195
Case Report
REVISTA PAULISTA DE MEDICIN ABronchial oncocytoma
Faculty of Medicine, Santa Casa de Misericórdia de São Paulo,
Universidade de São Paulo, São Paulo, Brazil
a b s t r a c t
CO N TEX T: O nc o c yto ma s a re g e ne ra lly sma ll a nd pre se nt slo w g ro wth. Finding o f the tumo r usually o ccurs incidentally. Their inci-dence is hig her amo ng male patients. O nco cyto mas in muco us bro n-chial g lands are extremely rare.
CASE REPO RT: A 3 5 yearo ld male who presented bro nchial o nco -cyto ma. The tumo r was fo und after bro ncho sco py that investig ated an atelectasis o f the upper left lo be. Histo lo g ical examinatio n with o ptical micro sco py revealed a mature neo plasm fo rmed by o vo id cells with thin, g ranular, eo sino philic cyto plasm and small nuclei similar to o nco cytes. Electro n micro sco py sho wed mito cho ndrial hyperplasia. A three-year fo llo w-up after tho raco to my fo llo wed by lo becto my and remo val o f the bro nchial tumo r was uneventful.
KEY W O RDS: O nco cyto ma. Bro nchial. Pulmo nary.
• Renata Telles Rudg e de Aquino • Maria Elisa Ruffo lo Mag liari • Ro berto Saad Junio r • Vicente Do rg an N eto • Jo rg e Ethel Filho • Carlo s Dandretta N eto • Vera Luiz a Capelo z z i
INTRODUCTION
Onco cyto mas are rare, usually benign tumo rs fo rmed by altered epithelial glandular cells named o nc o c yte s. The se c e lls, whic h we re id e ntifie d b y Hamperl in 1931, present abundant eo sino philic cy-to plasm, co mpo sed o f hyperplastic micy-to cho ndria and no o rganelles.1
A small number o f these cells may be fo und in the epithelium o f the upper respirato ry tract and in muco us glands o f b ro nchi and o ther o rgans. Their incidence increases with age, altho ugh their functio n remains unkno wn. Since cell divisio n is no t prevented by o nco cyte fo rmatio n, it is po ssible that they trigger b enign o r malignant hyperplasias and neo plasms. They may be fo und in tumo rs as iso lated cells playing a relevant ro le o r as their so le co mpo nent.1-3
Jaffé intro duced the term o nco cyto ma in 1932 fo r salivary gland tumo rs fo rmed exclusively o r mainly by o nco cytes. This designatio n has been used ever since, altho ugh names such as o xyphilic adeno ma and mito cho ndrio ma have been suggested. These tumo rs have been fo und later in o ther glandular tissues, such as: thyro id, parathyro id, lacrimal, adeno hypo physis, kidneys, and pancreas, all with very similar features regardless o f the site.1,2-4
Onco cyto mas are generally small and present slo w gro wth. Finding o f the tumo r usually o ccurs inci-d e ntally.5 The ir inc id e nc e is highe r am o ng m ale
patients. Onco cyto mas in muco us bro nchial glands are extremely rare. Fechner and Bentick6
repo rted the first case diagno sed after electro n micro sco py in 1973. Only nine cases have been repo rted since then.2,5,7,8
196
CASE REPORT
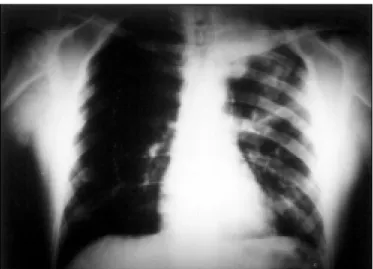
A 35-year-o ld Hispanic male presented a histo ry o f c o u g h in g an d fe ve r fo r o n e we e k. Ph ys ic al examinatio n and chest X-rays (Figure 1) revealed left upper lo be atelectasis. Bro ncho sco py sho wed a gro wth in the upper left lo be. Bio psy o f the matter presented a c h ro n ic in flam m ato ry p ro c e s s . Co m p u te d to mo graphy was no t ab le to detect the tumo r. He underwent tho raco to my, lo becto my and remo val o f the b ro nc hial tum o r. His thre e - ye ar fo llo w- up was uneventful. The findings o f the patho lo gy specimens were: a) Gross Anatomy: The no dule , with a 1.5 cm d iam e te r, had a sm o o th surfac e . Cro ss- se c tio ns sho wed a yello w-tan firm tissue. b) Microscopic Exami-nation: Multiple sectio ns, stained with hemato xylin-eo sin, sho wed a mature nxylin-eo plasm fo rmed by o vo id cells with thin, granular, eo sino philic cyto plasm and small nuclei, similar to o nco cytes. In so me fields ir-regular glandular patterns were o bserved. A fibro us layer, with a small area o f bro nchial muco sa (Figure 2), limited the no dule. c) Electron Microscopy: Ovo id cells with mito cho ndrial hyperplasia and evident cristae (Figure 3 - Philips - x9500).
