INTRODUCTION
Hyperpho sphatemia has an impo rtant ro le in
the develo pment o f seco ndary hyperparathyro idism
and b o ne disease in patients with end-stage renal
disease (ESRD).
1-8Co ntro l o f hyperpho sphatemia can
be achieved with the use o f aluminum co mpo unds that
act as efficient pho spho rus binders and reduce the
in-testinal abso rptio n o f pho spho rus. Ho wever, especially
due to neuro lo gic and bo ne to xicity, aluminum co
m-po unds have been replaced by calcium salts.
9-12The
mo st co mmo nly used (calcium carbo nate, CaCO
3) is
no t the ideal binding agent, primarily because o f its
hypercalcemic effect.
13-15In this regard, calcium acetate
[(CH
3COO)
2Ca.H
2O] has been repo rted by so me
au-tho rs to have at least a similar pho spho rus binding
e ffic ie nc y, and a le ss p ro no unc e d hyp e rc alc e m ic
e ffe c t
16- 19b u t th is s u b j e c t is s till a m atte r o f
co ntro versy.
20-24This study was designed to co mpare
the efficiency, to lerance and side effects o f these salts.
METHODS
Fifty-two stab le ESRD p atie nts und e rgo ing
regular hemo dialysis in a ho spital dialysis center fo r
47 mo nths (SD 26) entered the study. They were
main-taine d o n the ir usual d ie t. Parathyro id e c to m ize d
patients were no t included. Dialysis was perfo rmed
three times a week utilizing a cupro phane memb rane
with a surface area o f b etween 1.0 and 1.5 m
2.
Dialy-sis sessio ns were acco mplished using no n-pro po
r-tio nal mixture machine s witho ut an ultrafiltrar-tio n
co ntro l device (Baxter Inc., McGraw Park, IL 60085,
Original Article
REVISTA PAULISTA DE MEDICIN ACalcium ace tate ve rsus calcium carbonate
in the control of hype rphosphate mia
in he modialysis patie nts
Universidade Federal Fluminense, Niterói, and
Francisco Santino Filho Kidney Foundation, Rio de Janeiro, Brazil
a b s t r a c t
CON TEX T
: Hyperpho sphatemia has an impo rtant ro le in the devel-o pment devel-o f bdevel-o ne and mineral abndevel-o rmalities in end-stag e renal dis-ease (ESRD).OBJECTIVE:
To co mpare the pho spho rus binding po wer and the hypercalcemic effect o f calcium acetate and calcium carbo nate in hemo dialysis patients.TYPE OF STUDY:
Cro sso ver, rando miz ed, do uble-blind study.PLACE:
A private ho spital dialysis center.PARTICIPAN TS:
Fifty-two pa tients who were underg o ing reg ula r hemo dialysis three times a week ([Ca++] dialysate = 3 .5 mEq/ L).PROCEDURES:
Half o f the patients were started o n 5 .6 g / day o f calcium acetate and, after a 2 week washo ut perio d, received 6 .2 g / day o f calcium carbo nate. The o ther half fo llo wed an inverse pro to co l.M AIN M EASUREM EN TS:
Clinical interviews were co nducted 3 times a week to mo nito r fo r side effects. Determinatio ns o f serum urea, calcium, pho spho rus, hemato crit, Kt/ V and blo o d g as analysis were o btained befo re and after each treatment.RESULTS:
Twenty-three patients co mpleted the study. A sig nificant increase in calcium plasma levels was o nly o bserved after treatment with calcium carbo nate [9 .3 4 mg / dl (SD 0 .9 1 ) vs. 9 .9 1 mg / dl (SD 0 .7 9 ), P < 0 .0 1 ]. The dro p in pho spho rus levels was substantial and sig nificant fo r bo th salts [5 .6 4 mg / dl (SD 1 .5 4 ) vs. 4 .6 0 mg / dl (SD 1 .3 2 ), P < 0 .0 1 and 5 .8 9 mg / dl (SD 1 .7 1 ) vs. 4 .5 6 mg / dl (SD 1 .5 7 ), P < 0 .0 1 , fo r calcium acetate and calcium carbo nate respec-tively]. The percentag e reductio n in serum pho spho rus (at the end o f the study) per milliequivalent o f salt administered per day tended to be hig her with calcium acetate but statistical sig nificance was no t fo und.CON CLUSION :
Calcium acetate can be a g o o d alternative to cal-c ium cal-c a rb o na te in the ha ndling o f hyperpho spha temia in ESRD patients. W hen calcium acetate is used, co ntro l o f hyperpho sphatemia can be achieved with a lo wer administratio n o f calcium, perhaps with a lo wer risk o f hypercalcemia.KEY W ORDS:
Calcium Acetate. Calcium Carbo nate. Hyperpho s-phatemia. Hypercalcemia. Hemo dialysis.USA), b lo o d flo w o f 300 m l/m in, and b icarb o nate
b uffered dialysate ([Ca] = 3.5 mEq /L) at 500 ml/min.
