www.jped.com.br
ORIGINAL
ARTICLE
Hospital-based
surveillance
of
intussusception
among
infants
夽
Eder
Gatti
Fernandes
a,∗,
Eyal
Leshem
b,
Manish
Patel
c,
Brendan
Flannery
d,
Alessandra
Cristina
Guedes
Pellini
e,
Maria
Amelia
Veras
f,
Helena
Keico
Sato
gaFieldEpidemiologyTrainingProgram/SãoPauloState(EPISUS-SP),SecretariadeEstadodaSaúdedeSãoPaulo,SãoPaulo,SP,
Brazil
bEpidemicIntelligenceService,OfficeofWorkforceandCareerDevelopment,CentersforDiseasesControlandPrevention,
Atlanta,UnitedStates
cDivisionofViralDiseases,CentersforDiseasesControlandPrevention,Atlanta,UnitedStates dCentersforDiseasesControlandPrevention,Atlanta,UnitedStates
eEmergencyDivisionofPublicHealth,SecretariadeEstadodaSaúdedeSãoPaulo,SãoPaulo,SP,Brazil
fDepartmentofSocialMedicine,FaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo,SãoPaulo,SP,Brazil gDivisionofImmunization,SecretariadeEstadodaSaúdedeSãoPaulo,SãoPaulo,SP,Brazil
Received14November2014;accepted2June2015 Availableonline21January2016
KEYWORDS Rotavirusvaccines; Intussusception; Surveillance; Brazil
Abstract
Objective: Intussusceptionsurveillancewasinitiatedafterthenationwideintroductionoflive attenuatedmonovalentrotavirusvaccine(RV1).Theobjectiveistoassesstheepidemiologyof intussusceptionandcomparethenumberofcasesbeforeandaftertheintroductionofrotavirus vaccine.
Methods: CasesofintussusceptionoccurringbetweenMarch2006andJanuary2008were iden-tifiedthroughaprospectiveenhancedpassivesurveillancesystemestablishedinsentinelstate hospitals.Retrospectivereviewofmedicalrecordswasusedtoidentifycases,whichoccurred insentinelhospitalsbetweenJanuary2001andFebruary2006.
Results: From2001to2008,331intussusceptioncaseswereidentified,59.5%weremale,with peakincidenceamongthose18---24weeksofage.Overall<10%ofcaseswereamonginfants6---14 weeksofage(whenthefirstdoseofRV1isadministered).Themostfrequentlyobservedsigns orsymptomsofintussusceptionincludedvomiting(89.4%),bloodystool(75.5%),andabdominal distention (71.8%). A majority(92.1%)ofthe case-patients required surgeryfor treatment; 31.8%ofthosewhounderwentsurgeryrequiredbowelresection,and13(3.9%)died.Among the21hospitalsthatreportedcasesthroughouttheentiresurveillanceperiod(2001---2008),the numberofintussusceptioneventsduring2007(n=26)and2008(n=19)wasnotgreaterthan theaverageannualnumber(n=31,range24---42)duringbaselineyears2001---2005.
夽 Pleasecitethisarticleas:FernandesEG,LeshemE,PatelM,FlanneryB,PelliniAC,VerasMA,etal.Hospital-basedsurveillanceof intussusceptionamonginfants.JPediatr(RioJ).2016;92:181---7.
∗Correspondingauthor.
E-mail:[email protected](E.G.Fernandes). http://dx.doi.org/10.1016/j.jped.2015.06.008
Conclusions: Althoughthisanalysisdidnotidentifyanincreaseinintussusceptioncasesduring thetwoyearsafterRV1introduction,theseresultssupporttheneedforspecialepidemiologic methodstoassessthepotentiallinkbetweenrotavirusvaccineandthisveryrareadverseevent. ©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE Vacinacontra rotavírus; Intussuscepc¸ão; Vigilância; Brasil
Vigilânciahospitalardeintussuscepc¸ãoentreneonatos
Resumo
Objetivo: Avigilânciadaintussuscepc¸ãofoiiniciadaapósaintroduc¸ãodavacinamonovalente vivaatenuadacontrarotavírus(RV1)emtodoopaís.Oobjetivoéavaliaraepidemiologiada intussuscepc¸ãoecompararaquantidadedecasosantesedepoisdaintroduc¸ãodavacinacontra rotavírus.
