CI:hematopoieticcell transplantation-comorbidityindex.
a Mean(min-max;standarddeviation).
b Median.
Twooutof17patientswithMDShadrefractoryanemiawith
excessblasts(RAEB),onehadrefractoryanemia(RA),fourhad
refractoryanemia withringedsideroblasts (RARS),twohad
isolateddel(5q)andsixhadrefractorycytopeniawith
multi-lineagedysplasia(RCMD).TwoMDSpatientsweretreatedwith
hypomethylatingmorethansixmonthspriortothefunctional
evaluation. In addition, two patients were on the
thalido-mideprotocol23 and twohadreceivedthis drugmorethan
sixmonthspriortothefunctionalassessment.Twopatients
withchronicmyelomonocyticleukemiawereincludedinthe
MDSgroup.
SixoutoftenpatientswithAMLhadreceived
chemother-apy,onaverage, 86daysbeforethe evaluationand were in
hematological remission at the moment of the functional
assessment.ThereweresevenAMLnototherwisespecified,
twowithmyelodysplasia-relatedchangesandonewith
recur-rentgeneticabnormalities[t(8;21)].
TheHbconcentration, the incidenceofanemiaand the
transfusionstatusweredifferentacrosstheMNtypes(Table2).
Inviewofthisevidence,patientsweredividedinto:GroupI(PV,
ETandCML),II(MF)andIII(MDSandAML).
TheHb concentration washigher inpatientswith good
PS(KPS/ECOG)thaninpatientswithpoorPS(p-value<0.01).
Likewise, the Hb concentrationwas higher inindependent
patients(ADL/IADL)thaninthosewithdependenceindaily
tasks(p-value<0.01).Patientswithsomedependenceindaily
activities were older than those with no dependence in
ADL/IADL(p-value<0.01).Therewasnosignificantdifference
inagebetweenpatientswithgoodandpoorPS.Womenhad
higherADL/IADLdependencescoresthanmen(p-value<0.01).
Eightypercent(n=65)ofthepatientshadgoodPS,however
50%ofthesepatients(n=33)hadsomedependenceindaily
activities.SeventeenpatientshadpoorPSandallofthemwere
dependentforsomedailyactivities(Table3).
TherewerepatientswithgoodPSandindependent;others
withgoodPSanddependentand,finally,therewerepatients
withpoorPS,allofwhohadsomedependencefordailytasks
(Table4).
Table 4 shows that whencompared to Groups Iand II,
Group III(MDSand AML) had ahighernumber ofpatients
withpoorPSandlowernumberofpatientswithgoodPSbut
dependent.
Table2–GroupingofpatientsbasedonmeanHbconcentrationandtransfusiondemand.
GroupI GroupII GroupIII p-value
PV(n=15) ET(n=6) CML(n=9) MF(n=25) MDS(n=17) AML(n=10)
Hb(g/dL) 14.8a
(12.1–16.8; 1.51)
13.55a (11.8–15.1; 1.31)
12.13 (11.0–13.2; 0.78)
11.33a (3.5–15.1; 2.90)
9.99a (6.3–12.9; 1.54)
9.66a (5.9–13.0; 2.36)
<0.01a
Tx Yes 0 0 0 7 7 8 <0.001
b
No 15 6 9 18 10 2
PV:polycythemiavera;ET:essentialthrombocythemia;CML:chronicmyeloidleukemia;MF:myelofibrosis;MDS:myelodysplasticsyndromes; AML:acutemyeloidleukemia;Hb:hemoglobinconcentration;TX:redcelltransfusionduring30daysbeforefunctionalassessment.
a Identifysignificantdifferences(ANOVAwithTukey’stest).
Table3–Distributionofpatientsbyperformanceand functionalstatus.
Functionalstatus Performancestatus Total
Good Poor
Independent 32(50%) 0 32
Dependent 33(50%) 17(100%) 50
Total 65 17 82
Goodperformancestatus:KPS≥80%andECOG<2;Independent:no
dependenceforADLandIADL.
Table4–Distributionofpatientsbygroupsand functionality.
Groups(n) Goodperformance
status
Poorperformance status
Independent Dependent Dependent
I–PV+ET+ CML(30)
13 14 3
II–MF(25) 13 11 1
III–MDS+ AML(27)
6 8 13
TOTAL(82) ap=0.001
GoodperformanceStatus:KPS≥80%andECOG<2;Independent: nodependenceinADLandIADL.
PV: polycythemia vera; ET: essential thrombocythemia; CML: chronicmyeloidleukemia;MF:myelofibrosis;MDS:myelodysplastic syndrome;AML:acutemyeloidleukemia.
a Fisher’sexacttest.
