w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Investigating
alpha-globin
structural
variants:
a
retrospective
review
of
135,000
Brazilian
individuals
Elza
Miyuki
Kimura
a,b,
Denise
Madureira
Oliveira
a,b,
Susan
Elisabeth
Jorge
a,b,
Daniela
Maria
Ribeiro
a,b,
Tânia
Regina
Zaccariotto
a,b,
Magnun
Nueldo
Nunes
Santos
a,b,
Vanessa
Almeida
a,b,
Dulcinéia
Martins
Albuquerque
b,c,
Fernando
Ferreira
Costa
b,c,
Maria
de
Fátima
Sonati
a,b,∗aDepartmentofClinicalPathology,SchoolofMedicalSciences,UniversityofCampinas(UNICAMP),Campinas,SP,Brazil
bNationalInstituteofBloodScienceandTechnology,NationalCouncilforScientificandTechnologicalDevelopment(CNPq),Ministryof
ScienceandTechnology(MCT),Brazil
cHematologyandHemotherapyCenter,UniversityofCampinas(UNICAMP),Campinas,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30July2014 Accepted30September2014 Availableonline31January2015
Keywords:
Hemoglobinopathies Alpha-globinvariants Alpha-globingenes Alpha-thalassemia Multiethnicpopulations
a
b
s
t
r
a
c
t
Background:Brazil has a multiethnic population with a high diversity of hemoglobinopathies. While screenings for beta-globin mutations are far more com-mon,alterationsaffectingalpha-globingenesareusuallymoresilentandlesswellknown. Theaimofthisstudywastodescribetheresultsofascreeningprogramforalpha-globin genemutationsinarepresentativesampleoftheSoutheasternBrazilianpopulation.
Methods:A total of 135,000 individuals, including patients with clinical suspicion of hemoglobinopathiesandtheirfamilymembers,randomlychosenindividualssubmitted tobloodtestsandblooddonorswhowereabnormalhemoglobincarrierswereanalyzed. Thevariantswerescreenedbyalkalineandacidelectrophoreses,isoelectricfocusingand cation-exchangehighperformanceliquidchromatography(HPLC)andtheabnormalchains wereinvestigatedbyreverse-phasehighperformanceliquidchromatography(RP-HPLC). Mutationswereidentifiedbymolecularanalyses,andtheoxygenaffinity,heme–heme coop-erativityandBohreffectofthevariantswereevaluatedbyfunctionaltests.
Results:Fournewand22rarevariantsweredetectedin98families.Someofthese vari-antswerefoundinco-inheritancewithotherhemoglobinopathies.Oftherarehemoglobins, Hasharon,StanleyvilleIIandJ-Rovigowerethemostcommon,thefirsttwobeingS-likeand associatedwithalpha-thalassemia.
∗ Correspondingauthorat:DepartmentofClinicalPathology,SchoolofMedicalSciences,UniversidadeEstadualdeCampinas(UNICAMP),
Campinas,SP,Brazil.
E-mailaddress:[email protected](M.d.F.Sonati).
http://dx.doi.org/10.1016/j.bjhh.2015.01.005
Conclusion: The variabilityofalpha-globinalterationsreflects thehighdegree ofracial miscegenationandanintenseinternalmigratoryflowbetweendifferentBrazilianregions. Thisdiversityhighlightstheimportanceofprogramsfordiagnosinghemoglobinopathies and preventing combinations that may lead to important clinical manifestations in multiethnicpopulations.
©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
Introduction
Alpha-globinchainvariantsaretheresultofpointmutations (singlenucleotidepolymorphisms–SNPs)orsmallbase inser-tionsordeletionsthataffecttheregionencodingthe␣1and␣2
genes,thusresultinginaminoacidsubstitutionsintheprotein chainsorevenelongatedchains.1
Morethan400structuralchangesinthealpha-chainhave beendescribedtodate2,mostofwhicharecausedbysimple
DNAbasesubstitutionswiththecorrespondingsubstitutions ofaminoacid residuesinthe protein.Manyofthese alter-ations do not result in clinical symptoms; however, some can affect the function of the hemoglobin (Hb) molecule, resultinginerythrocytosisorcyanosis,anditsstability, caus-ing hemolytic anemia.3 In addition, there are elongated
and extremely unstable variants that lead to thalassemia phenotypes.4
TheHemoglobinopathyLaboratoryoftheHospitaldas Clin-icas, Universidade Estadual de Campinas (UNICAMP), São Paulo,SoutheasternBrazilisareferrallaboratoryforthe diag-nosis of hemoglobinopathies. This paper summarizes the alpha-chain structural variants identified inthe laboratory duringits30yearsofexistence.
