Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
w w w . r b h h . o r g
Original
article
Normative
evaluation
of
blood
banks
in
the
Brazilian
Amazon
region
in
respect
to
the
prevention
of
transfusion-transmitted
malaria
Daniel
Roberto
Coradi
Freitas
a,b,∗,
Elisabeth
Carmen
Duarte
aaUniversidadedeBrasília(UnB),Brasília,DF,Brazil
bAgênciaNacionaldeVigilânciaSanitária(ANVISA),Brasília,DF,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received12August2013 Accepted25June2014
Availableonline27September2014
Keywords:
Healthevaluation Malaria
Bloodbanks Donorselection Bloodsafety
a
b
s
t
r
a
c
t
Objective:ToevaluatebloodbanksintheBrazilianAmazonregionwithregardtostructure andproceduresdirectedtowardthepreventionoftransfusion-transmittedmalaria(TTM).
Methods:ThiswasanormativeevaluationbasedontheBrazilianNationalHealth Surveil-lanceAgency(ANVISA)ResolutionRDCNo.153/2004.Tenbloodbankswereincludedinthe studyandclassifiedas‘adequate’(≥80points),‘partiallyadequate’(from50to80points),or ‘inadequate’(<50points).Thefollowingcomponentswereevaluated:‘donoreducation’(5 points),‘clinicalscreening’(40points),‘laboratoryscreening’(40points)and‘hemovigilance’ (15points).
Results:Theoverallmedianscorewas49.8(minimum=16;maximum=78).Fivebloodbanks wereclassifiedas‘inadequate’andfiveas‘partiallyadequate’.Themedianclinicalscreening scorewas26(minimum=16;maximum=32).Themedianlaboratoryscreeningscorewas 20(minimum=0;maximum=32).Eightbloodbanksperformedlaboratorytestsformalaria; sixtestedalldonations.Sevenusedthicksmears,butonlyoneperformedthisprocedure inaccordancewithMinistryofHealthrequirements.OneservicehadaProgramof Exter-nalQualityEvaluationformalariatesting.Withregardtohemovigilance,twoinstitutions reportedhavingprocedurestodetectcasesoftransfusion-transmittedmalaria.
Conclusion:Malariaisneglectedasablood–bornediseaseinthebloodbanksofthe Brazil-ianAmazonregion.Noneoftheinstitutionswereclassifiedas‘adequate’intheoverall classificationorwithregardtoclinicalscreeningandlaboratoryscreening.Bloodbank pro-fessionals,theMinistryofHealthandHealthSurveillanceservicemanagersneedtopay moreattentiontothismattersothatthesafetyproceduresrequiredbylawarecomplied with.
©2014Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthorat:UniversidadedeBrasília(UnB),CampusUniversitárioDarcyRibeiro,NúcleodeMedicinaTropical,70910-900
Brasília,DF,Brazil.
E-mailaddress:[email protected](D.R.C.Freitas).
http://dx.doi.org/10.1016/j.bjhh.2014.09.002
Introduction
Malariais endemicinthe BrazilianAmazonianregion and is mainly transmitted by vectors. Transfusion-transmitted malaria (TTM) is, however, one of the most important blood–borne parasitic diseases and representsa significant riskforpatientsinendemicareasascasesareusuallyvery severe.1,2 IntheUnitedStates,malariaisnotendemicwith onlythreeTTMcasesbeingreportedonaverageperannum.2 In Brazil, the National Hemovigilance System, created in 2002,3hasthusfarregisteredfourTTMcases,threein2006and onein2007.Byusingnucleicacidtests(NAT)todetect Plas-modiuminendemicareasinBrazil,theprevalenceofmalaria ineligibledonorsisestimatedtobebetween0.3%and3%.4–6 ItisthereforelikelythatTTMisunderreportedtotheNational HemovigilanceSystem.
InBrazil,theHealthSurveillanceservice(VISA)worksto controltransfusion risk and blood quality through actions suchas standard regulations, inspection, health education andhemovigilance.ThesemeasuresarecarriedoutbyVISA atfederal,stateandmunicipallevels.7Thetechnicaland san-itaryrequirementsforbloodbanks(BBs)topreventTTMhave beendefinedsince1988byLaw7649/19888 andother regu-lations–Decrees,MinistryofHealth(MoH)Ordinancesand ResolutionsoftheCollegiateDirectorate(RDC)oftheNational HealthSurveillanceAgency(ANVISA).
In1989,theMoHOrdinanceNo.721/GM/19899introduced the requirement for donor clinical and epidemiological screening, including history of previous infections, recent signsandsymptomsandtraveltoendemicareas.During reg-ulatory reviews,two substantial updates were included by ANVISARDCNo.343/2002,10namely: BBsinendemicareas mustusetheannualparasiteindex(API)toexcludedonors whovisithigh-risk areas(API >49.9cases/1000inhabitants) andmustperformlaboratorytestsoneligibledonors.All sub-sequentregulationshavemaintainedtheseobligationswith smallmodifications.
ThisstudypresentsanormativeevaluationofselectedBBs intheBrazilianAmazonregionwiththe aimofpreventing
TTM.Thestudy’sobjectivewastoanalyzetheadherenceof theseBBstoprevailingregulationsandstandards,todescribe anddiscussthecurrentpracticesoftheseestablishmentsand torecommendmeasurestoimprovethepreventionofTTM.