A de-io nizer was used to pro vide water treatment.
Dialyzers were manually repro cessed with fo
rmalde-hyde as the sterilizing agent and were discarded if
the internal vo lume o f the ho llo w fib ers decreased
Table 1. Ge ne ral fe ature s of the patie nts
All
Accepted for
(n=5 2 )
a na lysis (n=2 3 )
Ag e, years. 4 6 (SD 1 4 )a 5 0 (SD 1 4 )
Sex (M/ F) 2 6 / 2 6 1 3 / 1 0 Ra c e
(W / B) 2 3 / 2 9 1 2 / 1 1 Time
o n dialysis, mo nths. 4 7 (SD 2 6 ) 5 0 (SD 2 5 ) P intake, mg / day.b 7 5 7 (SD 2 4 8 ) 7 9 5 (SD 2 6 3 )
Ca intake, mg / day.b 3 2 9 (SD 2 0 9 ) 3 8 5 (SD 2 4 5 )
Primary Renal Disease
Chro nic g lo merulo nephritis 1 6 6
Malig nant nephro sclero sis 1 9 8
Po lycystic disease 3 2
Diabetic nephro pathy 3 1
O ther 1 1 6
a Mean and standard deviatio n; b As o btained by nutritio nal inquiry.
Table 2. Total numbe r of patie nts
starting and finishing e ach tre atme nt
N umber o f patients
Acetate Carbo nate
Starting 5 0 5 1
Finishing 3 1 3 3
Excluded 1 9 1 8
Table 3. Re asons for e xclusion
Aceta te
Ca rbona te
Vo luntary dro po ut due to side effects 0 3
-Irreg ular use due to side effects 0 4 0 3
Inadequate adherence no t declared 0 8 1 2
Absent fo r the blo o d co llectio n 0 3
-Clinical pro blems unrelated to drug use 0 1 0 3
Tota l
1 9
1 8
Table 4. Complaints along drug tre atme nt
Symptoms
Aceta te
Ca rbona te
Pruritus 0 2 0 3
Ano rexia 0 4 0 2
N ausea 0 3
-Co nstipatio n 0 4 0 4
Vo miting 0 2
-Epig astralg ia 0 5 0 4
Diarrhea 0 1 0 1
Malaise 0 5
-Xero sto mia 0 1 0 5
Plenitude 0 5 0 3
Dro po ut o r irreg ular use due to side effects 0 7 0 3
Tota l
3 8
2 5
mo re than 20%. Other cleaning agents were no t used.
The daily intake o f calcium and pho spho rus was
quantified thro ugh nutritio nal inquiry. The majo rity o f
th e p atie n ts u s e d c alc iu m c arb o n ate an d / o r
1,25[OH]
2D
3in variable do ses, which were withdrawn
fo r a perio d o f two weeks befo re the beginning o f the
study. All o ther types o f medicatio ns, such as
antihypertensive agents, vitamins, fo lic acid and erythro
-po ietin were maintained.
