Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
w w w . r b h h . o r g
Original
article
Nutritional
status
of
patients
submitted
to
transplantation
of
allogeneic
hematopoietic
stem
cells:
a
retrospective
study
Érika
Elias
Ferreira
a,
Daiane
Cristina
Guerra
a,∗,
Kátia
Baluz
a,
Wander
de
Resende
Furtado
b,
Luis
Fernando
da
Silva
Bouzas
a aInstitutoNacionaldeCâncerJoséAlencarGomesdaSilva(INCA),RiodeJaneiro,RJ,BrazilbFaculdadedeMedicinadeRibeirãoPreto(FMRP),UniversidadedeSãoPaulo(USP),RibeirãoPreto,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received7May2014 Accepted8June2014 Availableonline18July2014
Keywords:
Hematopoieticstemcell transplantation Nutritionalstatus Nutritionaltherapy
a
b
s
t
r
a
c
t
Objective:Thisstudyaimedtodescribeandcomparethenutritionalstatusofadultpatients submittedtoallogeneichematopoieticstemcelltransplantationattwodifferenttimepoints (admissionanddischarge).
Methods:Aretrospective,descriptiveandquantitativestudywasperformedbasedon clini-cal,laboratoryandnutritionaldataobtainedfrommedicalrecordsofadultpatientsofboth genderssubmittedtoallogeneichematopoieticstemcelltransplantationinabonemarrow transplantationreferencecenterinRiodeJaneirointheperiodfrom2010to2013.Statistical analysiswasperformedusingtheSPSSsoftware(version22.0).
Results:Sixty-fourpatientswereevaluated.The mean agewas42.1±3.2years andthe mostprevalentdiseasewasacutemyeloidleukemia(39%).Therewasahighprevalence ofgastrointestinalsymptomsincludingnausea(100%),vomiting(97%)andmucositis(93%). Betweenadmissionanddischargetherewasasignificantdecreaseinthemedianweight (−2.5kg;71.5vs.68.75kg;p-value<0.001),bodymassindex(−0.9kg/m2;24.8vs.24.4kg/m2; p-value<0.001),andserumalbuminlevels(−0.2g/dL;3.7vs.3.6g/dL;p-value=0.024).The survivaltimeafterhematopoieticstemcelltransplantationcorrelatednegativelywith C-reactiveproteinatdischarge(CC=−0.72;p-value<0.001)andpositivelywithserumalbumin levels(CC=0.56;p-value=0.004)andwithhightotalproteinlevelatdischarge(CC=0.53;
p-value=0.006).
Conclusion:Ourresultssuggestthatpatientssubmittedtoallogeneichematopoieticstem celltransplantationhavecompromisednutritionalstatusduringthehospitalstayfor trans-plantation.
©2014Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthorat:CentrodeTransplantedeMedulaÓssea(CEMO),InstitutoNacionaldeCâncerJoséAlencarGomesdaSilva
(INCA),Prac¸aCruzVermelha,23,7◦andar,Centro,20230-130RiodeJaneiro,RJ,Brazil.
E-mailaddress:[email protected](D.C.Guerra).