Methods
Thiswas anormativeevaluationstudy that focusedonan evaluation toinform management.11 According to Contan-driopoulosetal.,12toevaluateistomakeavaluejudgment aboutaninterventionoritscomponentsinordertoassist deci-sionmaking.Thejudgmentcanbebasedontheapplicationof criteriaandregulationsand,inthiscase,itiscalleda normat-iveevaluation.This,inturn,isdefinedastheactofmakinga judgment,comparingtheorganization(structure),the proce-dureormethodsdeveloped(process),theresourcesdeployed andtheresultsobtainedwiththerequirementsandcriteria establishedbyregulations.Itisascientificactivitythatmust becarriedoutwithmethodologicalrigor.13
This study used external evaluators with the eval-uation being performed in a natural context (without interventions).12 TheevaluationwasbasedonANVISARDC No.153/200414(RDC153/2004),inforceatthetime,regarding theissueofTTMprevention.Thecomponentsevaluatedwere structureandprocess.15
DatacollectiontookplacebetweenJanuary2009andJune 2011.All nineCoordinatorBBsresponsiblefortheBrazilian Amazon region and onehemotherapynucleus were evalu-ated. A standardizedsemi-structured list ofquestions was used tocollect databyinterviewingthe person technically responsible for the BB and/or the person responsible for the sectors/activities evaluated. Donor education, clinical screening,laboratoryscreeningandhemovigilancewere eval-uated.Theinterviewswereconductedbyjustoneresearcher withexperienceinadministeringinspectionquestionnaires andepidemiologyinterviewing.Inadditiontotheinterview, information was collected from educational materials for donorsandstandardsoperationalprocedures(SOP).
TheBBswereclassifiedasadequate,partiallyadequateor inadequate(Table1),dependingonthescoreobtained.The
Table1–Descriptionofthemodelforclassifyingsectors/activitiesandbloodbanksincludingscoresobtainedfollowing evaluation.
Sector/activity Weight No.ofitems Scorerange Classification
Education 0.5 1 0 Inadequate
5 Adequate
Clinicalscreening 4 10
0–20 Inadequate
>20–32 Partiallyadequate
>32–40 Adequate
Laboratoryscreening 4 5
0–20 Inadequate
>20–32 Partiallyadequate
>32–40 Adequate
Hemovigilance 1.5 2
0 Inadequate
7.5 Partiallyadequate
15 Adequate
Finalclassification – 18
0–50 Inadequate
form50to80 Partiallyadequate
conceptofpotentialrisk16wasdefinedas‘thepossibilityofthe occurrenceofadisease,whilstnotnecessarilydescribingthe diseaseorthelikelihoodofitsoccurrence.Thisconceptwhich expressesthevaluejudgmentaboutpotentialexposuretoa possibleriskwasusedtodefinetheweightingofeach activ-ityanditem.Differenttoepidemiologicalriskwhichcanbe measuredandcalculated,potentialriskisoftendetermined basedonthecumulativeperceptionofspecialistsregarding thedefectsorfaultsinagivenproduct,processorserviceover time.16Thecriteriaforthescoreswerethereforebasedonthe authors’assessmentofthepotentialriskofTTMcases occur-ringowingtonon-compliancewiththeitemsofthenorms. Clinicalandlaboratoryscreeningwereconsideredtobe criti-calfortheregulationofTTM.Thedetailsofthescoresforeach itemareshowninTable2.Althoughthecriteriaarebasedon RDC153/2004,thefinaltextofthecriteriaforeachitem eval-uatedexpressesthespecificfocusoncontrollingtheriskof TTM.Thecriteriaarenotthereforeliteraltranscriptionsofthe requirementsinRDC153/2004.
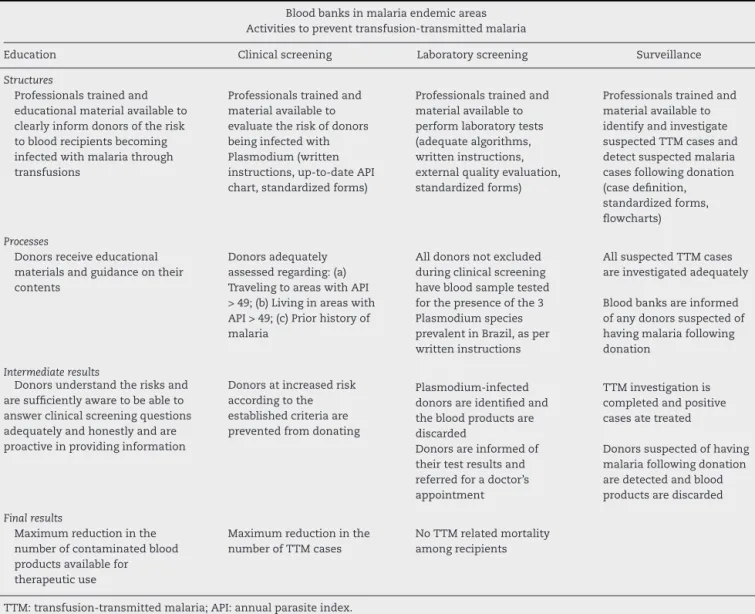
Theidealmodelofbestpracticesforensuringmaximum TTMriskreduction,accordingtoRDC153/2004,isshownin
Table3.InthismodelthefouractivitiesinvolvedinTTM
pre-ventionareshownastheyrelatetostructures,processesand results.
ThisstudywasapprovedbytheResearchEthics Commit-teesoftheJúlioMüllerUniversityHospitaloftheUniversidade FederaldeMatoGrossoandtheMedicineSchoolofthe Uni-versidadedeBrasília.
Results
ThefinalmedianscorefortheBBsasawholewas49.8 (min-imum=16; maximum=78) (Table4). None ofthe BBs were considered‘Adequate’;fivewere classifiedas‘Partially Ade-quate’ and five as ‘Inadequate’. Table 5 provides detailed resultsofthecomponentsanditems.