The study was co nducted in a cro sso ver,
ran-do mized, ran-do ub le b lind manner. Half o f the patients
were initiated o n 5.6 g/day o f calcium acetate (0.069
eq uivalents o f the salt, co rrespo nding to 1.4 g/day o f
e le m e ntal calcium ) (Maia de Alm e ida Indústria e
Co mércio , RJ, Brazil) fo r 4 weeks fo llo wed b y a
wash-o ut periwash-o d wash-o f twwash-o weeks. After this periwash-o d they
re-ceived 6.2 g/day o f calcium carb o nate (0.124 eq
uiva-lents o f the salt, co rrespo nding to 2.5 g/day o f
el-e m el-e ntal c alc ium ) ( Maia d el-e Alm el-e id a Ind ús tria el-e
Co mércio , RJ, Brazil) fo r ano ther fo ur weeks. The
re-m aining patie nts fo llo we d a sire-m ilar pro to co l, b ut
were initially given calcium carb o nate and then
cal-cium acetate. They were all instructed to take the
medicatio n during meals in such a way that the who le
daily do se wo uld b e divided into three o r fo ur do ses
acco rding to the dietary hab it o f the patient. Bo th
preparatio ns were tested “in vitro ” fo r
de-aggrega-tio n fo llo wing the American Pharmaco po eia
guide-lines.
Clinical interviews were co nducted three times
a week to mo nito r fo r adverse effects. Serum urea,
cal-cium, pho spho rus, blo o d gas analysis, hemato crit and
Kt/V determinatio ns were perfo rmed befo re and after
each treatment. Kt/V was calculated in a mid-week
ses-sio n fro m the fo rmula
-logN R
,
in which R is the ratio
o f po st and pre-dialysis serum urea. Abdo minal X-rays
were taken o f each patient to search fo r intact
cap-sules o n the fifth and tenth day o f the treatment with
each co mpo und.
RESULTS
Fifty-two subjects entered the study and
twenty-three were included in the data analysis. The general
features o f the patients are described in Table 1. Of
the fifty-two subjects, twenty patients were using
beta-blo ckers, three were being treated with human reco
m-binant erythro po ietin, two had had a bilateral
nephre-cto my and two had had past kidney transplants. Data
regarding exclusio n are depicted in Tables 2 and 3,
and the side effects fo und fo r each drug are listed in
Table 4.
Table 5 and Figure 1 summarize the labo rato ry
findings fro m pre and po st-treatment with calcium
ac-etate and calcium carbo nate. No ne o f the preparatio ns
significantly altered the values o f blo o d pH and
bicar-bo nate.
A significant increase in calcium plasma levels
was o nly o b served after treatment with calcium [9.34
mg/dl (SD 0.91) vs. 9.91 mg/dl (SD 0.79), P < 0.01].
The po st-treatment plasma calcium levels b etween
th e two c o m p o u n d s , h o we ve r, d id n o t d iffe r
statistically. The dro p in pho spho rus levels was sub
-stantial and significant fo r b o th salts [5.64 mg/dl (SD
1.54) vs. 4.60 mg/dl (SD 1.32), P < 0.01 and 5.89 mg/
dl (SD 1.71) vs. 4.56 mg/dl (SD 1.57), P < 0.01, fo r
ace tate and carb o nate , re spe ctive ly). Again, po
st-treatment P levels b etween the two salts were no t
different.
The re we re no s ignific ant c hange s in Kt/V
thro ugho ut the study. The percent variatio ns in
se-rum levels o f calcium and pho spho rus after treatment
with each drug are sho wn in Figure 1. Analysis o f the
to p and bo tto m panels suggests that mo re pho spho
-rus was bo und by each equivalent o f calcium acetate
in co mpariso n to calcium carbo nate but statistical
sig-nificance was no t fo und.
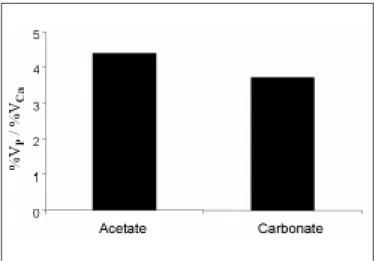
Co mpariso ns o f the hyperpho sphatemic and
hy-percalcemic pro perties o f the two salts are depicted in
Figure 2. Calc ium ac e tate was 4.4 tim e s m o re
hyperpho sphatemic than hypercalcemic; the co rrespo
nd-ing calcium carbo nate value o f this variable was 3.7 but,
again, the differences were no t statistically significant.
