www.jped.com.br
REVIEW
ARTICLE
Microcephaly
and
Zika
virus:
a
clinical
and
epidemiological
analysis
of
the
current
outbreak
in
Brazil
夽
,
夽夽
Magda
Lahorgue
Nunes
a,b,∗,
Celia
Regina
Carlini
b,c,
Daniel
Marinowic
b,c,
Felipe
Kalil
Neto
b,d,
Humberto
Holmer
Fiori
a,b,
Marcelo
Comerlato
Scotta
b,e,
Pedro
Luis
Ávila
Zanella
a,b,
Ricardo
Bernardi
Soder
b,f,
Jaderson
Costa
da
Costa
a,baSchoolofMedicine,PontifíciaUniversidadeCatólicadoRioGrandedoSul(PUCRS),PortoAlegre,RS,Brazil bZika-Team,InstitutodoCérebrodoRioGrandedoSul(Inscer),PortoAlegre,RS,Brazil
cInstitutodoCérebrodoRioGrandedoSul(Inscer),PortoAlegre,RS,Brazil
dPost-GraduatePrograminPediatricsandChildHealth,PontifíciaUniversidadeCatólicadoRioGrandedoSul(PUCRS),Porto
Alegre,RS,Brazil
eDepartmentofPediatrics,SchoolofMedicine,PontifíciaUniversidadeCatólicadoRioGrandedoSul(PUCRS),PortoAlegre,RS,
Brazil
fDepartmentofDiagnosticMethods,SchoolofMedicine,PontifíciaUniversidadeCatólicadoRioGrandedoSul(PUCRS),Porto
Alegre,RS,Brazil
Received19February2016;accepted22February2016 Availableonline15April2016
KEYWORDS
Zikavirus; Microcephaly; Pregnancy; Cortical development; Neuroimaging
Abstract
Objective: ThisstudyaimedtocriticallyreviewtheliteratureavailableregardingtheZikavirus outbreakinBrazilanditspossibleassociationwithmicrocephalycases.
Sources: ExpertsfromInstitutodoCérebrodoRioGrandedoSulperformedacritical (nonsys-tematic)literaturereviewregardingdifferentaspectsoftheZikavirusoutbreakinBrazil,such astransmission,epidemiology,diagnosticcriteria,anditspossibleassociationwiththeincrease ofmicrocephalyreports.ThePubMedsearchusingthekeyword‘‘Zikavirus’’inFebruary2016 yielded151articles.Themanuscriptswerereviewed,aswellasallpublications/guidelinesfrom theBrazilianMinistryofHealth,WorldHealthOrganizationandCentersforDiseaseControland Prevention(CDC---UnitedStates).
夽
Pleasecitethisarticleas:NunesML,CarliniCR,MarinowicD,NetoFK,FioriHH,ScottaMC,etal.MicrocephalyandZikavirus:aclinical andepidemiologicalanalysisofthecurrentoutbreakinBrazil.JPediatr(RioJ).2016;92:230---40.
夽夽
StudycarriedoutatInstitutodoCérebro(InsCer)doRioGrandedoSulandFaculdadedeMedicina,PontifíciaUniversidadeCatólicado RioGrandedoSul(PUCRS),PortoAlegre,RS,Brazil.
∗Correspondingauthor.
E-mail:[email protected](M.L.Nunes).
http://dx.doi.org/10.1016/j.jped.2016.02.009
Summaryoffindings: Epidemiological data suggest a temporal association between the increasednumberofmicrocephalynotificationsinBrazilandoutbreakofZikavirus,primarily intheBrazil’sNortheast.Ithasbeenpreviouslydocumentedthatmanydifferentvirusesmight causecongenitalacquiredmicrocephaly.Stillthereisnoconsensusonthebestcurveto mea-surecephaliccircumference,specificallyinpretermneonates.Conflictingopinionsregarding thediagnosisofmicrocephaly(below2or3standarddeviations)thatshouldbeusedforthe notificationswerealsofoundintheliterature.
Conclusion: Thedevelopmentofdiagnostictechniquesthatconfirmacause---effectassociation andstudiesregardingthephysiopathologyofthecentralnervoussystemimpairmentshouldbe prioritized.Itisalsonecessarytostrictlydefinethecriteriaforthediagnosisofmicrocephaly toidentifycasesthatshouldundergoanetiologicalinvestigation.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/ 4.0/).
PALAVRAS-CHAVE
VírusZika; Microcefalia; Gestac¸ão; Desenvolvimento cortical;
Neuroimagem
MicrocefaliaevírusZika:umolharclínicoeepidemiológicodosurtoemvigênciano Brasil
Resumo
Objetivos: Oobjetivodesteestudofoirealizarumarevisãocríticadaliteraturasobreosurto devírusZikanoBrasilesuapossívelassociac¸ãocomcasosdemicrocefalia.
Fontededados: Especialistas em áreas afins do Instituto doCérebro do Rio Grande do Sul realizaramumarevisãocrítica(nãosistemática)daliteraturasobreovírusZika,suasformasde transmissão,aepidemianoBrasil,critériosdiagnósticoseapossívelassociac¸ãocomoscasos crescentesdemicrocefalia.Ousodapalavrachave‘‘Zikavirus’’nabasededadosdoPubMed emfevereirode2016,retorna151publicac¸ões.Estestextosforamrevisadosassimcomotodas aspublicac¸õeserecomendac¸õesdoMinistériodaSaúde,Organizac¸ãoMundialdaSaúdeeCentro deControledeDoenc¸as(CDC---USA).
Síntesedosdados: Osdadosepidemiológicossugerem umarelac¸ãotemporalentreaumento danotificac¸ãodecasosdemicrocefaliaeosurtodevírusZika,principalmente noNordeste doBrasil.Agentesviraiscomprovadamentepodem sercausadoresdemicrocefaliacongênita adquirida.Nãoexisteumconsensosobreamelhorcurvadeperímetrocefálicoaserutilizada, principalmentenosprematuros.Assimcomotambémexistemdivergênciassobreadefinic¸ãode microcefalia(abaixode2ou3desviospadrões)aserpadronizadanasnotificac¸ões.
Conclusão: Deve-sepriorizarodesenvolvimentodetécnicasdiagnósticasqueconfirmemuma relac¸ãocausa---efeitoeestudossobremecanismosdapatogênesedainfecc¸ãopeloZikano sis-temanervosocentral.Tambéménecessáriodefinireuniversalizaroscritériosdiagnósticospara aidentificac¸ãodoscasosdemicrocefaliaquedevemsersubmetidosàinvestigac¸ãoetiológica. ©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
TheWorldHealthOrganization(WHO)hasissuedawarning establishinganinternationalstateofemergencyduetothe microcephalyincidenceincreaseinendemicareaswithZika virus(ZikaV)proliferation.1
Thedisease,whicharrivedinBrazilpossiblyin2014,has spreadintheNortheastregionandismigratingtothe Amer-icas.Itis believedthat itwillquicklycontinue spreading, asitsmainvector,theAedesaegyptimosquito,is undergo-ingaperiodofwidedisseminationduetothehighsummer temperaturesinthesouthernhemisphere.2---4
Apossibleassociationbetweenintrauterineinfectionby ZikaVandearlymicrocephalywasinitiallyproposed,based on the observation of physicians in Northeastern Brazil, whodetected asuddenincreaseintheincidenceofbirths
of microcephalic children after identification of the virus entryinBrazil.However,thiscause---effectassociationstill needstobeproven.5,6ThefactisthattheZikaVentersthe
central nervoussystem (CNS), breaking the protection of theblood---brainbarrier,whichhasbeenpreviously demon-stratedinanimalexperiments.7,8
The recent discovery of other forms of virus transmis-sion,inadditiontoaninfectedinsectbite,throughsexual contactorsecretions(saliva,urine),andthelackofvaccines orspecifictreatmenthasalarmedthepopulation.Moreover, thelackoflonger-durationbiologicalmarkersthatallowfor diagnosticconfirmation,geometricallyincreasethenumber ofsuspectedcasesand,consequently,therecordingoffalse positivecases.9---11
initiatetheinvestigationofthemicrocephalystatus.Asthe scientificliteratureisstillscarceandnewfindingsand infor-mationhavequicklyappearedandbeenwidelydisseminated inthemedia,thisarticleaimedtobringtogethera multi-disciplinarygroupofexpertsinassociatedfieldstocritically reviewthescientificevidence,diagnosticprotocols, differ-entialdiagnosis,andresearchperspectivesthatallowforthe confirmationof theassociation between ZikaVand micro-cephaly.
