www.jped.com.br
REVIEW
ARTICLE
Association
between
nutritional
status
and
outcomes
in
critically-ill
pediatric
patients
---
a
systematic
review
夽
Caroline
A.D.
Costa
a,b,∗,
Cristian
T.
Tonial
a,b,
Pedro
Celiny
R.
Garcia
a,baPontifíciaUniversidadeCatólicadoRioGrandedoSul(PUC-RS),PortoAlegre,RS,Brazil
bPostgraduatePrograminPediatricsandChildren’sHealth,HospitalSãoLucas,PontifíciaUniversidadeCatólicadoRioGrande
doSul(PUC-RS),PortoAlegre,RS,Brazil
Received24June2015;accepted19August2015 Availableonline6February2016
KEYWORDS
Nutritionalstatus; Pediatricintensive careunit;
Mortality; Lengthofstay; Mechanical ventilation
Abstract
Objectives: Tosystematically reviewtheevidence aboutthe impactofnutritional statusin
critically-ill pediatricpatients onthefollowing outcomesduringhospitalizationinpediatric
intensivecareunits:lengthofhospitalstay,needformechanicalventilation,andmortality.
Datasource:Thesearchwascarriedoutinthefollowingdatabases:Lilacs(LatinAmericanand
CaribbeanHealthSciences),MEDLINE(NationalLibraryofMedicineUnitedStates)andEmbase
(ElsevierDatabase).Nofilterswereselected.
Results: Atotalofsevenrelevantarticlesaboutthesubjectwereincluded.The publication
periodwasbetween1982and2012.Allarticlesassessedthenutritionalstatusofpatientson
admissionatpediatricintensivecareunitsandcorrelatedittoatleastoneassessedoutcome.A
methodologicalqualityquestionnairecreatedbytheauthorswasapplied,whichwasbasedon
somereferencesandtheresearchers’experience.Allincludedstudiesmetthequalitycriteria,
butonlyfourmetalltheitems.
Conclusion: The studiesincludedinthisreview suggestthatnutritional depletion is
associ-atedwithworseoutcomesinpediatricintensivecareunits.However,studiesarescarceand
those existing show no methodological homogeneity, especially regardingnutritional status
assessmentandclassification methods.Contemporaryandwell-designedstudiesareneeded
inordertoproperlyassesstheassociationbetweenchildren’snutritionalstatusanditsimpact
onoutcomesofthesepatients.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:CostaCA,TonialCT,GarciaPC.Associationbetweennutritionalstatusandoutcomesincritically-illpediatric patients---asystematicreview.JPediatr(RioJ).2016;92:223---9.
∗Correspondingauthor.
E-mails:[email protected],[email protected](C.A.D.Costa).
http://dx.doi.org/10.1016/j.jped.2015.09.005
224 CostaCAetal.
PALAVRAS-CHAVE
Estadonutricional; UnidadedeTerapia IntensivaPediátrica; Mortalidade;
Tempodeinternac¸ão; Ventilac¸ãomecânica
Relac¸ãodoestadonutricionalcomdesfechosempacientespediátricoscríticos ---Revisãosistemática
Resumo
Objetivos: Revisar,deformasistemática,asevidênciasacercadoimpactodoestadonutricional
depacientespediátricoscríticossobreosseguintesdesfechosduranteainternac¸ãoemUnidades
deTerapiaIntensivaPediátrica:Tempodeinternac¸ão,necessidadedeventilac¸ãomecânicae
mortalidade.
Fontededados: Abuscafoirealizadanasseguintesbasesdedados:Lilacs(Literatura
Latino-AmericanaedoCaribeemCiênciasdaSaúde),Medline(NationalLibraryofMedicineEstados
Unidos),eEmbase(ElsevierBasedeDados).Nãohouveselec¸ãodefiltros.
Resultados: Foramincluídos seteartigosrelevantes sobreo tema.Operíodode publicac¸ão
variou entre1982e2012. Todosavaliamo estadonutricionaldepacientesnomomentoda
internac¸ãoemTerapiaIntensivaPediátricaerelacionamcompelomenosumdesfechoestudado.
Foiaplicadoumquestionáriodequalidademetodológicacriadopelosautores.Elefoibaseado
emalgumasreferênciaseexperiênciadospesquisadores.Todososestudosincluídosalcanc¸aram
oscritériosdequalidade,porémapenasquatro,atenderamàtodosositens.