Methods
Todate,135,000caseshavebeeninvestigatedinthis labora-tory.Thispopulationsampleincludespatientswithclinical suspicionofhemoglobinopathiesandtheirfamilymembers, randomlychosenindividualswhohadbloodtestsandblood donorswhowerecarriersofhemoglobinvariants.Thelocal ethics committee approvedthis study and the subjects or theirlegalguardiansgaveinformedconsentforparticipation. Structuralchangesinthealpha-chainwereidentifiedin124 individualsfrom98differentfamilies(approximately0.1%of theanalyzedcases).
Peripheral blood samples were collected in tubes con-tainingEDTA,andhematological analyseswere carriedout usinganautomatedcounter(SysmexXE2100,Sysmex,Kobe, Japan).Hbvariantswereidentifiedandcharacterizedby elec-trophoresis on cellulose acetateat pH 8.9 and agar gel at pH6.0,isoelectricfocusing (RESOLVENeonatal Hemoglobin Test Kit, PerkinElmer Wallace,Akron, OH, USA)and cation exchange high performanceliquid chromatography (HPLC) (VARIANTII,Bio-RadLaboratories,Hercules,CA,USA). Abnor-mal globin chains were identified by reverse phase HPLC (RP-HPLC)(WatersAllianceHPLCSystem,Waters,Milford,MA,
USA).Stabilitytests(heatstabilityandstabilityinn-butanol andinisopropanol)andsolubilitytestswerealsocarriedout, aswellasaninvestigationofHeinzbodiesandHbHinclusion bodiesinredcells.5
Functional studies were carried out by plotting the oxygen–hemoglobin dissociation curve at different pHs to measure the Bohreffect and evaluateheme–heme cooper-ativity ofthe globinchainsinthepresenceandabsenceof allostericeffectors.1,5–7
Genomic DNA samples were extracted from peripheral blood leukocytes, initially by organic methods8 and, more
recently using a specific kit (Blood Genomic Prep Mini Spin, GE Healthcare, UK). Alpha-globin genes were selec-tivelyamplifiedbypolymerasechainreaction(PCR)according to the method described by Dodé et al.9 and sequenced
using an automated technique (ABI PRISM 377 DNA Auto-mated Sequencer, Applied BioSystems, Foster City, CA, USA). Mutations were confirmed by sequencing the oppo-site DNA strand, family analysis and enzyme restriction analysis, whenever possible. The presence of concomitant deletionalalpha-thalassemia wasinvestigatedbymultiplex PCR and gap PCR.10,11 The most common non-deletional
alpha-thalassemic mutations were also investigated when theseweresuspected.12,13
Results
Fournewalpha-chainvariants(Table1)and22rarevariants
(Table2)weredetected,fiveofthelatterconcomitantlywith
otherstructuralorthalassemicmutations.
Newvariants
The four new variants were identified in 13 individuals belonging to sixdifferent families (Table1). None resulted insignificanthematologicalorclinicalabnormalitiesintheir carriers.
Hb Campinas [HBA2:c.80C>T p.Ala26Val] was first described in a nine-year-old boy and his mother and later was observed in three related individuals during a hemoglobinopathyscreeningprogram.14
Table1–Newalpha-globinvariantsidentified.