http://dx.doi.org/10.1016/j.bjhh.2014.07.014
Introduction
Hematopoieticstem cell transplantation (HSCT)isa highly complex procedure indicated for the treatment of various diseases, including aggressive hematological, oncohemato-logical, and genetic diseases and autoimmune disorders. HSCTinvolvesanintravenousinfusionofhematopoieticstem cells(HSC)usedtorestorebonemarrowfunction.Allogeneic HSCTuseshematopoieticstemcells(HSC)eitherfromrelated orunrelateddonors.1,2
Theconditioningregimenisintendedtoeradicate resid-ualdiseaseofthepatientand,inthecaseofallogeneicHSCT, toinduceimmunosuppressiontoallowengraftment ofthe infusedHSC.3,4
Theaggressiveconditioning regimenusedforallogeneic HSCTmaycombinechemotherapywithtotalbodyirradiation (TBI).Alargenumberofclinicalcomplicationsisassociated withthistypeoftransplantation;themorbidityandmortality aremainlyassociatedtoopportunisticinfections,graftversus hostdisease (GVHD),organfailure,graft failureorrejection andrelapseoftheunderlyingdisease.5,6
Patients submitted to allogeneic HSCT should be con-sideredatnutritional risk7–9 dueto reducedenergyintake,
impaired absorption of nutrients and increased metabolic demands.10
TheadverseeffectsofchemotherapyandTBIaffect,in par-ticular,thegastrointestinal(GI)tractandtheimmunesystem.7
Accordingly,inadditiontosymptomsofnauseaand vomi-ting,severemucositisassociatedwithintenseodynophagia, abdominalpainanddiarrheaoftenoccurs.11,12 GI
complica-tionsoftheconditioningregimenmaylastforupto21days aftertransplantation.8,10
HSC transplant patients are likely to develop a series of metabolic disorders of varying severity, mostly during theimmediatepost-transplantperiod.Themaincausesare the adverse effects of the conditioning regimenitself, the immunosuppressivedrugs (tocontrolor forprophylaxis of GVHD)and thetotalparenteralnutrition(TPN),whichmay increasetheriskofopportunisticinfectionsandinflammatory processes.13
GVHDisoneofthemostimportantclinicalcomplications relatedtoallogeneicHSCT.Itisrelatedtoanimmuneresponse triggeredbythedonorHSCcellsagainstthehosttissueswhich usuallyinvolvesthe liver,skinandtheGItract.Acute diar-rheainthepost-transplantperiodisusuallyassociatedwith infectionsandGVHD.8,12,14
Thepresentstudyaimedtocomparethenutritionalstatus ofadultallogeneicHSCTpatientsattwodifferenttimepoints (hospitaladmissionand discharge)and describethe preva-lenceofGIsymptoms,theoccurrenceofGVHDanddeathsup to100daysaftertransplantation(D+100).
Methods
Studydesignandpopulation
Thiswasaretrospective,descriptive andquantitativestudy based onclinical, and laboratorydata and a reviewofthe nutritional status of patients treated in a bone marrow
transplantation referralcenter inthe cityofRiodeJaneiro, Brazil.DatawereobtainedfrommedicalrecordsfromAugust 2010toMay2013.
Patientsaged18andolder,ofbothgenders,with neoplas-ticornon-neoplasticdiseasessubmittedtoallogeneicHSCT (relatedorunrelated)wereincludedinthestudy.Patientswith previous historyofHSCTandthose whosemedicalrecords wereunavailablewereexcludedfromthestudy.
Ofthe76patientswhounderwentallogeneicHSCTduring thestudyperiod,twelvewereexcludedfromthestudy,seven duetopriorHSCTandfiveduetothelackofmedicalrecords. Thusthestudysampleconsistedof64patients.
Anthropometricparametersandlaboratorydatacollected arefortwodifferenttimepoints,admissiontotheinpatient unitfortransplantation(T1)andunitdischarge(T2).Clinical parameterswerecollectedfromadmissionuntil100daysafter transplant(D+100).DataonthefoodintakeandGIsymptoms refertothehospitalizationperiod.
ThestudywasapprovedbytheEthicsCommitteeofthe bonemarrowtransplantationreferralcenter.
The following clinical data were investigated:diagnosis oftheunderlyingdisease,comorbidities,typeoftransplant (relatedorunrelated),sourceofHSC(bonemarrow,peripheral bloodorumbilicalcordblood),conditioningregimen,length ofhospitalization,timetoengraftment,GIsymptoms,useof enteralnutrition(EN)andTPN,occurrenceofGVHDanddeath. Dataonage,gender,education,ethnicityandlifestyle (smok-inganddrinking)werealsocollected.
Laboratorytestsincludedbloodsugar,albumin,creatinine, hemoglobin, hematocrit, potassium, phosphorus, magne-sium,total bilirubin,direct bilirubinand C-reactiveprotein (CRP)levels.