Conclusão: Osestudosincluídosnestarevisãosugeremqueadeplec¸ãodoestadonutricional
estárelacionadocompioresdesfechosemTerapiaIntensivaPediátrica.Porémosestudossão
escassos,eosexistentes,não temuniformidademetodológica,em especialnosmétodosde
avaliac¸ãoeclassificac¸ãodoestadonutricional.Sãonecessáriosestudosatuaisebemdelineados
comoobjetivodeavaliaradequadamenteestarelac¸ãoentreoestadonutricionaldecrianc¸as
esuarepercussãonosdesfechosdestespacientes.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos
reservados.
Introduction
Critically-illpediatricpatientscanhaveanumberoforganic alterations,leadingtoa state ofmetabolic stress. There-fore,inmanycases,thenutritionalneedsofthesepatients canbeincreased.1Theinadequatesupplyofnutrientscan
resultinworsenednutritionalstateleadingtomalnutrition,
whichhasbeenassociatedinseveralstudieswithincreased
mortalityandhospitalizationtime,aswellasahigher
num-beroforgandysfunctionsandcomplications.2,3Theanalysis
ofthecumulativeproteincaloriedeficitinchildrenadmitted
toapediatricintensivecareunit(PICU)intheNetherlands
showed a significant association between this deficit and
reducedZ-scoreforweightandarmcircumference.4
Therearemanybarrierstoadequatenutritionalsupply
in thePICU, which contributesto nutritionalstatus
dete-rioration. Among them, the most often mentioned in the
literatureare:gastrointestinaldisorders,pausefor
proce-dures,andfluidrestriction;however,towhatextentthese
barrierscanbepreventableisamatterofdebate.5,6
This groupof critically-illpatientsis extremely
vulner-able.Theirnutritionalstatusatadmissionanditspossible
deteriorationduring hospitalization can bea predictor of
worseoutcomes.7---9
This study aimed to systematically review the
evi-denceabouttheimpactofnutritionalstatusincritically-ill
pediatric patients onthe following outcomesduring PICU
hospitalization:lengthofhospitalstay,needformechanical
ventilation(MV),andmortality.
Methods
Datasource
A research protocol wasdeveloped, in which the authors definedtheaim,keywords,searchstrategies,database def-inition,inclusionandexclusioncriteria,andmethodologyto beusedbythereviewers.Thesearchwascarriedoutinthe followingdatabases:Lilacs,MedlineandEmbase.Nofilters wereselected.
Descriptors
The descriptorsusedforthesearchwere:Nutritional Sta-tus(EstadoNutricional)andIntensiveCareUnitsPediatric
(UnidadedeTerapiaIntensivaPediátrica).Thecombination of descriptors for the Lilacsand MEDLINE databaseswas: ‘‘NutritionalStatus’’AND‘‘IntensiveCareUnitsPediatric’’
For the Embasedatabase, the following combination was used:‘‘NutritionalStatus’’AND((IntensiveCareUnitsAND Pediatric)OR(IntensiveCareUnitsANDChild*)).
Inclusioncriteria
atleastoneofthefollowingoutcomes:mortality,hospital lengthofstay,andneedforand/ortimeofMV.
Exclusioncriteria
Studiesconductedinaneonatalintensivecareunit,articles withoutfulltext,reviewarticles,letterstotheeditor,case reports, andstudiesthat didnotaddress theissue by not performingnutritionalassessment and associatingit toat leastoneoutcomeofinterestwereexcluded.
Studyselection
Thesearchwasperformedbyoneinvestigatorusingthe pre-defined keywords.The initial selection wasperformed by twoblindedresearchers,incompliancewiththe inclusion andexclusioncriteriadescribedinthestudyprotocol.
