w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Pilot
randomized
controlled
trial
to
evaluate
the
effect
of
aquatic
and
land
physical
therapy
on
musculoskeletal
dysfunction
of
sickle
cell
disease
patients
Camila
Tatiana
Zanoni,
Fábio
Galvão,
Alberto
Cliquet
Junior,
Sara
Teresinha
Olalla
Saad
∗UniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received11June2014 Accepted25July2014
Availableonline21November2014
Keywords: Anemia,sicklecell Hydrotherapy
Physicaltherapymodalities
a
b
s
t
r
a
c
t
Objective:Tocomparetheeffectofaquaticandland-basedphysiotherapyinreducing mus-culoskeletalhipandlowerbackpainandincreasingoverallphysicalcapabilitiesofsickle celldiseasepatients.
Methods:Informedwrittenconsentwasobtainedfromallvolunteerswhoweresubmittedto evaluationsusingdifferentfunctionalscales:Lequesne’sAlgofunctionalQuestionnaireand OswestryDisabilityIndex,trunkandhiprangeofmotion,goniometry,trunkandhipmuscle strengthassessmentusingloadcell,andsurfaceelectromyographyoftheiliocostalis,long dorsal(longissimus),gluteusmaximus,gluteusmediusandtensorfasciaelataemuscles. Tenpatientswererandomizedintotwogroups:aquaticphysiotherapywithameanageof 42years(range:25–67)andconventionalphysiotherapywithameanageof49years(range: 43–59).Bothgroupsweresubmittedtoatwelve-weekprogramoftwosessionsweekly. Results:After the intervention, significant improvements were observed regarding the Lequesne index (p-value=0.0217), Oswestry Disability Index (p-value=0.0112), range of motionoftrunkextension(p-value=0.0320),trunkflexionmusclestrength(p-value=0.0459), hipextensionandabductionmusclestrength(p-value=0.0062andp-value=0.0257, respec-tively).Rangeofmotionoftrunkandhipflexion,extension,adductionandabduction,trunk extensormusclestrengthandallsurfaceelectromyographyvariablesshowednosignificant statisticaldifference.
Conclusion:Physicaltherapyisefficienttotreatmusculoskeletaldysfunctionsinsicklecell diseasepatients,irrespectiveofthetechnique;however,aquatictherapyshowedatrend towardimprovementinmusclestrength.Furtherstudieswithalargerpatientsampleand longerperiodsoftherapyarenecessarytoconfirmtheseresults.
©2014Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthorat:HemocentroUnicamp,InstitutoNacionaldeCiênciaeTecnologiadoSangue,RuaCarlosChagas,480,Cidade
UniversitáriaZeferinoVaz,13083-878Campinas,SP,Brazil. E-mailaddress:[email protected](S.T.O.Saad). http://dx.doi.org/10.1016/j.bjhh.2014.11.010
Introduction
Sickle cell disease (SCD) is a genetic disorder that results inthe sickling ofred blood cells,triggering vaso-occlusion episodeswhichleadtopainandorgandamage.This inher-iteddisorderiscausedbyapointmutationinthebeta-globin gene.ThemutantformofhemoglobininSCD(HbS)is capa-bleofpolymerizationandcomplexmolecularandstructural changeswithinthered cell.Occurringinhomozygotes(Hb SS) and in compound heterozygotes, such as those carry-ing Hb Sand beta-thalassemia (Hb SB+ or HbSB0)and Hb
S and hemoglobinC (Hb SC), hemolytic anemia and vaso-occlusioncrisesarethemaincomplicationsofSCD.Theillness tendstograduallydeveloptowardmultisystemorganfailure.1 Boneinvolvement,frequentlycausingpainfulvaso-occlusive crises,isthemostcommonclinicalmanifestation. Further-more,boneinvolvementisasourceofchronic, progressive disability, with long-term effects upon bone mass density, growth, and bone damage suchas avascular necrosis and osteomyelitis.Osteopeniaandosteoporosisareoften asymp-tomatic;however,pain,fractures,deformities,andvertebral collapsemayoccurandrequirechronicanalgesia,mechanical support,andsurgicalinterventions.2,3
Chronic and progressive damage such as, for example, avascular necrosisof the femoral head, the leading cause ofhipdeformityinthesepatients,commonlyresultsingait disturbances,pain,andactivityandfunctionallimitationsin adultpatients.Lowerbackpainisoneofthemaincomplaints amongSCD patients and occurs dueto the flattening and wideningofthevertebralbodieswithbiconcavedepressions oftheendplates,probablycausedbyinfarctionofthecentral portionofthevertebralbody.4,5 Therearefewstudiesinthe literatureontheroleofphysiotherapyasaresourcetoprevent andtreatlocomotorsystemdisordersinSCDindividuals.
