www.jped.com.br
REVIEW
ARTICLE
Obesogenic
environment
---
intervention
opportunities
夽
Mauro
Fisberg
a,b,c,∗,
Priscila
Maximino
c,
Juliana
Kain
d,
Irina
Kovalskys
e,faInternationalLifeSciencesInstitute(ILSIBrasil),Brazil
bEscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo(Unifesp),SãoPaulo,SP,Brazil cInstitutoPensi,Fundac¸ãoJoséLuizEgydioSetúbal,HospitalInfantilSabará,SãoPaulo,SP,Brazil
dInstitutodeNutricionyTecnologiadelosAlimentos(INTA),UniversidaddeChile,SantiagodeChile,Chile eInternationalLifeSciencesInstitute(ILSIArgentina),Argentina
fSchoolofMedicalSciences,UniversidadFavaloro,BuenosAires,Argentina
Received18January2016;accepted5February2016 Availableonline19March2016
KEYWORDS
Schoolenvironment; Physicalactivity; Children; Adolescents; Obesity
Abstract
Objectives: Toevaluateenvironmentalobesogenic-relatedfactors,suchasphysicalactivityin neighborhoodsandschools,nutritionalbehavior,andinterventionprograms.
Sources: Criticalanalysisofliteraturewithpersonalpointofviewfrominfantobesityexperts andpoliticaladvisorsforpublicintervention.
Datasynthesis: Althoughobesityisapublichealthproblemaffectingseveralagegroups,itis amongchildrenandadolescentsthatitplaysamoreimportantrole,duetotreatment complex-ity,highlikelihoodofpersistenceintoadulthood,andassociationwithothernon-transmissible diseaseswhilestillinearlyage.Environmentisamaincomponentofthegenesisandoutcomes inthenearfutureorlongterm.Modificationofintakewithhigh-densityfood,mealskipping, andhighintakeofsaturatedfat,sugar,andsalt,associatedtohighlevelsofsedentarismare maincausesofobesity.
Conclusion: Interventionopportunitiesarerelatedtomodificationsinpolitical,environmental, andindividualsettings.Schoolandphysicalactivitiesintheeducationalenvironmentare inter-twinedwithnutritioninterventionincontinuouseducation.Acriticalreviewofsomedifferent scenariosinLatinAmericancountriesispresented.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/ 4.0/).
夽
Pleasecitethisarticleas:FisbergM,MaximinoP,KainJ,KovalskysI.Obesogenicenvironment---interventionopportunities.JPediatr (RioJ).2016;92(3Suppl1):S30---9.
∗Correspondingauthor.
E-mails:[email protected],[email protected](M.Fisberg).
http://dx.doi.org/10.1016/j.jped.2016.02.007
0021-7557/©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND
PALAVRAS-CHAVE
Ambienteescolar; Atividadefísica; Crianc¸as; Adolescentes; Obesidade
Ambienteobesogênico---oportunidadesdeintervenc¸ão
Resumo
Objetivos: Avaliarosfatoresrelacionadosaoambienteobesogênico,comoatividadefísicanos bairrosenasescolas,comportamentonutricionaleprogramasdeintervenc¸ão.
Fontes: Análisecríticadaliteraturacompontodevistadeespecialistasemobesidadeinfantil econselheirospolíticosdeintervenc¸õespúblicas.
Resumodosdados: Emboraaobesidadesejaumproblemadesaúdepúblicaqueafetadiversas faixasetárias,éentrecrianc¸aseadolescentesqueeladesempenhaumpapelmaisimportante devido àcomplexidade do tratamento, àalta probabilidade de persistência navidaadulta eàassociac¸ãocomoutrasdoenc¸as nãotransmissíveiscominícioprecoce.Oambienteéum componenteprincipaldagêneseedosresultadosnofuturopróximoouemumprazomaislongo. Amodificac¸ãodoconsumodealimentosdealtadensidade,pularrefeic¸õeseoaltoconsumode gordurasaturada,ac¸úcaresal,associadosaosaltosníveisdesedentarismo,sãoasprincipais causasdaobesidade.
Conclusão: Asoportunidadesdeintervenc¸ãoestãorelacionadasamodificac¸ões noscenários político,ambiental eindividual. Atividadesescolaresefísicasnoambienteeducacional são intercaladascomintervenc¸ãoalimentarem umaeducac¸ãocontínua.Uma análisecríticade algunscenáriosdiferenteséapresentadaempaíseslatino-americanos.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Obesity is defined as excessivebody adiposity, above the ideallevelsforgoodhealth.Itdevelopsfromachronic, posi-tiveenergybalance,undertheinfluenceofmultiplefactors of social,behavioral, andenvironmentalorigin.1Although obesity is a public health problem affecting several age groups, it isamongchildren and adolescentsthatit plays amoreimportantrole,duetotreatment complexity,high likelihood of persistence into adulthood, and association withother non-transmissiblediseases starting at an early age.2,3 Between 1990 and 2010, childhood obesity in the worldincreasedfrom4.2%to6.7%,beinghigher in devel-opedcountries(7.9---11.7%)ascomparedtodevelopingones (3.7---6.1%).4It isestimatedthatin LatinAmerica,7.1%of childrenbelowtheageof5yearsareobese.Obesity preva-lencebetweentheagesof5and11yearsrangesfrom18.9% to36.9%,whereasamongadolescents(12---19yearsofage) itvariesfrom16.6%to35.8%.5
InBrazil,intheyearsencompassedbetweentheNational StudyofFamilyExpense(EstudoNacionaldeDespesa Famil-iar[ENDEF])of1974/75andtheResearchofFamilyBudget (PesquisadeOrc¸amentosFamiliares[POF])6of1996/97,the obesity prevalence observed amongchildren of the coun-tryincreasedfrom4.9%to17.4%.7Nevertheless,ananalysis by age bracket shows that obesity amongchildren below the age of 2 years decreased 2.5%. Currently it affects 6.5% of this age group, having increased among children betweentheagesof2and5yearsfrom3.0%to7.7%.8 Obe-sityincreasedsix-foldamongschoolchildrenbetween the agesof5and9years,affecting16.8%and11.8%ofboysand girls, respectively. Among adolescents,this condition was estimatedat5.9%amongboysandat4.0%amonggirls.9
An obesogenic environment includes all aspects that have been shown to be related to possible cause-effects
of generingobesity. Based onthe concept that obesity is agenetic-metabolicdiseasemodifiedbyenvironmental fac-tors,thepresentstudyfocuses onphysicalandnutritional issuesthatcouldmodifyorberelatedtoinfantobesity res-olution.Anon-systematicreviewofintervention programs wasperformed,basedonacriticalapproachandthe expe-rienceof internationalorganizationsfor thepreventionof infantobesity.