Amixedlogisticregressionmodelwasappliedtoexplain
PS(byKPSandECOGscales)whichwasinfluencedbyHb
con-centration(p-value=0.019)andHCT-CI(p-value=0.07).Gender
(p-value=0.22)andage(p-value=0.77)didnotimpactonthe
PS.Thus,thefinallogisticmodelincludedonlytheHb
con-centrationandHCT-CI.Thevarianceoftherandomeffectof
groupingwas1.18.Therandomeffects(intercepts)inGroups
I,II,andIIIwere0.27,−1.15and1.06,respectively.
ThehypotheticalHb concentrationsatwhichtherewere
increasedrisksofhavingpoorPSarereportedinTable5.These
Hbconcentrationsdependedonthegroup(I,IIorIII)andonthe
HCT-CI(0,1,2or≥3).Thismodelhadanareaunderthereceiver
operatingcharacteristic(ROC)curveof0.85,withsensitivityof
76%andspecificityof75%.
Amixedlogisticregressionalsodemonstratedtheimpact
ofage(p-value=0.006),gender(p-value=0.002),comorbidities
(p-value=0.014)andHbconcentration(p-value=0.058)onthe
functionalstatus(byADLandIADL).Thevarianceofrandom
effectofgroupingwas0.09.Therandomeffects(intercepts)in
GroupsI,II,andIIIwere0.07,−0.23and0.16,respectively.
Consideringsimilar conditionsofcomorbidities, Hb and
age,femalepatientsweremorelikelytobedependentinsome
dailyactivitythanthemaleindividuals.Olderageandhigher
HCT-CIandlowerHbconcentrationincreasedthelikelihood
offunctionaldependence.Thismodelindicatedavalueof0.84
fortheareaundertheROCcurve,withsensitivityof74%and
specificityof72%,indicatinggoodpredictivepower.
Discussion
This study showed that the sensitivity of the functional
assessmentoftheseelderlypatientswithMNwasincreased
byaddingADLandIADLtotheKPS/ECOG.Thiswasproven
bythefactthat50%ofthepatientswithgoodPShadsome
dependenceindailyactivities(Table3).
Ontheotherhand,theheterogeneityofMNshowedthat
KPSandECOGhaddifferentsensitivityandspecificity
depend-ingontheclinicalcontexttheywereappliedin.Inthisstudy,
these instruments had higher sensitivityand specificity in
patients withAMLandMDS. AsillustratedbyTable4, this
grouphadalownumberofindividualswithgoodPSbutwith
dependenceinADL/IADL,andahighnumberofpatientswith
poorPSwithsomedependenceinADL/IADL.
Here,thecharacteristics relatedtoeachMNwere
repre-sentedbytheHb,transfusiondemandsandthediagnosisof
anemia.Alloftheotherdisease-relatedvariableswere
char-acterizedbythelogisticregressionmodelasrandomeffects.
Themodelfittedinthisstudyincorporatedthedifferences
betweentheMNasrandomeffects.Thesecharacteristicswere
relatedtothepathogenesisandtothetreatmentofeach
dis-ease. Thus, the analysis ofthe data ofGroups I, II and III
was significantto themixed logisticregression modelthat
detectedtheimpactofthesedifficult-to-controlvariables.
InthisgroupofpatientstheHbconcentrationandthe
HCT-CI,butnottheageorgender,impactedonthePSofelderly
patientswithMNasassessedbyKPSandECOG.Themixed
logisticregressionfittedamodelthathypothesizedanHb
con-centration that wascritical to poorPS (Table 5). Themost
importantclinicalvalueisthatthiscriticalHbconcentration
dependedontheaggressivenessoftheMNandontheHCT-CI.
ThisHbconcentrationshouldnotbeextrapolatedbut,as
farasweknow,thisisthefirstsurveythatfittedamodelwhich
Table5–Thehypotheticalhemoglobinconcentrationforpoorperformancestatusandhematopoieticcell transplantation-comorbidityindexofpatientswithmyeloidneoplasms.
Groups HCT-CI
0 1 2 ≥3
I–PV/ET/CML 9.53 10.52 11.51 12.50 Criticalhemoglobin
(g/dL)concentration forpoorperformance status
II–MF 5.61 6.61 7.60 8.59
III–MDS/AML 11.71 12.70 13.69 14.68
couldcomprisefunctionalassessmentandcomorbidityscore,
linkedbyHbconcentration.Thus,itispossibletoconclude
thatanemiaandHCT-CIimpactonthefunctionalityofelderly
withMN,mainlythosewithAMLandMDS.