Moreover, anthropometric evaluations consisted of the following indicators: current weight, usual weight, height, percentageofweightlossandBMI.Nutritionalstatuswas clas-sifiedaccordingtotheBMIas:severemalnutrition(<16kg/m2),
moderate malnutrition (16–16.9kg/m2), mild malnutrition
(17–18.49kg/m2),normalweight(18.5–24.9kg/m2),overweight
(25–29.9kg/m2), mildly obese (30–34.9kg/m2), moderately
obese (35–39.9kg/m2)or severelyobese(>39.9kg/m2).15 The
percentageofweightlosswascalculatedfrom thehospital dischargeweightandtheadmissionweight.
Thefoodintakewasclassifiedaslow(<60%),partial(from 60% to 99%) or full(100%) based onthe patient’s reported intakeonmedicalrecords.Theclassificationusedistheone standardizedbytheDepartmentofNutritionandDieteticsat theBoneMarrowTransplantationcenter.Nausea,vomiting, mucositis(GradesItoIV),odynophagia,hyporexia,diarrhea, amongotherGIsymptomsreportedbypatientsduring hospi-talizationwererecorded.
Statisticalanalysis
Wilcoxon signed-ranktest and theSign test wereused for non-parametricvariables.TheStatisticalProgramforSocial Sciences(SPSSversion22.0)wasusedforthestatistical anal-yses.Thelevelofsignificancewassetat5%forallstatistical tests.
Results
Socioeconomiccharacteristics
Themean ageofthepatientswas 42.1±3.2years,with8% ofelderly (>60 years), and the distribution between males andfemaleswasequal(50%).Thepercentageofsmokerswas 17.7%and12.9%consumedalcohol.Skincolorwas predomi-nantlywhite(46%)andbrown(46%)andintermsofschooling 31%ofpatientshadcompletedhighschooland28%had uni-versity degrees; there were no illiterate individuals in the sample.
Clinicalcharacteristicsofpatients
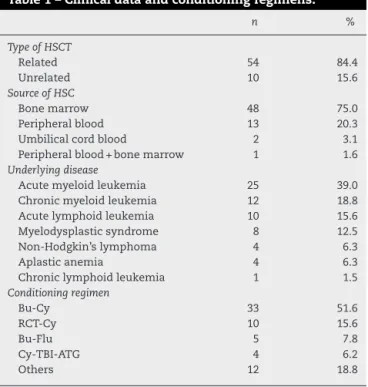
Fifty-fourpatients(84.4%)underwentrelatedandtenpatients (15.6%)unrelatedallogeneic HSCTwiththemainsourceof CTHbeingbonemarrow(75%).Themostcommon underly-ingdiseaseswereacutemyeloidleukemia(39%)andchronic myeloidleukemia(18.8%).Therewereprevalencesofdiabetes mellitus(6%)andhypertension(13%).
Themainconditioningregimensandotherclinicaldataare showninTable1.Themeanhospitalstaywas36±10days.The meantimetoengraftmentwas18.3±6.6days.Themortality
Table1–Clinicaldataandconditioningregimens.
n %
TypeofHSCT
Related 54 84.4
Unrelated 10 15.6
SourceofHSC
Bonemarrow 48 75.0
Peripheralblood 13 20.3 Umbilicalcordblood 2 3.1 Peripheralblood+bonemarrow 1 1.6
Underlyingdisease
Acutemyeloidleukemia 25 39.0 Chronicmyeloidleukemia 12 18.8 Acutelymphoidleukemia 10 15.6 Myelodysplasticsyndrome 8 12.5 Non-Hodgkin’slymphoma 4 6.3
Aplasticanemia 4 6.3
Chroniclymphoidleukemia 1 1.5
Conditioningregimen
Bu-Cy 33 51.6
RCT-Cy 10 15.6
Bu-Flu 5 7.8
Cy-TBI-ATG 4 6.2
Others 12 18.8
Bu:busulfan;Cy:cyclophosphamide;TBI:totalbodyirradiation;Flu: fludarabine;ATG:anti-thymocyteglobulin;Mel:melphalan;Others: Bu-Cy-ATG,Cy-ATG,Flu-Mel,Flu-Cy,Flu-ATG-Cy,Bu-Mel, Flu-Bu-ATG,Cy.
ratebyD+100was34.4%(22patients),with50%ofthedeaths occurringduringhospitalization.