Intervention
Onemeasurealoneisnotenoughtoimprovethenutritional profileofthepopulationbecauseoftheepidemiologic com-plexityofchildobesity.Interventionsshouldencompass:
- Incentive measures: disseminate information and moti-vateindividualstoadoptahealthylifestyle;
- Support:facilitate healthy optionsamongalready moti-vatedpeople;
- Healthprotection:preventexposureofindividualsto fac-torsthatstimulatenon-healthyhabits.10
Brazilian
politics
regarding
obesity
prevention
and
intervention
BeforethesignatureofthePlan,policiesaimingat mak-ing individuals aware of the importance of healthy life styles,includingtheadoptionofhealthyfoodhabitsandan activelifestyle,hadbeen alreadypublishedinBraziland hadimpactedchildobesity.AnexampleistheNational Pol-icyonFoodandNutrition(PolíticaNacionaldeAlimentac¸ãoe Nutric¸ão[PNAN]),thefirstnationalpolicytoproposeactions thataimatrespecting,protecting,promoting,and provid-inghumanrightsrelatedtohealth andfood,aswellasto emphasizethe importanceofoverweightand obesityasa nationalpublichealthproblem.12
Recently, the Intersectorial Plan of Obesity Prevention and Control in Brazil (Plano Intersetorial de Prevenc¸ão e ControledaObesidade doBrasil) wasalsopublished. The actionsprovidedbythisplanaimatimprovingthe popula-tion’sconsumptionstandards,promotingthepracticeofPA, andorganizingthetreatmentservicesforthiscondition.13
The objective of the National Policy of School Food (PolíticaNacional deAlimentac¸ão Escolar [PNAE]), imple-mented in 1955, is to cater to the nutritional needs of studentswhiletheyareintheclassroom.Accordingtothe policy,schoolfoodshouldofferthreeservingsoffruitsand vegetableseachweek,andamaximumof10%ofenergyfrom simplesugar,15---30%fromtotalfats,10%fromsaturatedfat, and1%fromtransfat.Purchasingoflownutritionalcontent drinksisforbiddenandisrestrictedforsemi-ready prepara-tions,aswell asfor concentratedfoodwithhighlevelsof sodiumorsaturatedfat.Moreover,instateschoolfacilities thesaleofsnacksanddrinkswithproductsand/or prepara-tions,whetherindustrializedornot,containinghighcontent ofcalories,saturatedfat,transfat,freesugars,salt, alco-holcontent,andlownutritionalcontentisforbidden.10The Health Department published, for the private schools, a manualforhealthyschoolcafeterias, withessential infor-mationregardingwhatrepresentsahealthysnackandhow topromoteit.9
Astoadvertisementandmarketingoffood,theNational Agencyof Sanitary Surveillance(Agência Nacional de Vig-ilânciaSanitária [ANVISA])publishedRDC#24/2010,which regulates the supply, advertising, information, and other similarpracticeswhoseobjectiveistodisseminateand com-merciallypromotefoodswithhighlevelsofsugar,saturated fat, trans fat, sodium, and low nutritional content bev-erages.This Resolution representedamajoradvance, but wassuspended,byan injunctionof theFederal Justiceof Brasília, filed by the Brazilian Association of Food Indus-tries (Associac¸ão Brasileira das Indústrias daAlimentac¸ão [ABIA]),whichquestionedANVISA’scompetencetoregulate theissue.14
Healthy
eating
initiatives
In the field of support and incentive for healthy eating, somestudieswereconductedinBrazilfocusingonpromoting breastfeedingandguidancerelatedtothe introductionof supplementaryfood.Interventionswerefocusedon updat-ing the training of professionals regarding feeding in the first year of life and educational activities with infants’ mothersandgrandmothers.Themostusedtheoretical ref-erence in those actions was the ‘‘Ten steps for healthy feeding of children under2 years of age.’’ By and large,
resultspointedtoimprovementinfoodconsumption,such aslonger durationof breastfeeding,less earlyfood intro-duction,delayinintroducing processedfoodtothechild’s diet, and higher frequency in meat consumption without alteringthe nutritionalstatus.15---17 Theauthors praise the positive and protective results for child’shealth and sug-gestthatother etiologicalfactorsshouldbeconsidered in interventionsaimingatobtainingfavorableresultsregarding nutritionalstatus.
Consideringtheeducationalactionstoincentiveand sup-port healthyfoodsin schools,a reviewstudy showedthat mostoftheactionsconductedinBrazilwereimplementedin thelastfiveyears,andanincrementinknowledgeon nutri-tionandchangesinfoodhabitsinchildrenwereobserved.18 However,regardingthenutritionalstatus,andsimilarlyto whatwasidentifiedinactionsgearedtoinfants,thestudies didnot findanystatisticallysignificant changes.This may beexplainedbytheacknowledgmentthatchangesinbody massdonotoccurinashortperiod.19
School-based
intervention
programs
In a nine-month, controlled intervention study conducted amongadolescents(10---11 yearsofage)ofDuquede Cax-ias(RJ),monthlyone-hoursessionsonnutritionaleducation promotedtheconsumptionoffruitandhomemade prepara-tionsinsteadofsugarybeveragesandotherultra-processed foods. Theresults showedareductionintheconsumption of industrializedcookiesandsoftdrinks, togetherwithan increaseinfruitconsumption,withnoimpactonbodymass index(BMI)andonobesityprevalence.19
InTeresina(PI),arandomized,quasi-experimentalstudy withadolescentsof10---14yearsofage,frompublicschools, andwithnineweeklymeetings,showedasignificant reduc-tionintheconsumptionofsoftdrinksandprocessedjuices, aswellasalowerfrequencyofconsumptionofcoldcutsand friedfood.20
Thus, the success of intervention actions with the pediatricgroupisevident,relatedtochangesinfood con-sumptionandtheneedforlongerstudiestoevaluatethereal effectivenessofthechangesinnutritionalstatus.Moreover, thereis a need for studies todecreasethe prevalence of childhoodobesitythat evaluatetheimpactofpublic poli-cies.