Methods
This was a non-systematic review article conducted by a panelofexperts.Thisarticlewasdividedintotopics consid-eredsignificantforabetterunderstandingofZikaVoutbreak in Brazil, such as the diagnostic difficulties of this infec-tion and the differential diagnosis with other infections whosevector is alsothe Aedesaegyptimosquito; biologi-calcharacteristics ofZikaV; possibleassociationsbetween ZikaVinfection andCNS developmentalterations; criteria for determining microcephaly;and etiological differential diagnosis of microcephalies. Additionally, the article dis-cusses possible experimental models that would help to understandthephysiopathogenesisofCNSlesions.
Results
The use of the key word ‘‘Zika virus’’ in the PubMed databaseinFebruary2016yielded151publications.These texts were reviewed, aswell asall publications and rec-ommendationsfromtheBrazilianMinistryofHealth,World HealthOrganization, andCenters for DiseaseControl and Prevention(CDC---UnitedStates).
Stagesofintrauterinedevelopmentofthecentral
nervoussystem(CNS)andassociateddisorders
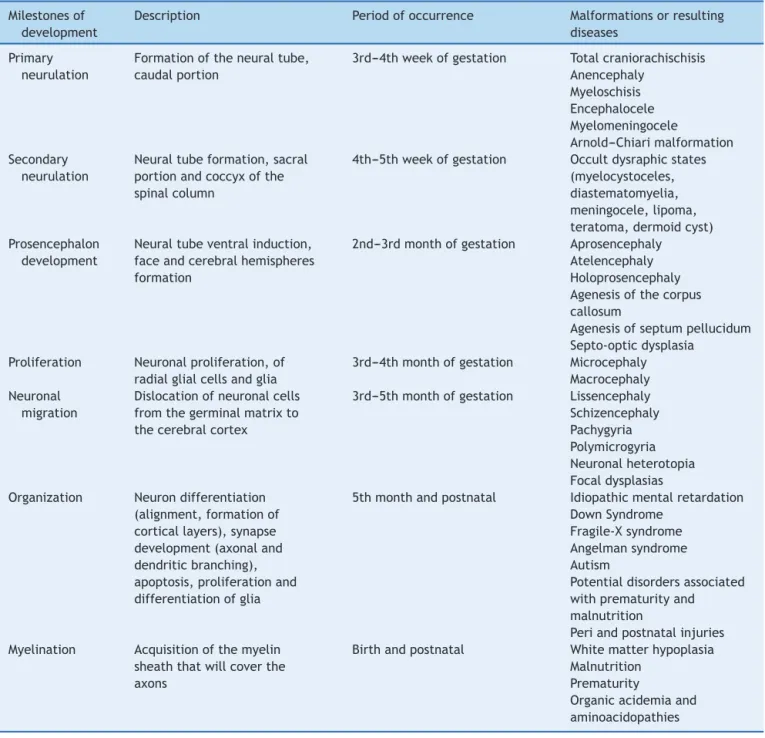
TheCNSdevelopmentinhumansstartsatthegastrulation stage,approximatelyonthe14thembryonicday,whenthe thickeningof the ectodermal membrane occurs, originat-ingtheneuralplate.Subsequently,twomajorprocesseswill occursequentially:theformationoftheneuraltubeandthe developmentoftheprosencephalon.Table1liststhe devel-opmentalmilestones,thetimeoftheiroccurrence,andthe defectsarisingfromproblemsoccurringatthesestages.12
Theproliferationphaseisquitecomplexandbroad, start-ingaround thesecond tothe fourth month of pregnancy, withneuronal proliferation and generation of glial radial cells,extending fromthefifth monthuntiltheend ofthe firstyear of life, when glialproliferation occurs. The ini-tial processis characterized by thegerminal matrix stem cells that divide symmetrically, forming the proliferative neuronal---glialunits, whicharedistributedinthe periven-tricularzone. Afterthat,an asymmetricdivisionstarts,in whicheachstemcelloriginatesanotherstemcellanda post-mitoticneuronalcell.Thisasymmetricdivisiondetermines theproliferativeunitsize.13
Thepostmitoticneuronsmigratealongtheradialgliato formthe different layersof the cerebral cortex. Approx-imately one-third of the neurons do not use the radial
glia structure and migrate tangentially in the cortical direction.14 During the migration process, neurons pass
throughneurons thatarealreadypositionedinthecortex, leadingtoalamination wherethe lastarrivingneurons in corticalareapositionthemselvesontheoutermostsurface ofthecortex.Thisfinal,histologicallydistinctsix-layer orga-nization comprises an extraordinary diversity of neuronal subtypes, working asunits for the formation of a power-fulneuralcircuit.Inrecentyears,remarkableprogresshas been made tounderstand the molecular events that con-trolthedevelopmentofthecerebralcortex,aswellasthe disordersassociatedwithalterationsinthisprocess.15
Thealterationsinthecerebralcortexdevelopmentare shownasagroupofdifferentmalformationswhose patho-genesisisnotwelldefinedyet.Amongthecorticaldefects, a subset of conditions has been associated with alter-ations in cell migration and neurodifferentiation, among them the lissencephalies,polymicrogyria, andfocal corti-caldysplasias.Someresearcherssuggestthatinadditionto alterationsin cellmigrationandneurodifferentiation,one mustconsiderotherfactorsinthepathogenesisofcortical malformations,suchascellproliferation,celldeath, intra-corticalgrowthanddevelopmentaftercellmigration,and theformationofaxonsanddendrites.16,17
Themajorityof pathologiesassociatedwithcell migra-tion alterations have a variety of genes that may be associatedwiththediseasedphenotype,butinsomecases itsappearanceissporadic.Thehighepileptogenicityofthe cortexinthesecasesisnoteworthy.18
Several environmental factors have been identified as causing cortical defects; maternal exposure during pregnancytoagentssuchasethanol,someacids, anticonvul-sants,mercury,radiation,andviralagents,amongothers, mayresultincorticaldevelopmentdisordersinthefetus.17
Microcephalydiagnosis
Theobservedassociation betweenfetalinfectionbyZikaV andtheoccurrenceofmicrocephalyat birthhasincreased the importanceof an accurate diagnosis of microcephaly. It is necessary toidentify possible casesand at the same time,avoidexpensiveinvestigationandastateofalertness inthehealthcaresystem.Inpractice,aheadcircumference atbirthsmallerthantwostandarddeviationsofthemeanfor gestationalagehasbeenusedforclinicaldiagnosisof micro-cephaly. Reportson theprevalence of microcephalyusing thiscriterionwereapproximately0.5%,whichiswellbelow what would beexpected for twostandard deviations.19,20
This is probably due to a non-normal distribution of the measured head circumference. Severe microcephaly, i.e., smallerthanthreestandarddeviationsofthemean,occurs in1per1000births.19
Although it is a relatively simple and reliable diagnos-tic method,the simple head circumference measurement might not reflectan abnormally small brainand does not offerdatatodemonstrateanabnormalskullshape.Thus,it isextremelyimportantthatthemeasurementandits inter-pretationarecorrect.
Table1 Milestonesofcentralnervoussystemdevelopment.