Withregardtothedonoreducationcomponent,allBBsonly usedleafletsandposterstoinformdonorsaboutblood–borne diseases.Malaria wasmentioned inleaflets inonlytwo of
thetenBBs(Table4).Fourtypesofleafletsproducedbythe
MoH werefound intwoBBs, but noneofthemmentioned TTM.
Six BBs were considered partially adequate and four wereconsideredinadequateinrelationtoclinicalscreening
(Table4).FiveBBshadSOPsforclinicalscreeningofmalariabut
onlyoneusedastandardizedscreeningformcontainingall theitemsrequiredbytheregulationtoevaluatepriorhistory ofmalaria (fever,suspectedmalaria andhavehad malaria)
(Table5).
SevenBBsusedexclusioncriteriaincasesofexposureto riskareas(Table5)basedonAPIratesandallofthemdefined high-riskareas as themunicipal.One BBalsotook district APIratesintoconsiderationwhenthemunicipalinquestion wasthestatecapitalcity.Fourdifferentineligibilityperiods wereidentifiedfordonorswhohadtraveledtohigh-riskareas, namely7(1/7),15(1/7),30(2/7)and180(3/7)days.The Epi-demiologicalSurveillanceServiceprovidessixofthetenBBs withtheAPIratesandoneofthetenBBsdirectlyaccessedthe APIratesintheInformationSystemforMalariainEndemic
Regions(SIVEP-Malaria).AllofthemusedAPIforthepreceding yeartodefinehigh-riskareasinthecurrentyear.
Withregardtoexclusionowingtopriorhistoryofmalaria, onlyoneBBdidnotapplyanyofthecriteriaestablishedbythe regulationandthreeappliedalltherequiredcriteria(Table5). Nine BBs applied the criterion ‘hadmalaria in the last 12 months’,sevenappliedthecriterion‘feverinthelast30days’ andthreeappliedthecriterion‘suspectedmalariainthelast 30days’.TwoBBsusedtheselasttwocriteriaconsideringa periodof15daysratherthan30.Othercriteriamentionedwere ‘havingtaken(ortaking)medicationformalaria’(2BBs)and ‘someoneathomehasgotmalaria’(2BBs).
AnalysisofthescreeningformshowedthatonlyoneBB usedaformcontainingthethreeexclusioncriteriaforprior historyofmalaria,whilsttwoBBshadnoquestionforthese criteria(Table5).Considerablevariationswereobservedinthe questionsonthescreeningformsregardinghavingtraveled toandlivinginhigh-riskareas,namely:(1)‘Haveyou been in ahigh malaria riskarea?’; (2) ‘Have you been ina high malariariskarea?Where?Howlongago?’;(3)‘Haveyou trav-eledtoadifferentmunicipalitywithinthestate?Whenand whichone?’;(4)‘Haveyoutraveledanywhereinthelastsix months?Ifyes,where?’;(5)‘Doyoucomefromanendemic malaria zone?’; (6) ‘Have you been inan endemic malaria regioninthelast30days?’;(7)‘Doyouliveinahighmalaria riskarea?’;and(8)‘Doyouliveinahighmalariariskarea? Where? For how long?’. Withthe exception ofquestions 3 and 4, it is possibletointerpret that the responsibilityfor indicatingexposuretomalariariskareaswasplacedonthe donor.
In relationtolaboratory screeningformalaria, four BBs wereclassifiedaspartiallyadequateandsevenasinadequate
(Table4).OnlysixBBsperformedlaboratoryscreeningonall
donations in accordance withthe regulation requirements
(Table5).TwoBBsonlytesteddonorsexposedtoareaswith
APIbetween10.0and49.9casesper1000inhabitants(medium risk)andafurthertwodidnotperformanytestatall,arguing thattheywerenotintheendemicarea.SevenBBsusedthick smearsinlaboratoryscreeningandoneused immunochro-matographictesting.WithregardtoSOPsfortheperformance oflaboratorytests(thickbloodsmearor immunochromato-graphic tests), two BBs were considered to have adequate instructions.Oneofthemperformedthickbloodsmeartesting andtheinstructionsadequatelystatedthat200fieldsshould beevaluatedbeforeestablishinganegativeresult.17
WhenconsideringtheeightBBsthatperformedsometype of laboratory test for malaria (whether or not it complied adequatelywiththeregulations),sixreportednothaving iden-tified anypositive testsinthe lastfive years.Furthermore, only oneBB reported havinga malariatest External Qual-ityEvaluationProgram(EQE)(Table5).Ontheotherhand,all the participatingBBs hadEQEfortheremaininglaboratory screeningtestsandforimmunohematology.
Table2–Detailsofthecriteriaassessedforeachbloodbanksectorandactivity,theirscoresandtheRDC153/2004item usedasabasisfortherequirement.
Sector/activity Itemevaluated Score RDC153/2004item
Donoreducation Provideeducationalmaterialstodonorscontaining informationabouttransfusion-transmittedmalaria.
10.0 B.4
Clinicalscreening
Interviewthedonorindividuallyinaprivateplace. 1.0 B.2andB.5 Havestandardsoperationalproceduresforclinical
screeningofdonorscontainingmalariaexclusion criteria.
1.0 A.11,B.5.2.6.2andP.1
Usethecriterionoftraveltoriskareatoreject donations,i.e.rejectcandidatescomingfromhigh malariariskareasasperAPI.
1.0 B.5.2.6.2
Usethecriterionoflivinginariskareatoreject donations,i.e.rejectcandidateslivinginhigh-riskareas asperAPI.