gradestudentsaftertwoyearsofinterventionrevealedthat childrenin APPLESschools consumedmorefruitsand veg-etables,consumedlesscalories,andwerelesslikelytobe obese.22
Afewexamplesofpolicy-basedinterventionstochange the school food environment are briefly described here. ‘‘The Healthy Options for Nutrition Environments in Schools’’(HealthyONES)23isbasedonamodelwhichfocuses onorganizationalchange byusingspecificimplementation cycles designed to build capacity within an organization. Thisapproachwasusedinsomelow-incomeschoolsinthe US.Theintervention,whichlastedtwoyears,included elim-inatingthesaleofunhealthyfoodsandthetrainingofschool staffinhealthyeating.Thenutritionenvironmentwasused to determine the amount of foods and beverages avail-able at the schools. Observations were made monthly in eachtargetedschoolenvironment.Resultswerepromising; theunhealthyfoodandbeverageitemsperchildperweek decreasedovertimeininterventionschools,whileincontrol schoolstheyincreased.24,25
The Nutrition Policy Initiative (www.thefoodtrust.org) also was implemented in US schools, but only in those withmorethan50%ofchildreneligibleforfederally subsi-dized,free,orreduced-pricemeals.In2008,Fosteretal.26 includedthefollowingcomponents:schoolself-assessment, nutritioneducation,nutritionpolicy,socialmarketing,and parentoutreach.Arecentevaluationexaminedtheeffects onobesityratesamongfourthtosixthgradestudents.Overa two-yearperiod,itshoweda50%reductionintheincidence ofoverweight,i.e.,significantlyfewerchildreninthe inter-vention schools(7.5%) than inthe control schools (14.9%) becameoverweight;however,nodifferenceswereobserved intheincidenceorprevalenceofobesityaftertwoyears.
Nutrition detectives (www.nutritiondetectives.com),27 whichisactiveinhundredsofschoolsintheUnitedStates and Canada, includes teaching children andtheir parents how to read food labels and detect deceptive marketing strategies, while learning to identify healthful foods. An initial evaluationof thisprogramshowed thatthird grade studentsandparentsininterventionschoolsshoweda signif-icantincreaseinnutritionlabelliteracy,whiletotalcalories, sodium,andsugardecreasednon-significantly,andasfound inmostinterventions,BMIdidnotchange.
Constant28 reviewed theevidence onthe effectiveness of school-based nutrition policy on the food environ-ment, student’s dietary intake, and BMI. The author found that although several policies have been imple-mentedinbothdevelopedasindevelopingcountries,very few have been evaluated. In some countries nutritional standards have already been established for competitive foods,while inother countriesthesewillbeimplemented soon.
Establishing
social
healthy
habits
Becausepreferencesandpurchasingrequestsareinfluenced byculturalandsocialaspectsaswell asmarketing strate-gies, which include advertisements on TV, the Internet, and advergames, schools should take advantage of these strategiestopromotetheappealofhealthierfoodsand bev-erages in variousways (Institute ofMedicine, 2006-online
http://iom.nationalacademies.org/Reports/2005/Food-Marketing-to-Children-and-Youth-Threat-or-Opportunity. aspx).Tastetestinginimaginativeformsprovidesstudents an opportunity to try healthy foods especially fruits and vegetables. Older children can be involved in making changes in order to improve food habits. In the United States,theActionforHealthyKids,StudentsTakingCharge program(http://www.studentstakingcharge.org)29 andthe Alliance for a Healthier Generation’s empowerME@school toolkit (http://www.empowerme2b.org) are resources that provide examples in this area. Social marketing can be especially useful in targeting unhealthy behaviors.30 It is defined as the application of commercial marketing principles (i.e., the four ‘‘Ps’’ of place, price, product, andpromotion) tobenefit society andthe intended audi-enceratherthanthemarketer (Task ForceonCommunity PreventiveServices). Physicalactivity: increasing physical activity through information approaches, behavioral and socialapproaches,environmentalandpolicyapproaches.31 These ‘‘P’’ principles can change community norms by delivering health messages, as well as encouraging indi-vidual behavior change. For example, social marketing can encourage parents to adopt protective behaviors by demonstrating positive parental role models in order to createahealthyhomeenvironment,whichalsoinfluences whatchildrenbuyat school.Socialmarketingcanbeused to promote engagement and positive role modeling, and canalsoinfluencehealthpolicybycreatingandpromoting positivesocialimagesofhealthybehaviors(i.e.,showthat ahealthy option, suchas eatingfruits andvegetables, is superiortoeatingjunkfood).32
Hawkes C. et al.33 recently proposed a novel way of understanding food policy for obesity prevention, iden-tifying four mechanisms, namely: providing an enabling environment for healthy preference, overcoming barri-ers,encouragingindividualstore-evaluatetheirunhealthy choices,andstimulatingafoodsystemsresponse.The evi-dence presented by the authors show that food policies canaffectdietaryintakefromthreeareas:economictools (taxes,subsidies), school settings, and nutritionlabeling. Withrespecttoschools, theimplementationofarangeof activities, mostly nutrition education and changes to the environment,haveproducedmoresignificantandsustained changes. Regarding nutrition education, Kain J. et al.34 showed in a series of interventions in Chile that it had minimaleffects,duetoproblemswithadequate implemen-tation,pre-existingunhealthypreferencesamongchildren, parents, and teachers, as well as lack of changes to the environment. Yet, other studies have shown that nutri-tion education-only interventions have been effective in changing intake of certain foods. Although policies that influence the school environment for obesity prevention are very important, the behavior of parents related to food, nutrition, and physical activity are probably more relevant.Thereisevidencethattherearebarriersfor par-ents to adopting healthy lifestyles, as demonstrated by somestudiesbasedonfocusgroups.Thesebarriersinclude the number of siblings, lack of time and money, neigh-borhood safety,and the child’spreferences for sedentary activities.35---37
recommendations for obesity prevention of sweetened drinks and snacks chips in schools was shown ineffective by Cullenet al.39 becausein some schools students com-pensated by purchasing unhealthy ‘‘non-banned foods.’’ However,anotherstudythatassessed theimpactofa dis-trictlevelnutritionpolicyinLosAngeles(US),whichbanned soft-drinksandsnackswithlimitednutritionalvaluethrough vending machines and direct sales to all students during schooldays,showedthat 55.5% ofstudents reducedtheir softdrinkconsumptionand52.6% reducedsnackintakein school.40
Programs
targeting
the
environment
Reductioninpriceofhealthierfoods,suchaslow-fatsnacks and fruit and vegetables, might increase their sales, as wasshown first by French S., in 2003.41 In addition, ini-tiatives to promote fruit and vegetables consumption at schools have been proven successful42; however, it is not realistic to expect that students will continue to adopt healthy diet behavior at school if the school environ-mentdoes not supportthesebehaviorscontinually, which requires investigating whether students return to their former behavior when the intervention is no longer in place.