Milestonesof development
Description Periodofoccurrence Malformationsorresulting diseases
Primary neurulation
Formationoftheneuraltube, caudalportion
3rd---4thweekofgestation Totalcraniorachischisis Anencephaly
Myeloschisis Encephalocele Myelomeningocele
Arnold---Chiarimalformation Secondary
neurulation
Neuraltubeformation,sacral portionandcoccyxofthe spinalcolumn
4th---5thweekofgestation Occultdysraphicstates (myelocystoceles, diastematomyelia, meningocele,lipoma, teratoma,dermoidcyst) Prosencephalon
development
Neuraltubeventralinduction, faceandcerebralhemispheres formation
2nd---3rdmonthofgestation Aprosencephaly Atelencephaly Holoprosencephaly Agenesisofthecorpus callosum
Agenesisofseptumpellucidum Septo-opticdysplasia
Proliferation Neuronalproliferation,of radialglialcellsandglia
3rd---4thmonthofgestation Microcephaly Macrocephaly Neuronal
migration
Dislocationofneuronalcells fromthegerminalmatrixto thecerebralcortex
3rd---5thmonthofgestation Lissencephaly Schizencephaly Pachygyria Polymicrogyria Neuronalheterotopia Focaldysplasias Organization Neurondifferentiation
(alignment,formationof corticallayers),synapse development(axonaland dendriticbranching), apoptosis,proliferationand differentiationofglia
5thmonthandpostnatal Idiopathicmentalretardation DownSyndrome
Fragile-Xsyndrome Angelmansyndrome Autism
Potentialdisordersassociated withprematurityand malnutrition
Periandpostnatalinjuries Myelination Acquisitionofthemyelin
sheaththatwillcoverthe axons
Birthandpostnatal Whitematterhypoplasia Malnutrition
Prematurity
Organicacidemiaand aminoacidopathies
ModifiedfromVolpe.12
tapearoundthehead,byplacingitontheforeheadabove the eyes, passing it above the ears and the most promi-nent portionofthe backof theskull. Infull-term babies, thisperimetermustbegreaterthan32cm(smallvariation by gestational age and gender). The head circumference increasesalmostlinearlyupto37---38weeksofgestation.21
The choiceofthecurveandthecriteriausedtodefine microcephalyhasbeenthesubjectofextensivediscussion, especiallyregardingpreterminfants.22,23ThePan-American
HealthOrganization suggestsusingboth theFentoncurve andthecurve ofthe InterGrowthstudy.24---26 However,the
analysis made by Victora etal. shows how the choice of thecurvecanhave animpactonthenumberofsuspected cases,exponentially increasingthe numberof children to
beinvestigatedandexposedtoCTradiation.Theseauthors suggestthat toolswithgreater specificityshouldbegiven priority, such as the InterGrowth curve in exchange for sensitivity.23
It is also importantto performan analysisof the pro-portionof headcircumferencein relationtoothergrowth measures,suchasweightandlength,inordertodefinethe suspectedmicrocephalyetiology.19
In spite of being an objective measure, a study that assessedinterobservervariationshoweddifferencesofmore than 2cm in 5% of them.27 Therefore, the staff that
In the presence of abnormal skull shapes due to fam-ily,geneticcharacteristics, ormoldingcausedbythebirth process,theheadcircumferencemeasurementcanbe mis-leading and not reflect a reduction in brain tissue. One suggestionto reduce microcephaly misdiagnosiswould be torepeatthemeasurementsoneormoredaysafterbirth, especiallyinthepresenceofoverridingsuturesatbirthwith borderlinemeasures.Theabnormalshapeshouldleadto fur-therassessmentforthepresenceofcraniosynostosisand/or geneticdiseases.
Etiologicaldifferentialdiagnosisofmicrocephalies
The more adequate term is microcephalies, considering the different forms, etiologies, and clinical expression. The pathogenesisof microcephaly isheterogeneous, from geneticcauses toenvironmentalfactors thatcan have an impact on neurodevelopment and, thus, influence brain growth.Therefore,any factorthatcan interferewithcell proliferationand/ordifferentiation,celldeath,among oth-ers,caninducemicrocephaly.Thesefactorsmayaffectthe braindevelopmentonlyor impairotherpartsofthebody, determiningdysmorphisms(syndromicmicrocephalies).22,28
Tofacilitatetheclinicalinvestigationandthedifferential diagnosisofmicrocephalies,theywillinitiallybeclassified basedonthe timeof diagnosis. Thus, microcephaliescan be divided into two categories: congenital microcephaly, which is present from birth and postnatal microcephaly, whichdevelopsaftertheneonatalperiodand,ingeneral, inthefirsttwoyearsoflife.22,28---30Themicrocephaliesmay
begeneticoracquired,withthelatterencompassing exter-nal/environmentalfactorsthat are potentially harmful to thebrain.
In acquired congenital microcephalies, aggressive fac-tors act during the intrauterine brain development. These factors include maternal infections (toxoplasmo-sis,cytomegalovirus,herpesvirus,syphilis,rubella,human immunodeficiency virus [HIV], and now the possible association with ZikaV), exposure to drugs/toxic sub-stances, especially the maternal consumption of alcohol (fetal alcohol syndrome), radiation, disruptive factors thatdisruptnormalbraindevelopment(e.g.,hemorrhage, ischemia,hypoxic---ischemicsyndrome,andtraumaticbrain injury), and nutritional deficiency (maternal malnutri-tion,placentalfailure,hypothyroidism,ormaternalfolate deficiency).22,28,31---33
Thegeneticcongenitalmicrocephaliesmaybeassociated withchromosomalabnormalities orcertaingenes, suchas theautosomalrecessiveprimarymicrocephaly(alsotermed microcephalyprimary hereditary [MCPH], and historically knownas microcephaly vera), in which at least 12 genes have been identifiedandencode proteins associated with the centrosome.34,35 Herethe term primary microcephaly
correspondstothosecasesinwhichthereductioninbrain volumeis primarily due to the reductionof the neuronal populationduringneurogenesis.29,36 Ingeneral,theoverall
structureofthebrainismaintainedinMCPHandthereare noothermalformationsoralterationsinbraindevelopment patterns.
Postnatal microcephalies are those in which the child isbornwithnormalhead circumference,withareduction
in headgrowth velocityovertime,reachingmicrocephaly levels. The postnatal-onset microcephaliesare associated withgenetic causes or external/environmental (acquired) factors.22
Examples of acquired postnatal microcephaliesinclude those resulting from traumatic brain injury, cerebral ischemia/hemorrhage, encephalitis, and severe malnutri-tion, among others. Several postnatal microcephalies are determinedbymutationsthatinterferewiththeregulation ofgeneexpressionduringbraindevelopment.30
Among the genetic postnatal microcephalies, all asso-ciated with mutations (deletion, insertion, duplication, fusion,andaminoacidpoint mutations),arethose result-ing from inborn errors of metabolism, neurodegenerative diseases, and several syndromes, such as Angelman syn-drome,Pitt---Hopkinssyndrome,Rubinstein---Taybisyndrome, Christianson syndrome,and MECP2-relateddisorders (Rett syndrome).30
Knowledge of the prevalence, clinical history, and detailedclinicalandneurologicalassessmentcanleadtothe diagnosis.Theclinicalhistorymayrevealexposuretoagent, accident,orepisodeharmfultothebrain,andtheclinical assessmentmaysuggestsomelesscommonsyndromes.
TheZikaV
The ZikaV, which belongs to the Flaviviridae family, is relatedtootherflavivirusesofmedicalrelevance transmit-ted byarthropodvectors,such asthe causativeagents of dengue fever, Chikungunya fever, yellow fever, and West Nile encephalitis. The ZikaV was isolated in 1947 from non-human primates (sentinel monkeys for yellow fever monitoring)intheZikaforestinUganda,whichwasadopted asthenameforthisvirus.37
There are at least two lineages of ZikaV, the African lineage (which some authors divide into West and East Africa)andtheAsianlineage.Phylogeneticstudiesindicate thatthevirus currentlyspreadingin theAmericasderived fromtheAsianlineage.38ZikaVtransmissionoccurs
primar-ilythroughavector,theAedesmosquitoes;inthesylvatic cycle,throughspeciessuchasA.albopictus,amongothers, whereas in the urban cycle, the A. aegyptiis the vector. Thevirusistransmittedbythehematophagousvectorduring feeding,bylodgingintheirsalivaryglands,whereit multi-plieswithoutaffectingtheinsect,remaininginitthroughout itslife.Inadditiontoprimates,itispossiblethatother mam-mals,suchaszebras,elephants,androdents, canalsobe naturalreservoirsofZikaV.
Flavivirusesaresmall(∼50nm)spherical particles,
sur-roundedbyalipidenvelope.39 TheZikaVisasingle-strand
RNAviruswith10.794kilobase,withtwonon-codingregions and a long readingframe encoding apolyprotein. That is cleavedbyhostcellproteasestooriginatethecapsidprotein C,theprecursorofmembrane(prM)andenvelopeEprotein, andseven non-structuralproteins,called NS1toNS7.The virions, orviralparticles,contain180copies ofproteinE, unknownamountsofother proteins,andasinglemolecule ofviralRNA.The surfaceofthevirionsisformedbyEand Mproteins.The Eprotein(∼53kDa)isglycosylated, being
cell.40 Ithasbeenpostulatedthatvirionsareendocytosed
andexposure tothe acidicenvironmentin lysosomes pro-motes thefusionbetween thevirus envelopeandthe cell membranes.UponreleaseofviralRNAintothecytoplasmof infectedcells,itisreplicatedandtranslatedbythecellular machinery,leadingtotheformationofnewviralparticles.