Métodos: Oscasosdeintussuscepc¸ãoentremarc¸ode2006ejaneirode2008foramidentificados pormeiodeumsistemadevigilânciapassivoprospectivoaprimoradoestabelecidoem hospitais-sentinelaestaduais.Aanáliseretrospectivadeprontuáriosmédicosfoiutilizadaparaidentificar oscasosqueocorreramemhospitais-sentinelaentrejaneirode2001efevereirode2006.
Resultados: De2001-2008,identificamos331casosdeintussuscepc¸ão,59,5%dosquais ocor-reramempacientesdosexomasculino,compicodeincidênciaentreaquelescom18-24semanas deidade.Em geral,<10%dos casosocorreramentreneonatos com6-14semanasde idade (quandoa1adosedeRV1éadministrada).Ossinaisousintomasdeintussuscepc¸ãoobservados commaisfrequênciaincluíamvômito(89,4%),fezescomsangue(75,5%)edistensãoabdominal (71,8%).A maioria(92,1%)dospacientesprecisoude cirurgiapara otratamento;31,8% dos quesesubmeteramàcirurgiaprecisaramderessecc¸ãointestinal,e13(3,9%)vieramaóbito. Entreos21hospitaisquerelataramcasosdurantetodooperíododevigilância(2001-2008), aquantidadedecasosdeintussuscepc¸ãoem2007(n=26)e2008(n=19)nãofoimaiorquea quantidademédiaanual(31,faixade24-42)duranteosanos-basede2001-2005.
Conclusões: Embora esta análise não tenha identificado um aumento nos casos de intussuscepc¸ãonosdoisanosapósaintroduc¸ãodaRV1,esses resultadosjustificama neces-sidadedemétodosepidemiológicosespeciaisparaavaliarapossívelassociac¸ãoentreavacina contrarotavíruseesseeventoadversomuitoraro.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Rotavirusisaleadingcauseofseverediarrhea,accounting for∼453,000deathsannuallyamongchildren<5yearsofage
worldwide.1TheWorldHealthOrganization(WHO)has
rec-ommendedglobalintroduction of oneofthe twolicensed rotavirus vaccines[RotaTeq or RV5 (Merck®, PA, USA)and
Rotarixor RV1(Rotarix®, GlaxoSmithKlineBiologicals,
Rix-ensart, Belgium)] in national immunization programs for preventing severe rotavirus disease.2 In March 2006, the
BrazilianMinistryof HealthintroducedRV1,a live attenu-atedmonovalentvaccinederivedfromhumanG1P[8]strain, simultaneouslyinall27states,throughitsNational Immu-nizationProgram(ProgramaNacionaldeImunizac¸ão[PNI]). A key issue for rotavirus vaccine immunization pro-grams is the need for safety monitoring with regard to intussusception,aformofintestinalobstruction occurring at a background rate of approximately 50 per 100,000 infants.3 An earlier rotavirus vaccine (Rotashield, Wyeth
Vaccines,PA,USA)basedonadifferent(rhesus)strainthan thecurrent WHO recommendedvaccines wasfoundtobe associatedwithan increased risk ofintussusception, with thevaccine causing roughly ten excess casesper 100,000
vaccinatedinfants.4Largeclinicaltrialshavenotdetecteda
riskofintussusceptionassociatedwitheithercurrentlyused vaccines5,6;however,post-licensuresurveillanceinMexico
and Australiahas observed asmallrisk of intussusception aftertheinitialdose.7,8InMexico,anassociationwasfound
between RV1 and intussusception, withthe vaccine caus-ingonetofourexcesscasesofintussusceptionper100,000 vaccinatedinfants.8,9InAustralia,apossibletemporal
clus-tering of intussusception episodes was noted during the sevendaysaftertheinitialdoseofbothRV1andRV5,though therewasnoincreaseinoverallriskat12monthsofage.7In
Brazil,noincreasedriskwasidentifiedafterthefirstdose, but a potential smallrisk wasidentified after thesecond dose of RV1 (excess of 1.5 cases per 100,000 vaccinated infants).9 Nodefiniteincreasedrisk ofintussusceptionhas
been identifiedafteruse of RV5in theUnitedStates, but an excess risk less than one in 65,000 vaccinated infants has not been excluded.10 Marked declines in severe and
fataldiarrheaweredemonstratedinearlyadoptercountries after theintroduction of rotavirus vaccine.11 Because the
rotavirus vaccinationfor all children worldwide.2 Ongoing
post-licensuremonitoringofthesafetyandeffectivenessof rotavirus vaccines is crucial for assessing the risk/benefit profileofrotavirusvaccines.