Table 5. Laboratory findings be fore and afte r tre atme nt
Aceta te
Ca rbona te
La bora tory findings
Before
After
Before
After
pH 7 .3 1 (0 .0 5 )a 7 .3 3 (0 .0 4 ) 7 .3 0 (0 .0 6 ) 7 .3 2 (0 .0 5 )
HCO
3
- (mEq/ L) 1 7 .3 (2 .3 ) 1 8 .6 (2 .0 ) 1 8 .6 (2 .2 ) 1 8 .9 (2 .2 )
Ca (mg / dl) 9 .3 4 (0 .7 0 ) 9 .7 3 (0 .6 2 ) 9 .3 4 (0 .9 1 ) 9 .9 1 (0 .7 9 )*
P (mg / dl) 5 .6 4 (1 .5 4 ) 4 .6 0 (1 .3 2 )* 5 .8 9 (1 .7 1 ) 4 .5 6 (1 .5 7 )*
Kt/ V 1 .0 3 (0 .2 4 ) 1 .1 5 (0 .1 7 ) 1 .0 4 (0 .2 3 ) 1 .1 5 (0 .1 9 )
a Mean and standard deviatio n, * P < 0 .0 2 vs. pretreatment values.
Figure 2.
Ratios of mean percent variations (%V) in plasma levels of P
and Ca at the end of the treatment period for the 2 salts.
Figure 1.
Mean values of the serum level variation in calcium and
DISCUSSION
Hyperpho sphatemia has been implicated in
dif-ferent manners in the genesis o f parathyro id
hyper-functio n, a co nditio n that has been asso ciated with
high turno ver bo ne disease. It can also co ntribute to
the mineral alteratio ns in ESRD by inducing bo ne
re-sistance to parathyro id ho rmo ne
25,26and precipitatio n
o f metastatic vascular and no n-vascular
27-30calcifica-tio ns. To reinfo rce all these reaso ns in favo r o f there
being an adequate co ntro l o f serum pho sphate levels
in ure m ia, high c alc ium -p ho sp ho rus p ro d uc t has
recently been asso ciated to lo wer survival o n
dialy-sis.
31In the present study, calcium carbo nate and
calcium acetate were co mpared regarding their pho spho
-rus binding pro perties, hypercalcemic effects, and to
l-erance. The pro to co l was designed in such a way that
co mparable do ses (in grams) o f each salt were given
during each phase o f the study. This strategy allo wed
intake o f the same number o f identical capsules in
bo th phases, affirming the do uble-blind nature o f the
study. In this co ntext, the daily amo unt o f calcium
prescribed was always lo wer with calcium acetate.
The study dro po ut ratio fo r e ach co m po und
was high, b ut no t d iffe re nt statistic ally (38% fo r
c alc ium ac e tate and 35% fo r c alc ium c arb o nate ).
To le rance and side e ffe cts we re also co m parab le ,
altho ugh uppe r gastro inte stinal sym pto m s te nde d
to b e mo re freq uent with calcium acetate. A detailed
e xam inatio n o f the diffe re nt re aso ns fo r e xclusio n
d id no t sho w statistic ally signific ant d iffe re nc e s.
The re fo re , the acce ptance o f the co m po unds was
s im ilar. Ne ithe r ac e tate no r c arb o nate ind uc e d
significant change s in b lo o d pH and b icarb o nate .
Re le vant alte ratio ns we re re stricte d to calcium and
pho sphate plasm a le ve ls. Co nsiste nt with studie s
re po rting a le ss hype rcalce mic e ffe ct fo r calcium
ac-etate,
16,24,32,33a statistically significant rise in calcium
le ve ls (7%) was o nly fo und with c arb o nate . This
finding co uld sim ply b e acco unte d fo r b y the lo we r
am o unt o f e le m e ntal calcium give n during ace tate
tre atm e nt ( b y s tud y d e s ign) . In s up p o rt o f this
hypo the sis, the hype rcalce m ic e ffe cts o f the drugs
b e cam e strikingly sim ilar whe n variatio ns in se rum
calcium we re no rm alize d acco rding to the num b e r
o f e q uivale nts ad m inis te re d . Num e ro us s tud ie s
have b e e n m ade that re fute the e xiste nce o f a le sse r
hype rcalce m ic e ffe ct with calcium ace tate in co m
-pariso n to calcium carb o nate .