Newvariant No.of
families/No.of cases
Mutation ␣-genotype Clinical manifesta-tions/hematological alterations
HbBoaEsperanc¸a 2/2 HBA2:c.50A>Cp.Lys16Thr ␣BoaEsperanc¸a␣/␣␣ No HbCampinas 2/5 HBA2:c.80C>Tp.Ala26Val ␣Campinas␣/␣␣ No HbBomJesusdaLapa 1/3 HBA1:c.92A>Cp.Glu30Ala ␣␣BJesusdaLapa/␣␣ No HbItapira 1/3 HBA3:c.92A>Tp.Glu30Val ␣␣␣Itapira/␣␣ No
Total 6/13
Twonewmutationsresultinginsubstitutionsofthesame aminoacidresidue(glutamic acidatposition30)by chem-icallysimilarresidueswerealsoidentified:HbBomJesusda Lapa[HBA1:c.92A>Cp.Glu30Ala]andHbItapira[HBA1:c.92A>T p.Glu30Val].Inboth,apolaraminoacidresiduewasreplaced by a nonpolar one, but no clinical manifestations were observedinthecarriers.HbBomJesusdaLapawasdetectedin threerelatedheterozygousindividualsofindigenousdescent. HbItapira,forwhichthemutationwasfoundinatriplicate alphaallele(␣␣␣anti-3.7)andwhichaccountedforonly5.5%of totalHbproduction,wasfoundinthreerelatedindividuals.15
Rarevariants
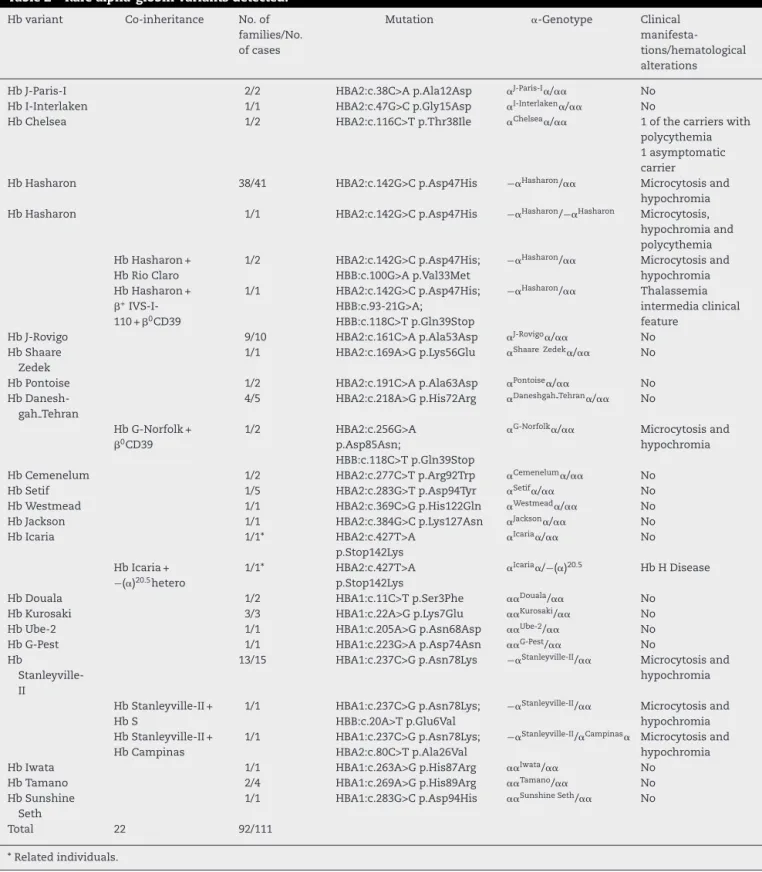
Twenty-tworare alpha-chain variantswere detectedin111 individuals from 92 different families. Of these, the most prevalentwasHbHasharon(41families,45cases)(Table2), correspondingto44.6%ofthefamilieswithrarealpha-chain structuralvariants. Thesecond mostprevalentvariantwas HbStanleyvilleII(15families,17cases–Table2), correspond-ing to 16.3% ofthe carrier families. In thirdplace was Hb J-Rovigo,withnineaffectedfamilies(10cases)(Table2)and correspondingto9.8%ofthecarrierfamilieswithrare alpha-globinvariants.HbHasharonandHbStanleyvilleIIresulted inslightlyalteredhematologicalfindings(hypochromiaand microcytosis),whichmaybeexplainedbythefactthatthey wereinassociationwiththe−␣3.7deletion.
HbHasharonwasfoundinheterozygosis(38families,41 individuals),inhomozygosis(1case)andinassociationwith othermutationsofglobingenes.Inonefamily,two individ-ualshadbothHbHasharonandHbRioClaro[HBA2:c.142G>C p.Asp47His;HBB:c.100G>Ap.Val33Met], abeta-chainvariant newly described in this laboratory.16 Both individuals had
microcytosisand hypochromia(Table2). Inanother family, HbHasharonwasdetectedwithone+ (IVS-I-110)and one 0(CD39)alleleinthesameindividual,whopresentedwitha typicalclinicalcourseofthalassemiaintermedia(Table2).17
Like Hb Hasharon, Hb Stanleyville II was found con-comitantlywith other structural variantsin two unrelated individuals(Table2).Inthe first,it waspresentwith HbS, themostcommonstructuralvariantinthe Brazilian popu-lation. Inthe second case, therewas a combination ofHb StanleyvilleIIandHbCampinas[HBA1:c.237C>Gp.Asn78Lys; HBA2:c.80C>Tp.Ala26Val]andtheindividualalsohad micro-cytosisand hypochromia(Table 2).18 Inboth cases,thered
bloodcellsofthecarriersshowedmicrocytosisand hypochro-miaasthe HbStanleyvilleIImutationwasassociatedwith alpha-thalassemia(−␣3.7deletion).