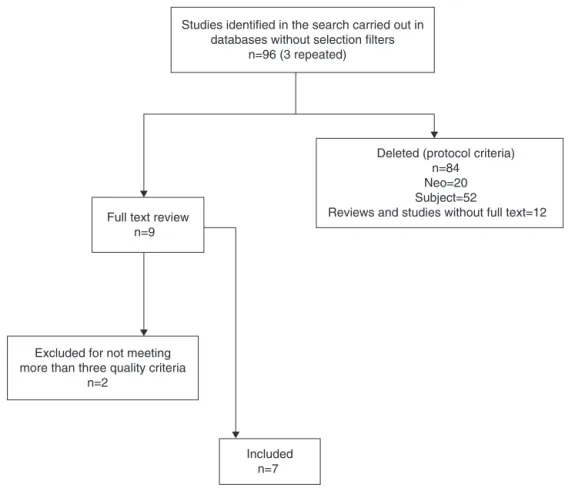
Firstly, articleswerescreened byreading thetitle and abstract. When the title and the abstract did not offer enough clarification, the authors searched for the full article. The disagreements were resolved by consensus, togetherwith athird researcher. After that,the full text of all articlesincluded wasobtained and thequality pro-tocolcreatedbytheauthorswasapplied.Fig.1showsthe
stepsofstudiesselectionuntilthefinalinclusion.
Study
quality
assessment
Afterthe studies were selected and their full texts were obtained, the methodological quality questionnaire was applied,which wascreated basedon tworeferences and theresearchers’experience.10,11Tocontemplatethe
techni-calissues,theauthorsconsideredtherecommendationson
nutritionalstatusassessmentandclassificationoftheWorld
HealthOrganization(WHO),accordingtotheyearofstudy
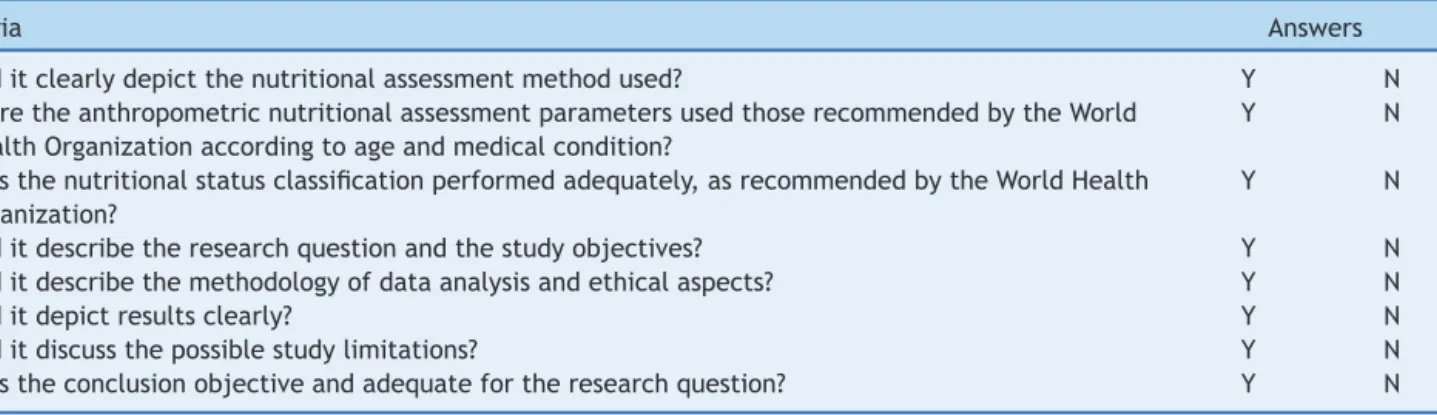
publication.Thequestionsusedinthequalityprotocolare
showninTable1.
Results
Descriptionofincludedstudies
Seven relevant articles on the topic were included. The publicationperiod ranged from 1982 to 2012. All studies assessedthenutritionalstatusofpatientsonadmissionat thePICUandcorrelatedittoatleastoneassessedoutcome. Threestudies assessedgroups ofpatientsinthePICUwith specific health conditions(ketoacidosis, hyper- and hypo-glycemia,and livertransplant), while the othersassessed nutritionalprofileasaprimaryor secondaryobjectiveand correlatedittotheoutcomes.
All included studies met the quality criteria, but only fourmet allitems. Nonetheless, thosethat didnot meet
Studies identified in the search carried out in databases without selection filters
n=96 (3 repeated)
Deleted (protocol criteria) n=84
Neo=20 Subject=52
Reviews and studies without full text=12 Full text review
n=9
Excluded for not meeting more than three quality criteria
n=2
Included n=7
226 CostaCAetal.
Table1 Qualitycriteria.
