www.jped.com.br
REVIEW
ARTICLE
Behavioral
and
neural
correlates
of
emotional
development:
typically
developing
infants
and
infants
of
depressed
and/or
anxious
mothers
夽
Juliana
A.
Porto
a,∗,
Magda
L.
Nunes
a,
Charles
A.
Nelson
baSchoolofMedicine,PontifíciaUniversidadeCatólicadoRioGrandedoSul(PUC-RS),PortoAlegre,RS,Brazil
bLaboratoriesofCognitiveNeuroscience,DivisionofDevelopmentalMedicine,BostonChildren’sHospital,HarvardMedical
School(HMS),Boston,UnitedStates
Received12November2015;accepted25November2015 Availableonline18March2016
KEYWORDS Infant;
Depressedmothers; Anxiety;
Face; Emotion; Behavior
Abstract
Objectives: To describe the main findings of studies of behavioral and neural correlates regardingthedevelopmentoffacialemotionprocessingduringthefirstyearoflifeintypically developinginfantsandinfantsofdepressedand/oranxiousmothers.
Sources: Comprehensive,non-systematicreviewoftheliteratureonstudiesaboutindividual differencesinfacialemotionprocessingbynewbornsandinfantsoverthefirstyearoflife. Summaryofthefindings: Maternalstressrelatedtodepressionandanxietyhasbeenassociated to atypical emotional processing and attentional behaviors inthe offspring. Recent neuro-physiologicalstudiesusingelectroencephalogramandevent-relatedpotentialshavebegunto shedlightonthepossiblemechanismsunderlyingsuchbehaviors.
Conclusions: Infants of depressed and/or anxious mothers have increased risk for several adverseoutcomesacrossthelifespan.Furtherneurobehavioralinvestigationsandthe promo-tionofclinicalanddevelopmentalresearchintegrationmighteventuallycontributetorefining screeningtools,improvingtreatment,andenablingprimarypreventioninterventionsfor chil-drenatrisk.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:PortoJA,NunesML,NelsonCA.Behavioralandneuralcorrelatesofemotionaldevelopment:typicallydeveloping infantsandinfantsofdepressedand/oranxiousmothers.JPediatr(RioJ).2016;92(3Suppl1):S14---22.
∗Correspondingauthor.
E-mail:[email protected](J.A.Porto).
http://dx.doi.org/10.1016/j.jped.2015.12.004
PALAVRAS-CHAVE Lactente;
MãesDeprimidas; Ansiedade; Face; Emoc¸ão; Comportamento
Basesneuraisecomportamentaisdodesenvolvimentoemocional:lactentes comdesenvolvimentotípicoelactentesfilhosdemãesdeprimidase/ouansiosas
Resumo
Objetivos: Descreverosprincipaisachadosdeestudosdecorrelac¸ãoentreocomportamentoe asbasesneuraisemrelac¸ãoaoprocessamentodeemoc¸õesfaciaisduranteoprimeiroanode vidadelactentescomdesenvolvimentotípicoelactentesdemãesdeprimidase/ouansiosas. Fontes: Análiseabrangenteenãosistemáticadaliteraturadeestudossobrediferenc¸as indi-viduaisnoprocessamentodeemoc¸õesfaciaisdeneonatoselactentesaolongodoprimeiroano devida.
Resumodosachados: Oestressematernorelacionadoàdepressãoeansiedadetemsido asso-ciado aalterac¸õesnoprocessamentoemocional enaalocac¸ãodaatenc¸ãodaprole.Estudos neurofisiológicosrecentesutilizandoelectroencefalogramaepotenciaisrelacionadosaeventos comec¸amaesclarecerospossíveismecanismosinerentesaessescomportamentos.
Conclusões: Lactentesfilhosdemãesdeprimidase/ouansiosastêmmaiorriscodeproblemas desaúdefísicaementaldurantetodavida.Oavanc¸odeestudosneurocomportamentaisea promoc¸ãodeintegrac¸ãoentreapesquisaclínicaededesenvolvimentopoderãocontribuirpara refinarasferramentasdetriagem,melhorarotratamentoepermitirintervenc¸õesdeprevenc¸ão primáriaparacrianc¸asemrisco.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
The abilitytorecognize andunderstandfacialexpressions ofemotionisafundamentalskillindailyinteractionswith others, and plays a particularly important role early in life,beforetheonsetoflanguage.1Facerecognitionisone
of the most salient cues for social interaction and affec-tivecommunication.Facialexpressionrecognitiondevelops graduallyduringinfancyandchildhood,andappearsto con-tinuetodevelopuntilearlyadulthood.2Duringthefirstyear
oflife,however,thedevelopmentofvisualorientationand thediscriminationofdifferentemotionsprogressesrapidly.3
Over thepast several decades,behavioral studies4---6 have
useddifferentmeasuresofvisualpreferencetoinferaspects ofrecognitionofemotionalfaces.Morerecently,new meth-odstoelucidatedistinctcorrelatesofbrainactivationhave provided significant contribution to the field.Two of the mostusedmethods,knownaselectroencephalogram(EEG) andevent-relatedpotentials(ERP),arereviewedhere.