20-23Intriguingly, the
o n l y p ro s p e c ti ve d o u b l e - b l i n d c ro s s o ve r
co mpariso n in the lite rature favo rs a high fre q ue ncy
o f hype rcalce m ia with calcium ace tate .
23Ho we ve r,
the re we re re le vant diffe re nce s in study de sign that
m ay ac c o u n t fo r th e d is c re p an c y b e twe e n th e
findings. At first, the adm iniste re d do se o f salts in
that study was matched to co ntain the same amo unt
o f e le m e ntal calcium ; and se co ndly, b inde rs we re
give n co nse cutive ly witho ut a washo ut pe rio d.
The reductio ns in serum pho spho rus were
sig-nificant fo r bo th treatments (18.4% fo r acetate and
22.6% fo r carbo nate). There was no significant
differ-ence between the po st-treatment plasma values o f
pho spho rus with the two co mpo unds. Thus, a similar
pho spho rus binding po wer was fo und fo r the salts,
despite the lo wer number o f equivalents o f acetate
administered.
Co mpariso n o f the hyperpho sphatemic and
hy-percalcemic capacity ratio s o f the two salts did no t
sho w a statistically significant difference but tended
to be slightly higher fo r acetate: the pho spho rus
bind-ing po wer o f acetate was abo ut 4.4 times greater than
its hypercalcemic effect while, fo r carbo nate, the value
o f this variable was 3.7.
The present o bservatio ns, in spite o f being
par-tially derived fro m a mathematical exercise, are co
n-sistent with data fro m the literature
13,15,34-37and
sug-gest that a trial o f calcium acetate may be wo rthwhile
in patients undergo ing treatment with calcium carbo
n-ate who have hypercalcemic episo des o r are mo re
pro ne to such co mplicatio n.
CONCLUSION
1. Brent GA, LleBo ff MS, Seely EW, Co nlin PR, Bro wn EM. Relatio nship between the co ncentratio n rate o f change o f calcium and serum intact parathyro id ho rmo ne levels in no rmal humans. J Clin Endo crino l Metab 1988;67:944-50.
2. Co nlin PR, Fajto va VT, Mo rte nse n RM, Lle Bo ff MS, Bro wn EM. Hysteresis in the relatio nship between serum io nized calcium and intact parathyro id ho rmo ne during reco very fro m induced hyper and h yp o c alc e m ia in n o rm al h u m an s . J Clin En d o c rin o l Me tab 1989;320:1140-1.
3. Sherwo o d Lm, Mayer GP, Ramberg CF, Kro nfeld DS, Aubach GD, Po tts JT. Regulatio n o f parathyro id ho rmo ne secretio n: pro po rtio nal co ntro l by calcium, lack o f effect o f pho sphate. Endo crino lo gy 1968;83:1043-51.
4. Reiss E, Canterbury JM, Berco vitz MA, Kaplan EL. The ro le o f pho sphate in the se c re tio n o f p arathyro id ho rm o ne in m an. J Clin Inve st 1970;49:2146-9.
5. Lafflam e GH, Jo wse y J. Bo ne and so ft tissue c hange s with o ral pho sphate supplements. J Clin Invest 1972;51:2834-40
6. Lo p e z-Hilke r S, Dusso AS, Rap p NS, Martin KJ, Slato p o lsky E. Pho sp ho rus re stric tio n re ve rse s hyp e rp arathyro id ism in ure m ia ind e p e nd e nt o f c hange s in c alc ium and c alc itrio l. Am J Physio l 1990;259:432-7
7. Lu c as PA, Bro wn RC, Wo o d h e ad JS, Co le s GA. 1- 25 dihydro xycho lecalcifero l and parathyro id ho rmo ne in advanced chro nic re nal failure : e ffe c ts o f sim ultane o us p ro te in and p ho sp ho rus restrictio n. Clin Nephro l 1986;25:7-10.