Criteria Answers
1.Diditclearlydepictthenutritionalassessmentmethodused? Y N
2.WeretheanthropometricnutritionalassessmentparametersusedthoserecommendedbytheWorld
HealthOrganizationaccordingtoageandmedicalcondition?
Y N
3.Wasthenutritionalstatusclassificationperformedadequately,asrecommendedbytheWorldHealth
Organization?
Y N
4.Diditdescribetheresearchquestionandthestudyobjectives? Y N
5.Diditdescribethemethodologyofdataanalysisandethicalaspects? Y N
6.Diditdepictresultsclearly? Y N
7.Diditdiscussthepossiblestudylimitations? Y N
8.Wastheconclusionobjectiveandadequatefortheresearchquestion? Y N
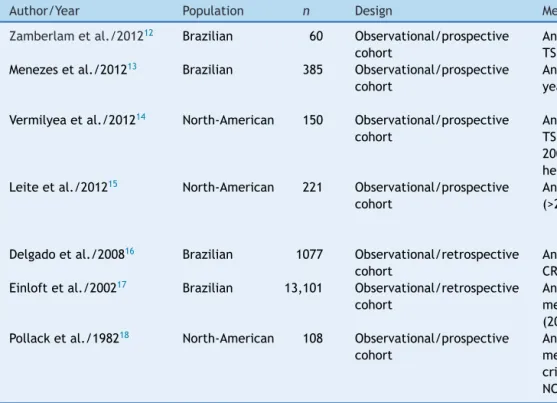
uptothreeitems were included, astheauthors believed theycontributedasevidenceforthediscussionsaboutthe studiedsubject.Table 2showsasummaryof theincluded
studies.12---18
Discussion
Nutritionalstatusassessmentofcritically-ill pediatricpatients
Oneofthegreatdifficultiesinthenutritionalassessmentof critically-illpatientsischoosingthebestmethod,asthere is no evidence to guidethe decision. The difficulties are foundindifferenttypesofassessment,whetherduetothe patient’sclinical condition, thehemodynamic alterations, body composition modification or even the lack of staff awarenessonthe importanceof appropriately performing datameasurement.Theseaspectsmakeitdifficultto stan-dardizethe assessment and qualityof studies carriedout withthesepatients.19
Weightandheightarethemeasurementsmostoftenused
and,basedonthese,thefollowingindicescanbeobtained:
W/A, H/A, W/H, and body mass index (BMI)/A. In 2006,
theWHOreleasednewgrowthchartsdevelopedfrom
sam-ples from six countries, among them Brazil. The Z-score
andpercentilecurveswerecreated. Thesecurvesinclude
theevaluationofchildrenaged0---5years.20 Subsequently,
duetotheneedtocreatenewrecommendationstandards
for children older than 5 years, the WHO reassessed the
datafromtheNationalCenterforHealthStatistics(NCHS,
1977), unifying it with the 2006 survey data, thus
pub-lishing new curves for children aged 5---19 years, also in
Z-scoresandpercentiles.21Thesecurvesarerecommended
forworldwideuseintheageranges,regardlessof raceor
ethnicity.22
Theassessmentthroughskinfolds,circumferences,orby
electricalbioimpedancemaybegoodanthropometric
indi-catorsforchildren,providingdataonthereservesoffatand
leanmass.However,thispracticeisyettobeestablishedfor
useinPICUs.23---25
Laboratoryparameterscanalsobeusedtocomplement
the nutritional assessment and/or monitor the
effective-ness of the established nutritional therapy. In general,
the parameters most often used are serum protein
lev-elsandimmunologicalassessment.However,incritically-ill
patients,itismorecomplextousethem,duetotheorganic
alterationscausedbythedisease.26
Analyzingthestudiesincludedinthissystematicreview,
the authors confirmed the abovementioned difficulties. It
wasobservedthattherewasnohomogeneityinthechoice
of methodsandparametersusedtoassessnutritional
sta-tus, even in studies with very similar objectives. Most
of them mention aslimitation thedifficulty of measuring
anthropometricdatainthispopulation.Weightandheight
measurementwasperformedinallstudies.Regardingother
less common assessment methods, as mentioned before,
onlytwostudiesusedlaboratoryassessment ofnutritional
status andthreeperformed themeasurement ofskinfolds
andcircumferences.