Evidence has become available that stress exposure during pregnancy and the postnatal period leads to sev-eral long lasting detrimental outcomes in the offspring, includingbehaviorandcognitiveproblemsand neurodevel-opmental delay.7 Studies on maternal negative affective
states, including both depression and anxiety, indicate a detrimentaleffectonthechild’shealthanddevelopment, increasing the risk for a wide range of disorders such as low birth weight and preterm birth, cognitive and motor developmentaldelay,achievementdeficits,andpsychiatric disorders.8Infantsof depressedandanxiousmothershave
increasedvulnerabilitytocognitiveandemotionalproblems throughouttheirlifespan.7,8
Psychologicalstress,depression,andanxietyareclosely linkedandoftencoexist.7Approximately10---20%ofwomen
will exhibit symptoms of depression during pregnancy
and/or the postpartum period.7 Anxiety disorders in the
perinatalperiodhavereceivedmorescientificattentiononly recentlyandtheirprevalenceisstillunclear,yetestimates rangeashighas30%.9Theoutcomesofanxietyand
depres-sionareoftenstudiedtogether,asthesymptomsfrequently overlap,andtheircoexistenceisamarkerofseverity.9,10
The mechanisms between maternal negative affective statesandtheinfantoutcomesarestudiedboth inanimal and human clinical research. During pregnancy, maternal stress induces the dysregulation of the hypothalamic-pituitary-adrenocortical(HPA)system,elevatingthecortisol levelsandinducingsympatheticactivation withreleaseof catecholamines.7,9 The latter is associated to increased
uterineartery resistance, reducing the blood flow tothe fetus,withrestrictedinflowofoxygenandnutrients.10,11
The higher levelsof maternal cortisol adversely affect fetal brain development, possibly due to epigenetic dysregulationthroughalterationsinsynaptogenesisand neu-rotransmitterfunctions.11,12Thereisevidenceofdisruption
ofthefetalHPAsystem,withadversephysiologicaland bio-chemicaleffectsonthefetusandnewborn10thatcanpersist
throughout infancy, resulting in altered infant perception andbehavior.
In the postnatal period, maternal anxiety and depres-sion are related to less sensitive and inconsistent care when interacting with infants, providing suboptimal lev-elsofgeneralstimulation,anddisruptingthemother---child relationshipandtheformationofattachments.8,13
Accumu-lating evidenceindicates that the emotional environment of the infants’ daily experiences influences their devel-opmentaltrajectory of facialrecognition.14 Typically, the
mother is the most present person in an infant’s life, and the mother’s facial expressions are the most preva-lent in their experience.14 Mothers with depression and
facial expressions, and interact with infants in a with-drawnandmutedstyle.14,15Asaresult,infantsofdepressed
and/oranxiousmothershavesystematicallyatypicalsocial experiences compared to infants of healthy mothers.14,16
Understandingthepossiblemechanismsbywhichmaternal stressrelatedtodepressionandanxietyaffectsaninfant’s developmentisakeytofurtherdevelopingbetter interven-tionstrategiesandpreventionprograms.
Thisreviewexaminesthefindingsofstudiesabout mater-naldepressionandanxietyonfacerecognitionbytheinfant, bothregardingbehaviorandneurophysiology.Itbeginswith abriefreviewoftypicallydevelopinginfantsinordertoset thestageforthediscussionthatfollows,focusedoninfants ofdepressedand/oranxiousmothers.
Behavioralstudies
The majority of early emotional behavioral studies mea-sure looking time or visual preference. Visual fixation graduallydecreases toarepeatedly presentedstimulus,a phenomenonreferredtoashabituation(orfamiliarization); presentationofanewstimulusleadstorecoveryoflooking iftheinfantscandiscriminatetheoldfromthenewstimulus (dishabituation).3Thismeasurecanbeusedtoexaminethe
abilitytodiscriminatedifferentvisualstimuli,suchasone facefromanotheroroneobjectfromanother,orinthe cur-rentcontext,one facialexpression fromanother. Another methodto measure visual preference is the visual paired comparisonprocedure,inwhichlookingtimeanddurationof thefirstvisualfixationaremeasuredcomparingtwo expres-sionsseenatthesametime.3
Emotionalinformationcanalsobeinferredfrom multi-sensorymodalitiespresentedsimultaneously,suchasfacial andvocal stimuli.Multimodal studiesinvestigate how dif-ferent sensory stimuli may influence the processing and perceptionof each other.5,17 Forexample,studies
analyz-ingcongruentandincongruentface---voicepairs(i.e.,same ordifferentemotionpresentedbytheface---voice)attempt toelucidatehowemotionalinformationisintegrated.5
Furthermore,emotionalresponsesaremeasured observ-ing infants’ specific behavioral reactions, such as facial expressions, vocalization, imitation, or body movements. One commonly used paradigm is the still-face, in which themother(ortheexperimenter)isinstructedtoshowflat affect,mimickingemotionalunavailability.Infantstypically respond with distress, manifested by less motor activity, frowning,gazeaversionandcrying.13,18,19
Neuralcorrelates-Electroencephalogram(EEG)
TheEEGisameasureofelectrophysiologicalbrainactivity thatrepresentssynchronizedactivationoflargepopulations ofcorticalpyramidalneuronsfiringtogether.The synchro-nizationofelectricalactivitygeneratesdifferentcontinuous frequenciesofoscillation,measurablebyelectrodesplaced at the scalp. EEG is a non-invasive method that can be usedininfant-friendly environmentsandhasan excellent temporalresolution.20 The study fieldof emotional
devel-opmenthasespeciallyexploredthepatternoffrontalEEG powerinthealphafrequency.20,21Alphafrequencyappears
early in life, matures rapidly over the first few years,
andthereafter remains relatively stable. Alphapower is inverselyrelatedtobrainactivity,confirmedwith hemody-namicandmetabolicmeasures(i.e.,negativelycorrelated with cerebral perfusion in functional magnetic resonance imaging(fMRI)andwithcerebralglucosemetabolismusing positron emission tomography (PET)).16,21 Therefore, EEG
alphapowerisusedasaninverseindicatorofregional corti-calactivation.TheEEGfrontalasymmetry(FA)isameasure computingthedifferencebetweenthescoresofalphapower comparingfrontalrightandleftareas.21,23
AlargebodyofempiricalworkmeasuringFArelates dif-ferent patterns of activation to differentially specialized typesofemotions.20,21GreaterrelativeleftFAisassociated
withapproachbehaviors(suchasjoy,anger,andsurgency) andwiththeexpressionofpositiveaffect.Inturn,greater relativerightFAisassociatedwithavoidanceandwithdrawal behaviors,aswellastheexpressionofcertainnegative emo-tions,suchasfearandsadness.Thestudies16,21---24ofFAare
relatedtobothtraitandstatemeasures,considering indi-vidualdifferencesinaffectivestyleandemotionaldisorders, andacuteaffectiveresponse,respectively.