According torecent studies, the lifeexpectancy ofSCD patients’ hasimproveddramaticallyover the lastcentury.6 Howeverthislongerlifespanhas,asanunfortunate conse-quence,thedevelopmentofprogressiveorgandamagewhich includesosteoarticularlesions.7
Chronicpainisconsideredaseriouspublichealth prob-lemwhichnegativelyaffectsthequalityoflifeofindividuals. Therefore,amulti-actiontherapeuticplan,specifically phys-iotherapy, could help decrease pain, and improve mobility andtherehabilitationofosteoarticulardisorders,positively impactingonthequalityoflife.8
Despitethisfact,therearefewstudiesintheliteratureon theroleofphysiotherapyasaresourcetopreventandtreat locomotorsystemdisordersinSCDpatients.Onestudy9 com-paredtheefficacyofphysiotherapyalonewithphysiotherapy associatedwithsurgicalfemurdecompressioninSCDpatients withosteonecrosisofthefemoralhead.Theresultsshowedno significantdifferencebetweenthesetwoapproaches, suggest-ingthatphysicaltherapyaloneappearedtobeaseffectiveas surgicaldecompressiontoimprovehipfunction,thus defer-ringtheneedforsurgery.
Withintheexistingphysiotherapyresources,aquatic phys-iotherapyused inrehabilitation hasdemonstrated positive effects againstpain, in regaining physicalfunction and in improving quality of life in adults with musculoskeletal
conditions.10 Movements performed inthe waterare facil-itated bytheelimination ofthe effectsofgravity, resulting inincreasedmusclestrength(MS)andflexibility.The bene-fitsofwateraremainlyexplainedbythephysiologicaleffects ofimmersion and bythehydrodynamic principlesof exer-cise,suchasbuoyancy,inthisenvironmenttherebyenabling functional exerciseswithareduced gravitationalload. Fur-thermore,theimmersioninthermo-neutralwater(34◦C)in
combinationwiththeeffectsofhydrostaticpressurereduces the perceptionofpain.Thephysicalpropertiesand heated water play an important role in improving and maintain-ing the range ofjoint motions, reducing muscular tension and promoting relaxation, as well as preparing the mus-cleforstretching.Thebuoyancyinducesmusclerelaxation and thedecrease inimpactenablesincreasedmobilityand flexibility.11,12
Thisstudyaimedtoevaluatethe efficacyofaquaticand land-basedphysicaltherapyindecreasinghipandlowerback musculoskeletal pain and increasing overall physical well-beinginSCDpatients.
Methods
Adult SCD patients who regularly attended (at least three timesayearduringthepreviousthreeyears)theOutpatient Clinic of the Hemocentro ofthe Universidade Estadual de Campinas(UNICAMP)withchronichipandlumbarspinepain, andwhohadnotparticipatedinaphysicaltherapyprogram duringtheprevious12months,wereinvitedtoparticipatein thisstudy.Patientswithacuteepisodes,absenceofoverthree physicaltherapy sessions without justification, or any der-matologicalissuewhichwouldpreventthemfromenteringa therapeuticpool,wereexcludedfromthestudy.TheNational Ethics Boardapprovedthisstudy,and allpatientsprovided writteninformedconsent.
Studydesign
Questionnaires
TheLequesne’sAlgofunctionalQuestionnairewasdeveloped forpatientswithosteoarthritisandevaluatessymptomsand functionalcapacityofthehipandknee.Thisindexis com-posed of 11 questions that evaluate pain, discomfort and function.TheODIisaself-administeredquestionnaireused tomeasurethedegreeoflumbarspinedisability,andcontains topicsconcerningintensityofpainandphysicalactivity.17The ODIhasbeenusedinscientificresearchtoevaluatepatients withnonspecificorspecificlow-backpainaftersurgical pro-cedures,medicationandrehabilitation.