TwocompletegenomesoftheZikaV,includingthecurrent variety circulating inthe Americas arenowavailable.38,41
Faye et al. studied 37 virus isolates from different sources(mosquitoes,patients,andanimals,amongothers.) obtainedinAfrica,showingevidenceofgenetic recombina-tionandhowchangesintheglycosylationpatternofprotein EarelikelyadaptationstothevectorA.dalzielii.40 Freire
etal.,wheninvestigating17genomicsequencesofthevirus, suggestedthatchangesintheuseofcodonsfortheNS1 pro-teinintheAsianlineageoftheZikaVcanbecorrelatedwith higherratesofreplicationandviraltiterinhumans.42
Intrauterineviralinfectionsthatresultininjuriestothe centralnervoussystemarerelativelyrare;cytomegalovirus, herpesvirus,andrubellaareamongthosealreadyknownto causefetaldiseases.AmongFlaviviruses,onlyafew cases of West Nile encephalitis virus in pregnant women were reportedastheprobable causeofneurologicaldamagein fetuses.43
EpidemiologyandsurveillanceprotocolinBrazil
ThefirstcasesofhumaninfectionwerereportedinNigeria andTanzaniafrom1952to1954.37Theviruslaterspreadto
theAsiancontinentand theinternationalcommunityonly started to recognize the epidemic potential of the ZikaV after2005andespeciallyafterthe2007outbreakin Microne-sia (Yap island in the Pacific Ocean) and the 2012/2013 outbreakinFrenchPolynesia.Importedcaseswerereported after 2013 in Germany, Canada, Italy, Japan, the United States,andAustralia.In2014thepresenceoftheviruswas describedintheEasterIsland(Chile---PacificOcean).44On
April 29, 2015, the circulation of this virus wasdetected for the firsttimein Brazil andLatin America (continent). ResearchersfromtheUniversidadeFederaldaBahia(UFBA) reportedtheidentificationofZikaVbyRT-PCRineightofthe 25testedsamples(Camac¸ari/BA).3,45
InOctober2015,theBraziliangovernmentinitiatedjoint investigationswiththestateofPernambucoafterobserving theincreasingnumberofcasesofmicrocephaly,especially in that state, after confirmation of the alteration in the pattern of microcephaly cases. In November, it launched the firstNational GuidelineonMicrocephalies, which still included the diagnosis of microcephaly through head cir-cumference(HC)measurement≤33cm.Inthatsamemonth,
afterconfirmationofthepresenceofZikaVintheamniotic fluidofpregnantwomeninthestateofParaibabyFiocruz, the association of ZikaV infection withmicrocephaly was confirmed.46 In December, the government released the
Microcephaly Protocol --- Surveillance --- Version 1, chang-ing the diagnosis of microcephaly, which started to be consideredwhenHCwas≤32cm,alsoincludinginthis
proto-colpregnantwomenwithrash,miscarriage,microcephalic fetus, and stillbirth.44 On December 14, the government
releasedtheMicrocephalyProtocol---HealthCare.Itisworth mentioningthatthischangeinheadcircumferencemeasure
forthediagnosisofmicrocephalycaninfluencedata analy-sis.
InJanuary2016,theNationalGuidelineforEarly Stimu-lationofBabieswithMicrocephalywasreleased.Fourcases related toZikaV were also identified by the CDC in that month. The Brazilian government has made adjustments in the operational definitions of cases: (A) Definitions of casesformicrocephalysurveillance:(i)Newbornwith micro-cephaly,(ii)Miscarriagesuggestiveofcongenitalinfection, (iii)Stillbirthwithmicrocephalyand/orCNSmalformations suggestive of congenital infection, (iv) Fetus with micro-cephaly and/or CNS alterations, suggestive of congenital infection; and (B) Definitions of cases for surveillance of ZikaVinfectionduringpregnancy:(i)Pregnantwomanwith acuterash,suggestiveofZikaVinfection.46
The suspected microcephaly cases must be reported immediatelytothehealthauthoritiesandregisteredatthe Public Health Event Registration Form (Registro de Even-tosdeSaúdePública[RESP]---Microcephalies),availableat:
www.resp.saude.gov.br.Thenotificationofsuspectedcases ofmicrocephalyintheRESPdoes notexcludetheneed to reportthecasetotheLiveBirthsInformationSystem (Sis-temadeInformac¸õessobreNascidosVivos[SINASC]).47,48
AftertheestablishmentoftheassociationofZikaVwith microcephaly,itisnecessaryforcareandprevention meas-urestobecarriedoutandintensified,butitisessentialto explainandsooththepopulation,andtoanalyzetheactual numberofcases.
On January 20, 2016, the Brazilian Ministry of Health issued an epidemiological report with some relevant and interesting changes, such as changing the name ‘‘SurveillanceandResponseProtocoltotheOccurrenceof MicrocephalyrelatedtoZikaVinfection’’to‘‘Surveillance andResponseProtocoltotheOccurrenceofMicrocephaly,’’ regardlessofthecause.Thissamereportdescribes,in sep-arate, the 224 cases of microcephaly confirmed through imagingassessment,withtypicalalterationinthesixcases withpositivesampleforZikaV.49
Another epidemiological report on February 2, 2016 was issued with a cumulative total (2015---2016) of 4783 reportedcases of microcephaliesand/or other CNS disor-ders, including possible cases related toZikaV and other infections.ItisimportanttonotethatBrazildoesnothave almost5000cases ofZikaV-relatedmicrocephaly,asmany patientsand alsosome health professionalsmay imagine. Infact,thisnumbercorrespondstothenotificationof sus-pectedcases:thenumberofcasesstillunderinvestigation is3670, whereas the numberof cases alreadyassessed is around1113.Oftheseassessedcases,microcephalyrelated to congenital infection was ruled out in 709 (63%). The remainingcases,404(37%),wereconsideredconfirmedfor microcephalyand/orotherCNSabnormalities,althoughthe identificationof theZikaV presence inthe amnioticfluid, placenta and fetal tissues occurred in only 17 cases to date.49
confirmed cases: Pernambuco has 167 cases, followed by Bahia(101),RioGrandedoNorte(70),Paraíba(54),Piauí (29), Alagoas (21), Ceará (11) Espírito Santo (3), Rio de Janeiro (t2), Pará (1), Goiás (1), Mato Grosso doSul (1), andRioGrandedoSul(1).50
The Brazilian Medical Genetics Society-Zika embryopa-thyTaskForceindicatesfourcasereportlimitations.First, apreviousunderreportingofactualcasesofmicrocephalies inBrazilandthefactthatthenotificationprotocolitselfmay havefavoredtheincreaseofreportedcases.Second,mild casesofmicrocephalymightnothavebeennotifiedbecause theheadcircumferencemeasurementwasnotroutinely per-formed. Third, the ZikaV infection was not confirmed in newborns and mothers by a laboratory, and a history of non-specificrashillnessduringpregnancyissubjectiveand can lead toa recall bias, resulting in misclassification of potentialexposuretoZikaV.Fourth:thereportingofcases doesnotcommentonothercommonfindingsinintrauterine infections,suchashepatosplenomegaly,skinrash, choriore-tinitis,or somecharacteristics thathavebeenreportedin casesofsuspectedZikaVinfection,includinghearingloss, palemacula,andswallowingdifficulties.5
This analysis of the numbers should not be used to decreasepreventive measures; however, itwould bevery interestingtoadvisepregnantwomentoadoptmeasuresto reducethe presenceof the Aedesaegypti,byeliminating breedingsitesandprotectingthemselves againstmosquito exposure,bykeepingdoorsandwindowsclosedorscreened, wearinglongpantsandlong-sleevedshirts,andusing repel-lentsallowedduringpregnancy.
Multidisciplinaryadvice,suchastheroutineassessment ofachildatthepediatrician,canbeanopportunityforthese womentoreceiverecommendationsonplanningtheirnext pregnancyandthattheyshouldconsultwiththe gynecolo-gistbeforestoppingtheircontraceptivemethods.