Neuralcorrelates-Event-relatedpotentials(ERPs)
ERPsarethemostcommonmethodusedininfancyto inves-tigatetheneural correlatesofavarietyofperceptualand cognitive functions. ERPs are transient changes in brain activitythatoccurinresponsetoadiscreteevent,extracted from the EEGrecording. Electrical brain activity is mea-suredduringthepresentationofrepeatedstimuli,revealing reliable patterns according to each stimuli category.It is successfullyusedtoinvestigateperceptiondiscrimination, emotionrecognition,andmemoryininfantsandadults.25
Studies in infants have identified several components involved in visual human face processing: P1 (positive deflectionthatpeaksaround120msafterstimulusonset), N290 (negative deflection at 290ms post stimulus), P400 (positivedeflectionat390---450msforinfantsbetween3and 12 months of age), Nc (Negative central deflection peak-ingaround400msafterstimulus),andpositive slowwave (PSW, positive deflection beginning around 800ms after stimulus).25,26Theprecisemeaningofeachcomponentand
thedevelopmentaltrajectoryremaintobeclarifiedbothin children andinadults,although anumberof recent stud-ies have begun toshed light onthis subject. Specifically, consistentevidencerelatessimilarface-sensitiveprocessing forboththeN290andtheP400totheN170,acomponent reliablystudiedinfaceprocessinginadults.25Additionally,
theNcisconsideredanindexofattentionandorientingto salientstimuliininfants,stimulithatrecruitmoreattention appeartoenhancetheamplitudeoftheNc.27
The electrophysiological processes underlying multi-modal sensory integration in emotion began recently to beexamined throughout development.AuditoryERP com-ponentscan be exploredin paradigms usingsimultaneous face---voice stimuli.5 Some authors have shown that the
thePcevincesalargeramplitudetofamiliarstimuli.17Other
researchersrefer toinfants’responses toauditory stimuli astheP150-N250-P350-N450ERPcomplex,andconsiderthe N450equivalenttotheNc.28 Theseinfantcomponentsare
believedtobeprecursorsofchildren’sandadults’ compo-nents (P1, N1, N2,P2, P3a, and N4) and can already be observedatbirth.28
Typicallydevelopinginfants
Studies with newborns reveal that infants already look longer and preferentially orient to face-like stimuli sev-eralhoursafterbirth,29 suggesting theyhavesomeability
to orient to the most salient social stimuli in their envi-ronment: faces. The developmental process is defined as ‘‘experienceexpectant’’:theinnateneuralarchitecturehas the potential to become specialized for face processing, butitneedstobeprimedthroughexperience,allowingthe face-processingpathwaytomature.26
A few studies30---32 have shown that newborns already
react distinctly to different facial expressions. Field et al.30,31 conducted a series of studies with newborns,
bothtermandpreterm,usingdishabituationprocedureand behaviorobservation.Theauthorsreportedthatnewborns wereabletodiscriminateandimitatehappy,surprise,and sadexpressions(althoughtherewasnocontrolgroupinthis study). In a more recent dishabituation study, term new-bornsshowedincreasedlookingtimetohappycomparedto fearfulfacespresentedatthesametime,andnodifference betweenneutralandfearfulcategories.32
Eventhoughthereisevidencethatnewbornsmight dif-ferentiatesomefacialexpressions,itisnotuntil3---4months of age that infants can reliably distinguish among happy comparedtosomeotheremotionalexpressions.5Infantsat
3monthsofagecandiscriminateamonghappyandsurprised faces,5andbetweenhappyandsadfacesoftheirown
moth-ers or a stranger.6 In another experiment,4 3-month-olds
discriminatedbetweenhappyandneutralfacesandwithin thepositiveemotionalcategory (i.e.,differentdegreesof happy),demonstratingincreasingpositivevisualpreference with the intensity of the smile rising, peaking with max-imally toothy smiles. In this study, maternal style to the infants’perceptualsensitivitywascategorized.Motherswho actively encouragedtheir infants toattendtothem more oftenhadinfants whodetectedfacialexpressionsof smil-ingmorereadily,apossiblereflectionoftheeffectsofearly experiencewiththemother’sinteractionstyles.4
Accordingly, happy faces appear to be the first to be discriminated in infants comparing to all other facial expressions.29 The infant’s early preference for positive
emotionsisbelievedtoberelatedtothenecessityof bond-ingatthisattachmentformationstage.29Astheinfantpays
moreattention,thecaregiversmilesandtheinfantimitates itback,promotingapositiveenvironmentandstrengthening theirrelationship,crucialtotheinfant’ssurvival.4,29
Thestudiesoninfantsaftertheageof7monthspresent more consistent data of the infant’s ability tocategorize other expressions than happiness.5 In fact,at some point
between5and7monthsofage,infantsdevelopapreference for fearful faces over other emotions.1 Seven-month-old
infants look longer to fearful than to neutral or happy
faces,andarelesslikelytodisengageattentionfrom fear-fulfaces.1,33Thispatternistypicallyseeninadults,possibly
toprioritize the identification of potential environmental threats.1 As infants begin to crawl, and their locomotion
abilityimprovesthisresponse,thusmayreflectanadaptive increase in vigilance in response to cuesof threat in the environment.1,33
In a multimodal face---voice experiment, 5-month-old infantsreliablydetectedemotionalvocalchanges,butonly iftherewasasimultaneouspresentationoffaces,suggesting thatfacialcuesmightfacilitateinfants’perceptionof emo-tionalvoicetones.34 Inanotherstudy,7-month-oldinfants
recognized face---voice common affect, displaying prefer-ence for face and voice emotionally congruent matching stimuliratherthanincongruentones,evenwhenvoicewas playedoutofsynchronywiththeface.5
Neuralcorrelates
Stablepatternsof FAemergeearly inlifeand arerelated to individual differences in emotional trait dispositions, suchasemotionregulationandreactivity.16,20,21Infantswith
moredifficulttemperaments(i.e.,highlyreactive,fearful, andinhibited)showgreater relativeright FA.7,10 FAisalso