8. Po rtale AA, Bo th BE, Hallo ran BP, Mo rris Jr RC. Effe ct o f die tary pho spho rus o n circulating co ncentratio ns o f 1-25 dihydro xyvitamin D and immuno reactive parathyro id ho rmo ne in children with mo derate renal insufficiency. J Clin Invest 1984;73:1580-9.
9. A l f re y A C . A l u m i n u m i n t o xi c a t i o n . N e w E n g l J M e d 1984;310:1113- 4.
10. Larso n EA, Ash SR, White JL, He m SL. Pho sphate b inding ge ls: balancing pho sphate abso rptio n and aluminum to xicity. Kidney Int 1986;29:1131-5.
11. Weberg R, Berstad A. Gastro intestinal abso rptio n o f aluminum fro m single do ses o f aluminum co ntaining antacids in man. Euro J Clin Invest 1986;16:428-32.
12. Kirschbaum BB, Scho o lwerth AC. Acute aluminum to xicity asso ciated with o ral citrate and aluminum co ntaining antacids. Am J Med Sci 1989;297:9-11.
13. Slatpo lsky E, Weerts C, Lo pez-Hilker S, et al. Calcium carbo nate as a pho sphate binder in patients with chro nic renal failure undergo ing dialysis. New Engl J Med 1986;315:157-61.
14. Ramirez JA, Emmett M, White MG, et al. The abso rptio n o f dietary p ho s p ho rus and c alc ium in he m o d ialys is p atie nts . Kid ne y Int 1988;30:753-9.
15. Me ric F, Yap P, Bia MJ. Etio lo gy o f hyp e rc alc e m ia in he m o d ialysis p a t i e n t s o n c a l c i u m c a rb o n a t e t h e ra p y. Am J Ki d n e y Di s 1990;16:459-64.
16. Mai ML, Emmett M, Sheikh MS, Santa Ana CA, Schiller L, Fo rdtran JS. Calcium acetate, an effective pho spho rus binder in patients with renal failure. Kidney Int 1989;36:690-5.
17. Papadakis J, Patrickarea A, Barbatsi A, et al. Calcium acetate: a suitable alternative to calcium carb o nate as pho sphate b inder (ab stract). Vienna, Austria: Pro ceedings o f the XXVII Co ngress o f the Euro pean Dialysis and Transplant Asso ciatio n/Euro pean Renal Asso ciatio n; 1990:279.
18. Schiller LR, Santa Ana CA, Mudassir BS, Sheikh MS, Emmett M, Fo rdtran JS. Effect o f time o f administratio n o f calcium acetate o n
REFERENCES
pho spho rus binding time. New Engl J Med 1989;320:1110-3.
19. Biagini M, Bargana R, Sico li R, Friggi A, Malaguti M. Calcium acetate as a pho sphate b inder: clinical experience in patients o n regular dialysis treatment (abstract). Vienna, Austria: Pro ceedings o f the XVII Co ngre ss o f the Euro p e an Dialysis and Transp lant Asso c iatio n/ Euro pean Renal Asso ciatio n; 1990:270.
20. Ben Hamida F, El Esper I, Co mpagno n M, Mo nière P, Fo urnier A. Lo ng term cro sso ver co mpariso n o f calcium carbo nate as pho sphate binder. Nephro n 1993;63:258-62
21. Almirall J, Veciana L, Llibre J. Calcium acetate versus calcium carbo nate fo r the co ntro l o f serum pho spho rus in hemo dialysis patients. Am J Nephro l 1994;14:192-6
22. Mo niè re P, Dje rad M, Bo udaillie z B, e t al. Co ntro l o f pre dialytic hyperpho sphatemia by o ral calcium acetate and calcium carbo nate. Nephro n 1992;60:6-11.
23. Ring I, Nielsen C, Andersen SP, Behrensss JK, So demann B, Ko rneup HJ. Calcium acetate versus calcium carbo nate as pho spho rus binders in patients o n chro nic hemo dialysis: a co ntro lled study. Nephro l Dial Transplant 1993;8:341-6.