HbG-Norfolkwasidentifiedincombinationwith0(CD39) thalassemia [HBA2:c.256G>A p.Asp85Asn; HBB:c.118C>T p.Gln39Stop]intworelatedindividualsresultingin microcy-tosisandhypochromia(Table2).
HbChelsea[HBA2:c.116C>Tp.Thr38Ile]wasfoundintwo related individuals, one with erythrocytosis and the other withoutanyabnormalhematologicalfindings(Table2).
Conversely, Hb Icaria [HBA2:c.427T>A p.Stop142Lys] was identified in combination with a common ␣0 thalassemia determinant,the(␣)20.5allele.HbIcaria(X142K)isanelongated
chainwith31extraresiduesandachangeintheC-terminal region of the protein [(142)Lys-Ala-Gly-Ala-Ser-Val-Ala-Val- Pro-Pro-Ala-Arg-Trp-Ala-Ser-Gln-Arg-Ala-Leu-Leu-Pro-Ser-Leu-His-Arg-Pro-Phe-Leu-Val-Phe-(172)Glu-COOH]. In this case,theelongatedandunstablealpha-chaininassociation withthe−(␣)20.5deletion,resultedinHbHdiseasewithhigh levelsofHb HandHbBart’s(14.7%and19.0%,respectively)
(Table2).4
Theotherrarealpha-globinvariants(Table2)werefoundin blooddonorsandasymptomaticindividualsparticipatingina hemoglobinopathyscreeningprogram,whichalsoidentified mostofthecasesofHbHasharon,HbStanleyvilleandHb J-Rovigo.
Discussion
Hbvariantsandthalassemiashaveadiversegeographic dis-tributioninBrazilastheyareverycloselyrelatedtotheethnic origins ofthe populationandthe colonizationprocess that tookplacebetweenthe16thand19thcenturies.Thelargest ethnicalinfluenceduringthecolonizationofBrazilwasdueto PortugueseandAfricanimmigrants.
BrazilhasthelargestBlackpopulationinSouthAmerica, primarily asa resultofthe African slave tradewhich was responsible for some3.6million black people entering the country from the16thcenturyonwards,particularly tothe NortheastandSoutheast.Inthe19thcentury,other popula-tionsbegantoarrive,mostnotablyItalianimmigrants,who cameinlargenumberstosettleintheSouthandSoutheast. This miscegenation was also influenced by various migra-tionsfromotherEuropean(Spain,Germany,Holland,Russia andPoland),Asian(China,JapanandKorea)andMiddle East-erncountries, all ofwhichcontributed tothe formationof theBrazilianpopulation.Inaddition,internalmigratoryflows betweenthe populationsofdifferentBrazilianstatesledto miscegenationbetweenallthesepopulationgroups.19
Table2–Rarealpha-globinvariantsdetected.