observedinacuteaffective response,indicatinga current emotionalstate.FoxandDavidson35 conductedaseriesof
studiesexaminingFAduringavarietyofelicitorsproducing positiveor negativeemotions.Newbornsweretested with water,sucrose,andcitricacidsolutionswhileconcomitant EEGwasrecorded.Thesolutionselicitedfacialexpressions thattheexperimenterscodedasinterestanddisgust,which wereassociatedtogreater leftFAinresponse toa pleas-anttaste(sucrose)comparedtounpleasant(citricacid)or neutraltastes.35
Typically developing 10-month-old infants watched videotaped segments of a femalemodel displaying happy or sadfacialexpressions. The infantsshowed greater rel-ative left FA when observing the happy expressions.36 In
anotherstudy,23 thesameauthorsdocumented
asymmetri-calEEGactivationinthefrontalcortexwhen10-month-old infantswere observed while exhibitingspecific behaviors. Infants showed greater left FAwhen expressing approach behaviors like reaching with hands for their mother and elicitingfacialexpressionsofjoyaccompanied bypositive vocalizations.When the same infants displayed behaviors suchasgazeaversionanddistress(i.e.,activewithdrawal behavior),therewasgreaterrelativerightFA.23Inasimilar
posteriorstudy,6-month-oldinfantswhodemonstratedfear andsadness(whileastrangerwasapproaching)hadgreater rightFA.37
InthefirststudyininfantsusingERPstoanalyze differ-encesinresponsetofacialemotionalstates,NelsonandDe Haan27 reportedthat7-month-oldinfants evinceda larger
In a multimodal processing study, 7-month-old infants demonstrated a larger Nc for emotionally incongruent face---voice pairs of happy and angry stimuli, whereas congruentstimulielicitedlargeramplitudeforthePc.17The
pattern of an attenuated Nc and a larger Pc was related to the recognition of the congruent pairing.17 Recently,
9-month-old infants revealed modified auditory ERP com-ponents (larger positivity on P150 and P350 and smaller negativity in N250 and N450) for either happy or fearful vocalizationswhenprecededbyvisualexpositiontofearful faces.38BothP150andP350arerelatedtoorienting
atten-tion; therefore, the authors concludedthat fearful faces enhancedattentionallevels,modulatingERPresponses.38
Infantsofdepressedandanxiousmothers
Maternal depression and anxiety are implicated in atypi-calbehaviorsin infants sincebirth.9 Infants of depressed
and anxious mothers are believed tohave higher arousal andlessattentiveness,12 showinglessorientationtofacial
expressionsandface---voicepairsinexperimentalconditions and in live face---voice interactions.15 Studies of behavior
andneuralcorrelatesarebeginningtoimproveinsightsinto themechanismsunderlyingthepresumablyslower sensory processinganddelayedattentionintheseinfants.
Mostofthestudiesonmaternalnegativeaffectivestates are based on symptoms scales rather than a confirmed diagnosis of maternal depression and anxiety. Although self-reportscales donot provideaclinical diagnosis, they havebeen correlatedwithconfirmeddiagnosesonclinical evaluations.8,9,22 Itisparticularlynoteworthytoemphasize
thattheuseofdepressionsymptomsscaleshasbeenshown toinvariably assessa widerangeofanxiety symptoms,as well asother negativeaffective states such asangerand irritability.10,11 Therefore, although the majority of
stud-iesreviewed here rely ondepression symptoms scales, it isbelievedthattherelatedoutcomesmaybesecondaryto maternalanxietyaspectsaswell.8---10
Studies onnewborns indicatethat infantsof depressed mothers(IDMs) orient lessto faces andvoices asearly as duringthefirsthoursoflife.Hernandez-Reifetal.39tested
full-termnewbornsofdepressedandnon-depressed moth-ersfor visual preference andhabituation to themother’s face---voice,comparingtoafemalestranger.IDMsrequired one-thirdmoretrialsandalmosttwiceaslongastheinfants of nondepressed mothers (INDMs) to habituate to their mother’sface---voicepairing.Inthepost-testvisual prefer-encephase,IDMsfailedtodiscriminatetheirmothersfroma stranger.Inasubsequentexperiment,40agroupofmothers
wereevaluatedlongitudinally for continuityof depressive symptoms pre- and postnatally, including comorbid anxi-ety.Their3-month-oldinfantswereexposedtovideoclips of female models with face and voice stimuli for happy andsadconditions.As earlier reportedinnewborns, IDMs requiredlongertimetohabituatetofaces,particularlyto happyfacialexpressions.Unexpectedly,IDMswereableto discriminatesad fromhappy expressions but only if they werefirsthabituatedtosad, therebyindicating that they maynotperceivesadexpressionsasanovelty.40
Usingastill-faceprocedure,3-month-oldIDMsexhibited lessdistressand fewernegativeexpressionscomparing to
thetypicalresponseofINDMs,possiblyrelatedtobeingmore accustomedtoalessexpressiveenvironmentcharacterized by their mothers’ relatively flat affect and less interac-tivebehaviors.18,19Beyondthat,IDMshadalessinteractive
behavior(i.e.,fewerpositiveandnegativebehaviors)during therecordedspontaneousmother-infantinteractions,when motherswereinstructedtoengagewiththeirinfantinplay, astheywouldusuallydoathome.19Inastudy13thataddeda
tactilecomponenttothestill-faceprocedure,motherswere askedtomaintainaneutralfacewhiletouchingtheinfant. Three-month-oldIDMs showedmorepositiveaffect, mani-festing more smiles and vocalizations than infants in the still-facecontrolgroupwithouttouching.The authors sug-gestthatprovidingtouchstimulationcanincreaseinfants’ attention andpositive affect, thus improving the interac-tionsofdepressedmothersandtheirinfants.13
Five-month-old infants of mothers with a confirmed diagnosisofdepressionweresuccessfullyhabituatedto neu-tralor smiling faces,but theylaterfailedtodiscriminate between the facialexpressions.14 Striano et al.41
investi-gated6-month-oldIDMsandINDMsandfoundthatallinfants wereabletodiscriminateneutralfromprogressivelyhigher intensities of smiling and frowning faces. IDMs, however, presented a looking preference for all smiling faces, and agreaterpreferentiallookingtohighintensitysmilingand frowningexpressions,apatternnotobservedinINDMs.