Rangeofmotion
TheRoMwasevaluatedbyasingleexaminerusinga conven-tional360◦ freeshaftgoniometer.Thefollowingmovements
were assessed: trunk flexion and extension and flexion, extension,adductionandabductionofthehipjoint, accord-ing to the standardization of the goniometry manual of Marques.18
Musclestrength
MSwas analyzedbymaximal voluntaryisometric contrac-tion(MVIC)usingaloadcell(MIOTEC®,PortoAlegre,Brazil).
The load cell was connected to a Miotool400® apparatus
(MIOTEC®)usingaSDS1000®sensorconnectedviaaUSBcable
to a notebook. During movements, the force generated by tractionontheload cellwastransmittedtothe Miograph®
softwarewhichproducesaplotofMSinkilograms-force(kgf). VolunteersweresubmittedtoisometricMStestsofthetrunk flexorsandextensorsand hipflexors,extensors, adductors andabductors.
Surfaceelectromyography
Myoelectricsignalsofthegluteusmaximus,gluteusmedius, tensor fascialata, longdorsal (longissimus)and iliocostalis musclesweresampledat2000Hzinsingledifferentialmode
from each muscle through a four channel electromyogra-physystem(MIOTEC®,PortoAlegre,Brazil)usingdisposable
Ag/AgCIcircularbipolarelectrodes(3M®).The10mm
diame-terelectrodeswithadhesiveconductinggelwerepositioned on the skin overlying the muscles at an inter-electrode distance of 20mm. Abrasion of the skin was achieved at the fixation sites with gauze soaked in alcohol to reduce impedanceandtheelectrodeswerethenfixedatthemuscular belly, distant from the motor point, and fixed with trans-parenttapeand elasticband wrappingtoavoidmovement artifacts.ThedataacquisitionMiographUSB®software
sys-temwithwindowing32(RMS–RootMeanSquare)andgain of2000foreachchannelwasusedtocapturetheelectrical potentialsofthemusclesevaluatedinmicrovolts(V).
But-terworthfilterswereused:order4andbandpass20–500Hz. The four channels were connected toactive SDS500®
sen-sorsbyclamps.SignalanalysiswasperformedusingMiograph USB® system software.The sensorswere calibrated before
datacollection.Theelectricalpotentialsofthemuscleswere collected inaccordance to international standardizationof SENIAM.19
Aquaticphysiotherapy
The 9m2 pool in a 16m2 room was warmed to 34◦C;
the patients changed their clothes in this temperature-controlled room. Each session consisted of lower limb muscle stretching, jogging in the pool (forward, backward and sideways), suspended bicycle exercises in the vertical position, stair climbing exercises, active exercises in the supine position using floats, and finally relaxation exer-cises.
Conventionalphysiotherapy
Eachsessionconsistedoflowerlimbstretches,hipexercisesto strengthenhipadductorsandabductors,supinebridge, exer-cisesusingankle-weightstostrengthenthequadricepsand whennecessary,transcutaneouselectricalnervestimulation wasusedforpainrelief.
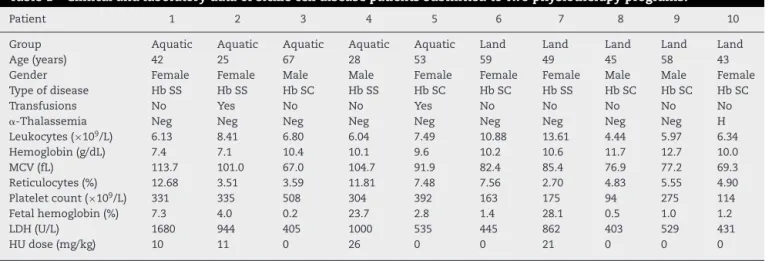
Table1–Clinicalandlaboratorydataofsicklecelldiseasepatientssubmittedtotwophysiotherapyprograms.