Ofthe 64patientsevaluated, 34 (53%)hadGVHDbefore
D+100. Among the patients with GVHD, the distribution
according to the organ involved was: skin (88%), GI tract
(73.5%),liver(47%);11patients(32%)hadGVHDinthreeorgans (skin,gastrointestinaltractandliver).
Nutritionalassessment
On admission, thenutritional assessmentaccording tothe
BMIshowedthat29patientshadnormalweight(45.3%),23
wereoverweight(35.9%),eightmildlyobese(12.5%),two mod-erately obese (3.1%), one had mildmalnutrition (1.6%) and onehadmoderatemalnutrition(1.6%).Moreover,atthistime point, 10.4% of patients had suffered aweight loss>5%of usualweight.Atdischargetherewasafurtherweightloss>5% comparedtotheweightatadmissionin40.4%ofcases.
Comparingthenutritionalstatusofpatientsonadmission and atdischarge (T1 vs.T2) the Wilcoxonsigned-rank test showedthattherewasastatisticallysignificantdecreasein themedianweight(−2.5kg;71.5vs.68.75kg;p-value<0.001), BMI (−0.9kg/m2; 24.8 vs. 24.4kg/m2; p-value<0.001), and
serumalbuminlevel(−0.2g/dL;3.7vs.3.6g/dL;p-value=0.024) (Table2).
Theserumalbuminlevelatdischargewaspositively corre-latedwithsurvivaltimeafterHSCT(CC=0.56;p-value=0.004). The serum total protein level at discharge also showed a positivecorrelationwithsurvivaltimeafterHSCT(CC=0.53;p -value=0.006).Ontheotherhand,theC-reactiveproteinlevel atdischargeshowedastrongnegativecorrelationwith sur-vivaltimeafterHSCT(CC=−0.72;p-value<0.001).
Table3showsthecharacteristics offoodintakeand the percentageofdaysoforallyacceptedfood(low,partialorfull), fastingandTPNinrelationtothetotallengthof hospitaliza-tion.
ThedistributionofGIsymptomsreportedbypatients dur-inghospitalizationisshowninTable4.
Discussion
This study in addition to describingthe nutritional profile of allogeneic HSCT patients also compared the nutritional status ofpatientsatadmission and atdischarge. Impaired nutritionalstatusisconsideredanegativeprognosticfactor inhospitalizedpatientsandisassociatedwithadverseclinical consequences.7,10
Themeanlengthofhospitalizationobservedinthisstudy wassimilartothosepreviouslyreportedbyBechardetal.(38 days)16 and Sommacalet al. (39 days).17 The mediantime
toengraftmentinthecurrentstudywasalsosimilartothat observedbyBechardetal.(20days).
The mortalityrate up toD+100 inthis study was34%, higherthanthatobservedbyLeeetal.,13whoreported11.5%
ofdeathsuntil D+100in asampleof315 allogeneicHSCT patients.
Table2–ComparisonbetweenanthropometricandlaboratoryvariablesofpatientssubmittedtoallogeneicHSCTat admission(T1)andatdischarge(T2).