Hbvariant Co-inheritance No.of families/No. ofcases
Mutation ␣-Genotype Clinical manifesta-tions/hematological alterations
HbJ-Paris-I 2/2 HBA2:c.38C>Ap.Ala12Asp ␣J-Paris-I␣/␣␣ No HbI-Interlaken 1/1 HBA2:c.47G>Cp.Gly15Asp ␣I-Interlaken␣/␣␣ No
HbChelsea 1/2 HBA2:c.116C>Tp.Thr38Ile ␣Chelsea␣/␣␣ 1ofthecarrierswith
polycythemia 1asymptomatic carrier
HbHasharon 38/41 HBA2:c.142G>Cp.Asp47His −␣Hasharon/␣␣ Microcytosisand hypochromia HbHasharon 1/1 HBA2:c.142G>Cp.Asp47His −␣Hasharon/−␣Hasharon Microcytosis,
hypochromiaand polycythemia HbHasharon+
HbRioClaro
1/2 HBA2:c.142G>Cp.Asp47His; HBB:c.100G>Ap.Val33Met
−␣Hasharon/␣␣ Microcytosisand hypochromia HbHasharon+
+ IVS-I-110+0CD39
1/1 HBA2:c.142G>Cp.Asp47His; HBB:c.93-21G>A;
HBB:c.118C>Tp.Gln39Stop
−␣Hasharon/␣␣ Thalassemia
intermediaclinical feature
HbJ-Rovigo 9/10 HBA2:c.161C>Ap.Ala53Asp ␣J-Rovigo␣/␣␣ No HbShaare
Zedek
1/1 HBA2:c.169A>Gp.Lys56Glu ␣Shaare Zedek␣/␣␣ No
HbPontoise 1/2 HBA2:c.191C>Ap.Ala63Asp ␣Pontoise␣/␣␣ No
Hb Danesh-gahTehran
4/5 HBA2:c.218A>Gp.His72Arg ␣DaneshgahTehran␣/␣␣ No
HbG-Norfolk+ 0CD39
1/2 HBA2:c.256G>A p.Asp85Asn;
HBB:c.118C>Tp.Gln39Stop
␣G-Norfolk␣/␣␣ Microcytosisand
hypochromia
HbCemenelum 1/2 HBA2:c.277C>Tp.Arg92Trp ␣Cemenelum␣/␣␣ No
HbSetif 1/5 HBA2:c.283G>Tp.Asp94Tyr ␣Setif␣/␣␣ No
HbWestmead 1/1 HBA2:c.369C>Gp.His122Gln ␣Westmead␣/␣␣ No HbJackson 1/1 HBA2:c.384G>Cp.Lys127Asn ␣Jackson␣/␣␣ No
HbIcaria 1/1* HBA2:c.427T>A
p.Stop142Lys
␣Icaria␣/␣␣ No
HbIcaria+
−(␣)20.5hetero
1/1* HBA2:c.427T>A p.Stop142Lys
␣Icaria␣/−(␣)20.5 HbHDisease
HbDouala 1/2 HBA1:c.11C>Tp.Ser3Phe ␣␣Douala/␣␣ No
HbKurosaki 3/3 HBA1:c.22A>Gp.Lys7Glu ␣␣Kurosaki/␣␣ No
HbUbe-2 1/1 HBA1:c.205A>Gp.Asn68Asp ␣␣Ube-2/␣␣ No
HbG-Pest 1/1 HBA1:c.223G>Ap.Asp74Asn ␣␣G-Pest/␣␣ No Hb
Stanleyville-II
13/15 HBA1:c.237C>Gp.Asn78Lys −␣Stanleyville-II/␣␣ Microcytosisand hypochromia
HbStanleyville-II+ HbS
1/1 HBA1:c.237C>Gp.Asn78Lys; HBB:c.20A>Tp.Glu6Val
−␣Stanleyville-II/␣␣ Microcytosisand
hypochromia HbStanleyville-II+
HbCampinas
1/1 HBA1:c.237C>Gp.Asn78Lys; HBA2:c.80C>Tp.Ala26Val
−␣Stanleyville-II/␣Campinas␣ Microcytosisand hypochromia
HbIwata 1/1 HBA1:c.263A>Gp.His87Arg ␣␣Iwata/␣␣ No
HbTamano 2/4 HBA1:c.269A>Gp.His89Arg ␣␣Tamano/␣␣ No HbSunshine
Seth
1/1 HBA1:c.283G>Cp.Asp94His ␣␣SunshineSeth/␣␣ No
Total 22 92/111
*Relatedindividuals.
ineach regionofthe country.19,20 Hence, anyinvestigation
into the prevalence of hemoglobinopathies in Brazil must take into account the historical processes involved in the ethnic make-upofthe population.To date,no evidenceof theexistenceofhemoglobinopathiesinpre-Columbian Amer-ica has been found, suggesting that these were brought to the Americas and to Brazil by the various migratory flows.20,21
indexinBrazilaccordingtoUnitedNationsDevelopment Pro-gram (UNDP) data.22 The population in this part of Brazil
is very mixed, mainly made up of individuals of Italian, Portuguese,Amerindian, African, Arabic, German, Spanish, JapaneseandChinesedescent.