Astudypublishedin 2008thatdeterminedtheefficacy of behavioral interventions to prevent childhood obesity throughameta-analysesofrandomizedtrialsconcludedthat the effect on target behaviors was small, while that on BMIwasnon-significant.Longerinterventions,greaterthan sixmonths,yieldedmarginallybetter effectsthanshorter ones.43
Becausein general, most childhoodobesity prevention interventionshave not proved to besufficiently effective to be sustainable in the long run and obesity in most countrieshaseitherincreasedor remainedstable,buthas not declined, several highly respected researchers have recentlyproposeda ‘‘systemsframework’’toaddressthis problem.Thesystemapproachfocusesontherelationships between different aspects of the environment and inter-actions between individuals with the environment.44 It is importanttodistinguishitfromamulticomponentmodel, theinteractionsamongallsectorsrequiredtoproduce sus-tainablechangesthatcanbescalable.Thiscanbeespecially importantto supportmodifications tothe school environ-ment that can make it easier to adopt healthy choices withintheschoolpremises.Theseissues,whichareunique ineach school,arecriticalwhendesigninganintervention anddeterminingitseffectiveness.
PA
opportunities
at
school
Thereisacommonagreementthatduringthelastdecades, there has been a displacement of time from playing, engagingsports,andrecreationalgamestowardsacademic activities. Even some of the after-school programs must competewithtechnologicaloptions.Additionally, physical education(PE)classesdonotalwaysinfluenceenergy bal-ance with moderate to vigorous physical activity (MVPA). The Center for Disease Control and Prevention of the UnitedStatesrecommends thatMVPA shouldtakeat least
50% of lesson time. A global review, published by Hol-lis, including studies from nine countries and published between 2005and2014, analyzed theproportionofMVPA during PE lessons.45 The authors concluded that studies based on direct observations report that children spent 57.6%ofthePElessonperformingMVPA,comparedto stud-ies based on accelerometers in which only 32.6% of the time was spent on MVPA. It is clear that although there arestilllimitations onPA evaluationmethods in children, interventions aimed at increasing MVPA in PE lessons are needed.
Schoolbreaks arean excellentopportunity todevelop motivational and recreational activities that improve the PAlevelandfairplay. ComparedtoPEclasses, breaksare usually full of non-competitive activities based onfun. A quasi-experimental intervention study conducted in three schools in Californiatested the timespent onMVFA after teachers’ social prompting of PA during recess. Findings from this study indicate that when a teacher prompted a child to engage in MVPA, it had a significant impact on the amount of MVPA while modeled by a competent adult.46
Unfortunately,whenthesetypesofinterventionsare ana-lyzedregardingobesityprevention,thesizeeffectonBMIis toosmallornull.Mostofthecurrentstudiesarefocusedon demonstratingresultsassociatedwithchronicdisease pre-vention; however, undera more qualitative standpoint of theintervention,itispossiblethatinthelongrun,thereis impactfromsustainablehealthybehaviorlinkedtoPA.
‘‘TAKE10!’’isanotherexample ofaprogramaimedat addressingthebarriersagainstsedentarybehavioratschool. It takesadvantage of theaccumulation of tenminutes of PAduringregularclasses, integratingmovementwith aca-demics in elementary schools. Up to August 2010, more than 40,000 schools in the United Sates had participated inTAKE10!fortheprevious tenyears.Theanalysisofthe programs influence onenergybalance suggests incremen-talexpenditureattributedTAKE10!activities,whichrange from24to43kcalper10-minute session.Thelonger-term studies reportedby Kibbe etal. suggest thatBMI mainte-nanceisachievedininterventionstudentswhenexposureis sustained.47
Effectiveness
of
PA
in
obesity
prevention
interventions
Generallyspeaking,pediatricobesity preventionprograms havebeenfoundtocausesmallchangesintargetbehaviors andsmallornosignificanteffectonchildren’sactivitylevel andBMI.43,49Ontheotherhand,demonstratedbythesame methodology(systematicreviewandmeta-analysis)within similarperiodsofsearch,anotherstudyshowedthe impor-tanceofthePAcomponentinschool-basedinterventionsto beeffectiveinreducingBMIinchildren.50
The bias associated to these differences could be attributed to the measurement of variables of energy expenditure (accelerometer, observational, and/or ques-tionnaires), and/or cut offs of anthropometric measure-ments,andalso,theselectionofthestudies(randomizedor non-randomized).Allareprobablycausesofthedifferences inassessmentsand,consequently,intheconclusions.
TwoCochranereviewsongeneralinterventionsfor pre-ventingobesityinchildrenandspecificallyonschool-based PAprogramshavedemonstratedmorepositive results.51,52 The first, which assessed educational, behavioral, and health promotion interventions, reported the success of interventions at preventing childhood obesity with no adverse outcomes, by improving both dietary and PA behavior.53,54
SpecificallyrelatedtoPA,inallagegroups(0---5,6---12, and 13---18 years), individual studies that met inclusion criteriademonstrateasignificantinterventioneffecton PA-relatedfactors(three, 21, andfivestudies, respectively), andsomeofthemintermsofadiposity.Thesecondreview publishedbyDobbinswasfocusedonprogramspromotingPA andfitnessinchildren.Afteranalyzing26studiesfrom302 eligibleones,therewasevidencethatschool-basedPA inter-ventionshadapositiveimpactonfourofthenineoutcome measures:durationofPA,televisionviewing,VO2max,and bloodcholesterol.