Thisstudy’sobjectivewastomonitorandcharacterizes theintussusceptioneventsinasubsetofparticipating hos-pitalsand comparesthenumberof intussusceptions cases beforeandaftertheintroductionofrotavirusvaccine.
Materials
and
methods
Intussusceptioncasedefinition
Intussusceptioncase-patientswereincludedifregisteredas
State of São Paulo residents, aged less than 1 year, and
diagnosedwithdefiniteintussusceptionbasedonLevelIof diagnosticcertainty asdefinedby theBrighton Collabora-tionIntussusceptionWorkingGroupcriteria.12 Diagnosisof
intussusceptionisclassifiedasLevel1ifconfirmedbyairor liquid contrastenema, ultrasound (with confirmed reduc-tiononsubsequentultrasoundorenema),or atsurgeryor autopsy.
Settinganddatasources
São Paulo is a highly industrialized Brazilian state. It
is also the most populous: over 41 million people live
there(41,579,695in 2011).The newborn cohorthasbeen
decreasinginrecentyears.In2001,686,533childrenwere borninSãoPaulo,while605,558werebornin2008.13
Two-doserotavirusvaccinecoverageamongchildren<1yearof agereached85.1%in2007and86.3%in2008.14InSãoPaulo
state,thereare9549clinicalpediatricbedsand1048 pedi-atricsurgerybedsdistributedacross893publicandprivate hospitals.
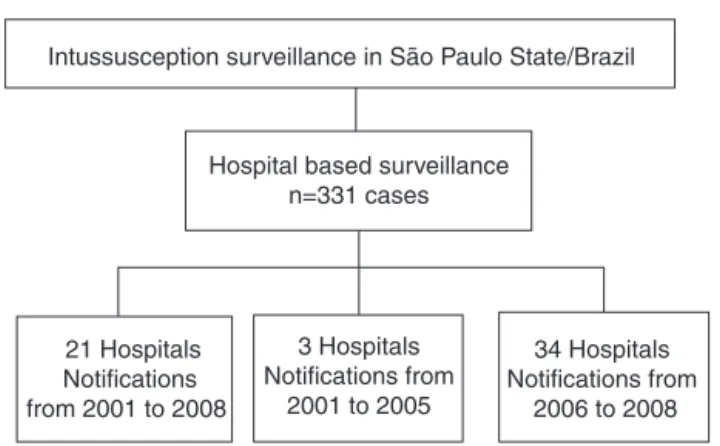
Data on intussusception were obtained from 58 hospi-tals in São Paulo state from 2001 through 2008. These sentinelhospitalswereselectedfromthosewithpediatric surgery services that served as the primary referral hos-pital for intestinal obstruction in each metropolitan area or groups of municipalities (Fig. 1). Not all of these hos-pitalsconducted surveillanceduringtheentire 2001---2008 studyperiod.Thus,for comparisonofthepre-vaccine and post-vaccine periods, data wasonly used from 21 of the 58 hospitals that conducted intussusception surveillance for the entire 2001---2008 period. These hospitals contain 10.2%oftheclinicalpediatricsbedsand12.7%ofthe pedi-atric surgery beds of São Paulo state, but accounted for approximately 30% of the discharge diagnoses of intesti-nal obstruction identified among children younger than 1 yearofageadmittedinpublichospitalsinSãoPauloduring 2001---2005.