AsillustratedbyTable5,GroupIIIhasthehighestcriticalHb
forpoorperformance.Thisfactiscongruenttotheevidenceof
higherKPS/ECOGsensitivityinpatientswithAML/MDSthan
inotherMN.Thus,KPSandECOGaremoreeasilyaffectedby
dropsinHbinGroupIIIcomparedtoGroupsIandII.
Thisevidencemaybejustified,inpart,bythe factthat,
usually,anemia in patients ofGroups I and II occurs over
alonger periodoftime than inthose of GroupIII. Hence,
adaptivemechanismscanbetriggeredovertimetobetter
pre-servethe functional autonomyofpatientsinGroups Iand
II.
Another important aspect to be considered is that
HCT-CI is a score specifically validated in patients with
AML/MDS.Asfarasweknow,therearefewstudiesassessing
patientswithchronicmyeloproliferativedisordersusingthis
instrument.24,25
All theseaspects show the necessityfor aprocess that
validatesthehypotheticalHbvaluesthatarecriticaltopoor
performance(Table5).Thisprocesscanbedesignedby
com-paring the results of this model applied to patients with
chronic myeloproliferative disorders using HCT-CI and the
Charlsonscale,26forexample.
Atthistime, theHb valuesshown inTable5should be
assumedlessasthe targets tobereachedinpatients with
MN and more as an alert that drops in Hb affect
func-tionality mainly of patients with AML/MDS and with high
HCT-CI.
FunctionalstatusassessedemployingADLandIADLwas
influencedbygender,age,Hbandcomorbidities.Therewas
anincreasing dependence in dailyactivities with drops in
Hbconcentration,increasesinHCT-CI,advancingageandfor
femalepatients.Thisevidencemay helphealthcare
profes-sionalsprovidesocialsupportbetteradjustedtothepatient’s
needs.
Asacross-sectionalsurvey,thisstudy wasnotdesigned
toanalyzeothermedicalprocedures.Itshouldbenotedthat
prognosticscoresforMFandMDStakeintoaccountHb
con-centrationand transfusion requirements. Thus, the model
fittedheresurelycanbebettercalibratedinalongitudinaltype
study.
Asanobservationalstudy,itwasveryhardtocontroleach
variableinparticularthosethatcomprisethelogistic
regres-sionmodel withmultivariate analysis. This study was not
designedtounderstandtheprognosticvalueofvariablesthat
wereincluded.Previousstudiespointedoutthatfunctionality
hasbeencorrelatednotonlytosurvivalbuttothequalityof
life,mainlyinelderlypatientswithMN.27
Thispaperisthepreliminaryresultofaresearchaimedat
improvingtheassessmentofelderlypatientswithMN.
Conclusions
The aggregation of ADL and IADL to the KPS and ECOG
scales improvedthe sensitivityand specificityofthe
func-tionalassessmentofelderlywithMN,mainlythosewithAML
and MDS.Age,gender,Hb andcomorbiditiesaffected
func-tionalstatus.However,onlycomorbiditiesandHbimpacted
on PS. The model fitted with KPS/ECOG identified
criti-cal Hb concentrations for poor PS which depends on the
aggressivenessoftheMNandonthe HCT-CI.Thusanemia
and HCT-CI impacted on thefunctionality ofthis groupof
patients, mainly those with AML and MDS. Patients with
AML and MDS were more sensitive in respectto KPS and
ECOG comparedtoother patients withless aggressive
dis-eases.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.ChauffailleML.Neoplasiasmieloproliferativas:revisãodos critériosdiagnósticosedosaspectosclínicos.RevBras HematolHemoter.2010;32(4):308–16.
2.PeyradeF,GastaudL,ReD,Pacquelet-CheliS,ThyssA. Treatmentdecisionsforelderlypatientswithhaematological malignancies:adilemma.LancetOncol.2012;13(8):
e344–52.
3.MalfusonJV,EtienneA,TurlureP,deRevelT,ThomasX, ContentinN,etal.Riskfactorsanddecisioncriteriafor intensivechemotherapyinolderpatientswithacutemyeloid leukemia.Haematologica.2008;93(12):1806–13.
4.KantarjianH,RavandiF,O’BrienS,CortesJ,FaderlS, Garcia-ManeroG,etal.Intensivechemotherapydoesnot benefitmostolderpatients(age70yearsorolder)withacute myeloidleukemia.Blood.2010;116(22):4422–9.
5.FerraraF.Treatmentofunfitpatientswithacutemyeloid leukemia:astillopenclinicalchallenge.ClinLymphoma MyelomaLeuk.2011;11(1):10–6.
