INTRODUCTION
During the 1980’s and 1990’s an inc re asing majo rity o f patients with AML achieved CR and the pro po rtio n o f patients remaining in permanent remis-sio n also impro ved.1,2
Intensified inductio n therapy may affect the lo ng term survival witho ut an apparent e ffe c t o n the initial re s p o ns e rate .3 CR rate s in previo usly untreated patients with de novo AML using High Do se Ara-C (HDAC) have been repo rted to be 50-80%.4,5
The general trend in the therapeutic strategy has invariab ly b e e n aim e d to ward s m o re aggre s s ive treatment administered as so o n as CR is achieved. The reaso n fo r this has been to pro vide a maximum o f anti-tumo r effect, a so -called co nso lidatio n o r intensifica-tio n treatment.6
Thre e inte nsive co nso lidatio n strate gie s are currently pro po sed fo r yo unger adults with AML in first CR: allo geneic o r auto lo go us bo ne marro w transplantatio n (BMT) o r inte nsive c o nso lid atio n c he m o -the rap y.7,8 Fo r p atie nts who are yo unge r than 45, myelo ablative treatment with allo geneic BMT, fro m an identical HLA sibling do no r, has beco me an accepted tre atm e nt, whe n a d o no r is availab le . Ho we ve r, allo geneic BMT carries sub stantial pro cedural risk related to mo rtality and mo rbidity, resulting in a 5-year o verall survival o f aro und 50%.8 Auto lo go us stem cell transplantatio n o ffers the po ssibility o f perfo rming the same myelo ablative regimen in patients witho ut a co mpatible do no r and witho ut the risks asso ciated with graft-versus-ho st-disease (GVHD).7
Results fro m rando mized studies co mparing
Original Article
REVISTA PAULISTA DE MEDICIN AConve ntional che mothe rapy for acute
mye loid le uke mia: a Brazilian e xpe rie nce
Hematology and Hemotherapy Center, Bone Marrow Transplantation Unit,
Universidade Estadual de Campinas, Campinas, Brazil
a b s t r a c t
CON TEX T: Yo ung patients affected by acute myelo id leukemia (AML) achieve co mplete remissio n (CR) using co nventio nal chemo therapy in abo ut 5 5 -8 5 %. Ho wever, 3 0 % o f patients fail to achieve CR and the remissio n duratio n is o ften o nly abo ut 1 2 mo nths. Mo re intensive treatment after CR seems to be necessary in o rder to maintain CR a nd o b ta in a de finitive c ure . In Bra z il, fe w re po rts ha ve b e e n published o n this impo rtant subject.
OBJECTIVE: The aim o f this study was to describe a Braz ilian expe-rience in the treatment o f “de no vo ” acute myelo id leukemia (AML) in yo ung er adult patients (ag e < 6 0 years).
DESIGN : Retro spective analysis.
SETTIN G: University Ho spital, Hemato lo g y and Hemo therapy Cen-ter, State University o f Campinas, Braz il.
PARTICIPAN TS: N ewly diag no sed cases o f “ de no vo ” AML in the perio d fro m January 1 9 9 4 to December 1 9 9 8 were evaluated ret-ro spectively, in relatio n to respo nse to treatment, o verall survival (O S) and disease free survival (DFS). Cases with acute pro myelo cytic leukemia (APL) were also included in this analysis.
RESULTS: O n the basis o f an intentio n to treat, 7 8 cases o f AML, including 1 7 cases o f APL, were evaluated. The o verall median fo llo w-up was 2 7 2 days. The co mplete remissio n (CR) rate was 6 3 .6 % in the AML g ro up (excluding APL) and 7 8 % in the APL g ro up. The 5 -year estimated disease-free survival (DFS) was 8 0 % fo r the APL g ro up and 3 4 % fo r the AML g ro up (P = 0 .0 2 ). The 5 -year estimated o ver-all survival (O S) was 5 2 % fo r the APL g ro up and 2 0 .5 % fo r the AML g ro up, respec tively (P = N S). Rela pse wa s o b served in 1 2 / 3 9 (3 0 .7 %) patients with AML and 1 / 1 1 (9 %) with APL.