Two approacheswereusedtoascertain intussusception cases.Toestablish apre-vaccinebaseline,intussusception caseshospitalizedbetweenJanuary2001andFebruary2006 were identified at each sentinel hospital through retro-spectivereviewof dischargediagnosescodedasintestinal obstruction (K56), according to the International Classifi-cation of Diseases, 10th edition (ICD-10), and diagnoses of intussusception in radiology or surgical log-books. The searchwasconductedduring2006anddatawereabstracted
Intussusception surveillance in São Paulo State/Brazil
Hospital based surveillance n=331 cases
21 Hospitals Notifications from 2001 to 2008
3 Hospitals Notifications from
2001 to 2005
34 Hospitals Notifications from
2006 to 2008
Figure 1 Intussusceptions surveillance among infants aged <12months basedon 58hospitals inSãoPauloState, Brazil, 2001---2008.
from medical records using standardized forms. Cases
occurring between March 2006 and December 2008 were
identified through a prospective surveillance system that was established in sentinel private and public state
hos-pitals. Medical and surgical staff at sentinel hospitals
participated in an initial training in identifying
intussus-ception cases using the validated Brighton Collaboration
Level I case definition. Hospital staff, particularly pedi-atric surgeons, were asked to report cases electronically usinga standard datacollection form.Periodic visits and callsweremadetothehospitaltoencouragereportingand toaddress concerns.Periodic reviewof surgical and
radi-ology logs was conducted to ensure the thoroughness of
reporting.
Statisticalanalysis
The demographic and clinical characteristics of
case-patientsfromallhospitalsweresummarizedusing descrip-tivestatistics.Toexaminepotentialseasonalvariationand
age distribution of intussusception cases, the number of
intussusceptionhospitalizationsinSãoPaulowasplottedby yearandweek ofage. Forthisanalysis,casesfromall58 surveillancehospitalswereused.
It was also of interest to monitor changes in number
of intussusception cases before and after the
introduc-tionofvaccine.Thus,thenumberofintussusceptioncases
per year was plotted for those 21 hospitals that
con-ducted surveillance during the entire 2001---2008 period.
Because rotavirus vaccine coverage among infants was
high after 2006,14 this study compared the number of
intussusceptioneventsduring2007and2008withthe aver-age annual number of cases during the baseline years 2001---2005, considering 2006 as a transition year when rotavirus vaccine was being introduced. The number of intussusceptioncasesfromthese21hospitalswasalso plot-ted by calendar year, according to four age groups: <6 weeks,6---14weeks,15---24weeks,and25---52weeks.All sta-tistical analyses were performed using Epi-Info 3.5.1 (Epi InfoTM,GA,USA)andMicrosoftExcel2007(Microsoft®,WA,
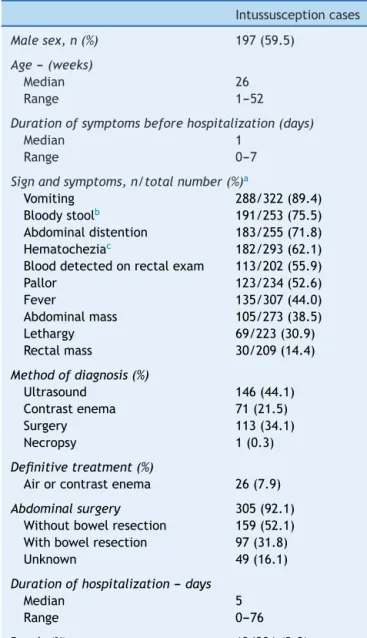
Table1 Demographic andclinicalcharacteristicsof hos-pitalizedintussusceptioncases.StateofSãoPaulo,Brazil, 2001---2008(n=331).