This miscegenation is reflected in the great variety of unusualhemoglobinsidentifiedinthecasesreferredtoour laboratory: Hb Stanleyville II, Hb Douala and Hb Chelsea are from the African continent2,23,24; Hb Jackson is found
inBlackAmericans fromSouthwesternUnitedStates25; Hb
Westmead,HbKurosaki,HbUbe-2,HbIwataandHbTamano are of Asian origin2,26–29; Hb Hasharon, Hb Shaare Zedek,
Hb Daneshgah-Tehran and Hb Setif are from the Middle East2,30–32;HbJ-Paris,HbI-Interlaken,HbJ-Rovigo,HbPontoise,
HbCemenelum,HbG-NorfolkandHbSunshineSetharefound inEuropeanpopulations33–39; and Hb Icariaand Hb G-Pest
arefromEasternEurope.40,41 Inthisrespect,different
alpha-globinvariantshave beenfoundinother Brazilianregions, suchasinthestateofMinasGerais,whereHbEtobicoke,Hb OttawaandHbSt.Luke’sweredetectedforthefirsttimein Brazil.42
Thus,despitetheindividualsanalyzedherebelongingto ahospitalsampleandnotreflectingthegeneralpopulation, thevarietyofhemoglobinsidentifiedistheresultofthe con-tributions made bythe different population groups to the ethnicmake-upoftheBrazilianpopulationandhighlightsthe importanceofprogramsfordiagnosinghemoglobinopathies inBrazil,particularlybecauseofthelargenumberof immi-grantsfromcountrieswithhighriskforhemoglobinopathies. Thecombination ofalpha-chain variantswith other struc-turalorthalassemicmutationscanresultinclinicallyrelevant phenotypes, highlighting the importance of characterizing hemoglobins.
Conclusion
The findings presented here corroborate the high degree of diversity among Hb variants in the Brazilian popula-tion, in which miscegenation has increased the likelihood of rare hemoglobinopathies. Identification of Hb variants cantherefore makeasignificant contribution to anthropo-logical studies of the different groups that make up the Brazilianpopulationandtoanassessmentoftheincidence of Hb variants, which, in combination with other com-mon hemoglobinopathies, such as Hb S, Hb C and alpha-andbeta-thalassemia,representapublichealthproblemin Brazil. This information could be used by individuals and theirfamiliesingeneticcounseling.Inaddition,identification andcharacterizationofnewhemoglobinstructuralvariants will contribute to a better understanding on the relation betweenstructureandfunctionofthisandotherimportant proteins.
Funding
This work was supported by the Fundac¸ão de Amparo à Pesquisa do Estado de São Paulo (FAPESP) (grant nos. 2008/57441-0and2010/00560-8andfellowships2009/18248-3
and 2010/00154-0), the Conselho Nacional de Desenvolvi-mentoCientíficoeTecnológico(CNPq)(grantno. 477407/2010-2), the Instituto Nacional de Ciência e Tecnologia do Sangue(INCTs)(grantno.573780/2008-0)andCoordenac¸ãode Aperfeic¸oamentodePessoaldeNivelSuperior(CAPES).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BunnHF,ForgetBG.Hemoglobin:molecular,geneticand
clinicalaspects.Philadelphia,London,Toronto:W.B.Saunders
Company;1986.p.690.
2.GlobinGeneServer.Availablefrom:
http://globin.bx.psu.edu/hbvar/menu.html[cited30.04.14].
3.SteinbergMH,ForgetBG,HiggsDR,NagelRL.Disordersof
hemoglobin.NewYork:CambridgeUniversityPress;2001.p.
1268.
4.KimuraEM,OliveiraDM,FertrinK,PinheiroVR,JorgeSE,
CostaFF,etal.HbHdiseaseresultingfromtheassociationof
an␣-thalassemiaallele[−(␣)]withanunstable␣-globin
variant[HbIcaria]:firstreportontheoccurrenceinBrazil.
GenetMolBiol.2009;32(4):712–5.
5.DacieJV,LewisSM.Practicalhematology.8thed.NewYork:
ChurchillLivingstone;1995.p.609.
6.AntoniniE,BrunoniM.Hemoglobinandmyoglobinintheir
reactionwithligands.Amsterdam:North-HollandPublishing
Company;1971.p.435.
7.Rossi-FanelliA,AntoniniE.Studiesontheoxygenandcarbon
monoxideequilibriaofhumanhemoglobin.ArchBiochem
Biophys.1958;77(2):478–92.
