revbrashematolhemoter.2014;36(6):442–444
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
w w w . r b h h . o r g
Case
report
Myelodysplastic
syndrome
with
synchronous
gastric
cancer:
when
the
symptoms
suggest
something
else
Paula
de
Melo
Campos
a,∗,
Fabiola
Traina
a,b,
Irene
Lorand-Metze
a,
Sara
Teresinha
Olalla
Saad
aaUniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
bUniversidadedeSãoPaulo(USP),RibeirãoPreto,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received17December2013 Accepted4June2014 Availableonline17July2014
Keywords:
Pancytopenia
Myelodysplasticsyndromes Hematologicneoplasms Secondaryneoplasms Primaryneoplasms
a
b
s
t
r
a
c
t
Althoughmyelodysplasticsyndromeshaveacleardefinitionintheory,themorphologic dys-plasiaassociatedwithineffectivehematopoiesismaybesubtleanddifficulttorecognizeand cancommonlybemimickedbysystemicconditions,suchasinfections,autoimmune disor-ders,nutritionaldeficiencies,toxicfactorsandnon-hematologicalmalignancies.However, myelodysplasticsyndromesmaytrulycoexistwithothersystemicdiseases,whichcanbe maskedwhenthepatient’ssymptomsareattributedexclusivelytomyelodysplastic syn-dromeswithoutfurtherinvestigation.Tobetterillustratethis,wehereindescribetwocases associatedwithsynchronousgastriccancers.
©2014Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
Introduction
Themyelodysplasticsyndromes(MDS)areclonal hematopoi-eticstemcelldisorderscharacterizedbydysplasiaofatleast oneofthemyeloidcelllines, increasedapoptosis and inef-fectivehematopoiesis.Theycompriseaheterogeneousgroup ofdiseasesvarying fromindolent cases, characterized pre-dominantlybycytopenias,toaggressivediseaseshowinghigh blastcountsandasignificantpropensitytoevolveintoacute
∗ Correspondingauthorat:Hemocentro,UniversidadeEstadualdeCampinas(UNICAMP),RuaCarlosChagas,480,13083-878Campinas,
SP,Brazil.
E-mailaddress:[email protected](P.deMeloCampos).
myeloidleukemia.1 Thus,medicalcentersutilizethe World
HealthOrganization(WHO)2008criteriaandtheInternational PrognosisScoringSystem(IPSS)toclassifyandpredict prog-nosisinthesepatients.
AlthoughMDShaveacleardefinitionintheory,the mor-phologicdysplasiaassociatedwithineffectivehematopoiesis maybesubtleanddifficulttorecognize,2andcancommonly
be mimicked by other systemic conditions, such as infec-tions, autoimmune disorders,nutritional deficiencies,toxic factorsandnon-hematologicalmalignancies.1However,MDS
http://dx.doi.org/10.1016/j.bjhh.2014.07.005
revbrashematolhemoter.2014;36(6):442–444
443
maytrulycoexistwithothersystemicdiseases,whichcanbe maskedifthepatient’ssymptomsareattributedexclusively toMDSwithoutfurtherinvestigation.Tobetterillustratethis, wereportontwocasesofMDSassociatedwithsynchronous gastric cancers. Thefirst patientis ayoung ladywho pre-sentedwithmoderateanemiaandconstitutionalsymptoms. Thesecondcaseisa67-year-oldmanwithpancytopeniaand fatigue.
Case1
Ourfirstpatient,a36-year-oldwomanwithaprevious his-toryofdiabetesmellitus andischemiccardiomyopathyhad complaints of persistent anemia, fatigue and weight loss (17 pounds in six months). She was 19 weeks pregnant and had no other significant past medical, family or exposure history. The results of her physical examination were unremarkable. She had neverrequired red blood cell transfusions. Her complete blood counts showed the fol-lowing: hemoglobin=6.0mg/dL, mean corpuscular volume (MCV)=96.3fL,plateletcount=158×109/L,andabsolute neu-trophil count=2.9×109/L. Iron studies were normal and nutritionaldeficiencieswere ruledout.Shehadnosignsof infectiousdiseasesandserologyforhepatitisBandC,human immunodeficiency virus (HIV) and cytomegalovirus (CMV) were negative.Abone marrow(BM) biopsy wasperformed whichshowedhypercellularity(95–100%)withnoatypiasor reticulin fibrosis. BM cytology showed 4.4% of blasts with nosignificant dysplasticchangesinany hematopoietic lin-eages,normalironstoresandnoringsideroblasts.Cytogenetic analysiswasnormal(46,XX).Flowcytometrydetectedthree immunophenotypicabnormalities.Atthattime,thecriteria wasnot yetsufficientto establish adefinitive hematologic diagnosis.Thepatientreceivedtwounitsofpackedredcells andherbloodcountsremainedstableduringtherestofthe pregnancy.