1.0 B.5.2.6.2
Usethecriterionofpriorhistoryofmalariatoreject donations,i.e.:(a)Rejectcandidateswhohavehad malariainthe12monthspriortodonation;(b)Reject candidateswhohavehadfeverinthelast30days;(c) Rejectcandidateswhohavehadsuspectedmalariain thelast30days.
None=0 1–2=0.5 3=1.0
B.5.2.6.2
Haveatrainingprogramthathasclinicalscreeningfor malariaaspartofitscontents.
1.0 P.2
Useastandardizedscreeningform(questionnaire)that assessestraveltoriskareas.
1.0 A.12,B.5.2.6.2andB.6.4
Useastandardizedscreeningform(questionnaire)that assesseslivinginariskarea.
1.0 A.12,B.5.2.6.2andB.6.4
Useastandardizedscreeningform(questionnaire)that assessespriorhistoryofmalaria.
–malaria12monthspriortodonation; –feverinthelast30days;
–suspectedmalariainthelast30days.
None=0 1–2=0.5 3=1.0
A.12,B.5.2.6.2andB.6.4
Existenceofawarningmechanismcapableof
preventingdonationbydonorwhoisineligibleowingto riskofmalaria,asperthecriteriausedbytheblood bank.
1.0 N.3andN.6.f
Laboratoryscreening
Performlaboratoryscreeningonalldonors,asrequired byRDC153,i.e.performparasitetestingonalldonors livinginorwhohavetraveledtoareaswithmediumor lowAPI,i.e.API<50.
4.0 B.5.2.6.2
Havewrittenproceduresfortestperformancein accordancewiththefollowingreferences: –Thicksmear:asperMinistryofHealthMalaria DiagnosisManual.
–Immunoenzymatictest:asperthemanufacturer’s instructions.
2.0 A.11andP.1
Havingatrainingprogramontheperformanceof laboratorytests.
1.0 P.2
Havewrittenproceduresfortestperformancein accordancewiththefollowingreferences:
–Thicksmear:theMinistryofHealthMalariaDiagnosis Manualrecommendsthatanegativeresultbegiven afteratleast200fieldshavebeenevaluated. –Immunoenzymatictest:asperthemanufacturer’s instructions.
2.0 A.11andP.1
HaveanExternalQualityEvaluationprogramfor malariatesting.
1.0 A.14
Hemovigilance Haveprocedurestodetectdonorswhohavesuspected orconfirmedmalariafollowingdonation.
5.0 A.10
Haveprocedurestodetectrecipientssuspectedof havingmalariatransmittedbybloodproductsproduced bytheservice.
5.0 A.11andA.17
Table3–Theidealmodelofbestpracticestoensuremaximumreductionoftransfusion-transmittedmalariarisk accordingtoRDC153/2004.
Bloodbanksinmalariaendemicareas Activitiestopreventtransfusion-transmittedmalaria
Education Clinicalscreening Laboratoryscreening Surveillance
Structures
Professionalstrainedand educationalmaterialavailableto clearlyinformdonorsoftherisk tobloodrecipientsbecoming infectedwithmalariathrough transfusions
Professionalstrainedand materialavailableto evaluatetheriskofdonors beinginfectedwith Plasmodium(written instructions,up-to-dateAPI chart,standardizedforms)
Professionalstrainedand materialavailableto performlaboratorytests (adequatealgorithms, writteninstructions, externalqualityevaluation, standardizedforms)
Professionalstrainedand materialavailableto identifyandinvestigate suspectedTTMcasesand detectsuspectedmalaria casesfollowingdonation (casedefinition, standardizedforms, flowcharts)
Processes
Donorsreceiveeducational materialsandguidanceontheir contents
Donorsadequately assessedregarding:(a) TravelingtoareaswithAPI >49;(b)Livinginareaswith API>49;(c)Priorhistoryof malaria
Alldonorsnotexcluded duringclinicalscreening havebloodsampletested forthepresenceofthe3 Plasmodiumspecies prevalentinBrazil,asper writteninstructions
AllsuspectedTTMcases areinvestigatedadequately
Bloodbanksareinformed ofanydonorssuspectedof havingmalariafollowing donation
Intermediateresults
Donorsunderstandtherisksand aresufficientlyawaretobeableto answerclinicalscreeningquestions adequatelyandhonestlyandare proactiveinprovidinginformation
Donorsatincreasedrisk accordingtothe establishedcriteriaare preventedfromdonating
Plasmodium-infected donorsareidentifiedand thebloodproductsare discarded
TTMinvestigationis completedandpositive casesatetreated
Donorsareinformedof theirtestresultsand referredforadoctor’s appointment
Donorssuspectedofhaving malariafollowingdonation aredetectedandblood productsarediscarded
Finalresults
Maximumreductioninthe numberofcontaminatedblood productsavailablefor therapeuticuse
Maximumreductioninthe numberofTTMcases
NoTTMrelatedmortality amongrecipients
TTM:transfusion-transmittedmalaria;API:annualparasiteindex.
Table4–Finalscoreobtainedbyeachsector/activityandclassificationofthetenbloodbanksaccordingtothecriteria establishedinthisevaluation.
Sector/activity Weightedscoresforbloodbanks Median
A B C D E F G H I J
Education 0.0 5.0 0.0 0.0 0.0 0.0 0.0 5.0 0.0 0.0 0.0
Classification I A I I I I I A I I
Clinicalscreening 28.0 26.0 24.0 20.0 16.0 26.0 32.0 32.0 16.0 30.0 26.0
Classification PA PA PA I I PA I PA I PA
Laboratoryscreening 20.0 32.0 0.0 28.0 28.0 28.0 8.0 20.0 0.0 8.0 20.0
Classification I PA I PA PA PA I I I I
Hemovigilance 0.0 15.0 0.0 0.0 7.5 0.0 0.0 0.0 0.0 7.5 0.0
Classification I A I I PA I I I I PA
Maximumscore 100 100 100 100 100 100 100 100 100 88.0a –
Scoreobtained 48.0 78.0 24.0 48.0 51.5 54.0 40.0 57.0 16.0 51.7 49.8
Finalclassification I PA I I PA PA I PA I PA
I:inadequate;PA:partiallyadequate;A:adequate.