CON CLUSION S: These results are similar to tho se repo rted in the literature. Ho wever, relapse and mo rtality rates remain hig h, and a search fo r mo re ag g ressive strateg ies in o rder to prevent relapse is reco mmended.
KEY W ORDS: Acute myelo id leukemia. Chemo therapy. Bo ne mar-ro w transplantatio n. Survival
chemo therapy alo ne to allo geneic and auto lo go us bo ne marro w transplantatio n have beco me available. 7-11 Better results are seen in APL, a distinct subtype o f
AML, in which a b alanced recipro cal translo catio n between chro mo so mes 15 and 17 results in the unio n o f po rtio ns o f the pro myelo cytic leukemia gene with the gene fo r retino ic acid recepto r alpha. The disease typically presents with a life-threatening hemo rrhagic diathesis, which wo rsens by cyto to xic chemo therapy, with early hemo rrhagic deaths o f abo ut 10-20%. The use o f all-trans-re tino ic ac id (ATRA) fo llo we d b y anthracycline in the inductio n therapy o f APL has impro ved the o utco me, with the CR rate reaching mo re than 90% and reducing the incidence o f relapse.12,13,14 The aim o f this study was to describe a Brazilian experience in the treatment o f adult patients affected by AML, including APL, pro viding a basis fo r mo re intensive appro aches in the future.
METHODS
Patients. Patients under 60 years o f age, with previo usly untreated “de novo” acute myelo id leukemia (AML) diagno sed and treated between 1994 and 1998 at the State University o f Campinas were enro lled in this study. The diagno sis was assessed by bo ne marro w (BM) aspiratio n sho wing at least 30% o f blasts, o r by a b o ne m arro w b io p s y, in the c as e o f as s o c iate d
myelo fibro sis. Each case was classified acco rding to the French-American-British (FAB) System.15,16 Patients with a p re vio u s h is to ry o f m ye lo d ys p las ia, myelo pro liferative disease and previo us chemo therapy o r radio therapy treatment were no t included in this study.
Leukemia diagnosis. Fo r the classificatio n we used the pro cedures reco mmended by Sco tt, et al.23 We used c o nve ntio nal c yto c he m is try te c hniq ue s fo r the classificatio n o f AML: Sudan Black, PAS and unspe-cific esterase, with and witho ut NaF inhibitio n. Cases co nsidered to be Sudan Black negative were studied by flo w cyto metry with the fo llo wing antibo dies: CD45, CD10/CD19, CD3/DR, CD7/CD33, CD14/CD34, CD13 and mye lo pe ro xidase (MPO). Immuno cyto che mistry in slides was perfo rmed with antibo dies to glyco pho rin, CD41 and CD62 when necessary. APL was classified by mo rpho lo gy. Cyto genetic studies were available fo r o nly two APL patients: o ne presented t (15.17) and PCR po sitive fo r the translo catio n PML/RAR
α
. The o ther o ne had variant micro granular mo rpho lo gy and had a no rmal karyo type.Treatment. The inductio n treatment co nsisted o f 1 o r 2 cycles o f TAD-9, as described elsewhere.1
Bo ne marro w aspiratio n was perfo rmed between the 14th and 21st day after the last day o f chemo therapy. Patients who did no t achieve co mplete remissio n (CR) after two cycles o f TAD-9 were treated with a salvage regimen, nam e d MEC.17
Patie nts who ac hie ve d CR we re submitted to two co nsecutive co nso lidatio n cycles,
o ne with HDAC plus dauno rubicin (ARAC 2g/m2 IV
twice a day o n days 1-4 and dauno rubicin 45 mg/m2
o n d ays 5-7), fo llo we d b y o ne c yc le o f TAD-7, as
described elsewhere.1
After these 2 cycles, patients we re sub m itte d to m ainte nanc e tre atm e nt fo r 24
mo nths, with mo nthly cycles o f ARAC 100 mg/m2 SC
twice a day o n days 15, alternating mo nthly cyclo -pho sphamide, dauno rubicin and thio guanine.2
A search fo r an HLA identical do no r was per-fo rmed per-fo r all patients under 50 years o f age, and allo geneic BMT was pro po sed to patients with an HLA-id e ntic al sib ling d o no r availab le (e xc e p t to APL patients).