Intussusceptioncases
Malesex,n(%) 197(59.5)
Age---(weeks)
Median 26
Range 1---52
Durationofsymptomsbeforehospitalization(days)
Median 1
Range 0---7
Signandsymptoms,n/totalnumber(%)a
Vomiting 288/322(89.4) Bloodystoolb 191/253(75.5)
Abdominaldistention 183/255(71.8) Hematocheziac 182/293(62.1)
Blooddetectedonrectalexam 113/202(55.9) Pallor 123/234(52.6)
Fever 135/307(44.0)
Abdominalmass 105/273(38.5) Lethargy 69/223(30.9) Rectalmass 30/209(14.4)
Methodofdiagnosis(%)
Ultrasound 146(44.1) Contrastenema 71(21.5)
Surgery 113(34.1)
Necropsy 1(0.3)
Definitivetreatment(%)
Airorcontrastenema 26(7.9)
Abdominalsurgery 305(92.1)
Withoutbowelresection 159(52.1) Withbowelresection 97(31.8)
Unknown 49(16.1)
Durationofhospitalization---days
Median 5
Range 0---76
Death(%) 13/331(3.9)
aMissingdatanotincluded.
b Bloodystool:stoolmixedwithblood(‘‘currantjelly’’). c Hematochezia:passageoffreshbloodthroughtheanus.
Ethics
ThestudywasapprovedbytheEthicsCommitteeof
Irman-dadedaSantaCasadeMisericórdiadeSãoPaulo,registration No.38053.
Results
Clinicalanddemographiccharacteristicsofcases
Between2001and2008,atotalof331intussusceptioncases wereidentifiedinSãoPaulostate(Fig.1).Intussusception casesweremorelikelytobemale(59.5%)andhadamedian ageof26weeks(Table1),withpeakincidenceamongthose
18---24weeksofage(Fig.2).Only9.1%oftheintussusception eventsoccurredamongchildren<15weeksofage,whenthe initialdoseofrotavirusvaccinesistypicallyadministeredin Brazil,whereas 36.6%occurredamongthose15---24 weeks ofage, whentheseconddose ofrotavirus vaccineis typi-callyadministered,and54.4%amongthose25---52weeksof age. Intussusception events occurred year-round,without evidenceofaseasonalpeak(datanotshown).
Themostfrequentlyobservedsignsorsymptoms(Table1) includedvomiting(89.4%),bloodystool(75.5%),and abdom-inaldistention(71.8%).Meandurationofsymptomsbefore presentingformedicalcarewasroughlyoneday.Diagnosis of intussusception wasmade byultrasonography, contrast enema, and surgery in 44.1%, 21.5%, and 34.1% of the case-patients,respectively.Amajority(92.1%)ofthe case-patients were surgically treated for intussusception,with at least 31.8% of those who underwent surgery requiring bowelresection.Amongthe331case-patientshospitalized forintussusceptionduringthestudyperiod,13(3.9%)died. Amongthosesurviving,themeandurationofhospitalization wasapproximatelyfivedays(range:0---76days).
Temporaldistributionofcases
Among the 331 case-patients, 246 (74.3%) were from 21
hospitalsthatidentifiedandreportedintussusception dur-ingtheentire surveillanceperiod,2001---2008. Theoverall demographicandclinicalcharacteristicsofcasesfromthese 21 hospitalswere similartothoseof cases fromhospitals thatonlyreportedcasesforpartofthesurveillanceperiod
(data not shown). When restricting the analysis to cases
at the21hospitalswithstablereportingduringtheentire 2001---2008surveillanceperiod,noincreasewasobservedin
the numberofreported intussusceptioneventsduring the
surveillanceperiodaftervaccineintroduction.Theobserved numberof intussusceptionevents during2007 (n=26)and 2008(n=19)wassomewhatlowerthantheaverageannual numberofintussusceptioncases(n=32casesperyear,range 24---42casesperyear)during2001---2005(Fig.3).
Discussion
Efforts tobuildcapacityfor intussusceptionmonitoring by theDivisionofImmunizationoftheStateofSãoPaulo iden-tifiedseveralimportantlessonsforfuturerotavirusvaccine safetymonitoringeffortsinBrazil.First,theagedistribution of intussusception in SãoPaulo is similartothat in other regions ofthe world,with<10% ofcases occurringamong those<15 weeksof age.15---17 At thisage, thefirst dose of
rotavirusvaccine---thedosewiththehighestpotentialrisk ofintussusception--- istypicallyadministered.Thisfinding indicates that it would be necessary to expand surveil-lance toa large number of hospitals in orderto identify enoughcasestoassessriskofintussusceptionaftertheinitial doseofrotavirusvaccination.Identifyingafour-tofive-fold increase in risk of intussusception relative tobackground mightnotbepossiblewhenassessingtrendsof intussuscep-tionamongallinfantsunderoneyearofagewhotypically have background rates of ∼40---50 per 100,000.18 Second,
25
20
15
10
5
Hospitalizations f
or intussusception (nº of cases)
0
1 3 5 7 9 11 13 15 17 19 21
Age at hospitalization (weeks)
23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Figure2 Agedistributionofinfantswithintussusceptionsbyweekofagefrom58hospitalsinSãoPauloState,2001---2008(n=331).