After delivery, the patient evolved with a deterio-ration of blood counts (hemoglobin=6.1mg/dL, platelet count=78×109/L,andabsoluteneutrophilcount=3.3×109/L) and began to require frequent red blood cell transfusions. Bonemarrowcytologywasagainperformedandshowed11% ofblasts,withnosignificantdysplasiaandanormal karyo-type.A BM biopsy revealed hypolobulated megakaryocytes (Figure1).ThediagnosisofMDS(WHO2008refractory ane-miawithexcess blasts-2[RAEB-2]and IPSSIntermediate-2) wasreached.
Subsequently,asthepatientcomplainedoffurther signif-icantweightlossandconstitutionalsymptoms,ascreening for malignancies was performed: a chest X-ray was nor-mal,but anabdominalcomputedtomographyscanshowed ahomogeneousenlargementofthe spleen(30cm), and an uppergastrointestinal endoscopyshowedanadvanced ele-vatedlesioninthestomachwithabiopsyconfirmingagastric tubularadenocarcinoma withareas showingadiffuse pat-ternofsignet-ringcellcarcinoma.Shewassubmittedtototal gastrectomy withlymphadenectomyand splenectomy. The stomachbiopsyconfirmedadiffusesignet-ringcellcarcinoma withinvolvedmarginsandsignsoflymphaticandperineural invasion,whereasthespleenbiopsyshowedonlyhyperplasia.
Figure1–Bonemarrowhistology.Moderate
hypercellularityandmildmaturationarrestofthe
granulocyticcompartment,predominatinginthe
erythroblastcompartment.Megakaryocytesareincreased
innumberandarehypolobulated(hematoxylinandeosin:
400×).
Thepatientstartedchemotherapywiththeetoposide, l-leucovorinandfluorouracil(ELF)regimenforadvancedgastric cancer,butdiedfourmonthslaterduetoamassivepulmonary thromboembolism.
Case2
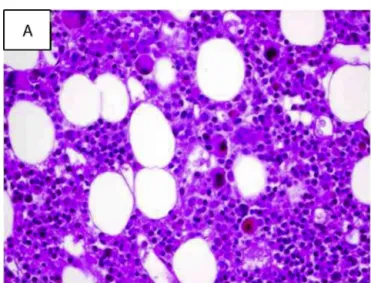
The second case is a 67-year-old gentleman who com-plained of weakness, fatigue and weight loss (31 pounds in four months). He had been diagnosed with systemic hypertension,diabetesmellitusandcongestiveheartfailure, but no other significant past medical, family or expo-sure history. His physical examination was unremarkable. His completeblood countrevealed:hemoglobin=6.4mg/dL, MCV=112.0fL, plateletcount=28×109/L, andabsolute neu-trophilcount=0.7×109/L.Screeningfornutritional deficien-ciesshowedavitaminB12levelof190pg/mL(belowreference range).ABMbiopsyshowedmoderatehypercellularitywith atypical megakaryocytes (Figure 2), no significant dysplas-tic changes and moderate diffuse reticulin fibrosis. A BM aspirationrevealeddyserythropoiesis,cytoplasmic hypogran-ularity, nomegaloblastic changes,no ring sideroblasts and 9%ofblasts,withnormalcytogenetics(46,XY).Flow cytom-etrydetectedfiveimmunophenotypicabnormalities.Vitamin B12wassupplemented,but therewasnoincreaseinblood counts.Infectiousdiseaseswereruledout.Thediagnosisof MDS(WHO2008RAEB-1andIPSSIntermediate-1)wasreached andthepatientwasincludedintheregulartransfusion pro-gram.