6.EsteyEH.Treatmentofacutemyeloidleukemiaintheelderly. Haematologica.2011;96(6):795–8.
7.LowenbergB,DowningJR,BurnettA.Acutemyeloid leukemia.NEnglJMed.1999;341(14):1051–62.
8.DeschlerB,deWitteT,MertelsmannR,LubbertM.Treatment decision-makingforolderpatientswithhigh-risk
myelodysplasticsyndromeoracutemyeloidleukemia: problemsandapproaches.Haematologica.
2006;91(11):1513–22.
9.SandesAF,RibeiroJC,BarrosoRS,SilvaMR,ChauffailleML. Improvingtheoutcomesofelderlypatientswithacute myeloidleukemiainaBrazilianUniversityHospital.Clinics (SaoPaulo).2011;66(8):1335–40.
10.KarnofskyDAAWH,CraverLF,BurchenalJH.Theuseofthe nitrogenmustardsinthepalliativetreatmentofcarcinoma– withparticularreferencetoBronchogeniccarcinoma.Cancer. 1948;1(4):634–56.
11.ZubrodCG,SchneidermanM,FreiIiiE,BrindleyC,Lennard GoldG,ShniderB,etal.Appraisalofmethodsforthestudyof chemotherapyofcancerinman:comparativetherapeutic trialofnitrogenmustardandtriethylenethiophosphoramide. JChronicDis.1960;11(1):7–33.
13.BalducciL.Thegeriatriccancerpatient:equalbenefitfrom equaltreatment.CancerControl.2001;8(Suppl2):1–25,quiz 7–8.
14.ExtermannM,HurriaA.Comprehensivegeriatricassessment forolderpatientswithcancer.JClinOncol.
2007;25(14):1824–31.
15.DeschlerB,IhorstG,PlatzbeckerU,GermingU,MarzE,de FigueridoM,etal.Parametersdetectedbygeriatricand qualityoflifeassessmentin195olderpatientswith myelodysplasticsyndromesandacutemyeloidleukemiaare highlypredictiveforoutcome.Haematologica.
2013;98(February(2)):208–16.
16.KatzS,FordAB,MoskowitzRW,JacksonBA,JaffeMW.Studies ofillnessintheaged.TheindexofAdl:astandardized measureofbiologicalandpsychosocialfunction.JAmMed Assoc.1963;185(12):914–9.
17.LawtonMP,BrodyEM.Assessmentofolderpeople: self-maintainingandinstrumentalactivitiesofdailyliving. Gerontologist.1969;9(3):179–86.
18.SwerdlowSH.WHOclassificationoftumoursof haematopoieticandlymphoidtissues.WorldHealth Organization;2008.
19.SorrorML,MarisMB,StorbR,BaronF,SandmaierBM, MaloneyDG,etal.Hematopoieticcelltransplantation (HCT)-specificcomorbidityindex:anewtoolforrisk assessmentbeforeallogeneicHCT.Blood.2005;106(8):2912–9.
20.WilliamsJR.TheDeclarationofHelsinkiandpublichealth. BullWorldHealthOrgan.2008;86(8):650–2.
21.BauyoeL,LingsmaHF,SteyerbergEW,LesaffreE.Logistic
randomeffectsregressionmodels:acomparisonofstatistical
packagesforbinaryandordinaloutcomes.BMCMedRes
Methodol.2011;11:77.PubmedCentralPMCID:http://www.
biomedcentral.com/1471-2288/11/77
22.FreesEW,KimJS.Multilevelmodelprediction.Psychometrika. 2006;71(1):79–104.
23.RazaA,MeyerP,DuttD,ZoratF,LisakL,NascimbenF,etal. Thalidomideproducestransfusionindependencein long-standingrefractoryanemiasofpatientswith myelodysplasticsyndromes.Blood.2001;98(4):958–65.
24.PavluJ,KewAK,Taylor-RobertsB,AunerHW,MarinD, OlavarriaE,etal.Optimizingpatientselectionfor
myeloablativeallogeneichematopoieticcelltransplantation inchronicmyeloidleukemiainchronicphase.Blood. 2010;115(20):4018–20.
25.LekovicD,GoticM,Perunicic-JovanovicM,VidovicA, BogdanovicA,JankovicG,etal.Contributionofcomorbidities andgradeofbonemarrowfibrosistotheprognosisofsurvival inpatientswithprimarymyelofibrosis.MedOncol.
2014;31(3):869.
26.CharlsonME,PompeiP,AlesKL,MacKenzieCR.Anewmethod ofclassifyingprognosticcomorbidityinlongitudinalstudies: developmentandvalidation.JChronicDis.1987;40(5):373–83.