non-surgical treatment with air/contrast enema is used
moreoften.19---21 Thisfindinghasimplicationsfor
resource-poorsettings,inthatnetworkingwithsurgeonsandhospitals withsurgical centerscouldenhancesurveillancefor intus-susception after theintroduction of vaccine. Third,while cautious interpretation is warranted, this study did not observe asubstantial increase in the number of intussus-ceptioncasesduringthepost-vaccineintroductionperiod, whensome85% oftheinfantshadreceivedvaccinationin Brazil.
Brazilwasoneoftheearlyadoptersofrotavirusvaccine, and has documented large reductions in hospitalizations anddeaths relatedtodiarrhea amongchildren underfive years age since the introduction of rotavirus vaccines.14
Whileclinicaltrialsfor rotavirusvaccineshave not identi-fiedavaccine-associatedincreasedriskofintussusception, largepost-licensureevaluationsinMexicoandAustraliahave foundalow riskafterthefirstdoseof bothrotavirus vac-cines, amounting to roughly one to four excess cases of intussusception for every 100,000 vaccinated children.7---9
While a cautious interpretation is warranted, since the present surveillance wasnot intended to quantify risk of intussusception associated with RV1, it is reassuring that therewas nolarge increase in intussusceptioncases at a populationlevelfollowingvaccineintroductioninthestate ofSãoPaulo,Brazil.
Trendanalysiscannotexcludeariskofsimilarmagnitude tothatseen inMexicoandAustralia aftertheinitialdose, particularly because background rates of intussusception areverylow(∼10---20per100,000infantyearsduring6---12
weeksofagewhenthefirstdoseisadministeredinBrazil).3,9
Assessingtrendsinnarrowagewindowsmightbeuseful,but samplesizeistypicallyinsufficientforconfidentlyexcluding risk,evenwithnationaldatasetsfromcountrieswithlarge birthcohorts,suchastheUnitedStates.3
Analytic epidemiologic studies, such as those employ-ingthe case-seriesor thecase---controlmethod,would be
45
RV1 introduction
40
35
30
25
20
15
10
5
0
2001 2002 2003 2004 2005
Year of Hospitalization
Hospitalizations f
or intussusception
(nº of cases)
2006 2007 2008
Figure 3 Trends in yearly intussusception hospitalizations amonginfantsaged<12monthsbetween2001and2008.Data arefrom21 sentinel hospitalsofthehospital-based intussus-ceptionsurveillanceofSãoPauloState,Brazil(n=246).
necessary forassessing a magnitudeof riskof one totwo
excess adverse events per 100,000 vaccinated children.
Surveillance platforms similar to that established by the
State of São Paulo are the backbone for such
epidemio-logicstudies, providedthat intussusceptioncase-findingis activeandindependentofthevaccinationstatus. Indeed,
several of these hospitals from São Paulo enhanced and
continued surveillance as part of a nationwide study in
Brazilthatassessedrisk ofintussusceptionafterRV1using self-controlledcase-seriesandcase---controldesign.Inthat nationwidestudy,noriskofintussusceptionwasfoundafter thefirstdoseofrotavirusvaccineinBrazil,butalow-level risk was detected after the second dose.9 Initiating this
monitoring inother settingswithout any existingnational safetymonitoringplatforms,particularlyforbuilding capac-ity for safety monitoring and for obtaining established platforms that can be utilizedfor specialized studies for assessingriskasnewsafetyconcernsarise.