These results indicate that despite BMI not being an effective primary outcome measure, some other positive healthoutcomescouldbeconsideredaspartofthevariables thatdeterminepreventionofchronicdiseases.
OpportunitiesforPAinschools,interventionstoincrease duration and recreational PA, and capacity building for teachers appear to be critical to determine and sustain healthy habits. Sincethese behaviorsareoften promoted byenvironmentalcues,currentfindingssuggestvalueofthis typeofintervention,especiallyinproposingchange strate-giesthatfavorPA(Table1).
Recommendations
Despitedifferencesinsizeeffectofpositiveoutcomesfrom PAinterventions,thereisnodoubtaboutthegeneral ben-eficialeffectof PAduringgrowth anddevelopment.From psychological tobiological issues, thereare awide range ofhealthoutcomesthathaveprovedtobebeneficialfora healthylife.RecommendationofPAduringchildhoodisthus aconsensusamongscientistsandresearchers.55
Oneofthekeypointsincludesstartingasearlyas possi-bletofavoralinkbetweenearly-lifeexperiencesandlater healthoutcomes,creatingapatternofPAbehaviorsthrough
life.AnotheraspectisthatcurrentlevelsofPAareverypoor, andbothdevelopedanddevelopingcountriesdonotmeet PArecommendations,despitetheexistentguidelines.Asa generalrule,recommendationsinclude,type,andduration ofPA,andlevelofintensity.
The environmentplaysa criticalrolein infancy, favor-ingordiscouraging engagementin recreationalmovement activities, PA, and sports. The role of education through messages,or academiccontentswithinthecurricula, con-troversially does not influence behaviors if they are not supportedbyanincreaseinopportunitiesandmoreaccessto facilitiesandactivities.Educationaloneislesseffectivefor preventionthantreatmentprograms,incontrastto encour-agingteachersandtheentireschoolstafftobecomedrivers ofphysicalandhealthliteracyandbehaviorchange,andalso forbeingthemselvesmorephysicallyactive.56
Summaryofrecommendations
• Time:Elementaryschools150/minutes/week.Secondary
schools225---300minutes/week.
• Intensity in PE classes: Students are physically active
(MVPA)foratleast50%ofthePElessontime.
• Quality: Enjoyable classes while teaching and children
developappropriateskillsforageandgender.
• Duringschool time:Increase opportunities tobeactive
duringrecessandlunchtime.ConsiderintegratingPAinto classroomactivities.
• Schoolsshouldprovideadequateenvironments,including
equipmentandplaygrounds,andalsoorganizeactivities duringbreaks.
• Encourageandofferafterschoolactivities,both
compet-itive andnon-competitive, in orderto include asmany studentsaspossible.
• Engage teachers and familythroughevents, education,
messages,andmarketingfavoringPA,workingpositively tocreateanactiveschoolcommunity.
Barriers
and
conclusions
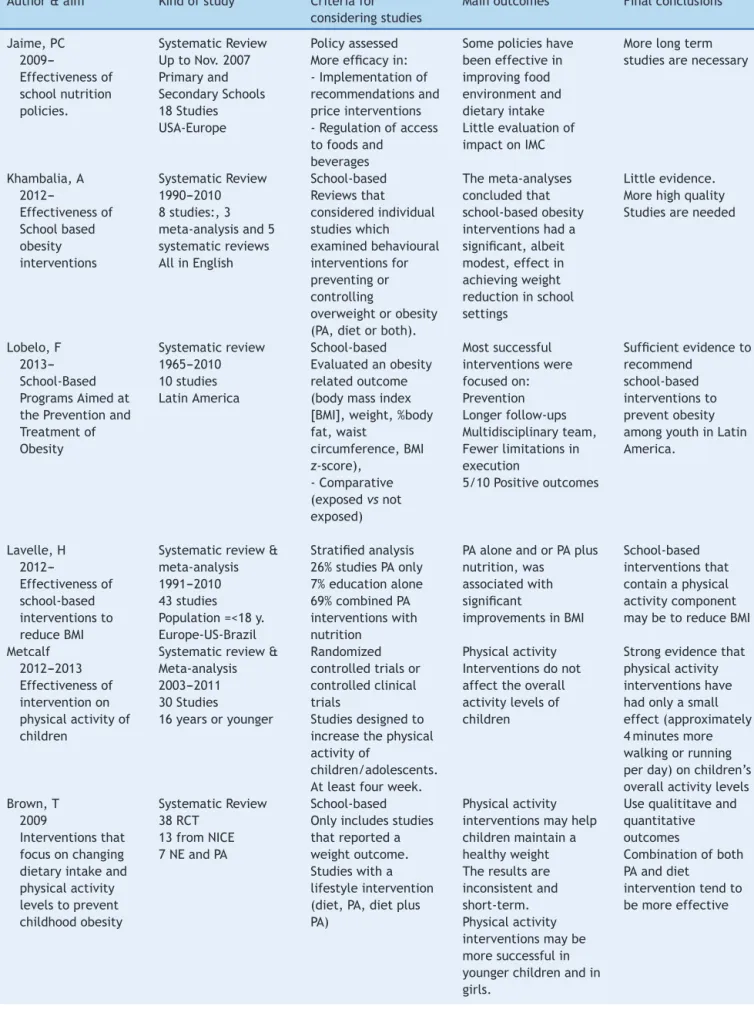
Table1 Summaryofreviewsand/ormeta-analysisforphysicalactivityintervention.
Author&aim Kindofstudy Criteriafor consideringstudies
Mainoutcomes Finalconclusions
Jaime,PC 2009---Effectivenessof schoolnutrition policies. SystematicReview UptoNov.2007 Primaryand SecondarySchools 18Studies USA-Europe
Policyassessed Moreefficacyin: -Implementationof recommendationsand priceinterventions -Regulationofaccess tofoodsand
beverages
Somepolicieshave beeneffectivein improvingfood environmentand dietaryintake Littleevaluationof impactonIMC
Morelongterm studiesarenecessary
Khambalia,A 2012---Effectivenessof Schoolbased obesity interventions SystematicReview 1990---2010 8studies:,3 meta-analysisand5 systematicreviews AllinEnglish
School-based Reviewsthat consideredindividual studieswhich examinedbehavioural interventionsfor preventingor controlling
overweightorobesity (PA,dietorboth).