Mechanicalventilation
Respiratorydysfunctionisoftenconsideredthemost preva-lent organ dysfunction as cause of patient admission in epidemiological studies carried out in the PICU.8,27,28 The
evolutionofthesepatientscanbeunfavorable,leadingto
respiratory failure and need for MV. The nutritional
sta-tusalterationcanleadtoproteincatabolism,withfat-free
massdepletion,whichreducesrespiratorymusclestrength,
maximum voluntary ventilation, and vital capacity, and
also affects the lungs and the immune function,
increas-ing the risk of respiratory infections.9,29 Studies indicate
that this nutritionalstatus alteration anddepletion often
occurduringhospitalizationinthePICU,witha
multifacto-rialcause.2---4,6
Inadditiontotheinfluenceofnutritionalstatusonthe
need for MV, studies show that this depletion can also
be associated with the difficulty in MV weaning, as well
as its chronic use.30---32 In a study in adults with chronic
pulmonary disease using VM at home, Hitzl et al.
com-paredtheassessmentofnutritionalstatusthroughelectrical
bioimpedance (BIA)withBMI,concludingthatthe fat-free
massvaluesobtainedbyBIAwerepredictiveof survivalin
thesepatients.32SimilarfindingswerereportedbyMartinez
et al., whoassessed body composition by BIA in children
usingVMathomeandconcludedthatthesechildrenhada
highprevalenceofmalnutritionandimportantfat-freemass
depletion.33
Amongthestudiesselectedforthisreview,twousedMV
asone ofthe assessedoutcomes, focusingon
status
and
clinical
outcomes
227
Table2 Summaryofincludedstudies.
Author/Year Population n Design Method(s)ofnutritionalstatusAssessment/Classific. Outcomes
Zamberlametal./201212 Brazilian 60 Observational/prospective
cohort
Anthropometrics:W/A,H/A,W/H,BMI/A,AC/A, TSF/A/WHO2006and2007
Mortality/timeof hospitalization Menezesetal./201213 Brazilian 385 Observational/prospective
cohort
Anthropometrics:W/A(upto2years)andBMI/A(>2 years)/WHO2006and2007
Mortality/timeof hospitalization/Timeof MV
Vermilyeaetal./201214 North-American 150 Observational/prospective
cohort
Anthropometrics:W/A,H/A,W/H,BMI/A, TSF/A,CMA/A,CP/A/WHO2006and 2007/Laboratory:TotalWBC,albuminand hemoglobincount/SubjectiveAssessmentProtocol
Timeofhospitalization
Leiteetal./201215 North-American 221 Observational/prospective
cohort
Anthropometrics:W/A(upto2years),H/A,BMI/A (>2years)/WHO2006and2007)
Mortality/timeof hospitalization//MV-free
time Delgadoetal./200816 Brazilian 1077 Observational/retrospective
cohort
Anthropometrics:W/A,W/H,CMA/I/Laboratory: CRP,albumin,andIL6
Mortality/timeof hospitalization Einloftetal./200217 Brazilian 13,101 Observational/retrospective
cohort
Anthropometrics:Weightandheight
measurement/Classific.accordingtoGomezcriteria (2000)
Mortality
Pollacketal./198218 North-American 108 Observational/prospective
cohort
Anthropometrics:Weightandheight
measurement/Classific.accordingtoWaterlow criteria(1973),TSFandAC/Classific.accordingto NCHS
Timeofhospitalization
228 CostaCAetal.
highprevalenceofmalnutritionintheirsample,indicating this variableas one that showed a significant association with MV time>5 days (p=0.02).13 Leite et al. evaluated
patients admitted to the PICU who had blood glucose
alterations, using MV-free time as one of the secondary
outcomes.Itwasverifiedthatmalnourishedpatients with
hypoglycemiaremainedMV-freeforashorterperiodoftime
(p<0.01).15 An agreement between the findings of these
studiescan beobserved, asboth indicatethatnutritional
statusinfluencesMVtime.
PICUlengthofstay
The length of stay of a patient in the PICU may reflect diseaseseverity,qualityofcare,andunitprocedures,and italsohasan importantimpactonhospitalcosts.34,35 The
authorsemphasizethatthisoutcomevariable,togetherwith
mortality, is one of the most criticalstudied in pediatric
patients.Itwasusedinsixofthesevenselectedstudiesin
thepresentsample.