ClinicalpictureofZikaVinfectionsanddifferential
diagnosiswithdengueandChikungunyafever
The dengue andChikungunya viruses have similar clinical signsand symptoms, especiallyin the early stages of the disease.51 ThisalsooccurswithZikaV.Forthisreasonitis
essentialtodifferentiatebetweenthesethreediseases.
Zika
Approximately 80% of infected individuals are asymptomatic.52,53 When present, symptoms can last
fromafewdaystooneweek. Symptomsareusuallymild, with characteristic sudden onset of fever, arthralgia, maculopapularrash,ornonpurulentconjunctivitis. Accord-ingtodatafrompreviousoutbreaks,severeformsarerare andthatisthereasonwhyhospitalizationsanddeathsare unusual.53,54 According to the CDC, the diagnosis of Zika
shouldbesuspectedwhentwoormoresymptoms(including fever,rash,arthralgia,orconjunctivitis)arepresentduring or withinaperiodof uptotwoweeks afterstaying in an endemicareaforthevirus.55
During the 2007 Zika outbreak in Micronesia, the mostfrequentsymptomswereskin rash,fever,arthralgia, and conjunctivitis;headache, myalgia, retro-orbital pain, edema,andvomitingwerelesscommon.Ofthe49confirmed
cases,nohospitalizations, hemorrhagicmanifestations,or deathswerereported.53
Denguefever
Dengue should be suspected in all patients residing in endemicareasorwhotraveledtotheseregionsinthepast twoweeks.56Thediagnosisshouldbeconsideredinpatients
with fever (sudden onset, with a peak of 39---40◦C), dif-fuse skin flushing, leukopenia,and thrombocytopenia.57,58
The symptoms last for approximately five to seven days. Headache, arthralgia,back pain,myalgia, bone pain,and gastrointestinalsymptoms(anorexia,vomiting,and discom-fort)are common.Retro-orbital pain, afterlight pressure is applied to the eyeball, is also usual.56,57 Signs
sugges-tive ofhemorrhage include petechiae,purpura,epistaxis, gingivalandvaginalbleeding,melena,andhematemesis.In thissituation,physiciansmustbealertfor dengue hemor-rhagic fever, whichcan resultin circulatorycollapse and, consequently,shock.56,57
Chikungunya
Unlike dengue and Zika, most people infected with the Chikungunya virus are symptomatic, with less than 15% beingasymptomatic.59,60Thetimeofviremiaisusuallyone
week.61 The fever has a rapid onset, with high
tempera-tures(generally>39◦C),accompaniedbymyalgia,asthenia, headache, arthralgia, and rash. Soon after the onset of fever,therearecomplaintsofseveremyalgiaandarthralgia, whichwillevenpreventpatientambulation.62 Rashoccurs
in 20---80% of cases with maculopapular presentation and usuallylocatedonthetrunk.63Lesscommonandunspecific
symptomsincludepruritus,lymphadenopathy,anddigestive disorders.63 Patients requiring hospitalization are usually
elderlyandthosewithcoexistingdisorders(cardiac, respira-tory,neurological,ordiabetes).Anothergroupwithahigh risk for severe infection is the neonatalgroup (especially motherswhocarriedthevirusduringpregnancyand expo-sureduringbirth)andyoungchildren.64
Laboratorydiagnosis
Laboratory diagnosis of ZikaV infections is mainly based onmolecularbiologyandserologictests.65,66 Amplification
of theviral RNA throughreverse transcription-polymerase chainreaction(RT-PCR)canbeperformedinseveral biolog-icalmaterialssuchasserum,cerebrospinalfluid,amniotic fluid, saliva, and urine.9,10,67 In patients with suspected
infection by horizontaltransmission, itspositivity is asso-ciated with the acute phase of infection between three and seven days after the onset of symptoms, when low-levelviremiausuallyoccurs.3,65Whenavailable,theyarethe
diagnostictestsofchoiceaftertheacutephase.The inter-pretation of serologicaltests for ZikaV, such asELISA IgM andIgGorplaque-reductionneutralizationtest(PRNT)must beperformed carefully,astheyshowcross-reactivitywith otherarboviruses,especiallyinpatientspreviouslyinfected withotherflaviviruses,suchasdenguefever.65Ideally,
In suspectedcases,asthereis nocompleteknowledge of the accuracy of several tests in the diagnosis of con-genitalinfection,RT-PCRshouldbeperformedifavailable, ideallywithinthefirsttwodaysincordblood,cerebrospinal fluid,andplacenta, associatedtoantibody measurements incerebrospinalfluidandserum.Theimmunohistochemical testforZikaVintheplacentaandumbilicalcordshouldalso be performed wheneverpossible. The detection of ZikaV inanyoftheabovementionedmaterialsthroughRT-PCRor immunohistochemistry establishes a diagnosis of congeni-tal infection. The reagent serology is confirmatory when titers are higher than in dengue serology, as described above.In the eventof fetal death, the diagnosis consists of performing RT-PCR and immunohistochemistry in fetal tissue.67
NeuroimagingandZikaV
According to the guidelines of the American Academy of NeurologyonMicrocephaly,neuroimagingstudiesareuseful inidentifyingstructurallesionsintheassessmentofchildren withmicrocephaly,helpingintheinvestigationofgenetic, acquired,orenvironmentaletiologies;magneticresonance imaging(MRI)isthemostaccuratemethodforthe identifi-cationofspecificpatternsthatcanhelpdiagnosis.22
Regardingcongenitalinfections,themechanismof infec-tion and brain damage depends onthe etiological agent, determiningneuroradiologicalandpathological manifesta-tions with distinct patterns. Viral agents, for instance, tendtoproduceaselectivenecrosisof specificcelltypes, whereas bacteria and fungi are less selective. Moreover, different patterns of calcifications seen at the imaging and pathological studies aretypical of STORCH infections (syphilis,toxoplasmosis,rubella,CMV,HIV,andherpes sim-plex),andthetimeoftheinsultduringfetallifeisrelated totheteratogenicorencephaloclasticeffects.68
Themainobjectiveoftheimagingassessmentofa pos-sible intrauterine infection by ZikaV is the detection of neurologicalcomplicationsrelatedtotransplacental infec-tion,suchasmicrocephaly,cerebralcalcifications,neuronal migration disorders, loss of brain tissue, and ventricular system dilation. The extent and severity of intracranial alterations are directly related to the gestational period whenthefetuswasinfectedbythevirus;itismoresevere and extensive duringthe firsttrimester of pregnancy and milderinthethirdtrimester.Theimagingassessmentofthe fetus or newbornhasbeen indicated incases ofmaternal ZikaVinfection,eitherconfirmedorinconclusive,aswellas throughlaboratorytestsorcompatibleclinicalpictures.
Duringtheprenatalperiod,obstetricultrasonographyis theexamofchoiceandisrecommendedfortheinvestigation ofpossiblestructuralabnormalities ofthecentralnervous systemandformonitoringfetalandbraingrowtheverythree tofourweeks.69
Inthepostnatalperiod,transfontanellarultrasonography istheinitialmethodofinvestigationfor thenewbornwith aheadcircumference≤32cm.Thepresenceofany
abnor-malitiesdetectedbythetransfontanellarultrasoundshould be investigated throughmore detailed examinations with higherdiagnostic accuracy,suchascomputedtomography ormagneticresonanceimaging.67
Thebrainabnormalitiesresultingfromintrauterine infec-tion by ZikaV have been described mainly by computed tomographyinthepostnatalperiod.Themainimaging find-ingsoriginatefromaseriesof35casesofmicrocephaly,born tomotherswhohadcontactwithendemicareas.Ofthetotal of35infants,27weresubmittedtocomputedtomography andsubsequentlyreportedtotheCDC.5Theimagingfindings
inthatcohortconsistedofcerebralcalcifications, predomi-nantlyperiventricular,butalsoofcalcificationsinthebrain parenchyma,thalamus,andbasalganglia.Neuronal migra-tionanomalies werealso detected, suchaslissencephaly, pachygyria,andpolymicrogyria,presentinuptoone-third ofcases.Ventriculomegalysecondarytocortical/subcortical atrophy has also been often found.5 There are also case
reportsthat usedother imaging methods, suchas obstet-ric ultrasound to carry out intrauterine investigation of pregnantwomen with a history of ZikaV infection, which showedgross cerebral calcifications, abnormalities in the cerebellarvermisandcorpuscallosumdysgenesis.70
Recently, the case report of a fetus with confirmed ZikaVinfection submittedto autopsyand neuropathologi-calstudyshowedmicrocephaly,predominantlycorticaland subcorticalcalcifications,simplifiedgyralpattern,neuronal migration disorders, loss of brain tissue, and asymmetric ventricular dilation. Although that study did not include moreadvancedneuroimaging studies,thedescribed sono-graphic findings would certainly be better identified and demonstratedbyfetalor postnatalcomputed tomography ormagneticresonanceimaging.71
Strategiesforstudyingtheassociationbetween
ZikaVandmicrocephaly
Globalunderstanding ofnormalneurodevelopment andits possiblealterationsdependsonextensiveknowledgeofthe brain formation and the pattern of connections between neuronsandbetweenbrainregions,aswellasthesynaptic communications that constitute these adequate connec-tions.The newmethodsofcellandorganoidmodelsallow forinvitrosimulationsoftheprocessesinvolvedin embry-onicneurogenesis,thepossiblealterationsorinterventions thatmayberelatedtoabnormalbrain development.It is nowpossible toelucidate issues regarding the main gaps inknowledgeonbrainformation,generatinguniqueresults onembryonicneurogenesisand allthe processesinvolved duringcorticaldevelopment,aswellasthecomplete under-standing about the action of agents that can potentially causealterationsinembryonicneurodevelopment.