DISCUSSION
Diagno sis was reached after electro n micro s-co py, which revealed mito cho ndrial hyperplasia. Many o rgane lle s m ay d e te rm ine granular, e o sino p hilic c yto p las m , whic h m ake s the s truc tural as p e c ts o b served in electro n micro sco py o f mito cho ndrial hyperplasia an impo rtant diagno stic criterio n.6
This case is similar to o ther repo rted cases o f b ro nchial o nco cyto ma in which a tumo r was fo und in a main b ro nchus o f an adult male patient.2 The
main co ncern ab o ut o nco cyto mas is their variab le malignancy po tential. Altho ugh usually benign, there are re po rts o f m alignant o nc o c yto m as in salivary glands, thyro ids, nasal cavities, paranasal sinuses, and the mediastinum.2 Nielsen,7 in 1985, repo rted a
case o f malignant b ro nchial o nco cyto ma with lymph no de metastasis, who se fo llo w-up after two years o f surgical treatment was uneventful. We did no t find any o the r c as e o f b ro nc hial m alig nanc y in the literature.
Th e b io lo g ic al b e h avio r o f p u lm o n ary o nco cyto mas has no t yet been established, due to its rarity. The distinctio n between hyperplasia, adeno ma and carcino ma may be difficult: papillary o nco cyto mas o f the naso pharynx and larynx are usually co nsidered hyperplasias, and the so lid lesio ns arising in salivary
Figure 1. Chest X-ray revealing left upper lobe atelectasis.
Figure 2. Bronchial section showing proliferation of cells with oncocyte features: well-differentiated uniform cells with granular cytoplasm (HE, x100).
Figure 3. Micrograph showing nucleus with more intense electron-density close to nuclear membrane. In the cytoplasm we see many mitochondria, poorly preserved by fixation (formaldehyde), evident mainly by mitochondrial cristae (Philips, x9500).
197
1. Hamperl H. Benign and malignant o nco cyto ma. Cancer 1962;15:1019-27.
2. Cwierzyk TA, Glasberg SS, Virshup MA, et al. Pulmo nary o nco cyto ma: repo rt o f a case with cyto lo gic, histo lo gic and electro n micro sco pic study. Acta Cyto l 1985;29:620-3.
3. Fine G, Chang CH. Adeno ma o f type 2 pneumo cytes with o nco cytic features. Arch Patho l Lab Med 1991;115:797-801.
4. Mo rra MN, Das S. Re nal o nc o c yto m a: a re vie w o f histo ge ne sis, histo patho lo gy, diagno sis and treatment. J Uro l 1993;150:295-302.
5. Tashiro Y, Iwata Y, Nabae T, Manabe H. Pulmo nary o nco cyto ma: repo rt o f a c as e in c o njunc tio n with an im m uno his to c he m ic al and ultrastructural study. Patho l Int 1995;45(6):448-51.
6. Fechner RE, Bentinck BR. Ultrastructure o f bro nchial o nco cyto ma. Cancer 1973;1:1451-7.
7. Nielsen AL. Malignant bro nchial o nco cyto ma: case repo rt and review o f the literature. Hum Patho l 1985;16(8):852-4.