Patie nts affe cte d b y APL re ce ive d an ATRA-co ntaining regimen as inductio n treatment, acATRA-co rd-ing to initial leuko metry. Patients with WBC = 5x109/L were treated with ATRA. Patients with WBC between 6x109/L and 10x109/L were treated with ATRA and TAD-9 and p atie nts with WBC > 10x109
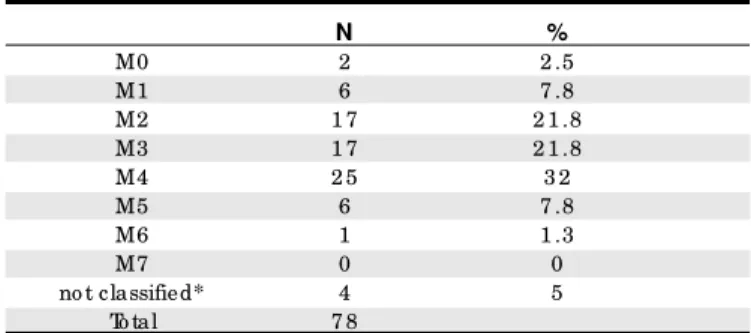
/L at d iagno sis received o nly co nventio nal chemo therapy as induc-tio n treatment (TAD-9). One patient was treated with ATRA and d auno rub ic in as ind uc tio n. ATRA was Table 1. Fre nch-Ame rican-British classification of 78
patie nts affe cte d by acute mye loid le uke mia
N %
M0 2 2 .5
M1 6 7 .8
M2 1 7 2 1 .8 M3 1 7 2 1 .8 M4 2 5 3 2
M5 6 7 .8
M6 1 1 .3
M7 0 0
no t classified* 4 5 To tal 7 8
* 3 bipheno typic AML, o ne case o f g ranulo cytic sarco ma.
Table 2. Clinical and laboratory characte ristics of patie nts with AML
AM L group (n=61) APL group(n=17)
median ag e 3 2 (1 4 to 5 9 ) 3 3 (1 6 to 5 4 ) S e x (M/ F) 3 1 / 3 0 7 / 1 0
Hb (g / dl) 8 .3 (4 .5 to 1 5 ) 8 .0 (5 to 1 2 ) W BC x1 09 / L 2 0 (0 .4 to 2 1 4 ) 3 .3 (0 .7 to 4 9 )
% blasts peripheral blo o d 6 0 .5 (0 to 9 8 ) 1 5 (3 to 9 1 ) % blasts bo ne marro w 7 6 (3 0 to 9 9 ) 7 5 .5 (3 8 to 9 9 ) Platelets x1 09 / L 4 2 (2 to 2 4 7 ) 1 8 (2 to 1 4 6 )
interrupted and chemo therapy added if patients pre-sented ATRA syndro me and/o r leuko cyto sis. The po st remissio n therapy fo r APL patients was the same used fo r the o ther AML subtypes. No allo geneic BMT was perfo rmed in APL patients during the first CR.
Response criteria. CR was defined as mo re than 1.0x109/L granulo cytes and mo re than 100x109/L plate-le ts in p e rip he ral b lo o d , and no rm o c e llular BM co ntaining less than 5% o f blasts cells. Patients who did no t fulfill the abo ve criteria were co nsidered no n-respo nders.
Statistical methods. Analysis was based o n status o f the patients o n April 20th 1999, based o n the last fo llo w-up. Overall survival (OS) was defined fro m the date o f diagno sis and beginning o f chemo therapy until death o r last fo llo w-up. Disease free survival (DFS) was calculated fro m the date o f first co mplete remissio n until the date o f death, first relapse o r last fo llo w-up in co ntinuo us CR. Survival curves were calculated by the Kaplan-Meier metho d and differences between the curves were analyzed with the lo g-rank test.18 The pa-tients were divided into the AML gro up (n=61) and APL gro up (n= 17). The co mpariso n b e twe e n WBC number o n diagno sis was based o n descriptive analy-sis using the Mann-Whitney test.