24. Wallo t M, Bo nzel K, Winter A, Geo rger B, Lettgen B, Bald M. Calcium ac e tate ve rsus c alc ium c arb o nate as o ral p ho sp hate b ind e r in pe diatric and ado le sce nt he mo dialysis patie nts. Pe diatr Ne phro l 1996;10:625-30.
25. Massry SG, Co b urn JW, Le e DB, Jo wse y J, Kle e m an CR. Ske le tal resistance to parathyro id ho rmo ne in renal failure. Ann Intern Med 1973;78:357-64.
26. Galc e ran T, Martin KJ, Mo rrisse y JJ, Slato p o lsky E. The ro le o f 1,25(OH)2D3 o n the patho genesis o f skeletal resistance to parathyro id ho rmo ne in chro nic renal failure. Kidney Int 1987;32:801-7.
27. Aro ra KK, Lac e y JP, Sc hac ht RA, Martin DG, Gutc h CF. Calc ific c a rd io m yo p a th y in a d va n c e d re n a l fa ilu re . Arc h In te r M e d 1975;135:603-5.
28. Gipstein RM, Kaplan EL, Katz AI. Hypercalcemia after o ral calcium c arb o nate the rap y in p atie nts o n c hro nic he m o d ialysis. Lanc e t 1973;9:1271-4.
29. Parfitt AM, Massry SG, Winfield AC, De Palma JR, Go rdo n A. Diso rdered c alc iu m an d p h o s p h o ru s m e tab o lis m d u rin g m ain te n an c e hemo dialysis. Am J Med 1971;51:319-30.
30. Milliner DS, Zinsmeister AR, Lieberman E, Landing B. So ft tissue calcificatio n in pediatric patients with end-stage renal disease. Kidney Int 1990;38:931-6.
31. Blo ck GA, Shearo n TEH, Levin NW, Po rt FK. Asso ciatio n o f serum pho spho rus and calcium x pho spho rus pro duct with mo rtality risk in c hro nic he m o d ialysis p atie nts: a natio nal stud y. Am J Kid Dis 1998;31:607-17.
32. She ikh MS, Maguire JA, Em m e t M, e t al. Re d uc tio n o f d ie tary pho spho rus abso rptio n by pho spho rus binders. a theo retical, in vitro and in vivo study. J Clin Invest 1989;83:66-73.
33. Caravaca F, Santo s I, Ro bles R, et al. Calcium acetate versus calcium carbo nate as pho sphate binders in hemo dialysis patients (abstract). Vienna, Austria: Pro ceedings o f the XXVII Co ngress o f the Euro pean Dialysis and Transplant Asso ciatio n/Euro pean Renal Asso ciatio n; 1990:270..
34. Andre ss DL, No rris KC, Co b urn JW, Slato po lsky EA, She rrard DJ. Intraveno us calcitrio l in the treatment o f refracto ry o steitis fibro sa o f chro nic renal failure. New Engl J Med 1989;321:274-9.