Patient 1 2 3 4 5 6 7 8 9 10
Group Aquatic Aquatic Aquatic Aquatic Aquatic Land Land Land Land Land
Age(years) 42 25 67 28 53 59 49 45 58 43
Gender Female Female Male Male Female Female Female Male Male Female
Typeofdisease HbSS HbSS HbSC HbSS HbSC HbSC HbSS HbSC HbSC HbSC
Transfusions No Yes No No Yes No No No No No
␣-Thalassemia Neg Neg Neg Neg Neg Neg Neg Neg Neg H
Leukocytes(×109/L) 6.13 8.41 6.80 6.04 7.49 10.88 13.61 4.44 5.97 6.34
Hemoglobin(g/dL) 7.4 7.1 10.4 10.1 9.6 10.2 10.6 11.7 12.7 10.0
MCV(fL) 113.7 101.0 67.0 104.7 91.9 82.4 85.4 76.9 77.2 69.3
Reticulocytes(%) 12.68 3.51 3.59 11.81 7.48 7.56 2.70 4.83 5.55 4.90
Plateletcount(×109/L) 331 335 508 304 392 163 175 94 275 114
Fetalhemoglobin(%) 7.3 4.0 0.2 23.7 2.8 1.4 28.1 0.5 1.0 1.2
LDH(U/L) 1680 944 405 1000 535 445 862 403 529 431
HUdose(mg/kg) 10 11 0 26 0 0 21 0 0 0
20
15
10
5
80
60
40
20
0
Pre Post Pre Post
Lequesne Os
w
estr
y
Questionnaires
AP CP
AP CP
P2=.3125
P2=.1250
P1=.0217 P1=.0112
P2=.0625
P2=.1250
Figure1–Median,minimumandmaximumvaluesoftheLequesneindex(Lequesne’sAlgofunctionalQuestionnaire)and OswestryDisabilityIndexevaluatedbeforeandafterinterventionsfortheaquaticphysiotherapy(AP)andconventional physiotherapy(CP)groups.Thep1-valuereferstothecomparisonofnumericalvaluesovertimewithrepeated
measurementswithtransformationstations(ANOVAtest).Thep2-valuereferstothecomparisonbetweentimepointsfor
eachgroup(Wilcoxontest).
Statisticalanalyses
Thestatisticalanalysissystem(SAS)computerprogramfor Windows (version9.2) and GraphPad Prism(version 5.00 – Trial)wereusedforstatisticalanalysis.Ap-valueof0.05orless wasconsidered statistically significant.Thefollowingtests werethenperformed.
Fisher’s exact test to compare proportions, the Mann–Whitney test to compare numerical measurements
betweenthetwogroups,ANOVAtocomparenumericalvalues overtimewithrepeatedmeasurementswithtransformation stationsandtheWilcoxontestforpairedsamplesbeforeand aftertheintervention.
Results
Thefinalsamplecomprisedtenvolunteersrandomizedinto twogroups:APandCP.Medianagewas42yearsold(range:
Pre Post
Pre Post
Pre Post
Pre Post
Pre Post
Pre Post
AP CP
AP CP
AP CP
AP CP AP CP AP CP Range of Motion
P2=1,0000
P2=.2500
P2=.6250
P2=.1250
P2=.6250
P2=1,0000
P2=.5000
P2=.8750
P2=.5000
P2=1,0000
P2=.1250
P2=.6250 120
100
80
60
160
140
120
100
80
40
35
30
25
20
RoM T
runk
Fle
xion
RoM Hip Fle
xion
RoM Hip Abduction
40
30
20
10
RoM T
runk
Extension
RoM Hip Extension
RoM Hip Abduction
80
60
40 30
25
20
15
10
P1=.1327 P1=.0320
P1=.0610 P1=.9029
P1=.6240 P1=1,0000
Figure2–Median,minimumandmaximumvaluesofRangeofMotion(RoM)oftruckflexionandextensionandhip flexion,extension,adductionandabductionmeasuredbygoniometry.Variablesevaluatedbeforeandafterinterventions fortheaquaticphysiotherapy(AP)andconventionalphysiotherapy(CP)groups.Thep1-valuereferstothecomparisonof
numericalvaluesovertimewithrepeatedmeasurementswithtransformationstations(ANOVAtest).Thep2-valuerefersto
25
20
20
10
5
25 20
15
10
5