8.DavisL,DibnerMD,BatteyJF.Basismethodsinmolecular
biology.NewYork:ElsevierSciencePublishingCo.Inc.;1986.
p.399.
9.DodéC,RochetteJ,KrishnamoorthyR.Locusassignmentof
humanalpha-mutationbyselectiveamplificationanddirect
sequencing.BrJHaematol.1990;76(2):275–81.
10.ChongSS,BoehmCD,HiggsDR,CuttingGR.Singletube
multiplex-PCRscreenforcommondeletionaldeterminantsof
alpha-thalassemia.Blood.2000;95(1):360–2.
11.KattamisAC,CamaschellaC,SiveraP,SurreyS,FortinaP.
Humanalpha-thalassemiasyndromes:detectionof
moleculardefects.AmJHematol.1996;53(2):81–91.
12.HallGW,TheinSL,NewlandAC,ChisholmM,
Traeger-SynodinosJ,KanavakisE,etal.Abasesubstitution
(T–>C)incodon29ofthealpha2-globingenecausesalpha
thalassaemia.BrJHaematol.1993;85(3):546–52.
13.BowdenDK,VickersMA,HiggsDR.APCR-basedstrategyto
detectthecommonseveredeterminantsofalpha
thalassaemia.BrJHaematol.1992;81(1):104–8.
14.WenningMR,SilvaNM,JorgeSB,KimuraEM,CostaFF,
Torsoni,etal.HbCampinas[alpha26(B7)Ala–>Val]:anovel,
electrophoreticallysilent,variant.Hemoglobin.
2000;24(2):143–8.
15.JorgeSE,KimuraEM,OliveiraDM,OgoS,AlbuquerqueDM,
CostaFF,etal.Threenewalpha-globinvariants:HbItapira
[alpha30(B11)Glu–>Val(alpha1)],HbBomJesusDaLapa
[alpha30(B11)Glu–>Ala(alpha1)]andHbBoaEsperanc¸a
[alpha16(A14)Lys–>Thr(alpha2)].Hemoglobin.
2007;31(2):151–7.
16.GrignoliCR,WenningMR,SonatiMF,KimuraEM,ArrudaVR,
electrophoreticallysilentvariantfoundinassociationwith
HbHasharon[alpha47(CE5)Asp–>His]and
alpha-thalassemia-2(−alpha3.7).Hemoglobin.1999;23(2):177–82.
17.CostaFF,FigueredoMS,SonatiMF,KimuraEM,MartinsCS.
TheIVS-I-110(G–>T)andcodon39(C–>T)beta-thalassemia
mutationsinassociationwithalpha-thal-2(−3.7Kb)andHb
Hasharon[alpha47(CE5)Asp–>His]inaBrazilianpatient.
Hemoglobin.1992;16(6):525–8.
18.WenningMR,KimuraEM,CostaFF,SaadST,GervásioS,de
JorgeSB,etal.Alpha-globingenes:thalassemicandstructural
alterationsinaBrazilianpopulations.BrazJMedBiolRes.
2000;33(9):1041–5.
19.ZagoMA,CostaFF.Hereditaryhaemoglobindisordersin
Brazil.TransRSocTropMedHyg.1985;79(3):85–8.
20.SalzanoFM,BortoliniMC.TheevolutionandgeneticsofLatin
Americanpopulation.Cambridge:CambridgeUniversity
Press;2002.p.511.
21.VarelaV,AbreuS,RossettiLC,TargovnikH.Mostfrequent
beta-thalassemiamutationsintheArgentinianpopulation.
Sangre.1996;41(2):137–40.
22.ProgramadasNac¸õesUnidasparaoDesenvolvimento. Availablefrom:http://www.pnud.org.br[cited26.04.14].
23.VanRosG,BealeD,LehmannH.HaemoglobinStanleyvilleII
(alphaasparaginereplacedbylysine).BrMedJ.
1968;4(5623):92–3.
24.PréhuC,HanichiA,YapoAP,ClaparolsC,ProméD,RiouJ,
etal.HbDouala[alpha3(A1)Ser–>Phe]:anewalpha1gene
mutationinaCameroonianwomanheterozygousforHbS
anda3.7kbdeletionalalpha-thalassemia.Hemoglobin.
2001;25(3):323–9.