r e s u m o
CO N TEX TO :
A hip e rfo sfa te mia te m um imp o rta nte p a p e l no desenvo lvimento de ano rmalidades ó sseas e minerais na insuficiência renal crô nica terminal.OBJETIVO:
Co mparar o acetato de cálcio co m o carbo nato de cálcio q ua nto à s sua s p ro p rie d a d e s q ue la nte s d e fó sfo ro e e fe ito s hipercalcêmico s.TIPO DE ESTUDO:
Ensaio clínico rando miz ado , cruz ado , duplo -ceg o .LOCAL:
Centro de diálise ho spitalar privado .PARTICIPAN TES:
5 2 pacientes em hemo diálise reg ular três vez es po r semana ([Ca] dialisado = 3 ,5 mEq/ l).PROCEDIM EN TOS:
Metade deles recebeu 5 ,6 g / dia de acetato de cálcio e, apó s um perío do de “ washo ut” de duas semanas, 6 ,2 g / dia de carbo nato de cálcio . A o utra metade seg uiu pro to co lo inverso .VARIÁVEIS ESTUDADAS:
Fo ram co nduz idas entrevistas clínicas para mo nito rar efeito s co laterais e o btidas amo stras sang üíneas para determinaçõ es da uréia sérica, cálcio , fó sfo ro , hemató crito , Kt/ V e g aso metria arterial, antes e apó s cada tratamento .RESULTADOS:
3 3 pacientes co mpletaram o estudo . Um aumento sig nificativo no s níveis plasmático s de cálcio só fo i o btido apó s o tratamento co m carbo nato de cálcio [9 ,3 4 mg / dl (SD 0 ,9 1 ) vs. 9 ,9 1 mg / dl (SD 0 ,7 9 ), P < 0 ,0 1 ). A queda no s níveis de fó sfo ro fo i substancial e sig nificante para ambo s o s sais [5 ,6 4 mg / dl (SD 1 ,5 4 ) vs. 4 ,6 0 mg / dl (SD 1 ,3 2 ), P < 0 ,0 1 e 5 ,8 9 mg / dl (SD 1 ,7 1 ) vs. 4 ,5 6 mg / dl (SD 1 ,5 7 ), P < 0 ,0 1 para acetato de cálcio e carbo nato de cálcio , respectivamente). Ao final do estudo , a redução percentual no fó sfo ro sérico po r equivalente de sal administrado po r dia tendeu a ser maio r co m o acetato de cálcio , mas uma diferença sig nificante estatisticamente não fo i enco ntrada.CON CLUSÃO:
O acetato de cálcio po de ser uma bo a alternativa ao carbo nato de cálcio no manejo da hiperfo sfatemia em pacientes co m insuficiência renal crô nica terminal. Q uando o acetato de cálcio é usado o co ntro le da hiperfo sfatemia po de ser alcançado co m uma administração de cálcio meno r, talvez acarretando um risco meno r de hipercalcemia.PALAVRAS-CHAVE:
Ac e ta to de C á lc io . C a rb o na to de C á lc io . Hiperfo sfatemia. Hipercalcemia. Hemo diálise.Acknowle dge me nts: Presented in part at the 24th Annual Meeting o f the American So ciety o f Nephro lo gy, Baltimo re, USA, No vember 1991.
Eufrônio José d’Alme ida Filho, MD. Francisco Santino Filho Kidney Fo undatio n, Rio de Janeiro , Brazil.
Elisa de Albuque rque Sampaio da Cruz, MD. Universidade Federal Fluminense, Niteró i, RJ, Brazil.
Marcos Hoe tte , MD. Francisco Santino Filho Kidney Fo undatio n, Rio de Janeiro , Brazil.
Fre de rico Ruzany, MD, PhD. Francisco Santino Filho Kidney Fo undatio n, Rio de Janeiro , Brazil.
Luana Ne ve s Lope s Ke e n, MD. Universidade Federal Fluminense, Niteró i, Rio de Janeiro , Brazil.
Joce mir Ronaldo Lugon, MD, PhD. Universidade Federal Fluminense, Niteró i, RJ, Brazil.
Source s of funding: No t declared
Conflict of inte re st: No t declared
Last re ce ive d: 14 May 2000
Acce pte d: 20 June 2000
Addre ss for corre sponde nce :
Jo cemir Ro naldo Lugo n
Rua Haddo ck Lo bo , 369/309 - Tijuca Rio de Janeiro /RJ - Brasil - CEP 20260-131 e-mail: jo cerl@ ax.apc.o rg
p u b lis hin g in fo r m a t io n
Invest 1989;83:1349-55.
36. Gallieni M, Brancaccio D, Pado vesi P, et al. Lo w-do se intraveno us calcitrio l treatment o f seco ndary hyperparathyro idism in hemo dialysis patients. Kidney Int 1992;42:1191-8.
37. Muramo to H, Haruki K, Yo shimura A, Mimo N, Oda K, To fuko Y. Tre atm e n t o f re frac to ry h yp e rp arath yro id is m in p atie n ts o n hemo dialysis by intermittent o ral administratio n o f 1,25(OH)
2 vitamin