0
20
20
10
5
30
25
20
10 15
5
25
20
20
10
5
25
20
20
10
5
Pre Post Pre Post
Pre Post Pre Post
Pre Post Pre Post
MS T
runk
Fle
xion
MS T
runk
Extension
MS Hip Fle
xion
MS Hip Extension
MS Hip Adduction MS Hip Abduction
P2=.3125
P2=.1250
P2=.4375
P2=.1875
P2=.3125
P2=.7500
P2=.5000
P2=.1250
P2=.6250
P2=.0625
P2=.1875
P2=.0625 AP
CP
AP CP
AP CP
AP CP AP CP AP CP Muscle Stren
P1=.0459 P1=.1159
P1=.2468 P1=.0062
P1=.1300 P1=.0257
Figure3–Median,minimumandmaximumvaluesofmusclestrength(MS)ofthetrunkflexorsandextensors,andhip flexors,extensors,adductorsandabductorsbyloadcell.Variablesevaluatedbeforeandaftertheinterventionsforthe aquaticphysiotherapy(AP)andconventionalphysiotherapy(CP)groups.Thep1-valuereferstothecomparisonofnumerical
valuesovertimewithrepeatedmeasurementswithtransformationstations(ANOVAtest).Thep2-valuereferstothe
comparisonbetweentimepointsforeachgroup(Wilcoxontest).
25–67)fortheAPgroupand49yearsold(range:43–59)forthe CPgroup.Theclinicalandlaboratorydataoftheparticipants areshowninTable1.
Comparisonofnumericalvaluesover time betweenthe two groups showed a statistically significant difference after the intervention in respect to the Lequesne index (p-value=0.0217),ODI(p-value=0.0112),RoMoftrunk exten-sion (p-value=0.0320), trunk flexion MS (p-value=0.0459), and hip extension and abduction MS (p-value=0.0062 and p-value=0.0257,respectively).Therewerenosignificant sta-tistical differences in the RoM of trunk and hip flexion, extension, adduction and abduction, trunk extensor MS and hip flexion and adduction MS and all SEMG variables (Figures1–4).
Discussion
Thepresentstudyaimedtoevaluatetwotypesof physiother-apyintervention forhip and lumbarspine functionalityof
adultSCDpatients.Thedominantsideofeachpatientwas consideredintheresults.15,16
Themajorlimitationofthisstudywastherecruitmentof volunteers,asmostofthepatientslivefarfrom thecenter andfinditverydifficulttoattendtheclinictwiceeveryweek. Therefore,onlytenpatients,sixcompoundheterozygousfor Hb SandHb CandfourHb Shomozygotes,completedthe physiotherapeuticprogram.
Surface Electromyography
Pro Post Pro Post
Pro Post
Pro Post
Pro Post
600
400
200
0
600
400
200
0
800
600
400
200
0
800
600
400
200
0
800
600
400
200
0
SEMG IIiocostalis
SEMG
T
ensor F
ascia Lata
SEMG Gluteus Medius
SEMG Gluteus Maxim
us
SEMG Dorsal Longissm
us
P2=.3125
P2=.3125
P2=.6250
P2=.3125
P2=.3125
P2=.6250
P2=.3125
P2=.8125
P2=1,0000
P2=.8125 AP CP
AP CP
AP CP
AP CP AP
CP
P1=.6424 P1=.1058
P1=.7210
P1=.9070
P1=.8576
Figure4–Median,minimumandmaximumvaluesofsurfaceelectromyography(SEMG)ofiliocostalis,longdorsal (longissimus),gluteusmaximus,gluteusmediusandtensorfasciaelataemuscles.Variablesevaluatedbeforeandafter interventionsfortheaquaticphysiotherapy(AP)andconventionalphysiotherapy(CP)groups.Thep1-valuereferstothe
comparisonofnumericalvaluesovertimewithrepeatedmeasurementswithtransformationstations(ANOVAtest).The p2-valuereferstothecomparisonbetweentimepointsforeachgroup(Wilcoxontest).