25.Moo-PennWF,BechtelKC,JohnsonMH,JueDL,HollandS,
HuffC,etal.HemoglobinJackson,alpha127(H10)Lys
replacedbyAsn.AmJClinPathol.1976;66(2):453–6.
26.FlemingPJ,HughesWG,FarmiloRK,WyattK,CooperWN.
HemoglobinWestmeadalpha2122(H5)HisreplacedbyGln
beta2:anewhemoglobinvariantwiththesubstitutioninthe
alpha1beta1contactarea.Hemoglobin.1980;4(1):39–52.
27.HaranoT,HaranoK,ImaiK,MurakamiT,MatsubaraH.Hb
Kurosaki[alpha7(A5)Lys–>Glu]:anewalphachainvariant
foundinaJapanesewoman.Hemoglobin.
1995;19(3–4):197–201.
28.MiyajiT,IuchiI,YamamotoK,OhbaY,ShibataS.Aminoacid
substitutionofhemoglobinUbe2(alpha-268aspbeta-2):an
exampleofsuccessfulapplicationofpartialhydrolysisof
peptidewith5percentaceticacid.ClinChimActa.
1967;16(3):347–52.
29.OhbaY,MiyajiT,HattoriY,FuyunoK,MatsuokaM.Unstable
hemoglobinsinJapan.Hemoglobin.1980;4(3–4):
307–12.
30.AbramovA,LehmannH,RobbL.HbShaareZedek(alpha56
E5LysleadstoGlu).FEBSLett.1980;113(2):235–7.
31.RahbarS,NowazariG,DanéshmandP.Haemoglobin
Daneshgah-Tehranalpha272(EPI)histidine–argininebetaA2.
NatNewBiol.1973;245(148):268–9.
32.WajcmanH,BelkhodjaO,LabieD.HbSetif:G1(94)Asp-Tyr.A
newchainhemoglobinvariantwithsubstitutionofthe
residueinvolvedinhydrogenbondbetweenunlikesubunits.
FEBSLett.1972;27(2):298–300.
33.TrincaoC,DeMeloJM,LorkinPA,LehmannH.HaemoglobinJ
ParisinthesouthofPortugal(Algarve).ActaHaematol.
1968;39(5):291–8.
34.MartiHR,PikC,MosimannP.AnewhemoglobinIvariant:
HbI-Interlaken.ActaHaematol.1964;32:9–16.
35.AlbertiR,MariuzziGM,ArtibaniL,BruniE,TentoriL.Anew
haemoglobinvariant:J-Rovigoalpha53(E-2)alanineleadsto
asparticacid.BiochimBiophysActa.1974;342(1):1–4.
36.ThilletJ,BlouquitY,PerroneF,RosaJ.Hemoglobinpontoise
alpha63AlareplacedbyAsp(E12).Anewfastmovingvariant.
BiochimBiophysActa.1977;491(1):16–22.
37.WajcmanH,KisterJ,M’RadA,SoummerAM,GalacterosF.Hb
Cemenelum[alpha92(FG4)Arg–>Trp]:ahemoglobinvariant
ofthealpha1/beta2interfacethatdisplaysamoderate
increaseinoxygenaffinity.AnnHematol.1994;68(2):
73–6.
38.HuntsmanRG,HallM,LehmannH,SukumaranPK.Asecond
andathirdabnormalhaemoglobininNorfolk.Haemoglobin
GNorfolkandhaemoglobinDNorfolk.BrMedJ.
1963;1(5332):720–2.
39.SchroederWA,SheltonJB,SheltonJR,PowarsD.Hemoglobin
SunshineSeth–alpha2(94(G1)AspreplacedbyHis)beta2.
Hemoglobin.1979;3(2–3):145–59.
40.CleggJB,WeatherallDJ,Contopolou-GrivaI,CaroutsosK,
PoungourasP,TsevrenisH.HaemoglobinIcaria,anew
chain-terminationmutantwithcausesalphathalassaemia.
Nature.1974;251(5472):245–7.
41.HollánSR,SzelenyiJG,BrimhallG,DuerstM,JonesRT,Koler
RD,etal.Multiplealphachainlociforhumanhaemoglobins:
HbJ-BudaandHbG-Pest.Nature.1972;235(5332):47–50.
42.SilvaMR,SendinSM,AraujoIC,PimentelFS,VianaMB.Alpha
chainhemoglobinswithelectrophoreticmobilitysimilarto
thatofhemoglobinSinanewbornscreeningprogram.Rev