Inthepresent cohort,90%of theintussusception case-patientsrequiredsurgery.Thisiscomparabletotreatment standards in resource poor settings, while in industrial-ized countries only 10---50% of patients require surgical treatment.15,19---21 The reasons for the high rates of
surgi-cal treatment among cases remain a subject for further investigation. Delays in presentation and treatment may also explain the higher in-hospital mortality of 4---5% in someregionsofBrazil9and
∼12---13%reportedfromAfrica,15
compared with 1% in Mexico9 and <1% in industrialized
countries.19---21 Improving diagnosis and early intervention
withnon-invasivereductiontechniques havethepotential toreducemorbidity andmortalityin Brazil.Further stud-iesidentifyingrisk-factors forsevere outcomesrelated to intussusceptioninBrazilarewarranted.
Thisevaluationhasseverallimitations.First,thisstudy consideredsentinelservices.Thereportedcasesdonot rep-resentall intussusception cases of São Paulo state during thestudiedperiod.Theselectedserviceshave30%of pedi-atricsbedsoftheStateofSãoPaulo’spublichealthsystem, whichcovers∼60%thepopulation.Withoutaprecise
popu-lationdenominator,itisnotpossibletocalculateincidences. Results in absolute numbers can be influenced by popu-lationchanges, such asdecrease in birth rate over time. Second, using different surveillance methods before and aftertheintroductionofvaccinelimitstheabilityto confi-dentlycomparetherateofeventsbetweenthetwoperiods, particularlybecauseofdifferencesinmethodsof ascertain-ingcases.These results alonecannot beusedtorefutea casualassociationbetweenrotavirusvaccinationand intus-susception,andcannotbedirectlycomparedwithdatafrom post-licensuremonitoringinMexicoandAustralia.7,8Third,
vaccinationhistoryofcaseswasnotavailable.Moreover,the completenessandaccuracy ofdata describing theclinical presentationand managementofintussusceptions reflects recordingcompleteness inmedicalrecords.Fourth, intus-susceptionisarareevent,especiallyamonginfantsaged<3 months;relativelysmallchangesinabsolutenumbersin nar-rowerageranges,suchasinfants aged6---14 weeks,could resultan increase or decrease in trend by chance alone. Last,hospitalbasedsurveillancemaynotberepresentative ofallintussusceptionevents, particularlyinresourcepoor settingswhereaccesstopediatricdiagnosticfacilitiesand treatmentislimited.
Since 2006, rotavirus vaccines have been introduced in over 30 countries worldwide.22 While the benefits of
rotavirusvaccinationintermsofreducingsevereandfatal diarrheahavefar outweighed thelow risk of intussuscep-tion,the ongoing monitoring of intussusception after the introduction of vaccine is important for ensuring vaccine safetyandmaintainingpublictrustintherotavirusvaccine program.Thepresentexperience,establishing intussuscep-tion surveillance for monitoring post licensure rotavirus vaccinesafetyinSãoPaulo,shouldprovidevaluable infor-mation for other similar countries that are introducing rotavirusvaccineanddonothaveexistingsafetymonitoring systems.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.ParasharUD,BurtonA, Lanata C,Boschi-Pinto C,Shibuya K, SteeleD,etal.Globalmortalityassociatedwithrotavirus dis-easeamongchildrenin2004.JInfectDis.2009;200:S9---15. 2.MeetingoftheStrategicAdvisoryGroupofExpertson
immuniza-tion,October2009--- conclusionsandrecommendations.Wkly EpidemiolRec.2009;84:517---32.
3.YenC,TateJE, Steiner CA,CorteseMM, PatelMM, Parashar UD.TrendsinintussusceptionhospitalizationsamongUSinfants beforeandafterimplementationoftherotavirus vaccination program,2000---2009.JInfectDis.2012;206:41---8.
4.MurphyTV,GargiulloPM,MassoudiMS,NelsonDB,JumaanAO, OkoroCA,etal.Intussusception amonginfantsgivenanoral rotavirusvaccine.NEnglJMed.2001;344:564---72.
5.Ruiz-PalaciosGM,Pérez-SchaelI,VelázquezFR,AbateH,Breuer T, Clemens SC, et al. Safety and efficacy of an attenuated vaccineagainstsevererotavirusgastroenteritis.NEnglJMed. 2006;354:11---22.