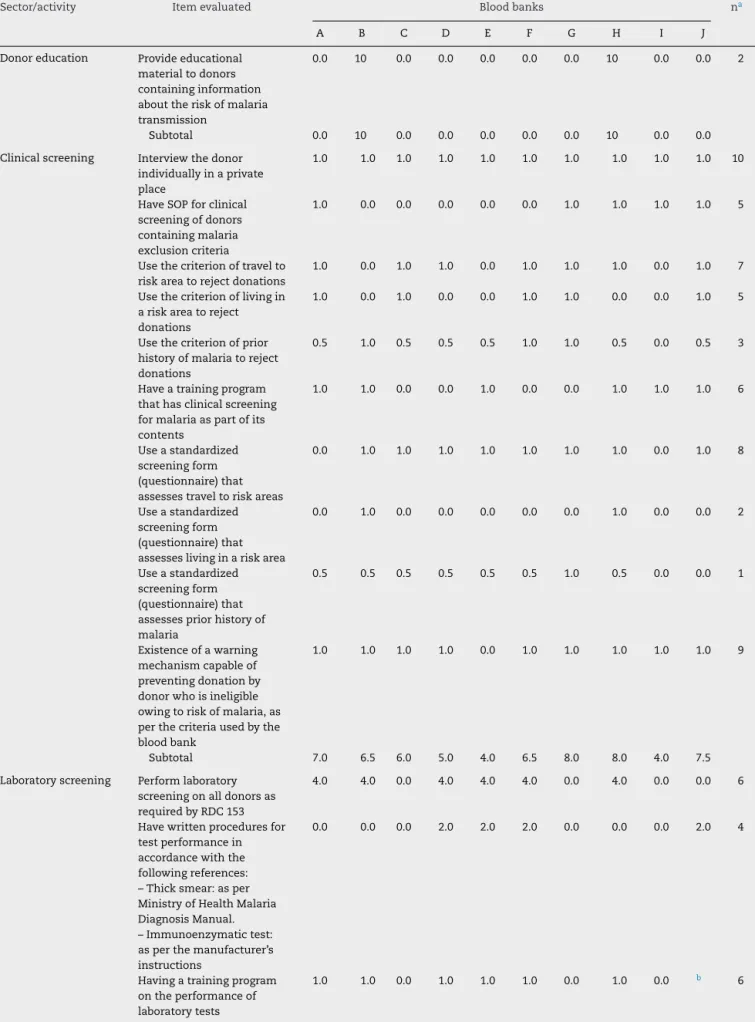
Table5–Scoresobtainedforeachitemevaluatedatthetenbloodbanksstudied(A–J)intheBrazilianAmazonregion.
Sector/activity Itemevaluated Bloodbanks na
A B C D E F G H I J
Donoreducation Provideeducational materialtodonors containinginformation abouttheriskofmalaria transmission
0.0 10 0.0 0.0 0.0 0.0 0.0 10 0.0 0.0 2
Subtotal 0.0 10 0.0 0.0 0.0 0.0 0.0 10 0.0 0.0
Clinicalscreening Interviewthedonor individuallyinaprivate place
1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 10
HaveSOPforclinical screeningofdonors containingmalaria exclusioncriteria
1.0 0.0 0.0 0.0 0.0 0.0 1.0 1.0 1.0 1.0 5
Usethecriterionoftravelto riskareatorejectdonations
1.0 0.0 1.0 1.0 0.0 1.0 1.0 1.0 0.0 1.0 7
Usethecriterionoflivingin ariskareatoreject donations
1.0 0.0 1.0 0.0 0.0 1.0 1.0 0.0 0.0 1.0 5
Usethecriterionofprior historyofmalariatoreject donations
0.5 1.0 0.5 0.5 0.5 1.0 1.0 0.5 0.0 0.5 3
Haveatrainingprogram thathasclinicalscreening formalariaaspartofits contents
1.0 1.0 0.0 0.0 1.0 0.0 0.0 1.0 1.0 1.0 6
Useastandardized screeningform (questionnaire)that assessestraveltoriskareas
0.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 0.0 1.0 8
Useastandardized screeningform (questionnaire)that assesseslivinginariskarea
0.0 1.0 0.0 0.0 0.0 0.0 0.0 1.0 0.0 0.0 2
Useastandardized screeningform (questionnaire)that assessespriorhistoryof malaria
0.5 0.5 0.5 0.5 0.5 0.5 1.0 0.5 0.0 0.0 1
Existenceofawarning mechanismcapableof preventingdonationby donorwhoisineligible owingtoriskofmalaria,as perthecriteriausedbythe bloodbank
1.0 1.0 1.0 1.0 0.0 1.0 1.0 1.0 1.0 1.0 9
Subtotal 7.0 6.5 6.0 5.0 4.0 6.5 8.0 8.0 4.0 7.5
Laboratoryscreening Performlaboratory screeningonalldonorsas requiredbyRDC153
4.0 4.0 0.0 4.0 4.0 4.0 0.0 4.0 0.0 0.0 6
Havewrittenproceduresfor testperformancein accordancewiththe followingreferences: –Thicksmear:asper MinistryofHealthMalaria DiagnosisManual. –Immunoenzymatictest: asperthemanufacturer’s instructions
0.0 0.0 0.0 2.0 2.0 2.0 0.0 0.0 0.0 2.0 4
Havingatrainingprogram ontheperformanceof laboratorytests
Table5–(Continued)
Sector/activity Itemevaluated Bloodbanks na
A B C D E F G H I J
Havewrittenproceduresto testperformancein accordancewiththe followingreferences: –Thicksmear:theMinistry ofHealthMalariaDiagnosis Manualrecommendsthata negativeresultbegiven afteratleast200fieldshave beenevaluated
–Immunoenzymatictest: asperthemanufacturer’s instructions
0.0 2.0 0.0 0.0 0.0 0.0 2.0 0.0 0.0 b 2
HaveanExternalQuality Controlprogram (Proficiency)formalaria testing
0.0 1.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 1
Subtotal 5.0 8.0 0.0 7.0 7.0 7.0 2.0 5.0 0.0 2.0
Hemovigilance Haveprocedurestodetect donorswhohavesuspected orconfirmedmalaria followingdonation
0.0 5.0 0.0 0.0 5.0 0.0 0.0 0.0 0.0 0.0 2
Haveprocedurestodetect recipientssuspectedof havingmalariatransmitted bybloodproductsproduced bytheservice
0.0 5.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 5.0 2
Subtotal 0.0 10 0.0 0.0 5.0 0.0 0.0 0.0 0.0 5.0
a Numberofbloodbanksadequatelycomplyingwiththeitem.