inhipfunctionalityandareinagreementwithWangetal.20 and Hinmanet al.21 who observed improvementin physi-calfunctionafteraprogramofaquaticphysicaltherapyfor patientswithhipandkneeosteoarthritis.Otherstudies car-riedoutinindividualswithhipand/orkneedisordershowever, showednosignificantdifferencesbetweenthetwo rehabilita-tionstrategies,suggestingthatbothtechniquesareequally effective.22–24
Lower back pain isone ofthe maincomplaints ofSCD patients.TheODIwashereinusedtoassesslowerbackpain andfunctionduringdailyactivities.Thisindexalsoshowed statisticallysignificant improvementsinbothstudy groups aftertheintervention.TheCPgroupimprovedfrom moder-atedisability(26.5%)tominimaldisability(18%);theAPgroup, however,despitesomesignificantimprovementinthescores ofthesecondassessment(from35%to22%)showednochange intheseverityofthedisabilitycausedbybackpain.Longeror morefrequentsessionsmayrenderbetterresults,ashasbeen describedbyothers.24,25 Thesestudiesshowedthatpatients who performed AP twoor more times weekly had greater improvementinphysicalassessmentscoresthanthosewho exercisedonlyonceaweek.24,25Nevertheless,Ariyoshietal.25
extended the program for six months and concluded that watertherapy exerciseswere usefulforpatients withback painastheyprovidepainrelief.
Inthisstudy,asignificantimprovementinRoMofthetrunk extensionandatrendtowardanimprovementintrunk flex-iongoniometrywereobservedinbothgroups,especiallyin theAPgroup.However,nosignificantchangewasdetectedin eithergroupregardingmotionamplitude,probablyduetothe inflammatoryphenomenaand boneinfarctionswhich may havecausedpermanentlimitations.
Furthermore,lateinterventionsmay notbesufficientto improvejointRoMinthisagegroupinwhichchronic degen-erativehipinjuriesmayhavereachedalevelofseveritythat precludesgreaterjointflexibility.
Moreover,thefactthattherewasnosignificant improve-mentingoniometrymaybeaconsequenceofthetechniques used inbothgroups whichmay favor strength gain.Thus, perhaps the program should increase the time devoted to stretchingcertaintargetmusclesduringtherapy,thereby pro-motingimprovedmuscleflexibility.
thetrendtowardimprovementintrunkextensorMSinthe APgroup,therewerenosignificantdifferencesbetweenthe twogroups.Theseresultsareinagreementwithotherstudies thatshowedimprovedMSafterspecificland-basedand water-basedtrunkexercises.24,26,27
Therewasastatisticallysignificantincreaseinhip exten-sionandabductionMSinbothgroupsaftertheinterventions. Although,hipflexionMSwasunchangedintheCPgroup,there wasatrendtowardimprovementinthe APgroup,andhip adductionMSshowedaslighttrendtowardimprovementin bothgroups.
Thus, albeit slight, the results of this study showed improvementofallMSvariablesintheAPgroup,inaccordance withWangetal.20whoalsoobservedimprovedflexibilityand lower limbstrength after12 weeksofaquatictherapy, and Cochraneetal.28 who observedsignificant improvementin painandphysicalfunctionafteraquaticexercisesinadults withhipandkneeosteoarthritis.Inanotherstudy,Rahmann29 demonstratedapositiveeffectofaspecificprogramofaquatic physicaltherapyonearlyrecoveryofstrengthafterhipand kneesurgeries.Furthermore,Hinmanetal.21observedaslight improvementinpain, physicalfunction, qualityoflifeand MS after aquatic therapy for patients with hip and knee osteoarthritis in a protocol of two sessions per week for sixweeks.However,Jigami23concludedthatbothprograms, land-basedandwater-based,evenwhentheexerciseswere performedonlyonceaweek,improvedoverallphysical activ-ityandMSinthelowerlimbsofosteoarthritispatients.