RESULTS
Between January 1994 and December 1998, 87 patients with age belo w 60 years o ld were diagno sed as AML in o ur ho spital. Ho wever, nine patients were no t evaluated because o f early death befo re starting chemo therapy. Amo ng the 78 evaluated patients, 61 (78.2%) patients were classified as AML gro up (no n-APL) and 17 (21.8%) were classified as APL. In the AML gro up, 31 patients were males and 30 females and the median age was 32 years (14-59). In the APL gro up, 7 patients were males and 10 females, with a median age o f 33 years (16-54). The median number o f white blo o d cells (WBC) at diagno sis was 20 x 109/L (0.4-214) fo r the AML gro up and 3.3 x 109/L (0.7-49) fo r the APL gro up (P = 0.004) (Tab le 1). The clinical and labo rato ry characteristics are sho wn in Table 1. The mo st co mmo n FAB subtypes were M4, M2 and M3 (32%, 21.8% and 21.8%, respectively) (Table 2). During the analysis perio d, no cases o f M7 subtypes were diagno sed. The o verall median fo llo w-up was 254 days (1-1842) and 540 days (4-1580) fo r the AML and APL gro ups, respectively.
Response. At the end o f o ur o bservatio n, 33/78 patients (42.3%) were alive; 32 (41%) in CR and 1 (1.2%) with refracto ry disease after relapse; 45/78 (57.6%)
patients died. AML group: 30 o ut o f 61 (49%) patients reached CR with o ne cycle o f TAD-9. Thirteen o ut o f 61 did no t achieved CR using o ne cycle o f TAD-9, and 5 o f them (8.1%) achieved CR after the seco nd cycle o f TAD-9. Three patients (4.9%) achieved CR after salvage che m o the rapy with MEC (2 patie nts) o r HDAC (1 patient). One patient (1.6%) received as an inductio n treatment lo w do se Ara-C due to po o r perfo rmance status at diagno sis and achieved CR. A to tal o f 39 p atie nts ac hie ve d CR (63.6%). Two p atie nts we re submitted to allo geneic bo ne marro w transplantatio n, while in first CR and remained in CR. Fo ur patients died during co nso lidatio n therapy while in CR. Twelve o ut o f 35 (34.2%) patients relapsed, after a median time o f 287.5 days (50-1265) fro m first CR (AML gro up). APL patients: Seven patients with WBC
≤
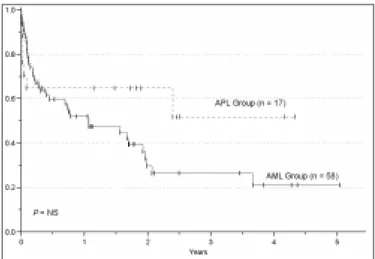
5X109/L were treated initially with ATRA. TAD-9 was asso ciated in 7 cases with a rise in WBC and/o r ATRA syndro me. Eleven o ut o f 14 (78%) patients who used an ATRA-co ntaining regimen ac hie ve d CR. Thre e p atie nts we re tre ate d with co nventio nal chemo therapy alo ne and died during inductio n. One o ut o f 11 (9%) relapsed, after 22 mo nthsFigure 1. Overall survival in patients affected by AML.
in CR, during maintenance treatment.
Survival. The median survival fo r alive patients was 409 days (67-1842) fo r the AML (no n-APL) gro up (n= 22) and 677 days (118-1580) fo r the APL gro up (n=10). The estimated OS fo r all patients (AML and APL gro ups) was 27% o ver 5 years. The 5-year esti-mated OS was 20.5% and 52% fo r AML and APL gro ups, respectively (P = NS). Ho wever, the 5-year estimated DFS was s ig nific antly hig he r in the APL ( 80%) co mpared to the AML gro up (34%) (P = 0.01). The o verall survival and disease free survival curves fo r the two gro ups o f patients are sho wn in Figures 1 and 2, respectively.