Hence,thereisevidencethatIDMsshowlessinterestin faces,orientpoorlytosynchronizedvisualandvocalstimuli, andhavediminishedsensitivitytochangesinfacial expres-sions frombirthand throughoutthe firstmonthsof life.15
The abnormalitiesarespeculated toberelatedtodeficits in attentiveness,aswell asalteredperceptual skills, per-haps secondary to atypicalvisual and/or auditory sensory processing.14,15
Neuralcorrelates
ThereisconsistentevidencethatIDMsshowgreaterrelative rightFAthandoinfantswhosemothersarenotdepressed. Thispatternis reportedfromnewbornsstudies,remaining stablethroughoutinfancyuptochildhood.16,20TherightFA
bias is alsoexhibited by depressedadults,which remains stableevenafteraremissionofthedepressivesymptoms.22
RelativerightFAisalsoassociatedwithanxiety.11
Duringface-to-faceinteractions,3-month-oldIDMs com-paredtoINDMswerelessresponsive tofacialexpressions, lookedlongeratsadfaces,anddisplayedlesspositiveand moreoften negativefaces themselves.42 Anothergroup of
3-month-oldwatched videosof afemalemodel displaying happyandsadfacialandvocalexpressions.TheINDMs exhib-itedgreaterrelativerightFAwhenviewingsadcomparedto happyface---voicestimuli.NodifferencesonFAwerefound forIDMs,possiblybecausetheEEGdatawereanalyzed dur-ingthewholeexperiment,ratherthanaccountingfor only theperiods whentheinfants wereactually lookingat the videos.43 Inasubsequentstudy,thesameresearchers
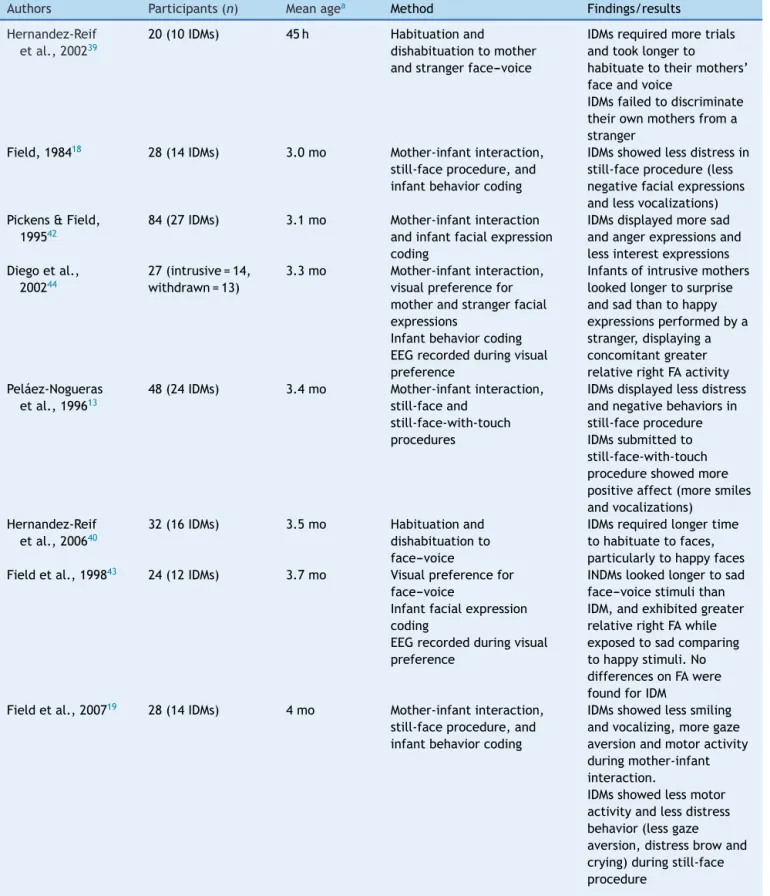
Table1 Studiesofbehaviorandneuralcorrelatesoninfantsofdepressedand/oranxiousmothers.