Surfaceelectromyographydidnotshowanysignificant dif-ferenceaftertheinterventionsofbothgroups.However,there seemedtobeanimprovementintheelectromyography sig-nalofallmusclesevaluatedintheAPgroup.Thebetterresult obtainedinthisgroupmayberelatedtothegreateramount ofmuscle fibers recruited in aquatictherapy added tothe physicalpropertiesofwatersuchasbuoyancyand multidi-rectionalstrength.Thesefindingsareinagreementwiththe resultsreportedbyKanedaetal.30whoobservedgreater elec-tromyographyactivityofallmusclemovementsperformedin thewaterwithfloatingdevices.
Theresultsofthisstudyshouldbeanalyzedwithcautionas thesamplesizemayhavebeenalimitingfactorandtherefore, furtherstudiesareneededtoconfirmtheseresults.
Conclusion
Theresultsobtainedheresuggestthatphysicaltherapyisa resourcecapableoftreatingmusculoskeletaldysfunctionin SCDpatientsregardlessofthetechniqueused.However, exer-cisesdesignedtostretchtoneand strengthenthecoreand limbmusclescarriedoutinthewaterrequiregreater stabi-lizationofthemusclesandmayjustifythetrendtowardthe betterresultsobtained.
Funding
ThisworkwassupportedbytheConselhoNacionalde Desen-volvimentoCientíficoeTecnológico(CNPq),andFundac¸ãode Coordenac¸ãodeAperfeic¸oamentodePessoaldeNível Supe-rior(CAPES).TheHemocentro,UNICAMP,isapartofInstituto
NacionaldeCiênciaeTecnologiadoSangue,Brazil(INCTdo Sangue–CNPq/MCT/FAPESP).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
The authors thankProf.MargarethCastroOzelo forkindly making the facilities at the Hemophilia Unit available; Dr. MarinaPereiraColellaforhelpingrecruitthepatients,Márcia Matta,JanaínaBossoRicciardiandGlendaFeldbergAndrade Pintofortheirtechnicalassistance;andRaquelFoglioforthe editingandEnglishrevision.
r
e
f
e
r
e
n
c
e
s
1.BaldanziG,TrainaF,MarquesNetoJF,SantosAO,RamosCD, OlallaSaadST.Lowbonemassdensityisassociatedwith hemolysisinBrazilianpatientswithsicklecelldisease. Clinics.2011;66(5):801–5.
2.AlmeidaA,RobertsI.Boneinvolvementinsicklecelldisease. BrJHaematol.2005;129(4):482–90.
3.SerarslanY,KalaciA,OzkanC,DogramaciY,CoklukC,Yanat AN.Morphometryofthethoracolumbarvertebraeinsickle celldisease.ClinNeurosci.2010;17(2):182–6.
4.AkinyoolaAL,AdediranIA,AsaleyeCM,BolarinwaAR.Risk factorsforosteonecrosisofthefemoralheadinpatientswith sicklecelldisease.IntOrthop.2009;33(4):923–6.
5.HuoMH,FriedlaenderGE,MarshJS.Orthopaedic manifestationsofsickle-celldisease.YaleJBiolMed. 1990;63(3):195–207.
6.ShethS,LicursiM,BhatiaM.Sicklecelldisease:timefora closerlookattreatmentoptions?BrJHaematol.
2013;162(4):455–64.
7.OsunkwoI.Anupdateontherecentliteratureonsicklecell bonedisease.CurrOpinEndocrinolDiabetesObes. 2013;20(6):539–46.
8.OharaDG,RuasG,CastroSS,MartinsPRJ,WalshIA.Dor osteomuscular,perfilequalidadedevidadeindivíduoscom doenc¸afalciforme.RevBrasFisioter.2012;16(5):431–8. 9.NeumayrLD,AguilarC,EarlesAN,JergesenHE,Haberkern
CM,KammenBF,etal.Physicaltherapyalonecomparedwith coredecompressionandphysicaltherapyforfemoralhead osteonecrosisinsicklecelldisease.Resultsofamulticenter studyatameanofthreeyearsaftertreatment.JBoneJoint SurgAm.2006;88(12):2573–82.
10.BarkerAL,TalevskiJ,MorelloRT,BrandCA,RahmannAE, UrquhartDM.Effectivenessofaquaticexercisefor
musculoskeletalconditions:ameta-analysis.ArchPhysMed Rehabil.2014;95(9):1776–86.