Causes of death. AML group: 21 o ut o f 61 (34.5%) patients died during inductio n treatment. 13 o ut o f 21 (61.9%) died due to infectio n, 2 o ut o f 21 (9.5%) due to CNS bleeding, 1 o ut o f 21 (4.8%) due to leuko stasis, 1 o ut o f 21 due to acute GVHD, and 4 o ut o f 21 (19%) due to unkno wn causes. After co nso lidatio n therapy, 4 o ut o f 39 patients (10.2%) died during the aplastic phase, due to infectio n; 3 o f them after the first cycle o f co nso lidatio n (HDAC) and o ne after the seco nd cycle o f co nso lidatio n (TAD-7). Eleven o ut o f 35 patients (31.4%) died after relapse. One o ut o f 11 (9%) patients died o f bleeding befo re receiving reinductio n treat-ment. Nine o ut o f 11 (82%) died due to infectio n, after reinductio n chemo therapy. One o ut o f 11 (9%) was submitted to allo geneic BMT and died due to pro gres-sive disease and central nervo us system b leeding. No ne o f the relapsed patients achieved CR using sal-vage therapy. No patients died during maintenance treatment, while in CR. APL group: There were 7 deaths in this gro up. Three o ut o f 7 (44%) patients died during TAD- 9 in d u c tio n , two d u e to d is s e m in ate d intravascular co agulatio n (DIC) and o ne due to infec-tio n. Am o ng the p atie nts tre ate d with an ATRA-co ntaining regimen, 2 o ut o f 7 (28%) patients died due to ATRA syndro me and o ne o ut o f 7 (14%) due to infe ctio n. One o f the 7 (14%) patie nts had a late relapse, 22 mo nths after starting CR and died during the aplastic phase po st-reinductio n therapy, due to infectio n.
DISCUSSION
In this re tro spe ctive study, we analyze d the results o f co nventio nal treatment fo r patients with AML, age < 60 ye ars, tre ate d at the Unive rsity o f Campinas. There are few Brazilian studies published co ncerning results o f treatment in AML.19 Fo r this age gro up, there are many repo rts referring to CR rates between 55% to 85%, with pro lo nged DFS, and cures
in abo ut 25%-30%.4
We used TAD-9 as inductio n therapy. The CR rate after the 1st cycle was 49%. The seco nd cycle o f TAD-9 bro ught little impro vement to the o verall CR (8.1%). In additio n, 4.9% o f patients achieved CR with salvage regimens. The o verall CR rate was 63.6%, similar to tho se re po rte d in the lite rature .2,4,5 With standard inductio n regimens (3 days o f anthracycline and 7 days o f cytarabine), appro ximately 30% o f patients still fail to achieve CR and the remissio n duratio n is o ften aro und 12 mo nths.
HDAC has been successfully used in a number o f co mbinatio ns in relapsed patients and as po st-remis-sio n o r co nso lidatio n therapy.9,10,11
We used o ne cycle o f HDAC fo r co nso lidatio n and did no t o bserve high to xic ity and m o rtality. Thus , this re g im e n was demo nstrated to be feasible in o ur patients. Altho ugh many different schedules have been used, including co nso lidatio n with o r witho ut pro lo nged maintenance, abo ut 25-30% o f patients will remain in CR fo r 5 years. Ho wever, the maintenance o f remissio n is still a chal-lenge. We o bserved relapse in 34.7% o f the AML gro up, half o f them o ccurring during the first year po st-remis-sio n. Our maintenance pro gram was no t able to sustain CR in a large number o f patients. The 5-year estimated o verall survival fo r the AML gro up was 20.5%, similar to that repo rted in the literature.2,4,5
Recently, new appro aches have been pro po sed to intensify AML treatment, with the purpo se o f de-creasing relapse incidence, leading to a better OS and DFS. The first large rand o m ize d stud y c o m p aring allo ge ne ic BMT, auto lo go us BMT and inte ns ive co nso lidatio n with HDARAC was pub lished b y the
EORTC and GIMEMA gro ups.20
1. Buchner T, Urbanitz D, Hiddemann W, et al. Intensified inductio n and co nso lidatio n with o r witho ut maintenance chemo therapy fo r acute myelo id leukemia (AML): two multicenter studies o f the German AML Co o perative Gro up. J Clin Onco l 1985;3(12):583-9.
2. Buchner T, Heddemann W, Wo rman B, et al. Do uble inductio n strategy fo r acute myelo id leukemia: the effect o f High-Do se cytarabine with mito xantro ne instead o f standard-do se cytarabine with dauno rubicin and 6-thio guanine: a rando mized trial by the German AML Co o perative Gro up. Blo o d 1999;93(12):4116-24.