Authors Participants(n) Meanagea Method Findings/results
Hernandez-Reif etal.,200239
20(10IDMs) 45h Habituationand
dishabituationtomother andstrangerface---voice
IDMsrequiredmoretrials andtooklongerto
habituatetotheirmothers’ faceandvoice
IDMsfailedtodiscriminate theirownmothersfroma stranger
Field,198418 28(14IDMs) 3.0mo Mother-infantinteraction,
still-faceprocedure,and infantbehaviorcoding
IDMsshowedlessdistressin still-faceprocedure(less negativefacialexpressions andlessvocalizations) Pickens&Field,
199542
84(27IDMs) 3.1mo Mother-infantinteraction andinfantfacialexpression coding
IDMsdisplayedmoresad andangerexpressionsand lessinterestexpressions Diegoetal.,
200244
27(intrusive=14, withdrawn=13)
3.3mo Mother-infantinteraction, visualpreferencefor motherandstrangerfacial expressions
Infantbehaviorcoding EEGrecordedduringvisual preference
Infantsofintrusivemothers lookedlongertosurprise andsadthantohappy expressionsperformedbya stranger,displayinga concomitantgreater relativerightFAactivity Peláez-Nogueras
etal.,199613
48(24IDMs) 3.4mo Mother-infantinteraction, still-faceand
still-face-with-touch procedures
IDMsdisplayedlessdistress andnegativebehaviorsin still-faceprocedure IDMssubmittedto still-face-with-touch procedureshowedmore positiveaffect(moresmiles andvocalizations)
Hernandez-Reif etal.,200640
32(16IDMs) 3.5mo Habituationand
dishabituationto face---voice
IDMsrequiredlongertime tohabituatetofaces, particularlytohappyfaces Fieldetal.,199843 24(12IDMs) 3.7mo Visualpreferencefor
face---voice
Infantfacialexpression coding
EEGrecordedduringvisual preference
INDMslookedlongertosad face---voicestimulithan IDM,andexhibitedgreater relativerightFAwhile exposedtosadcomparing tohappystimuli.No differencesonFAwere foundforIDM
Fieldetal.,200719 28(14IDMs) 4mo Mother-infantinteraction,
still-faceprocedure,and infantbehaviorcoding
IDMsshowedlesssmiling andvocalizing,moregaze aversionandmotoractivity duringmother-infant interaction.
Table1 (Continued)
Authors Participants(n) Meanagea Method Findings/results
Diegoetal., 200424
60(30IDMs) 4.2mo Visualpreferencefor
motherandstrangerfacial expressions
Infantbehaviorcoding EEGrecordedduringvisual preference
IDMsexhibitedlesspositive affectandlookedlessat theirmothers’surpriseand sadexpressions.IDMlooked lessatallstrangers’facial expressions,showedless positiveaffectduringhappy andsurpriseandmore negativeaffectduring surpriseexpressions IDMshadsignificantly greaterrelativeFA comparedtoINDMsinall differentexpressionsof boththemothersand strangers
IDMsandINDMsshowed relativegreaterrightFA duringtheirmothers’and strangers’sadvs.happy faces
Bornsteinetal., 201114
28(14IDM) 5.1mo Habituationandvisual
pairedcomparison procedure
IDMsandINDMshabituated toneutralandhappyfaces IDMsfailedtodiscriminate betweenneutralandhappy facesfollowinghabituation Strianoetal.,
200241
46(Maternal depression analyzedas acontinuous variable)
6mo Visualpairedcomparison procedurecomparing neutralfromprogressively higherintensitiesofsmiling andfrowningfaces. Mother-infantinteraction andinfantbehaviorcoding
Infantsofmothers’with higherdepressionscores showedgreaterlooking preferenceforallsmiling faces,andtohighintensity smilingandfrowning expressions
Infantsofmothers’with higherdepressionscores lookedlongerattheirown motherswhiletheywere smiling
Otteetal.,201512 81(Maternal
anxietyanalyzed asacontinuous variable)
10.1mo Multimodalface---voice compounds
ERPrecordedwithEEG duringface---voice compounds
Infantsofmothers’with highermaternalanxiety scoresshowedlargerP350 andP150amplitudesafter fearfulvocalizations, precededbyeitherhappyor fearfulfaces.
h,hours;mo,months;IDMs,infantsofdepressedmothers;INDMs,infantsofnon-depressedmothers;EEG,electroencephalogram;ERPs, event-relatedpotentials;FA,frontalasymmetry.
aMeanageispresentedinhoursormonths.
rightFAduringtheirmothers’andstrangers’sadvs.happy expressions;however,IDMshadsignificantlygreaterFA com-paredtoINDMsthroughoutthedifferentexpressionsofboth the mothers and strangers. IDMs were less interested in facialexpressions,showedlesspositiveandmorenegative affect,andevincedincreasedsalivarycortisollevelsafter theexperiment.24
Diego et al.44 further investigated infants of mothers
and displayedgreater relative right FA. Intrusive mothers showed rough physical contact and quick and loud ver-bal behavior when interacting with their infants. In the study,3-month-oldinfantsobservedtheirownmotheranda stranger,inhappy,surprised,andsadexpressions.Infantsof intrusivemotherslookedlongertosurpriseandsad expres-sionscomparedtohappyonesperformedbyastranger,and displayeda concomitantgreater relativeright FAactivity. These infantsalso hadan increasedsalivarycortisol, pos-siblyreflectingahigherresponsetothestressfulstimulus. Thenatureofthedifferentmaternaldepressivestylesand howtheyaffecttheinfants’ physiologyandbehaviorhave notyetbeenfullyunderstoodandrequirefurtherresearch. As previously reviewed, ERPprovide an excellent tool totemporarilycorrelate behaviorandneuralresponseand is easily administeredthroughout development.25 A
grow-ingnumberofstudieshavebeenperformedinchildrenand adults,expandingtheresearchonneuralvulnerability mark-ers for psychopathological disorders, includingdepression and anxiety.25 In infancy, a few studies on auditory ERP
and maternal affective disorders have begun to demon-strateneuralprocessingalterations,providinginsightsinto theunderlyingdevelopmentalpathwaysthatremaintobe betterclarified.