Median Mean±standarddeviation p-Value
n T1 T2 Mediandifference (T2−T1)
T1 T2
Currentweight(kg) 52 71.25 68.75 −2.5 70.50±12.78 68.27±11.82 0.000a
BMI(kg/m2) 52 24.80 24.40 −0.9 25.74±4.85 24.97±4.66 0.000a
Hemoglobin(g/dL) 48 10.80 9.55 −0.9 10.40±2.37 9.64±0.94 0.014b
Hematocrit(%) 48 32.95 28.40 −4.25 31.37±7.48 28.33±2.77 0.002a
Glycemia(mg/dL) 47 114.50 95.00 −13.5 147.92±122.83 125.94±91.85 0.041c
Albumin(g/dL) 47 3.70 3.60 −0.2 3.69±0.53 3.52±0.49 0.024a
Albumin/globulin 47 1.62 1.56 −0.15 1.70±0.46 1.54±0.36 0.005b
Totalbilirubin(mg/dL) 47 0.34 0.53 0.19 0.40±0.28 0.61±0.39 0.000a
Directbilirubin(mg/dL) 48 0.12 0.26 0.14 0.14±0.12 0.33±0.31 0.000a
Creatinine(mg/dL) 48 0.80 0.95 0.2 0.80±0.25 1.04±0.44 0.000a
Potassium(mg/dL) 48 4.10 4.50 0.4 4.10±0.40 4.41±0.61 0.005b
Phosphorus(mg/dL) 47 3.40 4.00 0.5 3.46±0.65 3.95±0.65 0.000a
Magnesium 48 2.30 1.70 −0.6 2.29±0.47 1.69±0.21 0.000a
CRP(mg/dL) 45 0.43 0.69 0.31 1.48±2.60 1.57±2.57 0.400a
T1:admission;T2:discharge;BMI:bodymassindex;CRP:C-reactiveprotein. a WilcoxonSigned-ranktest.
b Pairedt-test.
c Signtest.
immunosuppression,andalsorelatedtoGVHD.Inallogeneic HSCT,the serious sideeffects, including nausea, vomiting, mucositis,diarrheaandhyporexia,impairfoodintake;these sideeffectscanlastforuptofourweeksafterHSCT.18,19
ThefrequencyofacutetoxicityrelatedtoHSCT,inthis con-textrepresentedbyGIsymptoms,washighhoweverthehigh aggressivenessofallogeneictransplantation shouldbe con-sidered.Inthisstudy,over90%ofthesamplehadatleastthree symptomsofhighnutritionalimpact(nausea–100%,vomiting –96.6%,andmucositis–93.2%).Withregardtotheseverityof mucositis,36%ofpatientsdevelopedGradeIVmucositis,thus precludingtheuseoforalfeeding.
Dietaryintakewasaffectedgreatlyascanbeseenbythe high percentage of days of fasting (23.6±17.4%) and TPN (42.9±19.5%)andthelowacceptanceoffoodduringathird
Table3–Characterizationoffoodintakeindaysand percentageofhospitalstay.
Median Mean±SD Range
Lowintake(<60%)
n 11.0 11.9±6.9 1.0–28.0 % 34.6 33.2±17.7 4.3–77.0
Partialintake(60–99%)
n 12.0 13.5±7.08 1.0–36.0 % 35.7 37.6±19.9 2.1–76.9
Fullintake(100%)
n 4.0 4.8±3.6 1.0–19.0 % 10.7 13.6±8.9 3.1–38.8
Fasting
n 6.0 10.3±11.9 1.0–58.0 % 18.1 23.6±17.4 2.9–68.1
TPN
n 17.0 18.2±12.6 1.0–64.0 % 47.0 42.9±19.5 4.4–81.4
SD:standarddeviation;TPN:totalparenteralnutrition.
ofthehospitalstay.Severalstudieshavereportedthatfood intakeissignificantlycompromisedduringtheperiodof trans-plantationmainlybecauseofthe sideeffectsrelatedtothe conditioningregimen.19
Thefoodintakeofpatientsthroughoutthehospitalstay wasprobablyinfluencedbyGIsymptoms(Table4).Themean numberofdayswithfullfoodintakewasonly13.6%ofthe hospitalizationperiod.
Amongthepatientsstudied,62.7% receivedTPN,witha medianof47%daysonTPN.Hence,itisinterestingtonote thatthepercentageofdaysonwhichthepatientwasfasting islower,only18.1%.ThisindicatesthattheTPNwasassociated withoralingestionmostofthetime.
Table4–Gastrointestinalsymptomsduring
hospitalization.