3. Ro we JM, Tallman MS. Intensifying inductio n therapy in acute myelo id le u ke m ia : h a s a n e w s ta n d a rd o f c a re e m e rg e d ? Blo o d 1997;90(6):2121-6.
4. We i c k J, Ko p e c ky KJ, Ap p e l b a u m FR, e t a l . A ra n d o m i ze d i n ve s ti g a ti o n o f h i g h - d o s e ve rs u s s ta n d a rd - d o s e c yto s i n e arab ino side with dauno rub icin in patients with previo usly untreated acute myelo id leukemia: a So uthwest Onco lo gy Gro up Study. Blo o d 1996;88(8):2841-51.
5. Bisho p JF, Matthews J, Yo ung GA, et al. A rando mized study o f high-d o se c ytarab ine in inhigh-d uc tio n in ac ute m ye lo ihigh-d le uke m ia. Blo o high-d 1996;87(5):1710-7.
REFERENCES
6. Go rin NC. Auto lo go us stem cell transplantatio n in acute myelo cytic leukemia. Blo o d 1998;92(4):1073-90.
7. Haro usseau, JL, Cahn JY, Pigno n B, et al. Co mpariso n o f auto lo go us bo ne marro w transplantatio n and intensive chemo therapy as po st-remissio n therapy in adult acute myelo id leukemia (GOELAM). Blo o d 1997;90(8):2978-86.
8. Burnett AK, Go ldsto ne AH, Stevens RMF, et al. Fo r the UK Medical Research Co uncil Adult and Children’s Leukemia Wo rking Parties. Rando mized co mpariso n o f additio n o f auto lo go us b o ne-marro w trans p lantatio n to inte ns ive c he m o the rap y fo r ac ute m ye lo id le uke mia in first re missio n: re sults o f MRC AML 10 trial. Lance t 1998;351:700-8.
9. Champlin R, Ho W, Winsto n D, et al. Treatment o f adults with acute myelo id leukemia: pro spective evaluatio n o f high do se cytarabine in co nso lidatio n chemo therapy and with bo ne marro w transplantatio n. Semin Onco l 1987;14:1.
10. Mayer RJ, Schiffer CA, Peterso n BA, et al. Intensive po st-remissio n therapy in adults with acute no n-lympho cytic leukemia using vario us do se schedules o f Ara-C: a pro gress repo rt fro m CALGB. Semin Onco l 1987;14(2):25-31.
the standard risk gro up (neither go o d no r po o r) and the po o r risk gro up were tho se with adverse karyo type o r > 15% o f blasts after the first co urse o f inductio n. Ho wever, except fo r APL, there is still no co nsensus in the lite rature fo r d iffe re ntiating AML tre atm e nt acco rding to cyto genetic characteristics. In o ur study, it was no t po ssible to evaluate cyto genetics in mo st o f the cases, so we co uld no t stratify the patients into risk catego ries acco rding to this criterio n.
The treatment o f the APL gro up using chemo -therapy alo ne was sho wn to be inadequate, and high rates o f mo rtality due to DIC were o bserved. The use o f all- tran s - re tin o ic ac id ( ATRA) fo llo we d b y anthracycline, in the inductio n therapy o f APL, has impro ved the CR rate to greater than 90% and reduced the incidence o f relapse.12,13,14 The additio n o f ATRA to chemo therapy during inductio n o f APL has bro ught a great impro vement in terms o f CR and DFS, also in o ur patients. DFS was lo nger in APL (80%) than in the AML (no n-APL) gro up (34%) (P = 0.02). The difference in te rm s o f O S b e twe e n the 2 g ro up s was no t significant, pro bably due to the small number o f APL patients enro lled. Once CR was achieved, relapse was a rare event in this gro up. We did no t o bserve the high
inductio n mo rtality rates described by Pulcheri, et al.19 Except fo r APL, allo geneic bo ne marro w trans-plantatio n fro m an HLA sibling do no r is the treatment o f cho ice, despite the transplant-related mo rbidity and mo rtality. In o ur study, patients transplanted in the first CR had better results than tho se with refracto ry d ise ase . Ho we ve r, fe w p atie nts have an availab le d o no r. Mo re inte nsive c he m o the rap y fo llo we d b y auto lo go us BMT, o r mo re intensive co nso lidatio n, sho uld pro bably reduce the relapse risk and pro lo ng o verall survival.