Themeta-analyses concludedthat school-basedobesity interventionshada significant,albeit modest,effectin achievingweight reductioninschool settings
Littleevidence. Morehighquality Studiesareneeded
Lobelo,F 2013---School-Based ProgramsAimedat thePreventionand Treatmentof Obesity Systematicreview 1965---2010 10studies LatinAmerica School-based Evaluatedanobesity relatedoutcome (bodymassindex [BMI],weight,%body fat,waist
circumference,BMI z-score),
-Comparative (exposedvsnot exposed) Mostsuccessful interventionswere focusedon: Prevention Longerfollow-ups Multidisciplinaryteam, Fewerlimitationsin execution
5/10Positiveoutcomes
Sufficientevidenceto recommend
school-based interventionsto preventobesity amongyouthinLatin America. Lavelle,H 2012---Effectivenessof school-based interventionsto reduceBMI
Systematicreview& meta-analysis 1991---2010 43studies Population=<18y. Europe-US-Brazil
Stratifiedanalysis 26%studiesPAonly 7%educationalone 69%combinedPA interventionswith nutrition
PAaloneandorPAplus nutrition,was
associatedwith significant
improvementsinBMI
School-based interventionsthat containaphysical activitycomponent maybetoreduceBMI
Metcalf 2012---2013 Effectivenessof interventionon physicalactivityof children
Systematicreview& Meta-analysis 2003---2011 30Studies
16yearsoryounger
Randomized controlledtrialsor controlledclinical trials
Studiesdesignedto increasethephysical activityof
children/adolescents. Atleastfourweek.
Physicalactivity Interventionsdonot affecttheoverall activitylevelsof children
Strongevidencethat physicalactivity interventionshave hadonlyasmall effect(approximately 4minutesmore walkingorrunning perday)onchildren’s overallactivitylevels Brown,T
2009
Interventionsthat focusonchanging dietaryintakeand physicalactivity levelstoprevent childhoodobesity
SystematicReview 38RCT
13fromNICE 7NEandPA
School-based Onlyincludesstudies thatreporteda weightoutcome. Studieswitha lifestyleintervention (diet,PA,dietplus PA)
Physicalactivity interventionsmayhelp childrenmaintaina healthyweight Theresultsare inconsistentand short-term. Physicalactivity interventionsmaybe moresuccessfulin youngerchildrenandin girls.
Usequalititaveand quantitative outcomes
Combinationofboth PAanddiet
Table1 (Continued)
Author&aim Kindofstudy Criteriafor consideringstudies
Mainoutcomes Finalconclusions
Waters,E 2011
CochraneReview
Review& Meta-analysis Case-ControlStudies (Randomizedornot) Atleast12weeks 55Studies(37 meta-analysis) 6---12yearsold
Studieswereincluded iftheyevaluated interventions, policiesorprograms inplacefortwelve weeksormore
Programswere effectiveatreducing adiposity,althoughnot allindividual
interventionswere effective
Strongevidenceto supportbeneficial effectsofchild obesityprevention programsonBMI, Include
recommendationsand strategies
Guerra,PH 2013 School-based physicalactivity andnutritional education interventionson bodymassindex
Meta-analysis Publishedafter2000 33articles
6---18yearsold
Schoolbased RCTonPAandNE PerformedPAandNE interventionsfor childrenand adolescents DescribedtheBMI outcomeinboth interventionand controlgroups
Showednostatistically significantmean reductiononchildren’s andadolescents’BMIin normalpopulation. Littlepositiveeffect wasobservedwhen includingOWandOB
Morestudiesare neededinorderto provideaneffective frameworktobe implementedinthe schoolsetting.
RCT,randomizedcontrolledtrial;PA,physicalactivity;BMI,bodymassindex;OW,overweight;OB,obese;NE,nutritionaleducation.
facilitator,were proposed:a minimumnumber of materi-alsweredonated, playgroundswerepaintedtoencourage playing onthepainted ground, andthe teacher’straining wasadequate toincrease moderate andvigorousphysical activityduringschoolhours.57
Considering that global environmental conditions are leadingtoenergyimbalance,manyintervention opportuni-tiesappeartobeatleastpartofthesolution.Itseemsvery difficulttoarbitraryseparatethecomponentsofenergy bal-ance,butinchildren,theenergyexpenditurethroughPAis acrucialcomponentinpreventivestrategies.
Someauthorssuggestthatschool-basedinterventionsare more effective compared to home-based interventionsto preventobesityinchildrenandadolescents.De Bourdeaud-huihetal.58 reviewed11 Europeanstudies andconcluded thatcombiningeducationalandenvironmentalcomponents thatfocusonbothsidesoftheenergybalancecreatebetter and morerelevant effects, suggesting that environmental interventionsmightincludePAinterventionslikeorganized PA during breaks, or before and after school; improved availability of PA opportunities in and around the school environment;andincreasedPElessontime;withoutfailing toconsidertheinterventionsonhealthyfoodoptions.
Funding
ILSI, Coca-Cola, CPW, Danone Institute International and DanoneResearch,CNPq.
Conflicts
of
interest
Mauro Fisberg is an invited speaker for Abbott, Danone, Coca-Cola,Nestle,Unilever,EMS.Theotherauthorsdeclare tohavenoconflictsofinterest.
References
1.Swinburn BA, Sacks G, Hall KD, McPherson K, Finegood DT, Moodie ML, et al. The global obesity pandemic: shaped byglobal driversand local environments.Lancet. 2011;378: 804---14.
2.SBP.---SociedadeBrasileiradePediatria.Obesidadenainfância eadolescência:manualdeorientac¸ão.2ndedic¸ão.[cited2Feb 2012]. Available from: http://www.sbp.com.br/publicacoes/ para-a-familia/obesidade-na-infancia-e-adolescencia-manual-de-orientacao-2-edicao-revisada-e-ampliada/.
3.Daniels SR, Hassink SG, Committee On N. The role of the pediatrician in primary prevention of obesity. Pediatrics. 2015;136:e275---92.