Symptoms %
Nausea 100.0
Vomiting 96.6
Mucositis 93.2
GradeI 10.9
GradeII 21.8
GradeIII 29.1
GradeIV 36.4
Odynophagia 86.4
Hyporexia 78.0
Diarrhea 76.3
Abdominalpain 69.5
Epigastralgia 54.2
Syalorrhea 52.5
Abdominaldistension 44.1
Gastricfullness 30.5
Heartburn 13.6
Dysgeusia 13.6
Xerostomia 6.8
SeveralstudiescomparingENwithTPNreportedthatthe useofnutritionaltherapybasedontheGItractispreferred asit isamorephysiologicapproach.20Furthermore,TPNis
associated with an increased risk of infections, especially in immunocompromised patients, which include patients submittedtoHSCT.13,20 However,inAllogeneic HSCT,most
patientsprogresstoseveremucositisassociatedwith throm-bocytopenia,makingENlessusedinadultpatients.
Thepercentageofpatients withsomedegreeof malnu-trition on admissionwas only 3.1%and the percentage of overweight/obesitywas51.5%.Sucak etal.,inastudy with 71 patients, found a similar distribution in relationto the prevalenceofmalnutritiononadmission(5.6%)butlowerfor overweight/obesity(39.5%).21
Thepatientsshowedaworseningintheirnutritionalstatus duringhospitalizationaccording toanthropometric (weight lossanddecreaseinBMI)andlaboratoryparameters(decrease in serum albumin levels). Body weight, as well as other parameters,haslimitationsfornutritionalassessment dur-ing HSCT,especially in patientswho use TPN as theycan haveincreasedbodywater,therebymaskingtherealweight loss.22
AccordingtoasurveyofJapanesepatients submittedto allogeneic HSCTand evaluated bybioelectricalimpedance, morethan halfofthe population (50.6%)had lossof mus-clemassbeforetransplantation.Thesedatasuggestthatthe nutritional statusmeasured byweight and using BMIas a parameter,couldmaskalossofmusclemassandthe accu-mulationoffatmass.23
The nutritional status of patients during HSCT is not welldocumented intheliterature.Few studieshave evalu-atedthenutritionalimpactonadultsofallogeneicHSCT.10,24
Park and Park evaluated the nutritional status before and after allogeneic HSCT and observed a negative impact on thenutritionalstatuspost-transplantation,butthe relation-shipofnutritionalstatusontheoutcomeofHSCTwasnot evaluated,forexample,regardingthetimeofgraftingorthe appearanceofGIand/orclinicalcomplications.25Sucaketal.
observedanegativecorrelationbetweenBMIofpatients sub-mittedtoallogeneicHSCTandthedevelopmentofsymptoms andmetaboliccomplications,suchasmucositis, cardiotoxic-ityandhyperglycemia.21
Some studies indicate that the nutritional status of the patient before transplantation can affect the progno-sis,andtheextremes(malnutritionandobesity)arerelated to higher mortality and more complications associated withtransplantation.7,10 Inthis scenario,specialized
nutri-tionalinterventionsmaycontributetoincreasedtoleranceto chemotherapyandradiotherapy,contributingtothesuccess oftreatment.9,12,26
Asin thisstudy, Le Blanc,Ringdén and Remberger also foundnocorrelationbetweennutritionalstatusandtimeof neutrophilengraftment inpatients submittedtoallogeneic transplantation.27Hadjibabaeetal.howeverfounda
signifi-cantdelayinengraftmentofneutrophilsandplateletsinlow weightpatientssubmittedtoallogeneictransplantation.22
Moststudiesontherelationshipbetweennutritionalstatus andpost-transplanttoxicityrefertoadultpatientssubmitted toautologoustransplantation,whichisatreatmentmodality relativelywelltoleratedintermsoftoxicity.