We m ay the re fo re co nclude that the o ve rall results achieved at o ur Institutio n represent what is expected in the literature fo r co nventio nal chemo -therapy in AML and APL.
r e s u m o
CON TEXTO: Pacientes adulto s co m diag nó stico de leucemia mieló ide ag uda (LMA) o btém remissão co mpleta (RC) co m quimio terapia co nvencio nal em cerca de 5 5 -8 5 % do s caso s, e a sua duração é de apro ximadamente 1 2 meses. Cerca de 3 0 % do s pacientes não ating em a RC. Para manter a RC e o bter cura definitiva parece ser necessário intensificar o tratamento apó s a RC. N o Brasil, há um pequeno número de artig o s publicado s a esse respeito .
OBJETIVO: Descrever a experiência brasileira no tratamento de leu-cemia mieló ide ag uda “ de no vo ” em jo vens e adulto s co m idade inferio r a 6 0 ano s.
TIPO DE ESTUDO: Análise retro spectiva.
LOCAL: Ho spital das Clínicas e Hemo centro da Universidade Estadual de Campinas.
PARTICIPAN TES: Fo ram estudado s, retro spectivamente, caso s no vo s de LMA entre 1 9 9 4 e 1 9 9 8 , co m relação à respo sta ao tratamento de quimio terapia, so brevida g lo bal e so brevivência livre de do ença.
RESULTADOS: Entraram no estudo 7 8 pacientes de LMA, incluindo 1 7 caso s de leucemia pro mielo cítica (LPM). A média de seg uimento fo i de 2 7 2 dias. A taxa de RC fo i de 6 3 ,6 % no s pacientes co m LMA excluindo -se o s pacientes co m LPM, e 7 8 % no s pacientes co m LPM. A so brevida livre de do ença em 5 ano s fo i de 8 0 % no s pacientes co m LPM e 3 4 % para o s pacientes co m LMA (P=0 ,0 1 ). A so brevida g lo bal fo i de 5 2 % e 2 0 ,5 % para o s pacientes co m LPM e LMA respectivamente (P=N S). Recidiva fo i o bservada em 1 2 / 3 9 (3 0 ,7 %) do s pacientes co m LMA e 1 / 1 1 (9 %) na LPM.
CON CLUSÕES: Esses resultado s são semelhantes ao s enco ntrado s na literatura, entretanto , o número de recidivas e a mo rtalidade ma ntém-se a lta , rec o menda ndo -se pesq uisa de estra tég ia s ma is ag ressivas para prevenir recidivas.
PALAVRAS-CHAVE: Le uc e mia mie ló ide a g uda . Q uimio te ra pia . Transplante de medula ó ssea. So brevida.
Kátia Borgia Barbosa Pagnano, MD. Hemato lo gy and Hemo therapy Center,
Universidade Estadual de Campinas, Campinas, São Paulo , Brazil.
Fabiola Traina, MD. Hemato lo gy and Hemo therapy, Universidade Estadual
de Campinas, Campinas, São Paulo , Brazil.
Tatiana Takahashi, MD. Hemato lo gy and Hemo therapy Center, Universidade
Estadual de Campinas, Campinas, São Paulo , Brazil.
Gislaine Borba Olive ira, MD. Hemato lo gy and Hemo therapy Center,
Universidade Estadual de Campinas, Campinas, São Paulo , Brazil.
Marta Soare s Rossini, MD. Hemato lo gy and Hemo therapy Center,
Universidade Estadual de Campinas, Campinas, São Paulo , Brazil.
Ire ne Lorand-Me tze , PhD. Hemato lo gy and Hemo therapy Center,
Universidade Estadual de Campinas, Campinas, São Paulo , Brazil.
Afonso Ce lso Vigorito, PhD. Directo r o f the Bo ne Marro w Transplantatio n
Unit, Hemato lo gy and Hemo therapy Center, Universidade Estadual de Campinas, Campinas, São Paulo , Brazil.