11.BeckerBE.Aquatictherapy:scientificfoundationsandclinical rehabilitationapplications.PMR.2009;1(9):859–72.
12.PoyhonenT,SipilaS,KeskinenKL,HautalaA,SavolainenJ, MalkiaE.Effectsofaquaticresistancetrainingon
neuromuscularperformanceinhealthywomen.MedSci SportsExerc.2002;34(12):2103–9.
13.DoigGS,SimpsonF.Randomizationandallocation concealment:apracticalguideforresearchers.JCritCare. 2005;20(2):187–91.
15.SadeghiH,AllardP,PrinceF,LabelleH.Symmetricandlimbin able-bodiedgait:areview.GaitPosture.2000;12(1):34–45. 16.MartinWL,PoracC.Patternsofhandednessandfootedness
inswitchedandnonswitchedBrazilianleft-handers:cultural effectsonthedevelopmentoflateralpreferences.Dev Neurophysiol.2007;31(2):159–79.
17.CoelhoRA,SiqueiraFB,FerreiraPH,FerreiraML.
ResponsivenessoftheBrazilian–Portugueseversionofthe OswestryDisabilityIndexinsubjectswithlowbackpain.Eur SpineJ.2008;17(8):1101–6.
18.MarquesAP.ManualdeGoniometria:Segundaedic¸ão revisadaeampliada.Barueri:Manole;2003.
19.HermensHJ,FreriksB,Disselhorst-KlugC,RauG. DevelopmentofrecommendationsforSEMGsensorsand sensorplacementprocedures.JElectromyogrKinesiol. 2000;10(5):361–74.
20.WangTJ,BelzaB,ThompsonF,WhitneyJD,BennettK.Effects ofaquaticexerciseonflexibility,strengthandaerobicfitness inadultswithosteoarthritisofhiporknee.JAdvNurs. 2007;57(2):141–52.
21.HinmanRS,HeywoodSE,DayA.Aquaticphysicaltherapyfor hipandkneeosteoarthritis:resultsofasingle-blind
randomizedcontrolledtrial.PhysTher.2007;87(1):32–43. 22.BatterhamSI,HeywoodS,KeatingJL.Systematicreviewand
meta-analysiscomparinglandandaquaticexercisefor peoplewithhiporkneearthritisonfunction,mobilityand otherhealthoutcomes.BMCMusculoskeletDisord. 2011;12:123.
23.JigamiH,SatoD,TsubakiA,TokunagaY,IshikawaT,Dohmae Y,etal.Effectsofweeklyandfortnightlytherapeuticexercise
onphysicalfunctionandhealth-relatedqualityoflifein individualswithhiposteoarthritis.JOrthopSci. 2012;17(6):737–44.
24.Baena-BeatoPA,Arroyo-MoralesM,Delgado-FernándezM, Gatto-CardiaMC,ArteroEG.Effectsofdifferentfrequencies (2–3days/week)ofaquatictherapyprograminadultswith chroniclowbackpain.Anon-randomizedcomparisontrial. PainMed.2013;14(1):145–58.
25.AriyoshiM,SonodaK,NagataK,MashimaT,ZenmyoM,Paku C,etal.Efficacyofaquaticexercisesforpatientswith low-backpain.KurumeMedJ.1999;46(2):91–6.
26.FreitasCD,GreveJM.Estudocomparativoentreexercícios comdinamômetroisocinéticoebolaterapêuticanalombalgia crônicadeorigemmecânica.FisioterPesqui.2008;15(4): 380–6.
27.CarpenterDM,NelsonBW.Lowbackstrengtheningforthe preventionandtreatmentoflowbackpain.MedSciSports Exerc.1999;31(1):18–24.
28.CochraneT,DaveyRC,MatthesEdwardsSM.Randomized controlledtrialofthecosteffectivenessofwater-based therapyforlowerlimbosteoarthritis.HealthTechnolAssess. 2005;9(31),iii–iv,ix–xi,1–114.
29.RahmannAE,BrauerSG,NitzJC.Aspecificinpatientaquatic physiotherapyprogramimprovesstrengthaftertotalhipor kneereplacementsurgery:arandomizedcontrolledtrial. ArchPhysMedRehabil.2009;90(5):745–55.