Oneoftheauthorsthatcomparedthenutritionalstatus
withhospital length of stay is Pollack, in a study carried
outin1982;thiswastheonlyoutcomevariableusedinthe
research.This is the oldeststudy included in thisreview,
butitisareferenceoftenmentionedbyresearchers
inter-estedin thesubject. Nearly half of itssample (47%) was
malnourishedand showed depletion of fat tissue, aswell
asof fat-freemass. However,that studyfailedto
demon-strateasignificantlylongerlengthofstay whencompared
withpatientswithnormalweight.18
Aiming to assess the association of malnutrition and
inflammatoryresponsewithoutcomesincritically-ill
pedi-atricpatients,Delgadoetal.foundnosignificantdifference
inlengthofstayamongseverelymalnourished,moderately
malnourished,eutrophic patients.16 Vermilyeaet al.
con-ductedastudytovalidateanoverallsubjectiveevaluation
methodforcritically-illpediatricpatients.Theycompared
the tool with anthropometric and laboratory evaluation,
subsequently correlating them with the outcomes. Their
findings corroborate the studies by Pollack and Delgado,
demonstrating no significant association between
nutri-tionalstatusassessmentperformedwiththethreetoolsand
patients’ length of stay,thus raisingthe discussion about
inconsistenciesintheexistingdatathatassociate
malnutri-tionwithlengthofstay.14
Zamberlametal.studied apopulationof patients
sub-mittedtolivertransplant,evaluatingthenutritionalstatus
andassociatingit withoutcomes.Regardingthe lengthof
stayofthesepatients,theyobservedthatthosewith
mus-cle depletion remained longer at the PICU. Leite et al.
assessed a population of patients with abnormal glucose
levelsandfound that hypoglycemia,when combinedwith
malnutrition,wasassociatedwithincreasedhospitalization
(p<0.01).15Menezesetal.alsoobservedthatmalnutrition
isariskfactorforprolongedhospitalization(p=0.04),
mak-ingitclearinthestatisticalmethodologythatthisresultwas
obtainedattheunivariateanalysis,whereasthe
multivari-ateanalysis showedno significant association. Differently
fromwhatwasobservedinthepreviouslydiscussedoutcome
variable,theabovementionedstudieshavenohomogeneity
regardingtheirfindingsandconclusions.
Mortality
Deathisthemainandmostfearedprimaryoutcome;itsrisk is the mainreason for hospitalizationin aPICU. The pre-viouslydiscussed outcomesmaybethecomplications that precede death. The mortality risk assessment of patients admittedtothePICUcanbemeasured throughprognostic scores,whicharewidelyusedinalmostallstudies evaluat-ingtheassociationbetweennutritionalstatusandmortality in thisgroupof patients.The mostcommonly usedscores arethePediatricRiskofMortality(PRISM,1988),Pediatric IndexofMortality(PIM,1997),andPediatricLogisticOrgan Dysfunction(PELOD,1999).Inthepresentsample,all stud-iesthatusedmortalityasoutcomeincludedaseverityscore, mostlyoneoftheabovementionedscores.
Only two studies of those selected for the review did notusethisoutcome;thestudyofVermilyeaonlyassessed patientseverityrisk throughPIM2 andPRISMscores. Simi-larlytolengthofstay,mortalityshowedtobeavariablewith inconsistentevidenceofassociationwiththenutritional sta-tus, asthreeof thefivestudies thatwere includedfound no significant association between these variables.12,13,16
Despitethisfinding,allstudiesdiscussthisresult,pointing
outother studiesthatfound anassociation and
emphasiz-ingtheimportanceofnutritionalstatusassessmentandits
possibleassociationwithworseoutcomes.
Thetwostudiesthatfoundanassociationbetween
nutri-tionalstatusandmortalitywerethosebyEinloftetal.,and
Leiteetal.The firstdescribedhigh mortalityamong
mal-nourishedpatients(p<0.001),indicatingmalnutritionasa
determiningfactorforthisoutcome.17 Inthesecondstudy,
mortalitywasthethirdoutcomewithasignificant
associa-tioninhypoglycemicpatients,whenthiscomplicationwas
associatedwithmalnutrition(p<0.05).15
Searchstrategyandlimitations
The present search wasquite comprehensive and initially included studies of several populations. However, after reviewing,applyingtheinclusionandexclusioncriteria,and performing thequality assessment, only studies in Brazil-ianandNorth-Americanpopulationsremained.Theauthors considerthatthisaspectlimitsamoreconsistentconclusion abouttheassessedresearchquestion.