4.deOnisM,BlossnerM,BorghiE.Globalprevalenceandtrends ofoverweightandobesityamongpreschoolchildren.AmJClin Nutr.2010;92:1257---64.
5.RiveraJÁ,deCossíoTG,PedrazaLS,AburtoTC,SánchezTG, MartorellR.Childhoodandadolescentoverweightandobesityin LatinAmerica:asystematicreview.LancetDiabetesEndocrinol. 2014;2:321---32.
6.PesquisadeOrc¸amentosFamiliares2008---2009:antropometriae
estadonutricionaldecrianc¸as,adolescenteseadultosnoBrasil.
In:MinistériodoPlanejamento,Orc¸amentoeGestão,editor.Rio
deJaneiro(Brasil);MinistériodoPlanejamento,Orc¸amentoe
Gestão:2010.
7.Wang Y, Monteiro C, Popkin BM. Trends of obesity and underweightin olderchildrenand adolescentsinthe United States, Brazil, China, and Russia. Am J Clin Nutr. 2002;75: 971---7.
8.CocettiM,TaddeiJA,KonstantynerT,KonstantynerTC,Barros Filho AA. Prevalence andfactors associated withoverweight amongBrazilianchildrenyoungerthan2years.JPediatr(Rio J).2012;88:503---8.
9.Manual das cantinas escolares saudáveis: promovendo a
alimentac¸ão saudável. Ministério da Saúde. Secretaria de
Atenc¸ãoà Saúde.Departamentode Atenc¸ãoBásica. In:
Min-istériodaSaúde,editor.Brasilia(Brasil);MinistériodaSaúde:
10.ReisCE,VasconcelosIA,BarrosJF.Políticaspúblicasdenutric¸ão para o controle da obesidade infantil. Rev Paul Pediatr. 2011;29(4):625---33.
11.PAHO.PlanofActionforthePreventionofObesityinChildren and Adolescents.Washington,DC,USA:PanAmerican Health Organization;2014.
12.Política Nacional de Alimentac¸ão e Nutric¸ão. Ministério da
Saúde. Secretaria de Atenc¸ão à Saúde. Departamento de
Atenc¸ãoBásica.In:MinistériodaSaúde,editor.Brasília(Brasil);
MinistériodaSaúde:2012.
13.Planodeac¸õesestratégicasparaoenfrentamentodasdoenc¸as
crônicasnãotransmissíveis(DCNT)noBrasil2011---2022.In:
Min-istério da Saúde, editor. Secretariade Vigilância em Saúde.
DepartamentodeAnálisedeSituac¸ãodeSaúde.Brasília(Brasil);
MinistériodaSaúde:2011.
14.HenriquesP,DiasPC,BurlandyL.Aregulac¸ãodapropagandade alimentos:convergênciaseconflitosdeinteresses.CadSaude Publica.2014;30(6):1219---28.
15.Louzada ML, Campagnolo PD, Rauber F, Vitolo MR. Long-term effectiveness of maternal dietary counseling in a low-income population: a randomized field trial. Pediatrics. 2012;129:e1477---84.
16.VitoloMR,LouzadaML,RauberF.Atualizac¸ãosobrealimentac¸ão da crianc¸a para profissionais de saúde: estudo de campo randomizado por conglomerados. Rev Bras Epidemiol. 2014;17:873---86.
17.SchwartzR,VigoA,deOliveiraLD,GiuglianiER.Theeffectof apro-breastfeedingandhealthycomplementaryfeeding inter-vention targeting adolescent mothers and grandmothers on growth and prevalence of overweightof preschool children. PloSOne.2015;10:e0131884.
18.RamosFP,SantosLA,ReisAB.Educac¸ãoalimentarenutricional em escolares:umarevisãode literatura.CadSaudePublica. 2013;29:2147---61.
19.da Veiga GV, da Cunha AS, Sichieri R. Trends in overweight amongadolescentslivinginthepoorestandrichestregionsof Brazil.AmJPublicHealth.2004;94:1544---8.
20.MelodosSantosM,PassosOliveiraV,TeixeiraLimaSM,Climaco CruzKJ,SoaresdeOliveiraAR,SoaresSeveroJ.Effectiveness ofaneducationalinterventiontoreducetheconsumptionof high-caloriefoodsinpublicschoolchildreninTeresina,Piaui (Brazil).NutrHosp.2015;32:622---6.
21.KatzDL.School-basedinterventionsforhealthpromotionand weightcontrol:notjustwaitingontheworldtochange.Annu RevPublicHealth.2009;30:253---72.
22.Fung C, Kuhle S, Lu C, Purcell M, Schwartz M, Storey K, etal.Frombestpracticetonextpractice:theeffectivenessof school-basedhealthpromotioninimprovinghealthyeatingand physicalactivityandpreventingchildhoodobesity.IntJBehav NutrPhysAct.2012;9:27.
23.Coleman KJ,ShordonM,CaparosaSL, PomichowskiME, Dze-waltowskiDA.Thehealthyoptionsfornutritionenvironments inschools(HealthyONES)grouprandomizedtrial:using imple-mentationmodelstochangenutritionpolicyandenvironments inlowincomeschools.IntJBehavNutrPhysAct.2012;9:80.
24.BerwickDM.Aprimeronleadingtheimprovementofsystems. BMJ.1996;312:619---22.
25.LangleyGJ,MoenR,NolanKM,NolanTW,NormanCL,Provost LP.Theimprovementguide:apracticalaproachtoenhancing organizationalperformance.2ndedSanFrancisco:Wiley Desk-topEditions;2009.
26.FosterGD,ShermanS,BorradaileKE,GrundyKM,VanderVeur SS,NachmaniJ,etal.Apolicy-basedschoolinterventionto pre-ventoverweightandobesity.Pediatrics.2008;121:e794---802.
27.Katz DL, Katz CS, Treu JA, Reynolds J, Njike V, Walker J, etal.Teachinghealthfulfoodchoicestoelementaryschool stu-dentsandtheirparents:thenutritiondetectivesprogram.JSch Health.2011;81:21---8.
28.JaimePC,LockK.Doschoolbasedfoodandnutritionpolicies improvedietandreduceobesity?PrevMed.2009;48:45---53.
29.Makingithappen:schoolnutritionsuccessstoriesUSA:
Depart-mentofHealth and HumanServices 2005. [citedNov2015].