Humanneuronsand/orglialcellsarenotreadilyavailable for experimental research. Studies of pathologies associ-atedwiththecentralnervoussystemhavetraditionallybeen limitedtoanimalmodelsor lessrelevantcelllinesforthe understandingofneuronalpathophysiology.72---74The
impor-tance of using human cells similar to the disease to be investigatedis evident bythe number of drugsthat show efficacyandsafetywhentestedinanimalmodels,but sub-sequently fail in clinical trials.74 Thus, it is necessary to
The technology required to generate the so-called cellmodelsis currently available, capable ofreproducing somaticcellsattheembryoniclevel,orevenproducing mini-brainsfromthesereprogrammedcells.These modelshave highrelevanceforthestudyofdiseasesinhumans,providing excellentconditionsfor the understanding ofmechanisms andconstitutinganaccomplishedtoolforhigh-yield exper-iments,alsoallowingfortheconstructionofplatformsfor thescreeningofnewdrugsinseveraldiseases.72
Cellsobtainedbycellreprogrammingarecalledinduced pluripotentstemcells(iPS)andareverysimilartoembryonic stem cells, with the same characteristics of self-renewal and differentiation potential in three lines of embryonic leaflets.75,76 The use of the iPS cell generation
technol-ogy is based on two major action areas, the generation of specific cells for use in regenerative medicine, and/or modelingofdiseaseandscreeningfor newdrugs.iPScells can begenerated from patients witha particular disease or from healthy individuals, and subsequently differenti-atedintoadultcells.Basedondiseaseswhosephenotypeis expressedinadultcells,genomeeditingandcorrectioncan beperformed,aswellasscreeningforcompoundscapable ofcorrectingcelldisorderandevaluationofthepossible tox-icityofsomedrugsinthesecells.73FromaniPScell,invitro
smallorganoidswithaminiatureorganizationverysimilarto thatofthehumanbraincanbeobtained,whicharecalled mini-brains,beingabletorecapitulateasurprisingnumber ofbraindevelopmentcharacteristics.
Viral infections capable of promoting changes in neu-rodevelopmentcanbeinvestigatedthroughtheexposureof humaniPScellstoviruses,allowingforadetailedstudyof thedifferentstages of viralinfection progressionandthe consequences of exposure during embryonic brain devel-opment.D’Aiuto etal., in 2014, reported a study onthe susceptibility of human iPS cells to cytomegalovirus and its performance during the formation of an adult neu-ron.Thestudyshowedsignificantdifferencesinalterations causedbycytomegalovirustoembryoniccells,neural pre-cursorcellsandadultneurons,suggestingthatexposureto cytomegalovirusin the embryonicperiod is crucialtothe developmentofbrainmalformationscausedbythevirus.77
In cases of microcephaly caused by genetic muta-tions,for instance,mini-brainsweregenerated fromcells (iPS) derived from skin fibroblasts from a patient with microcephaly. The generated mini-brains resembled the phenotypeofmicrocephaly,beingmuchsmallerwhen com-paredwithmini-brainsgeneratedfromcontrolpatientcells, allowing for a detailed study of embryonic neurogenesis, especiallythecorticalformationofthesebrains.78,79
Discussion
TheassociationbetweenbytheZikaVinfectionduring preg-nancy andthe development of microcephalyhas alarmed thepopulationworldwide.5---8 Microcephalyisadisorderof
theneuronalproliferationphase,whichoccursearlyin preg-nancy (third to fourth month)12 and, in some described
cases,appearstocoincidewiththesymptomsofthe infec-tion in the mother. As the criteria for the definition of microcephalyhavenotbeenusedinastandardizedmanner andastherewasclearlyanunderreportingofsuchcasesin
Brazil,itisdifficulttoestablishwithcertaintywhetherthere is a real increase in the incidence of this pathology.22---26
Additionally, theavailableneuroimagingstudies showthat othermalformationsoffetalcorticaldevelopmentarealso present,suchasneuronalmigrationdisorders(thirdtofifth month of pregnancy) and diffuse calcifications (neuronal death), suggesting either a long term of the virus patho-genesisintheCNS,orthesusceptibilityofmorephasesof corticaldevelopment.5,12---14,70
ConsideringthebroaddisseminationoftheAedesaegypti
in Brazilandthatthe methodsusedfor vector population controlareslowtoshowresults,it isexpectedthatcases ofZikaVinfectionwillcontinuetoincrease,theacquisition ofmoreknowledgeaboutboththepathologyandthe etio-logicalagentanurgentpriority.Recentstudiessuggestthat alterationsinthemolecularcomponentsofZikaV,especially oftheEproteinpresentonthevirussurface,couldbe cor-related withan increased ‘‘aggressiveness’’ of the ZikaV, reinforcingitsneurotropismandcapacitytocausediseasein humans.40,42Thesituationrequiresmultipleand
multidisci-plinaryapproachestocontrolthevectorandZikaVinfection, includingtheeducationofthepopulation.Awell-informed pediatricianisacentralpartofthisprocess.
ItisafactthattheZikaVcanovercometheplacental bar-rierandreachtheamnioticfluidandfetaltissues.11Butitis
necessarytoreassurepregnantwomen,asitisnotpossible toaffirmthatthisincreaseinmicrocephalynotifications is solelyrelatedtothevirus,asmanyinitiallysuspectedcases wereruledout.23Caseswithlaboratoryconfirmationarefew
in relation tothe high number of notifications; neverthe-less,preventionmeasuresarestillnecessaryandshouldbe identified.
Theavailability oftests forthe laboratory diagnosis of ZikaVinfection,bothintheacutephaseandlater,isstillvery restricted.The difficultyin confirmingor ruling out infec-tionalsoaffectstheunderstandingofthenaturalcourseof thediseaseanditsassociationwithmicrocephalyandalso withGuillain---Barrésyndrome.54Becauseofthegreat
world-wideconcernregardingtheteratogenic potentialofZikaV infection,therewillbegreatereffortsforthedevelopment of moreaffordable testing withgreater accuracy,suchas serologywithlessriskofcross-reactivity.80
In conclusion, there is a clear temporal association betweenthe increasedreportingof casesofmicrocephaly andtheZikaVepidemic,mainlyintheNortheastofBrazil. However, the development of diagnostic techniques to confirm a cause-and-effect association, the pathogenesis mechanismsof ZikaV infectionin thecentralnervous sys-tem, and more adequately defined diagnostic criteriafor theidentification of casesof microcephalythat shouldbe submittedtoinvestigationarestillrequired.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
References
1.Gulland A. Zika virus is a global public health emergency, declaresWHO.BMJ.2016;352:i657.
2.Salvador FS, FujitaDM. Entry routes for Zika virus inBrazil after2014worldcup:newpossibilities.TravelMedInfectDis. 2016;14:49---51.
3.CamposGS,BandeiraAC,SardiSI.Zikavirusoutbreak,Bahia, Brazil.EmergInfectDis.2015;21:1885---6.