Conclusion
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
ToCAPES(Coordenac¸ãodeAperfeic¸oamentodePessoalde NívelSuperior),fortheMaster’sDegreeScholarship.
References
1.SkillmanHE,WischmeyerPE.Nutritiontherapyincriticallyill infantsandchildren.JParenterEnteralNutr.2008;32:520---34. 2.CahillNE,DhaliwalR,DayAG,JiangX,HeylandDK.Nutrition therapyin thecritical care setting: what is bestachievable practice.Aninternationalmulticenterobservationalstudy.Crit CareMed.2010;38:395---401.
3.MehtaNM,BechardLJ,LeavittK,DuganC.Cumulativeenergy imbalanceinthepediatricintensivecareunit:roleoftargeted indirectcalorimetry.JParenterEnteralNutr.2009;3:336---44. 4.HulstJM,VanGoudoeverJB,ZimmermannLJ,HopWC,Albers
MJ,TibboelD,etal.Theeffectofcumulativeenergyand pro-teindeficiencyonanthropometricparametersinapediatricICU population.ClinNutr.2004;23:1381---9.
5.MehtaNM,McAleerD,HamiltonS,NaplesE,LeavittK,Mitchell P,etal.Challengestooptimalenteralnutritionina multidis-ciplinarypediatricintensivecareunit.JPENJParenterEnteral Nutr.2010;34:38---45.
6.Rogers EJ, Gilbertson HR, Heine RG, Henning R. Barriers to adequate nutrition in critically ill children. Nutrition. 2003;19:865---8.
7.CorullónJL.PerfilepidemiológicodeumaUTIpediátricanosul doBrasil.[Dissertation].PortoAlegre(RS):Pontifícia Universi-dadeCatólicadoRioGrandedoSul;2007.
8.DrescherD.PerfilNutricionalearelac¸ãocomoestadodesaúde emumaUTIPediátrica.[Dissertation].PortoAlegre(RS): Pon-tifíciaUniversidadeCatólicadoRioGrandedoSul;2011. 9.MotaEM, GarciaPCR,PivaJP,FritscherCC.Theinfluenceof
poornutritiononthenecessityofmechanicalventilationamong childrenadmittedtothepediatricintensivecareunit.JPediatr (RioJ).2002;78:146---52.
10.ArmstrongR,WatersE,JacksonN,OliverS,PopayJ,Shepherd J,etal.Guidelinesforsystematicreviewsofhealthpromotion andpublichealthinterventions.Australia:Melbourne Univer-sity;2007.
11.MuradMH,MontoriVM,LoannidisJPA,JaeschkeR,Devereaux PJ,PrasadK,etal.Howtoreadasystematicreviewand meta-analysisandapplytheresultstopatientcareusers’guidesto themedicalliterature.JAMA.2014;312:171---9.
12.Zamberlam P,Leone C,Tannuri U, CarvalhoWB, Delago AL. Nutritionalriskandanthropometricevaluationinpediatricliver transplantation.Clinics.2012;67:1387---92.
13.MenezesFS, Leite HP,Nogueira PC.Malnutrition as an inde-pendentpredictorofclinicaloutcomeincriticallyillchildren. Nutrition.2012;28:276---80.
14.VermilyeaS, Slicker J, El-Chamas K, Sultan M, Dasqupta M, HoffmannRG,etal.Subjectiveglobalassessmentincritically children.JParenterEnterNutr.2013;37:659---66.
15.LeiteHP,LimaLF,deOliveiraIglesiasSB,PachecoJC,de Car-valhoWB.Malnutritionmayworsentheprognosisofcritically illchildrenwithhyperglycemiaandhypoglycemia.JParenter EnterNutr.2012;37:335---41.
16.DelgadoAF,OkayTS,LeoneC,NicholsB,DelNegroGM,VazFA. Hospitalmalnutritionandinflammatoryresponseincriticallyill
childrenandadolescentsadmittedtoatertiaryintensivecare unit.Clinics.2008;63:357---62.