b Notevaluatedbecausetheseareoutsourcedactivities.
TwoBBsreportedhavingdetectedcasesofTTMresulting frombloodproductsproducedbythem.Allthesecasesdied.
Discussion
PublicationsabouttheevaluationofBrazilianBBsarerareand, whentheyarefound,theirthemesaredonorsatisfaction,18 serological test performance19 or costs.20 This is the first Brazilianstudytoevaluatethequalityoftheproceduresand methodsusedbyBBstopreventTTM.
Overallperformanceregistered bythe study showsthat adherencetoRDC153/2004withregardtothepreventionof TTMisneglectedbytheparticipatingBBs.Onlyone establish-mentobtainedmorethan60pointsontheproposedscoring system.
Donor education is an important factor for reducing serological ineligibility and disease transmission through transfusions.21 Althoughthe participatingBBsusedleaflets asaninitiativeaimedatdonoreducation,mostoftheleaflets madenoreferencetoTTM. Thisstrengthenstheargument thatmalariaisusuallyneglectedasariskforpatients. More-over, the effectivenessof using leaflets to educate donors appearstobeminimal. Onestudyshowedthateducational leafletshadalimitedeffecttoreduceserologicalineligibility
owing to HIV when used in isolation.22 Other educational approachesthereforeneedtobeencouraged.
Clinicalscreeningwasalsoidentifiedasaweakpoint.This stageisthefirststepinensuringsafeblood andshouldbe performedbytrainedandcompetentpersonnel,usinga pre-defined,validatedandstandardizedquestionnaire.23Clinical screeningisevenmoreimportantforpreventingTTMasthe sensitivityofthelaboratoryscreeningtestsusedisnothigh.24 Thevariationinthequestionsfoundinthescreening ques-tionnairesshowsthatthereisnostandardizationamongthe participatingBBstoassessdonorsinrelationtomalaria. Stud-ies tovalidate questions posed to donorswith the aimof preventingTTMneedtobeconducted.
clinicalscreeningcanbeperformedbasedoncurrent infor-mationandnotoninformationfromthepreviousyear,aswas thecasewiththeBBsinthisstudy.
Laboratoryscreeningformalariarevealedrelevant short-comings,suchasnottestingalldonors,theabsenceofEQE formalariatestsand,inthecaseofthethickbloodsmeartest, aninsufficientnumberoffieldswereinspected(lessthan200) toconcludethattheslideswerefreeofPlasmodium.
Thethickbloodsmeartesthaslimitedsensitivitytodetect asymptomatic infections with low parasitemia.24 It must thereforebeusedwithgreatcautionsoastoreducefalse neg-ativeresultsasfaraspossible.Since2001theMoHhasoffered afreeEQEprogramforpublicBBsthatincludesserologicaland immunohematologicaltests.However,malariahasneverbeen includedinthisprogramanditsinclusionwithregardtothick bloodsmeartestinghasshowntoberelevant.
ScreeningformalariainBBsisaworldwidechallenge.In non-endemiccountries,ingeneral,theoptionismadeto tem-porarilyexcludedonorswhohavetraveledtoendemicregions and laboratory teststo directly detect the parasiteare not performed. Inendemiccountries consensusdoes notexist as to best practices to prevent TTM. Some countries with endemicareas, suchas Colombia26 and Ethiopia,27 do not uselaboratoryscreeningandundertakeriskassessmentand selectionbasedexclusivelyontheepidemiological question-naire.InTurkey,28selectionisdoneviaaquestionnaireand, ifdonorsarefoundtobeineligible,serologicalandmolecular testscanbeusedtoreducetheperiodofineligibility,as rec-ommendedbyEuropeanguidelines.Assuch,werecommend anevaluationas tothe possibility ofmunicipals or micro-regionswherenativecasesofmalariahavenotberecorded foralongtimeusingthesameselectioncriteriaasmunicipals innon-endemicareas.Thischangewouldreducethecostsof laboratoryscreeningformalaria,althoughtheremightbea possibleincreaseinclinicalineligibility.
Consideringthelimitationsofthicksmearsasascreening testinBBs,togetherwiththepossibilityofreducingthe num-berofBBsobligedtoperformlaboratoryscreeningformalaria, we suggest that the cost effectiveness of implanting NAT forPlasmodiumspeciesinBBsinendemicmunicipalitiesor micro-regionsshouldbeevaluated.