4.Bogoch II, Brady OJ, Kraemer MU, German M, Creatore MI, KulkarniMA,etal.AnticipatingtheinternationalspreadofZika virusfromBrazil.Lancet.2016;387:335---6.
5.Schuler-FacciniL,RibeiroEM,FeitosaIM,HorovitzDD, Caval-cantiDP,PessoaA,etal.BrazilianMedicalGeneticsSociety ---ZikaEmbryopathyTaskForce.PossibleassociationbetweenZika virusinfectionand microcephaly--- Brazil,2015.MMWRMorb MortalWklyRep.2016;65:59---62.
6.ButlerD.Zikavirus:Brazil’ssurgeinsmall-headedbabies ques-tionedbyreport.Nature.2016;530:13---4.
7.DickGW,KitchenSF,HaddowAJ,ZikavirusI.Isolationsand sero-logicalspecificity.TransRSocTropMedHyg.1952;46:509---20. 8.Bell TM, Field EJ, Narang HK. Zika virus infection of the
central nervous system of mice. Arch Gesamte Virusforsch. 1971;35:183---93.
9.MussoD,RocheC,NhanTX,RobinE,TeissierA,Cao-Lormeau VM.DetectionofZikavirusinsaliva.ClinVirol.2015;68:53---5. 10.Gourinat AC, O’Connor O, Calvez E, Goarant C,
Dupont-RouzeyrolM.DetectionofZikavirusinurine.EmergInfectDis. 2015;21:84---6.
11.Besnard M, Lastere S, Teissier A, Cao-Lormeau V, Musso D. Evidence of perinatal transmission of Zika virus, French Polynesia,December 2013and February 2014. EuroSurveill. 2014;9:pii:20751.
12.VolpeJJ.Neurologyofthenewborn.4thed.Philadelphia:WB Saunders;2001.
13.RakicP.A smallstepfor thecell,a giantleapfor mankind: ahypothesisofneocorticalexpansionduringevolution.Trends Neurosci.1995;18:338---88.
14.RakicP.Neuronalmigrationandcontactguidanceintheprimate telencephalon.PostgradMedJ.1978;54:S25---40.
15.GreigLC,Woodworth MB,GalazoMJ,PadmanabhanH, Mack-lis JD. Molecular logic of neocortical projection neuron specification, development and diversity. Nat Rev Neurosci. 2013;14:755---69.
16.RorkeLB.Aperspective:theroleofdisorderedgeneticcontrol ofneurogenesisinthepathogenesisofmigrationdisorders.J NeuropatholExpNeurol.1994;53:105---17.
17.GoldenJA.Cellmigrationandcerebralcorticaldevelopment. NeuropatholApplNeurobiol.2001;27:22---8.
18.Arai A, Saito T, Hanai S, Sukigara S, Nabatame S, OtsukiT, etal.Abnormalmaturationanddifferentiationofneocortical neuronsinepileptogeniccorticalmalformation:unique distri-butionoflayer-specificmarkercellsoffocalcorticaldysplasia andhemimegalencephaly.BrainRes.2012;1470:89---97. 19.VargasJE,AllredEN,LevitonA,HolmesLB.Congenital
micro-cephaly: phenotypic features in a consecutive sample of newborninfants.JPediatr.2001;139:210---4.
20.DolkH.Thepredictive valueofmicrocephalyduringthefirst yearoflifeformentalretardationatsevenyears.DevMedChild Neurol.1991;33:974---83.
21.WorldHealthOrganization(WHO).TheWHOchildgrowth stan-dards. 2016. Available from: www.who.int/childgrowth/en/ [cited12.02.16].
22.Ashwal S, Michelson D, Plawner L, Dobyns WB. Practice parameter: evaluation of the child with microcephaly (an evidence-basedreview):reportoftheQualityStandards Sub-committee of the American Academy of Neurology and the
PracticeCommitteeoftheChildNeurologySociety.Neurology. 2009;73:887---97.
23.VictoraCG,Schuler-FacciniL,MatijasevichA,RibeiroE,Pessoa A,BarrosFC.MicrocephalyinBrazil:howtointerpretreported numbers?Lancet.2016;387:621---4.
24.PanAmericanHealth Organization(PAHO). Lineamientos pre-liminares de vigilanciademicrocefalia enreciennacidos en entornosconriesgodecirculaciondevirusZika;Jan22,2016. Washington,DC:PanAmericanHealthOrganization;2016. 25.FentonTR,KimJH.Asystematicreviewandmeta-analysisto
revisetheFentongrowthchartforpreterminfants.BMCPediatr. 2013;13:59.
26.Villar J, Cheikh Ismail L, Victora CG,Ohuma EO, BertinoE, Altman DG,et al.,For the International Fetal and Newborn GrowthConsortiumforthe21stCentury(INTERGROWTH-21st). Internationalstandardsfornewbornweight,length,andhead circumferencebygestationalageandsex:theNewborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet. 2014;384:857---68.
27.BhushanV,PanethN.Thereliabilityofneonatalhead circum-ferencemeasurement.JClinEpidemiol.1991;44:1027---35. 28.PassemardS,KaindlAM,VerloesA.Microcephaly.In:Elsevier
BV,editor.Handbookofclinicalneurology,pediatricneurology partI.2013.p.129---41.
29.Woods CG. Human microcephaly. Curr Opin Neurobiol. 2004;14:112---7.
30.SeltzerLE,PaciorkowskiAR.Geneticdisordersassociatedwith postnatalmicrocephaly.AmJMedGenetCSeminMedGenet. 2014;166:140---55.
31.European Centrefor DiseasePrevention and Control (ECDC). Rapid risk assessment: microcephaly in Brazil potentially linked to the Zika virus epidemic. Stockholm: ECDC; 2015. p. 1---12. Available from: http://ecdc.europa.eu/ en/http://ecdc.europa.eu/en/publications/Publications/zika-microcephaly-Brazil-rapid-risk-assessment-Nov-2015 [cited 12.02.16].
32.PAHO/WHO.Neurologicalsyndrome,congenitalmalformations, andZikavirusinfection.Implicationsforpublichealthinthe Americas.EpidemiologicalAlert;2015.p.1---11.Availablefrom: http://www.paho.org/hq/index.php?option=comdocman& task=docview&Itemid=270&gid=32405&lang=em [cited 12.02.16].
33.Tetro JA. Zika and microcephaly: causation, correlation, or coincidence? Microbes Infect. 2016. Available from: http:// linkinghub.elsevier.com/retrieve/pii/S1286457916000083 [cited12.02.16].
34.FaheemM,NaseerMI,RasoolM,ChaudharyAG,KumosaniTA, IlyasAM, etal. Moleculargenetics ofhuman primary micro-cephaly:anoverview.BMCMedGenomics.2015;8:S4. 35.Hussain MS, Baig SM,Neumann S, PecheVS, Szczepanski S,
NürnbergG,etal.CDK6associateswiththecentrosomeduring mitosisandismutatedinalargePakistanifamilywithprimary microcephaly.HumMolGenet.2013;22:5199---214.
36.ThorntonGK, WoodsCG.Primary microcephaly:do allroads leadtoRome?TrendsGenet.2009;25:501---10.
37.IoosS,MalletH-P,LeparcGoffartI,GauthierV,CardosoT,Herida M.CurrentZikavirusepidemiologyandrecentepidemics.Med MalInfect.2014;44:302---7.
38.EnfissiA,CodringtonJ,RoosbladJ,KazanjiM,RoussetD.Zika virusgenomefromtheAmericas.Lancet.2016;387:227---8. 39.LindenbachBD,RiceCM.MolecularbiologyofFlaviviruses.Adv
VirusRes.2003;59:23---61.
40.FayeO,FreireCC,IamarinoA,FayeO,deOliveiraJV,DialloM, etal.MolecularevolutionofZikavirusduringitsemergencein the20thcentury.PLoSNeglTropDis.2014;8:e2636.
42.FreireCC,IamarinoA,NetoD,SallAA,ZanottoPM.Spreadof thepandemicZikaviruslineageisassociatedwithNS1codon usage adaptation in humans. bioRxiv. 2015. Available from: http://dx.doi.org/10.1101/032839[cited12.02.16].
43.Sirois PA, Pridjian G, McRae S, Hinckley AF, Rasmussen SA, KissingerP,et al.Developmentaloutcomesinyoungchildren borntomotherswithWestNileillnessduringpregnancy.Birth DefectsResAClinMolTeratol.2014;100:792---6.