6.Vesikari T, MatsonDO, DennehyP,Van DammeP, Santosham M, Rodriguez Z, et al. Safetyand efficacy ofa pentavalent human-bovine(WC3) reassortant rotavirus vaccine.N Engl J Med.2006;354:23---33.
7.Buttery JP, Danchin MH, Lee KJ, Carlin JB, McIntyre PB, Elliott EJ, et al. Intussusception following rotavirus vaccine administration: post-marketing surveillance in the National ImmunizationPrograminAustralia.Vaccine.2011;29:3061---6. 8.VelázquezFR,ColindresRE,GrajalesC,Hernández MT,
Mer-cadillo MG, Torres FJ, et al. Postmarketing surveillance of intussusception following mass introduction of the attenu-atedhumanrotavirusvaccineinMexico.PediatrInfectDisJ. 2012;31:736---44.
9.Patel MM, López-Collada VR, Bulhões MM, De Oliveira LH, BautistaMárquezA,FlanneryB,etal.Intussusceptionriskand healthbenefitsofrotavirusvaccinationinMexicoandBrazil.N EnglJMed.2011;364:2283---92.
10.Shui IM, Baggs J, Patel M, Parashar UD, Rett M, Belongia EA, et al. Risk of intussusception following administration of a pentavalent rotavirus vaccine in US infants. JAMA. 2012;307:598---604.
11.Richardson V, Hernandez-Pichardo J, Quintanar-Solares M, Esparza-AguilarM, Johnson B, Gomez-Altamirano CM, et al. Effectofrotavirusvaccinationondeathfromchildhooddiarrhea inMexico.NEnglJMed.2010;362:299---305.
12.Bines JE, Kohl KS, Forster J, Zanardi LR, Davis RL, Hansen J, et al. Acute intussusception in infants and children as anadverseeventfollowingimmunization:casedefinitionand guidelinesofdatacollection,analysis,andpresentation. Vac-cine.2004;22:569---74.
13.Fundac¸ão Sistema Estadual de Análise de Dados. Portal de Estatísticas do Estado de São Paulo; 2012. Available from: http://www.seade.gov.br/index.php?option=comjce&Itemid= 39&tema=5[cited17.12.12].
14.doCarmoGM,YenC,CortesJ,Siqueira AA,de OliveiraWK, Cortez-EscalanteJJ,et al.Declineindiarrhea mortalityand admissionsafterroutinechildhood rotavirus immunizationin Brazil:atime-seriesanalysis.PLoSMed.2011;8:e1001024. 15.SteeleAD,PatelM,CunliffeNA,BreseeJS,BorgsteinE,Parashar
UD.WorkshoponintussusceptioninAfricancountries---meeting report.Vaccine.2012;30:A185---9.
ina sentinelpaediatrichospital:benefitsandpitfallsfor use inpost-marketingsurveillanceofrotavirusvaccines.Vaccine. 2012;30:A190---5.
17.KhumjuiC,Doung-ngernP,SermgewT,SmitsuwanP,Jiraphongsa C.Incidenceofintussusceptionamongchildren0---5yearsofage inThailand,2001---2006.Vaccine.2009;27:F116---9.
18.PatelMM,HaberP,BaggsJ,ZuberP,BinesJE,ParasharUD. Intus-susceptionandrotavirusvaccination:areviewoftheavailable evidence.ExpertRevVaccines.2009;8:1555---64.
19.Tate JE, Simonsen L, Viboud C, Steiner C, Patel MM, Curns AT, et al. Trends in intussusception hospitalizations amongUSinfants,1993---2004:implicationsformonitoringthe
safetyof thenew rotavirus vaccination program.Pediatrics. 2008;121:e1125---32.
20.BinesJE,LiemNT,JusticeFA,SonTN,KirkwoodCD,deCampoM, etal.RiskfactorsforintussusceptionininfantsinVietnamand Australia:adenovirusimplicated,butnotrotavirus.JPediatr. 2006;149:452---60.
21.Buettcher M, Baer G, Bonhoeffer J, Schaad UB, Heininger U. Three-year surveillance of intussusception in children in Switzerland.Pediatrics.2007;120:473---80.