Theweaknessesfoundintheprocessofselectingand iden-tifyingdonors atriskofTTM indicatethe importanceof a sensitiveandstructuredhemovigilancesystem.Itis impor-tantthatdonorsletBBsknowiftheyhaveacquiredmalaria oraresuspectedofhavingmalariaafterdonation.Whether ornotdonorstakethisinitiativedependsonthemknowing thatmalaria can betransmittedthrough transfusions,and oneffectivecommunicationchannelswithBBs.Theinclusion onthe SIVEP-Malarianotificationformofaquestion ‘Have you donated blood in the last 30 days?’, and an informa-tionflowbetweenthenotifyingunitandBBs,couldidentify donationsmadeduringthediseaseincubationperiod,thereby reducingTTMcasesorenablingtimelyTTMidentificationand treatment,reducingitslethality.Nevertheless,asymptomatic donorswhohavemalariacontinuetobeachallengeforBBs andhemovigilancehasbecomeanessentialmainstayforearly TTMcaseidentification.
Thisstudy hassomemethodological limitations worthy of mention. The study’s design is cross-sectional and the
situation analyzedmayhavechangedfollowingit,possibly asaconsequenceoftheinterventionusedforthisthestudy. Moreover,theevaluationusedaregulationthatwasrevoked duringthecourseofthestudy.Nevertheless,thealterations contained inthe new regulations(ANVISA Resolution RDC 57/2010 and MoHOrdinance2712/2013) were minimalwith regardtoscreeningdonorsformalariainendemicareas,such as(i)municipalitieswheredonorsliveorhavetraveledwas definedastheAPIassessmentarea,(ii)definitionof ineligi-bilityperiodsincasesofhavingtraveledtohigh-risk areas and(iii)permissiontouselaboratoryteststhatdetect Plas-modiumantigens.Thesealterationsdonotalterthescores and theclassificationsobtainedinthis study.Moreover,all information received was self-reported and the answers wereconfirmed,wheneverpossible,bydocuments.However, asit wasanexternalevaluation,despitethe peoplelegally responsible forthe establishmentsagreeingtotake partin thestudy,attimesaccesswasnotauthorizedtoSOPsand, in thesecases, measureswere notadopted toconfirm the answersviaadifferentmeansofverification.Thissituation was rare however (2 cases). As a general rule, the person in charge of the sector was consulted in order to obtain morepreciseanswers regardingthe practiceinquestion.If this person was notavailable, then the person technically responsible fortheBBanswered thequestionnaire(1case). Assuch,verificationerrorsmayhaveoccurredinsomecases. With regard to the scores, we emphasize that the weight usedforeachquestionwasdecidedbytheresearchersbased on arbitrarycriteriaastotherelevance ofthe questionfor thepotentialriskofTTMoccurrence.Otherscoringsystems could have generated different final classification results. Nevertheless,thevalidationofsuchscoringandclassification systemsislimitedbythesmallnumberofevents.
Despitetheselimitations,theresultsofthelogical frame-workproposedareconsideredtohavemettheobjectivesof evaluating BBstructureand processesand canbeusedfor internalevaluationsandcorrectionofactivities.Theycanalso beusedbyVISAinsupportofitsactions,inparticular inspec-tions.
Finally,underliningtherelevanceofthissubject,itshould benotedthatin2004theWorldHealthOrganizationlaunched the Global Patient SafetyChallenge, which includes‘blood safety’asoneofitspillars.Assuch,programsarerequired tobeimplantedthatensureaccessibilityofhighqualityand safebloodtoallthosewhoreallyneedit.29Donorselection andhemovigilancearekeyelements ofthisprocess. Trans-missionofanydiseaserepresentsafailureandbestpractices mustbeadoptedsothatpatientsarenotharmedbyblood. ThisincludestakingcaretoensurethepreventionofTTM.
Conclusion
with,inparticularthe preparationofandcompliance with SOPsforclinicalandlaboratoryscreeningofmalaria,the inclu-sionofmalariadetectionEQEandtheimplementationofthe hemovigilancesystem.Inaddition,webelievethatthese reg-ulations,evenafterthe2010and2013revisions,canbefurther improved.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Tothe Conselho Nacionalde Desenvolvimento Científico e Tecnológico(CNPq)andAgênciaNacionaldeVigilância San-itária(ANVISA),fromBrazil,forfundingthisstudy,aswellas tothebloodbankstakingpartinthestudyforallowingaccess todonordataandfacilities.
r
e
f
e
r
e
n
c
e
s
1. MungaiM,TegtmeierG,ChamberlandM,PariseM.
Transfusion-transmittedmalariaintheUnitedStatesfrom
1963through1999.NEnglJMed.2001;344(26):1973–8.
2. PurdyE,PerryE,GorlinJ,JensenK.Transfusion-transmitted
malaria:unpreventablebycurrentdonorexclusion
guidelines?[Letter].Transfusion.2004;44(3):464.
3. FreitasDR,SimõesBJ,AraújoWN.Avaliac¸ãodoSistema
NacionaldeHemovigilânciadosanosde2002a2005.Cad
SaúdeColet(RioJ).2010;18(1):179–89.
4. Batista-dos-SantosS,RaiolM,SantosS,CunhaMG,
Ribeiro-dos-SantosA.Real-timePCRdiagnosisofPlasmodium
vivaxamongblooddonors.MalarJ.2012;11:345.
5. FugikahaE,FornazariPA,PenhalbelRS,LorenzettiA,Maroso
RD,AmorasJT,etal.MolecularscreeningofPlasmodiumsp.
asymptomaticcarriersamongtransfusioncentersfrom
BrazilianAmazonregion.RevInstMedTropSaoPaulo.