17.EinloftPR,GarciaPC,PivaJP,BrunoF,KipperDJ,FioriRM.Perfil epidemiológicodedezesseisanosdeumaunidadedeterapia intensivapediátrica.RevSaldePublica.2002;36:728---33. 18.Pollack MM, Wiley JS, KanterR. Malnutrition in critically ill
infantsandchildren.JParenterEnterNutr.1982;6:20---4. 19.FeferbaunR,DelagoAF,ZamberlamP,LeoneC.Challengesof
nutritional assessment in pediatric ICU.Curr Opin Clin Nutr MetabCare.2009;12:245---50.
20.Who MulticentreGrowth Reference StudyGroup.WHO Child GrowthStandardsbasedonlength/height,weightandage.Acta PaediatrSuppl.2006;450:76---85.
21.OnisM,OnyangoA,BorghiE,SiyamA,NishidaaC,Siekmanna J. Developmentofa WHO growth reference for school-aged childrenand adolescents. BullWorld HealthOrgan. 2007;85: 660---7.
22.NataleV,RajagopalanA.Worldwidevariationinhumangrowth andtheWorldHealthOrganizationgrowthstandards:a system-aticreview.BMJOpen.2014;4:e003735.
23.Telles R, Filho A. O uso da antropometria comométodo de avaliac¸ãodacomposic¸ãocorporalempediatria.RevCiencMed. 2003;12:351---63.
24.Sant’Anna M,PrioreS, FranceschiniS. Métodosde avaliac¸ão da composic¸ão corporal em crianc¸as. Rev Paul Pediatr. 2009;27:315---21.
25.Cômodo A, DiasA, Tomaz B,Filho A, Werustsky C,RibasD, etal.Utilizac¸ãodabioimpedânciaparaavaliac¸ãodamassa cor-pórea.ProjetoDiretrizes: Associac¸ãoBrasileirade Nutrologia SociedadeBrasileiradeNutric¸ãoParenteraleEnteral;2009. 26.LeteurtreS,DuhamelA,GrandbastienB,Proulx F,CottingJ,
GottesmanR,etal.Dailyestimationoftheseverityof multi-pleorgandysfunctionsyndromeincriticallyillchildren.CMAJ. 2010;182:1181---7.
27.TyppoKV,Petersen NJ,HallmanDM,MarkovitzBP,Mariscalco MM.Day1multipleorgandysfunctionsyndromeisassociated withpoor functionaloutcome and mortalityin thepediatric intensivecareunit.PediatrCritCareMed.2009;10:562---70. 28.Ferreira IM, Verreschi IT, Goldstein RS, Zamel N, Brooks D,
JardimJR.Theinfluenceof6monthsoforalanabolicsteroids onbodymassandrespiratorymusclesinundernourishedCOPD patients.Chest.1998;114:19---28.
29.DoleyJ,MallampaliA,SanbdbergM.Nutritionmanagementfor thepatientrequiring prolonged mechanicalventilation. Nutr ClinPract.2011;26:232---41.
30.Ambrosio N, Clini E. Long-term mechanical ventilation and nutrition.RespirMed.2004;98:413---20.
31.BudweiserS,MeyerK,JorresRA,HeinemannF,WildPJ,Pfeifer M. Nutritional depletion and its relationship to respiratory impairment in patients with chronic respiratory failure due to COPD or restrictive thoracic diseases. Eur J Clin. Nutr. 2008;62:436---43.
32.Hitzl PA, Jorres RA, Heinemann F, Pfeifer M, Budweiser S. Nutritionalstatusin patientswithchronic respiratoryfailure receivinghomemechanicalventilation:impactonsurvival.Am JClinNutr.2010;29:65---71.
33.Martinez EE, Smallwood CD, Bechard LJ, Grahan RJ, Mehta NM.Metabolicassessmentandindividualizednutritionin chil-drendependentonmechanicalventilationathome.J.Pediatr. 2014;14:887---97.
34.Marcin JP, SlonimAD, PollackMM. Long-stay patients inthe pediatricintensivecareunit.CritCareMed.2001;29:652---7. 35.NamachivaiamP,TaylorA,MontaqueT,MoranK,BarrieJ,