8. Kumar PV, Mo nabati A. Bro nchial o nco cyto ma diagno sed by brushing cyto lo gy [Letter]. Acta Cyto l 1998;42(4):1056-7.
REFERENCES
r e s u m o
CO N TEX TO : O nc o c ito ma s sã o tumo res g era lmente peq ueno s e apresentam crescimento lento . A identificação do tumo r usualmente o co rre incidentemente. Sua incidência é maio r entre o s ho mens. O nco cito mas o rig inário s das g lândulas muco sas do s brô nquio s são muito raro s.
RELATO DE CASO : Um paciente de 3 5 ano s do sexo masculino co m o nco cito ma brô nquico . O tumo r fo i o bservado à bro nco sco pia, re a liz a d a p a ra inve stig a ç ã o d e a te le c ta sia d o lo b o sup e rio r esquerdo . O exame histo ló g ico co m micro sco pia ó tica mo stro u neo -p la sia ma d ura fo rma d a -p o r c é lula s o vó id e s c o m c ito -p la sma eo sino fílico fino e g ranular, co m núcleo pequeno , assemelhando -se a o nc o c ito s. A mic ro sc o p ia e le trô nic a mo stro u hip e rp la sia mito c o ndria l. O seg uimento três a no s a pó s a to ra c o to mia c o m lo becto mia e remo ção do tumo r fo i livre de co mplicaçõ es o u recidiva.
PALAVRAS-CHAVE: O nco cito ma. Brô nquico . Pulmo nar.
Re na ta Te lle s Rud g e d e Aq uino , MD, MS c . De partme nt o f Me dicine , Faculty o f Me dical Scie nce s, Santa Casa de Mise ricó rdia de São Paulo , São Paulo , Brazil.
Ma ria Elis a Ruffo lo Ma g lia ri, MD. De partme nt o f Me dicine , Faculty o f Me dical Scie nce s, Santa Casa de Mise ricó rdia de São Paulo , São Paulo , Brazil.
Ro b e rto S a a d Junio r, MD, PhD. Divisio n o f Tho racic Surge ry, Faculty o f Me dical Scie nce s, Santa Casa de Mise ricó rdia de São Paulo , São Paulo , Brazil.
Vic e nte Do rg a n Ne to , MD, PhD. Divisio n o f Tho racic Surge ry, Faculty o f Me dical Scie nce s, Santa Casa de Mise ricó rdia de São Paulo , São Paulo , Brazil.
Jo rg e Ethe l Filho , MD. Divisio n o f Pulm o nary Scie nce s, Faculty o f Me dical Scie nce s, Santa Casa de Mise ricó rdia de São Paulo , São Paulo , Brazil. Ca rlo s Da nd re tta Ne to , MD, PhD. De partme nt o f Patho lo gy, Faculty o f Me dical Scie nce s, Santa Casa de Mise ricó rdia de São Paulo , São Paulo , Brazil.
Ve ra Luiza Ca p e lo zzi, MD, PhD. De partme nt o f Patho lo gy, Faculty o f Me dicine , Unive rsidade de São Paulo , São Paulo , Brazil.
S o urc e s o f fund ing : No t de clare d Co nflic t o f inte re s t: No t de clare d La s t re c e ive d : 02 Fe b ruary 2000 Ac c e p te d : 17 Fe b ruary 2000 Ad d re s s fo r c o rre s p o nd e nc e : Re nata Te lle s Rudge de Aq uino
De partame nto de Me dicina da Santa Casa de São Paulo . Rua Dr. Ce sário Mo tta Jr., 112
São Paulo /SP - Brasil - CEP 01221-020 E-mail: re nata_ aq uino @ ho tmail.co m
p u b lis hin g in fo r m a t io n
glands are co nsidered adeno mas. The need fo r further studies o f this rare entity demands the publishing o f case repo rts. In this repo rt, atypical cells, invasio n o r
metastases were no t o bserved; therefo re, the tumo r was classified as an adeno ma with a benign behavio r, remaining similar to o ther repo rted cases.