2007;49(1):1–4.
6. TorresKL,FigueiredoDV,ZalisMG,Daniel-RibeiroCT,Alecrim
W,Ferreira-da-CruzMF.Standardizationofaveryspecificand
sensitivesinglePCRfordetectionofPlasmodiumvivaxinlow
parasitizedindividualsanditsusefulnessforscreeningblood
donors.ParasitolRes.2006;98(6):519–24.
7. MotaDM,FreitasDR,AraújoWN.EvaluationoftheSystemof
SanitaryVigilanceofBloodatthefederallevelBrazil,2007.
CienSaudeColet.2012;17(1):191–202.
8. Brasil.LeiFederaln◦
7.649/1988.Estabeleceaobrigatoriedade docadastramentodosdoadoresdesanguebemcomoa realizac¸ãodeexameslaboratoriaisnosanguecoletado, visandoaprevenirapropagac¸ãodedoenc¸as,edáoutras providências.DiárioOficialdaUnião1988;27January. 9. MinistériodaSaúde.PortariaGMn◦721/1989.DiárioOficialda
União1989;11ago.
10.AgênciaNacionaldeVigilânciaSanitária.Resoluc¸ãode DiretoriaColegiadan◦343/2002.DiárioOficialdaUnião2002;
13dez.
11.NovaesHM.Evaluationofhealthprograms,servicesand
technologies.RevSaudePublica.2000;34(5):547–9.
12.ContandriopoulosAP,ChampagneF,DenisJL,PineaultR. Avaliac¸ãonaáreadasaúde:conceitosemétodos.In:Hartz ZMA(org.),Avaliac¸ãoemSaúde:dosModelosconceituaisà práticanaanálisedaimplantac¸ãodeprogramas.Riode Janeiro:EditoraFiocruz;1997.p.29–47.
13.UchimuraKY,BosiML.Qualityandsubjectivityinthe
evaluationofhealthservicesandprograms.CadSaude
Publica.2002;18(6):1561–9.
14.AgênciaNacionaldeVigilânciaSanitária.Resoluc¸ãoda DiretoriaColegiadan◦
153/2004.DiárioOficialdaUnião2004; 14June.
15.DonabedianA.Thequalityofcare.Howcanitbeassessed?
JAMA.1988;260(12):1743–8.
16.LeiteHJ,NavarroMV.Riscopotencial:umconceitoderisco operativoparavigilânciasanitária.In:CostaEA(org.), VigilânciaSanitária:temasparadebate[online].Salvador: EDUFBA;2009.237.p.61–68.
17.SecretariadeVigilânciaemSaúde.Manualdediagnóstico
laboratorialdamalária.Brasília:MinistériodaSaúde;
1999.
18.DiColliL,BassiLL,OmottoCA,RehmeLH,MatsuoT.Opapel
dousuárionaorganizac¸ãodosetordecoletadesanguedo
HemonúcleodeApucarana,Paraná,Brasil.RevBrasHematol
Hemoter.2009;31(2):98–103.
19.Saéz-AlquézarA,OtaniMM,SabinoEC,Ribeiro-dos-SantosG,
SallesN,ChamoneDF.Evaluationoftheperformanceof
BrazilianbloodbanksintestingforChagas’disease.Vox
Sang.1998;74(4):228–31.
20.UbialiEM,SampaioDA,PinhoPF,CovasDT.Customédiodo
MódulodeColetadesanguetotalpelométodoABC.RevBras
HematolHemoter.2008;30(3):213–7.
21.RamezaniH,BozorgiSH,NooranipourM,SadriM,
MolaverdikhaniS,AlavianSM.Successfulexclusionof
blood–borneviraldiseaseinblooddonors.EurJInternMed.
2011;22(6):e71–4.
22.Gonc¸alezTT,SabinoEC,SallesNA,Almeida-NetoC,
Mendrone-JrA,Dorlhiac-LaccerPE,etal.Theimpactof
simpledonoreducationondonorbehavioraldeferraland
infectiousdiseaseratesinSãoPaulo,Brazil.Transfusion.
2010;50(4):909–17.
23.OrtonSL,VirvosVJ,WilliamsAE.Validationofselected
donor-screeningquestions:structure,content,and
comprehension.Transfusion(Paris).2000;40(11):1407–13.
24.GrandeR,PetriniG,SilvaniI,SimoneschiB,MarconiM,
TorresaniE.Immunologicaltestingformalariaandblood
donordeferral:theexperienceoftheCa’GrandaPolyclinic
HospitalinMilan.BloodTransfus.2011;9(2):162–6.
25.KiesslichD,AraújoMA,YurtseverSV,TorresK.Controleda
maláriapós-transfusionalnaAmazôniaBrasileira:proposta
demodificac¸ãodasnormastécnicas.InformeEpidemiolSUS.
1999;8(2):53–7.
26.CastilloC,RamírezC.Tamizacióndemaláriaendonantes
sangredeCali,Colombia.Biomédica.2005;25(2):203–10.
27.GelawB,MengistuY.TheprevalenceofHBV,HCVandmalaria
parasitesamongblooddonorsinAmharaandTigrayregional
states.EthiopJHealthDev.2007;22(1):3–7.
28.De ˘girmenciA,Dös¸kayaM,CanerA,NergisS,GülK,Aydınok
Y,etal.Actionplantoregainunnecessarydeferredblood
donorsduetomalariariskinTurkey.TransfusApherSci.
2012;46(3):269–75.
29.PittetD,DonaldsonL.Cleancareissafercare:thefirstglobal
challengeoftheWHOWorldAllianceforPatientSafety