Inarecentstudy usingERPandmultimodalprocessing, Otte et al.12 analyzed 9-month-old infants exposed to
maternal anxiety during pregnancy (10% of the mothers also reported previous treatment for depression). Infants were presented with happy and fearful facial and vocal stimuli.Infantsprenatally exposedtohigherlevelsof anx-iety exhibited significantly larger P350 amplitudes and a trendforlargerP150amplitudesafterfearfulvocalizations, regardless of the preceding visual emotion type, poten-tially related to an increased attention to fearful vocal stimuli. The findings corroborate studies in children and adultsthatanxietysymptomsheightenedthesensitivityto threat-relatedinformation.12
Thefindingsofstudiesoninfantsofdepressedand anx-iousmothersaresummarizedinTable1.
Conclusions
Insummary,infantsofdepressedandanxiousmothershave increasedriskfor severaldetrimentaloutcomesacrossthe lifespan. They exhibit more difficult temperaments (i.e., highlyreactive,fearful,andinhibited)andhigherincidence ofattentional,emotional,andbehavioralproblems---suchas depression,anxiety,andconductdisorders9,10---throughout
childhood,adolescence,andadulthood.7,9,10
During the first year of life, these infants display a number of atypical behaviors, including less interest in facialexpressions,lesssmilingandvocalizations,moretime required to habituate to faces and to face---voice pairs, and failuretodiscriminatebetween different emotions.15
Impairmentsinsensoryandperceptualprocessingaswellas reducedattentivenessmayunderliesuchbehaviors.Recent neurophysiologicalstudieshavebeguntoshedlightonthe possiblemechanismslinkingmaternal depressionand anxi-etytooutcomesininfants.EEGstudiesspecificallyanalyzing facial emotion recognition corroborate findings from the extant literatureof a relativeright FAasymmetryand its
associationwithdepression andnegativeeffects. Compar-ingtoINDMs,IDMsshowsignificantlygreaterrelativeright FAacrossdifferentemotionalexpressions.24Arecentunique
ERPstudydescribedacorrelationbetweenmaternalanxiety andinfants’ enhancedERPcomponentstofearfulstimuli, potentiallyrelatedtoanincreasedbiastothreatinthese infants.12
Furtherresearchisneeded tobetterclarifythe poten-tial mechanisms related to infants’ negative outcomes. Expanding the researchwith current behavior and neuro-physiologicalmethods,aswellasexploringnewtoolssuch asnear-infraredspectroscopy,canhelpdetect biologically-basedmarkersthatmaymediatetheseassociationsfromthe earlieststages of life, months and yearsprior to adverse clinicaloutcomes.Fosteringclinical andresearch integra-tion,byincorporatinginvestigationtoolsinclinicalpractice or promoting longitudinal studies in risk populations, for example, should facilitate studying individual differences throughout development and enablethe potential identi-ficationofprecociousneural changesininfantsassociated with the later onset of clinical symptoms. Beyond that, developmental research might eventually contribute to refiningscreeningtools,improvingtreatment andenabling primarypreventioninterventionsforchildrenatrisk.
Funding
JulianaA.PortoissupportedbyCAPES/PDSEatPUCRSand by a researchfellowship at the Laboratories of Cognitive Neuroscience, Boston Children’s Hospital/HarvardMedical School.MagdaL.NunesisaPQresearcherfromCNPqBrazil.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.LeppänenJM,NelsonCA.Tuningthedevelopingbraintosocial signalsofemotions.NatRevNeurosci.2009;10:37---47. 2.SomervilleLH,Fani N,McClure-ToneEB.Behavioraland
neu-ral representationofemotionalfacial expressionsacrossthe lifespan.DevNeuropsychol.2011;36:408---28.
3.AslinRN.What’sinalook?DevSci.2007;10:48---53.
4.KuchukA,VibbertM,BornsteinMH.Theperceptionofsmiling anditsexperientialcorrelatesinthree-month-oldinfants.Child Dev.1986;57:1054---61.
5.Grossmann T. The development of emotion perception in face and voice during infancy. Restor Neurol Neurosci. 2010;28:219---36.
6.BarreraME,MaurerD.Theperceptionoffacialexpressionsby thethree-month-old.ChildDev.1981;52:203---6.
7.DunkelSchetterC,TannerL.Anxiety,depressionandstressin pregnancy: implicationsfor mothers,children,research, and practice.CurrOpinPsychiatry.2012;25:141---8.
8.LovejoyMC,GraczykPA,O’HareE,NeumanG.Maternal depres-sion and parenting behavior: a meta-analytic review. Clin PsycholRev.2000;20:561---92.
10.Field T.Prenataldepression effectsonearlydevelopment: a review.InfantBehavDev.2011;34:1---14.
11.Field T, Diego M, Hernandez-Reif M, Schanberg S, Kuhn C, Yando R, et al. Pregnancy anxiety and comorbid depression andanger:effectsonthefetusandneonate.DepressAnxiety. 2003;17:140---51.
12.Otte RA, Donkers FC, Braeken MA, Van denBergh BR. Mul-timodal processing of emotional information in 9-month-old infantsII:prenatalexposuretomaternalanxiety.BrainCogn. 2015;95:107---17.
13.Peláez-NoguerasM,FieldTM,HossainZ,PickensJ.Depressed mothers’touchingincreasesinfants’positiveaffectand atten-tioninstill---faceinteractions.ChildDev.1996;67:1780---92. 14.BornsteinMH,ArterberryME,MashC,ManianN.Discrimination
offacialexpressionby5-month-oldinfantsofnondepressedand clinicallydepressedmothers.InfantBehavDev.2011;34:100---6. 15.FieldT,DiegoM,Hernandez-ReifM.Depressedmothers’infants are less responsive to faces and voices. Infant Behav Dev. 2009;32:239---44.