Althoughthenutritionalstatusdoesnotpresentanymajor impactonimmunologicalcomplicationsortumorbehavior, nutritionalstatusmayhaveanimpactonthemetabolismof chemotherapeuticagents.Thedecreasedlevelsofplasma pro-teinsandareducedglomerularfiltrationratemayincreasethe freedrugconcentrationandaggravatethecytotoxiceffectsin patientswithlowweight.21
Furthermore, the altered nutritional status, particularly malnutritionandobesitycanhaveanegativeimpactonthe riskofinfection,whichisconsideredtobethemaincauseof morbidityand mortalityrelatedtoHSCT.8,21 Approximately
50% of patients remain withincreasedcaloric and protein needsuptooneyearafterHSCT.10
Hosley,BauerandGallagherfoundthatpatientsclassified asmalnourishedaccordingtotheSubjectiveGlobal Assess-ment(SGA)validatedforcancerpatientshadaBMIwithinthe normalrange(23.8kg/m2).24Theseresultscorroborateother
studiesshowingthatcancerpatientsclassifiedasnormalor overweight byBMI, could beclassified asmalnourished by theSGA,thussuggestingthatthebodyfatofthese individ-ualsmightbemaskingsomedegreeofmalnutritionnotyet revealedbytheweight.28
Althoughthisstudypresentssomelimitationsrelatedto thesamplesizeandtheretrospectivedesign,theresultsagree with previous studies,reiterating the impairment of nutri-tionalstatusduringthetransplantationprocess.
Conclusion
OurresultssuggestthatpatientssubmittedtoallogeneicHSCT haveaworseningintheirnutritionalstatusduring hospital-ization,mainlycharacterizedbyweightloss,highprevalence ofGIsymptomsandlowdietaryintake,probablyduetothe hightoxicityrelatedtothistypeoftransplantandits compli-cations.Thusitisimportanttoanalyzethefactorsinvolvedin causing thenutritionaldeficitsinordertoimplementearly nutritional interventioninpatientssubmitted toallogeneic HSCT.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.GratwohlA,BaldomeroH,AljurfM,PasquiniMC,BouzasLF, YoshimiA,etal.Hematopoieticstemcelltransplantation:a globalperspective.JAmMedAssoc.2010;303(16):1617–24.
2.LjungmanP,BregniM,BruneM,CornelissenJ,deWitteT,Dini G,etal.Allogeneicandautologoustransplantationfor haematologicaldiseases,solidtumoursandimmune disorders:currentpracticeinEurope2009.BoneMarrow Transplant.2010;45(2):219–34.
3.CastroJrCG,GregianinLJ,BrunettoAL.Transplantede medulaósseaetransplantedesanguedecordãoumbilical empediatria.JPediatr.2001;77(5):345–60.
bonemarrowtransplantation.AmJClinNutr. 2002;75(2):183–90.
5. HarousseauJL.Roleofstemcelltransplantation.Hematol OncolClinNorthAm.2007;21(6):1157–74.
6. MajhailNS,RizzoJD,LeeSJ,AljurfM,AtsutaY,BonfimC,etal. Práticasrecomendadasparatriagemeprevenc¸ãode
complicac¸õesemsobreviventesdelongoprazoapós transplantedecélulashematopoéticas.RevBrasHematol Hemoter.2012;34(2):109–33.
7. AkbulutG.Medicalnutritionalinhematopoieticstemcell transplantation(HSCT).IntJHematolOncol.2013;1(23):55–65.
8. RzepeckiP,BarzalJ,OborskaS.Bloodandmarrow transplantationandnutritionalsupport.SupportCare Cancer.2010;18(2):57–65.
9. ZatarainL,SavaniBN.Theroleofnutritionandeffectsonthe cytokinemilieuinallogeneichematopoieticstemcell transplantation.CellImmunol.2012;276(1-2):6–9.
10.SilvaML,VasconcelosMI,DiasMC,CostaGC,MoraesP. Terapianutricionalnotransplantedecélulahematopoiética. Associac¸ãoMédicaBrasileiraeConselhoFederalDeMedicina: ProjetoDiretrizes;2011.Availablefrom:http://www.
projetodiretrizes.org.br/9volume/terapianutricionalno transplantedecelulahematopoietica.pdf[07.05.14]. 11.deCastroJrCG,GregianinLJ,BrunettoAL.AnáliseClínicae
epidemiológicadotransplantedemedulaósseaemum servic¸odeoncologiapediátrica.JPediatr.2003;79(5):413–22.