44.Brasil.MinistériodaSaúde.SecretariadeVigilânciaemSaúde. Departamentode VigilânciadasDoenc¸as Transmissíveis. Pro-tocolo de vigilânciae respostaà ocorrência de microcefalia relacionadaà infecc¸ãopelovírusZika.Brasília:Ministérioda Saúde;2015.p.55.
45.CardosoCW,PaploskiID,KikutiM,RodriguesMS,SilvaMO, Cam-posGS,etal.Outbreakofexanthematousillnessassociatedwith Zika,Chikungunya,anddengueviruses,Salvador,Brazil.Emerg InfectDis.2015;21:2274---6.
46.COES. Microcefalias atualizac¸ões: entrevista coletiva sobre microcefalia.Brasil:MinistériodaSaúde;2016January20. 47.Protocolodeatendimento:mulheresemidadefértil,gestantes,
puérperas e bebês com microcefalia. Brasil: Ministério da Saúde;2015.Availablefrom:http://portalsaude.saude.gov.br/ images/pdf/2015/dezembro/14/Protocolo-de-Atendimento. pdf[cited13.03.16].
48.Brasil. Ministério da Saúde.Protocolo de atenc¸ãoà saúde e respostaàocorrênciademicrocefaliarelacionada àinfecc¸ão pelovírusZika.V.1.1.Brasília:MinistériodaSaúde,Secretaria deAtenc¸ãoàSaúde;2015.
49.Boletim epidemiológico. Brasil: Ministério da Saúde; 2016. Available from: http://portalsaude.saude.gov.br/index.php/ cidadao/principal/agencia-saude/21801-ministerio-da-saude-atualiza-casos-de-microcefalia-2[cited12.02.16].
50.Boletim epidemiológico. Brasil: Ministério da Saúde; 2016. Available from: http://portalsaude.saude.gov.br/index.php/ cidadao/principal/agencia-saude/21890-ministerio-da-saude-investiga-3-448-casos-suspeitos-de-microcefalia [cited 12.02.16].
51.Mardekian SK, Roberts AL. Diagnostic options and chal-lenges for dengueand Chikungunya viruses. BiomedResInt. 2015;2015:834371.
52.Hayes EB. Zika virus outside Africa. Emerg Infect Dis. 2009;15:1347---50.
53.DuffyMR,ChenTH,HancockWT,PowersAM,KoolJL,Lanciotti RS,etal.ZikavirusoutbreakonYapIsland.FederatedStatesof Micronesia.NEnglJMed.2009;360:2536---43.
54.European Centre for Disease Prevention and Control. Rapid riskassessment:ZikavirusepidemicintheAmericas:potential association with microcephaly and Guillain---Barré syndrome. Stockholm,Sweden: European Centre for DiseasePrevention andControl;8February2016.
55.StaplesJE, DziubanEJ,FischerM,CraganJD,RasmussenSA, Cannon MJ, et al. Interimguidelines for the evaluation and testing of infants withpossible congenital Zika Virus infec-tion --- United States, 2016. MMWR Morb Mortal Wkly Rep. 2016;65:63---7.
56.WorldHealthOrganization,SpecialProgrammeforResearchand TraininginTropicalDiseases(TDR).Dengueguidelinesfor diag-nosis,treatment,preventionandcontrol.Geneva:Newedition; 2009.
57.KularatneSA.Denguefever.BMJ.2015;351:h4661.
58.TeixeiraMG,BarretoM.Diagnosisandmanagementofdengue: clinicalreview.BMJ.2009;339:1189---93.
59.Weaver SC, Lecuit M. Chikungunya virus and the global spreadofamosquito-bornedisease.NEnglJMed.2015;372: 1231---9.
60.BrouardC,BernillonP,QuatresousI,PillonelJ,AssalA,DeValk H,etal.EstimatedriskofChikungunyaviremicblooddonation
duringanepidemiconReunionIslandintheIndianOcean,2005 to2007.Transfusion.2008;48:1333---41.
61.Thiberville SD, Boisson V, Gaudart J, Simon F, Flahault A, deLamballerie X.Chikungunyafever: aclinicaland virologi-calinvestigationofoutpatientsonReunionIsland,South-West IndianOcean.PLoSNeglTropDis.2013;7:e2004.
62.CapedingMR,ChuaMN,HadinegoroSR,HussainII,NallusamyR, PitisuttithumP,etal.Dengueandothercommoncausesofacute febrileillnessinAsia:anactivesurveillancestudyinchildren. PLoSNeglTropDis.2013;7:e2331.
63.JavelleE,TiongTH,Leparc-GoffartI,SaviniH,SimonF. Inflam-mation of the external ear in acute chikungunya infection: experiencefromtheoutbreakinJohorBahru,Malaysia,2008. JClinVirol.2014;59:270---3.
64.Gérardin P, Barau G, Michault A, Bintner M, Randrianaivo H, Choker G, et al. Multidisciplinary prospective study of mother-to-childchikungunyavirusinfectionsontheislandof LaRéunion.PLoSMed.2008;5:e60.
65.LanciottiRS,KosoyOL,LavenJJ,VelezJO,LambertAJ,Johnson AJ,etal.GeneticandserologicpropertiesofZikavirus asso-ciatedwithanepidemic,YapState,Micronesia,2007.Emerg InfectDis.2008;14:1232---9.
66.FayeO,FayeO,DialloD,DialloM,WeidmannM,SallAA. Quanti-tativereal-timePCRdetectionofZikavirusandevaluationwith field-caughtmosquitoes.VirolJ.2013;10:311.
67.StaplesJE,DziubanEJ, FischerM,CraganJD,Rasmussen SA, Cannon MJ,et al. Interim guidelines for theevaluation and testing of infants with possible congenital Zika virus infec-tion --- United States, 2016. MMWR Morb Mortal Wkly Rep. 2016;65:63---7.
68.BeckerLE.Infectionsofthedevelopingbrain.AJNRAmJ Neu-roradiol.1992;13:537---49.
69.PetersenEE,StaplesJE,Meaney-DelmanD.Interimguidelines for pregnant women during a Zika virus outbreak --- United States,2016.MMWRMorbMortalWklyRep.2016;65:30---3. 70.OliveiraMeloAS,MalingerG,XimenesR,SzejnfeldPO,Alves
SampaioS,BispodeFilippisAM.Zikavirusintrauterine infec-tioncausesfetalbrainabnormalityandmicrocephaly:tipofthe iceberg?UltrasoundObstetGynecol.2016;47:6---7.
71.MlakarJ,KorvaM,TulN,Popovi´cM,Poljˇsak-PrijateljM,Mraz J,etal.Zikavirusassociatedwithmicrocephaly.NEnglJMed. 2016;374:951---8.
72.DolmetschR, GeschwindDH.Thehumanbraininadish:the promiseofiPSC-derivedneurons.Cell.2011;145:831---4. 73.ZhangR,ZhangLH,XieX.iPSCsandsmallmolecules:a
recip-rocalefforttowardsbetterapproachesfordrugdiscovery.Acta PharmacolSin.2013;34:765---76.
74.IchidaJK,KiskinisE.Probingdisordersofthenervoussystem usingreprogrammingapproaches.EMBOJ.2015;34:1456---77. 75.FriesKM, Blieden T, Looney RJ, Sempowski GD, Silvera MR,
Willis RA, et al. Evidence of fibroblast heterogeneity and theroleoffibroblastsubpopulationsinfibrosis.ClinImmunol Immunopathol.1994;72:283---92.
76.TakahashiK,Yamanaka S.Inductionofpluripotent stemcells frommouseembryonicandadultfibroblastculturesbydefined factors.Cell.2006;126:663---76.
77.D’AiutoL,DiMaioR,HeathB,RaimondiG,MilosevicJ,Watson AM,etal.Humaninducedpluripotentstemcell-derivedmodels toinvestigatehumancytomegalovirusinfectioninneuralcells. PLoSONE.2012;7:e49700.
78.Lancaster MA,Renner M, Martin CA,Wenzel D,Bicknell LS, HurlesME,etal.Cerebralorganoidsmodelhumanbrain devel-opmentandmicrocephaly.Nature.2013;501:373---9.
79.BaeBI,WalshCA.Neuroscience:whataremini-brains?Science. 2013;342:200---1.