16.FieldT,FoxN,PickensJ,NawrockiT.RelativerightfrontalEEG activationin3-to6-month-oldinfantsofdepressedmothers. SpecialSection:Parentaldepressionanddistress:implications for developmentininfancy,childhood,and adolescence.Dev Psychol.1995;31:358---63.
17.GrossmannT,StrianoT,FriedericiAD.Crossmodalintegrationof emotionalinformationfromfaceandvoiceintheinfantbrain. DevSci.2006;9:309---15.
18.FieldTM.Earlyinteractionsbetweeninfantsandtheir postpar-tumdepressedmothers.InfantBehavDev.1984;7:527---32. 19.FieldT,Hernandez-ReifM,DiegoM,FeijoL,VeraY,GilK,etal.
Still---faceandseparationeffectsondepressedmother---infant interactions.InfantMentHealthJ.2007;28:314---23.
20.Davidson RJ.Anteriorcerebralasymmetryand thenatureof emotion.BrainCogn.1992;20:125---51.
21.Davidson RJ. Affective neuroscience and psychophysiology: towardasynthesis.Psychophysiology.2003;40:655---65. 22.DiegoMA,JonesNA,Field T.EEGin1-week,1-monthand
3-month-old infants of depressedand non-depressedmothers. BiolPsychol.2010;83:7---14.
23.FoxNA,DavidsonRJ.Patternsofbrainelectricalactivityduring facialsignsofemotionin10-month-oldinfants.DevPsychol. 1988;24:230---6.
24.DiegoMA,FieldT,JonesNA,Hernandez-ReifM,CullenC, Schan-bergS,etal.EEGresponsestomockfacialexpressionsbyinfants ofdepressedmothers.InfantBehavDev.2004;27:150---62. 25.NelsonCA3rd,McCleeryJP.Useofevent-relatedpotentialsin
thestudyoftypicalandatypicaldevelopment.JAmAcadChild AdolescPsychiatry.2008;47:1252---61.
26.NelsonCA.Thedevelopmentandneuralbasesofface recogni-tion.InfantChildDev.2001;10:3---18.
27.Nelson CA, De Haan M. Neural correlates of infants’ visual responsivenesstofacialexpressionsofemotion.DevPsychobiol. 1996;29:577---95.
28.KushnerenkoE,CeponieneR,BalanP,FellmanV,HuotilaineM, NäätäneR.Maturationoftheauditoryevent-relatedpotentials duringthefirstyearoflife.Neuroreport.2002;13:47---51. 29.BornsteinMH,ArterberryME.Recognition,discriminationand
categorization of smiling by 5-month-old infants. Dev Sci. 2003;5:585---99.
30.Field TM, Woodson R, Greenberg R, Cohen D. Discrimina-tionandimitationoffacialexpressionbyneonates.Science. 1982;218:179---81.
31.FieldTM,WoodsonR,CohenD,GreenbergR,GarciaR,Collins K.Discriminationandimitationoffacialexpressionsbyterm andpretermneonates.InfantBehavDev.1983;6:485---9. 32.FarroniT,MenonE,RigatoS,JohnsonMH.Theperceptionof
facialexpressionsinnewborns.EurJDevPsychol.2007;4:2---13. 33.PeltolaMJ,LeppänenJM,MäkiS,HietanenJK.Emergenceof enhancedattentiontofearfulfacesbetween5and7monthsof age.SocCognAffectNeurosci.2009;4:134---42.
34.Walker-AndrewsAS,LennonE.Infants’discriminationofvocal expressions:contributionsofauditoryand visualinformation. InfantBehavDev.1991;14:131---42.
35.FoxNA,DavidsonRJ.Taste-elicitedchangesinfacialsignsof emotionandtheasymmetryofbrainelectricalactivityinhuman newborns.Neuropsychologia.1986;24:417---22.
36.Davidson RJ, Fox NA. Asymmetrical brain activity discrimi-natesbetweenpositiveandnegativeaffectivestimuliinhuman infants.Science.1982;218:1235---7.
37.Buss KA, Schumacher JR, DolskiI, Kalin NH, Goldsmith HH, Davidson RJ. Rightfrontalbrain activity, cortisol, and with-drawal behavior in 6-month-old infants. Behav Neurosci. 2003;117:11---20.
38.OtteRA,DonkersFC,BraekenMA,VandenBerghBR.Multimodal processingofemotionalinformationin9-month-oldinfantsI: emotionalfacesandvoices.BrainCogn.2015;95:99---106. 39.Hernandez-Reif M, Field T, Diego M, Largie S. Depressed
mothers’newbornsshowlongerhabituationand failtoshow face/voicepreference.InfantMentHealthJ.2002;23:643---53. 40.Hernandez-ReifM,FieldT,DiegoM,VeraY,Pickens J.Happy facesarehabituatedmoreslowlybyinfantsofdepressed moth-ers.InfantBehavDev.2006;29:131---5.
41.StrianoT,BrennanPA,VanmanEJ.Maternaldepressive symp-tomsand6-month-oldinfants’sensitivitytofacialexpressions. Infancy.2002;3:115---26.
42.PickensJN,FieldT.Facialexpressionsandvagaltoneofinfants ofdepressed and non-depressedmothers. Early Dev Parent. 1995;4:83---9.
43.FieldT,PickensJ,FoxN,GonzalezJ,NawrockiT.Facial expres-sion and EEG responses to happy and sad faces/voices by 3-month-oldinfantsofdepressedmothers.Br JDevPsychol. 1998;16:485---94.