12.Martin-SalcesM,dePazR,CanalesMA,MesejoA, Hernandez-NavarroF.Nutritionalrecommendationsin hematopoieticstemcelltransplantation.Nutrition. 2008;24(7-8):769–75.
13.LeeJH,ChoiSJ,LeeJH,KimSE,SeolM,LeeYS,etal.Severe metabolicabnormalitiesafterallogeneichaematopoieticcell transplantation.BoneMarrowTransplant.2005;35(1):63–9.
14.MielcarekM,MartinPJ,LeisenringW,FlowersME,Maloney DG,SandmaierBM,etal.Graft-versus-hostdiseaseafter non-myeloablativeversusconventionalhematopoieticstem celltransplantation.Blood.2003;102(2):756–62.
15.WorldHealthOrganization.Obesity:preventingand managingtheglobalepidemicofobesity.ReportoftheWHO ConsultationofObesity.Geneva:WHO;1997,June3–5.
16.BechardLJ,GuinanEC,FeldmanHA,TangV,DugganC. Prognosticfactorsintheresumptionoforaldietaryintake afterallogeneichematopoieticstemcelltransplantation (HSCT)inchildren.JParenterEnteralNutr.2007;31(4):295–301.
17.SommacalHM,JochimsAM,IlaineSchuchI,SillaLM. Comparac¸ãodemétodosdeavaliac¸ãonutricional
empregadosnoacompanhamentodepacientessubmetidosa transplantedecélulas-troncohematopoéticasalogênico.Rev BrasHematolHemoter.2010;32(1):50–5.
18.MinWS.Bonemarrowtransplantation.KoreanJCritCare Med.2001;16(1):17–22.
19.SoEJ,LeeJS,KimJY.Nutritionalintakeandnutritionalstatus bythetypeofhematopoieticstemcelltransplantation.Clin NutrRes.2012;1(1):3–12.
20.GuièzeR,LemalR,CabrespineA,HermetE,TournilhacO, CombalC,etal.Enteralversusparenteralnutritionalsupport inallogeneichaematopoieticstemcelltransplantation.Clin Nutr.2014;33(3):533–8.
21.SucakGT,SuyanıE,BaysalNA,AltındalS¸,C¸akarMK,AkıS¸Z, etal.Theroleofbodymassindexandotherbody
compositionparametersinearlypost-transplant complicationsinpatientsundergoingallogeneicstemcell transplantationwithbusulfan–cyclophosphamide conditioning.IntJHematol.2012;95(1):95–101.
22.HadjibabaieM,IravaniM,TaghizadehM,Ataie-JafariA, ShamshiriAR,MousaviSA,etal.Evaluationofnutritional statusinpatientsundergoinghematopoieticSCT.Bone MarrowTransplant.2008;42(7):469–73.
23.MorishitaS,KaidaK,TanakaT,ItaniY,IkegameK,OkadaM, etal.Prevalenceofsarcopeniaandrelevanceofbody composition,physiologicalfunction,fatigue,andhealth relatedqualityoflifeinpatientsbeforeallogeneic hematopoieticstemcelltransplantation.SupportCare Cancer.2012;20(12):3161–8.
24.HorsleyP,BauerJ,GallagherB.Poornutritionalstatuspriorto peripheralbloodstemcelltransplantationisassociatedwith increasedlengthofhospitalstay.BoneMarrowTransplant. 2005;35(11):1113–6.
25.ParkMY,ParkJY.Preandpost-transplantnutritional assessmentinpatientsundergoingallogeneichematopoietic stemcelltransplantation.AsianOncolNurs.2012;12(1):110–6.
26.HabschmidtMG,BaconCA,GregoireMB,RasmussenHE. Medicalnutritiontherapyprovidedtoadulthematopoietic stemcelltransplantationpatients.NutrClinPract. 2012;27(5):655–60.
27.LeBlancK,RingdénO,RembergerM.Alowbodymassindex iscorrelatedwithpoorsurvivalafterallogeneicstemcell transplantation.Haematologica.2003;88(9):1044–52.