444
revbrashematolhemoter.2014;36(6):442–444Figure2–Bonemarrowhistology.(A)Intensehypercellularityandmaturationarrestofhematopoieticcomponents. Megakaryocytesareatypical:dwarfandhypolobulated(hematoxylinandeosin:400×).(B)Silverimpregnationshows
moderateincreaseinreticulinfibers(400×).
adenocarcinoma in situ. A therapeutic upper gastrointesti-nalendoscopywassubsequentlycarriedout,butendoscopic resection of the lesion was not possible, since the gas-tric mucosa was friable and hemorrhagic. At that time, blood counts continued to drop (hemoglobin=transfusion dependent, platelet count=6×109/L, absolute neutrophil count=0.3×109/L).Thepatientwassubsequentlysubmitted toapartiallaparoscopicgastricresection,butdiedelevendays laterduetopostoperativefeverandseveresepsis.
Discussion
and
conclusions
As the diagnosis of MDS is based mainly on an assess-ment ofthe morphology, the diagnosis can be subjective, particularly in patients with early low risk disease pre-sentinganormalkaryotype.Ingeneral,diagnosisiseasierin patientswithexcessblasts.Sincetherearemanyconditions thatcanmimicMDS,aclinicalassessmentwiththe exclu-sion ofadditional systemic conditions, such asnutritional deficiencies, autoimmunedisorders and non-hematological malignancies is needed.3 There are no studies describing
theincidenceofsynchronousnon-hematologicalneoplasms occurring concurrently with MDS, and so this seems to be relatively uncommon. However, the presence of symp-tomswhich are notfrequently associated with MDS, such as significant constitutional symptoms, excessive weight loss and localized pain should raise clinical suspicion of associatedmalignancies,leadingtoan extensive investiga-tion.
Hereinwedescribedtwocasesofsynchronousgastric can-cerandmyelodysplasiainayoungandanelderlypatient.This isararecondition,andthereareveryfewreportsdescribing thisassociation.4,5Similarly,intheclinicalpractice,dropsin
bloodcountsofpatientswithnon-hematological malignan-ciesareveryfrequentlyattributedto‘secondary’conditions, suchas,forexample,chronicdisease anemiaand immune thrombocytopenias.Itisimportanttopointoutthe possibil-ityofcoexistenceofMDSwithotherneoplasmsandsobone marrowstudiesshouldalwaysbeconsidered.
RegardingthesimultaneousoccurrenceofMDSand non-hematologicalneoplasms,wehypothesizethataninitialevent selecting a stem cell clone, together withabnormalities in immunosurveillance,maymanifestwithahigherpropensity tocancer.Alternatively,anincreasedchromosomal instabil-ity whichseems tobeassociatedwithimmunodeficiencies mightberesponsibleforthedevelopmentofcancer.5Finally,
a decreasedfunctionoftumorsuppression genescould be animportantfinalfactorthatwouldallowmalignantcellsto proliferate.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
TheauthorswouldliketothankRaquelS.Foglioforreviewing theEnglish,andProf.Dr.JoséVassaloforprovidingthefigures.
r
e
f
e
r
e
n
c
e
s
1.BrunninRD,OraziA,GermingU,LeBeauMM,PorwitA, BaumannI,etal.Myelodysplasticsyndromes/neoplasms, overview.WHOclassificationoftumorsofhaematopoieticand lymphoidtissues;2008.p.88–93.
2.OdenikeO,AnastasiJ,LeBeauMM.Myelodysplastic syndromes.ClinLabMed.2011;31(4):763–84.
3.Garcia-ManeroG.Myelodysplasticsyndromes:2011updateon diagnosis,risk-stratification,andmanagement.AmJHematol. 2011;86(6):490–8.
4.TakahashiT,KazamaY,ShimizuH,YoshimotoM,TsujisakiM, AokiS,etal.Myelodysplasticsyndromeprogressesrapidlyinto erythroleukemiaassociatedwithsynchronousdoublecancers ofthestomachandthepapillaofVater.IntJHematol. 2001;74(1):64–9.
5.KondoH,ShinboI.Myelodysplasticsyndromeassociatedwith gastriccancerandcolonpolyp.RinshoKetsueki.