Eliana Cristina Martins Miranda. Bio statistician, Bo ne Marro w
Transplanta-tio n Unit, Hemato lo gy and Hemo therapy Center, Universidade Estadual de Campinas, Campinas, São Paulo , Brazil.
Cármino Antonio De Souza, PhD. Directo r o f the Hemato lo gy and
Hemo therapy Divisio n, Hemato lo gy and Hemo therapy Center, Universidade Estadual de Campinas, Campinas, São Paulo , Brazil.
Source s of funding: No t declared
Conflict inte re st: No t declared
Last re ce ive d: 14 March 2000
Acce pte d: 02 May 2000
Addre ss for corre sponde nce :
Cármino Anto nio De So uza Universidade Estadual de Campinas Centro de Hemato lo gia e Hemo terapia, TMO Cidade Universitária “Zeferino Vaz” PO Bo x - 6198
Campinas/SP - Brasil - CEP 13081-970 E-mail: carmino @ o belix.unicamp.br
publishing in fo r m a t io n
11. Brito -Babapulle F, Cato vsky D, Newland AC, Go ldman JM, Galto n DAG Tre atm e nt o f ac ute m ye lo id le uke m ia with inte rm e d iate - d o s e cytarabine and mito xantro ne. Semin Onco l 1987;14(2):51-2. 12. Barbui T, Finazzi G, Falanga A. The impact o f all-trans-retino ic acid o n
th e c o ag u lo p ath y o f ac u te p ro m ye lo c ytic le u ke m ia. Blo o d 1998;91(9):3093-102.
13. Tallman MS, Andersen JW, Schiffer CA, et al. All-trans-retino ic acid in acute pro myelo cytic leukemia. New Engl J Med1997;337(15):1021-8.
14. De Bo tto n S, Do mb re t H, Sanz M, e t al. Incide nce , clinical fe ature s and o utco m e o f all-trans-re tino ic acid syndro m e in 413 case s o f n e wl y d i a g n o s e d a c u te p ro m ye l o c yti c l e u ke m i a . Bl o o d 1998;92(8):2712-8.
15. Benett JM, Cato vsky D, Daniel MT, et al. Pro po sals fo r the classificatio n o f the acute leukemias. Br J Haemato l1976;33(4):451-8.
16. Benett JM, Cato vsky D, Daniel MT, et al. Pro po sed revised criteria fo r the c las s ific atio n o f ac ute m ye lo id le uke m ia. Ann Inte rn Me d 1985;103(4):620-5.
17. Amado ri S, Arcese W, Isacchi G, et al. Mito xantro ne, eto po side and intermediate-do se cytarabine: an effective and to lerable regimen fo r the treatment o f refracto ry acute myelo id leukemia. J Clin Onco l
1991;9(7):1210-4.
18. Kaplan EL, Me ir P. No n-param e tric e stim atio n fro m inco m ple te o bservatio n. J Am Stat Asso c 1958;53:457.
19. Pulcheri W., Specto r N., Nucci M, de Mo rais JC, Pimenta G, de Oliveira HP. The treatment o f acute myelo id leukemia in Brazil: pro gress and o bstacles. Haemato lo gica 1995;80(2):130-5.
20. Zitto un RA, Mandelli F, Willemze R, et al. Auto lo go us o r allo geneic bo ne marro w transplantatio n co mpared with intensive chemo therapy in acute myelo geno us leukemia. New Engl J Med 1995;322:217 21. Whe atle y K, Burne tt AK, Go ldsto ne AH, e t al. A sim ple , ro b ust,
validated and highly predictive index fo r the determinatio n o f risk-directed therapy in acute myelo id leukemia derived fro m the MRC AML 10 trial. Br J Haemato l 1999;107:69-79.
22. To rresan M, Barbo sa KB, So uza CA, Lo rand-Metze I. Co mparação entre q uim io te rap ia e ATRA no tratam e nto d e ind uç ão d a le uc e m ia pro mielo cítica. Bo letim da So ciedade Brasileira de Hemato lo gia e Hemo terapia 1998;XX:111.