Availablefrom:http://www.studentstakingcharge.org.
30.Evans WD, Christoffel KK, Necheles JW, Becker AB. Social marketingasachildhoodobesitypreventionstrategy.Obesity (SilverSpring).2010;18Suppl1:S23---6.
31.Services:TFoCP.Theguidetocommunitypreventiveservices.
New York, Oxford; 2005. [cited Nov 2015]. Available from:
http://www.thecommunityguide.org.
32.TyboutASB.Brandpositioning.In:TyboutA,CalkinsT,editors. Kelloggonbranding.NewYork:JohnWileyandSons;2005.
33.HawkesC,SmithTG,JewellJ,WardleJ,HammondRA,Friel S,et al. Smartfood policiesfor obesity prevention.Lancet. 2015;385:2410---21.
34.KainJ,UauyR,ConchaF,LeytonB,BustosN,SalazarG,etal. School-basedobesitypreventioninterventionsforChilean chil-drenduringthepastdecades:lessonslearned.AdvNutr.2012;3, 616S-21S.
35.Gordon-LarsenP,GriffithsP,Bentley ME, WardDS, Kelsey K, ShieldsK,etal.Barrierstophysicalactivity:qualitativedataon caregiver-daughterperceptionsandpractices.AmJPrevMed. 2004;27:218---23.
36.IrwinJD,HeM,BouckLM,TuckerP,PollettGL.Preschoolers’ physicalactivitybehaviours:parents’perspectives.CanJPublic Health.2005;96(4):299---303.
37.ThompsonJL,DavisSM,GittelsohnJ,GoingS,BecentiA, Met-calfeL, et al. Patterns ofphysical activity among American Indianchildren:anassessmentofbarriersandsupport.J Com-munityHealth.2001;26:423---45.
38.SonnevilleKR,LaPelleN,TaverasEM,GillmanMW,ProsserLA. Economicandotherbarrierstoadoptingrecommendationsto preventchildhoodobesity:resultsofafocusgroupstudywith parents.BMCPediatr.2009;9:81.
39.CullenKW,HartsteinJ,ReynoldsKD,VuM,ResnicowK,Greene N,etal.Improvingtheschoolfoodenvironment:resultsfroma pilotstudyinmiddleschools.JAmDietAssoc.2007;107:484---9.
40.VecchiarelliS,TakayanagiS,NeumannC.Students’perceptions oftheimpactofnutritionpoliciesondietarybehaviors.JSch Health.2006;76:525---31,quiz40-2.
41.French S. Pricing effects on food choices. J Nutr. 2003;133:S841---3.
42.WellsL,NelsonM.TheNationalSchoolFruitSchemeproduces short-termbutnotlonger-termincreasesinfruitconsumption inprimaryschoolchildren.BrJNutr.2005;93:537---42.
43.Kamath CC, Vickers KS, Ehrlich A, McGovern L, Johnson J, SinghalV, et al. Clinicalreview: behavioral interventions to preventchildhoodobesity:asystematicreviewand metaanal-ysesof randomizedtrials.JClinEndocrinol Metab.2008;93: 4606---15.
44.NaderPR,HuangTT,GahaganS,KumanyikaS,HammondRA, ChristoffelKK.Nextstepsinobesityprevention:alteringearly lifesystemstosupporthealthyparents,infants,andtoddlers. ChildObes.2012;8:195---204.
45.HollisJL,Williams AJ,Sutherland R,Campbell E,Nathan N, Wolfenden L, et al. A systematic review and meta-analysis of moderate-to-vigorous physical activity levels in elemen-tary school physical education lessons. Prev Med. 2015;86: 34---54.
46.Efrat MW. Exploring effective strategies for increasing the amountofmoderate-to-vigorousphysicalactivitychildren accu-mulateduringrecess:aquasi-experimentalinterventionstudy. JSchHealth.2013;83:265---72.
48.Brown T, Summerbell C. Systematic review of school-based interventionsthatfocusonchangingdietaryintakeand phys-ical activity levels to prevent childhood obesity: an update to the obesity guidance produced by the National Insti-tutefor Health and Clinical Excellence.Obes Rev.2009;10: 110---41.
49.DobbinsM, Husson H, DeCorbyK, LaRocca RL. School-based physicalactivityprogramsforpromotingphysicalactivityand fitness in children and adolescents aged 6 to 18. Cochrane DatabaseSystRev.2013;2:CD007651.
50.LavelleHV, MackayDF,PellJP. Systematicreviewand meta-analysis of school-based interventions to reduce body mass index.JPublicHealth(Oxf).2012;34:360---9.
51.WatersE,deSilva-SanigorskiA,HallBJ,BrownT,CampbellKJ, GaoY,etal.Interventionsforpreventingobesityinchildren. CochraneDatabaseSystRev.2011:CD001871.
52.DobbinsM,DeCorbyK,RobesonP,HussonH,TirilisD. School-basedphysicalactivityprogramsforpromotingphysicalactivity andfitness inchildrenandadolescentsaged 6---18. Cochrane DatabaseSystRev.2009:CD007651.
53.SweetM.Childhoodobesitycanbeprevented,saysCochrane. BMJ.2011;343:d8014.
54.WangY,CaiL,WuY,WilsonRF,WestonC,FawoleO,etal.What childhoodobesitypreventionprogrammeswork?Asystematic reviewandmeta-analysis.ObesRev.2015;16:547---65.
55.Hills AP, Dengel DR, Lubans DR. Supporting public health priorities:recommendationsfor physicaleducationand phys-ical activity promotion in schools. Prog Cardiovasc Dis. 2015;57:368---74.
56.NgM,FlemingT,RobinsonM,ThomsonB,GraetzN,Margono C,et al. Global,regional, and national prevalence of over-weightand obesity inchildrenand adultsduring1980---2013: a systematicanalysisfortheGlobal BurdenofDiseaseStudy 2013.Lancet.2014;384:766---81.
57.Herscovici CR, Kovalskys I.Childhood Obesity --- A reviewof school-basedpreventiveinterventions---FindingsfromSALTEN, a pilotintervention designed to improve healthy eating and recreational physical activity in publicschools of Argentina. RevistaMexicanadeTranstornosAlimentario.2015;6:143---51.