1 Nurse; PhD in Nursing, e- m ail: soniaapaiva@t erra.com .br; 2 Professor, University of São Paulo at Ribeirão Preto, School of Nursing, WHO Collaborating Center for Nursing Developm ent Research, Brazil, e- m ail: elaus@glete.eerp.usp.br
Disponible en castellano/ Disponível em língua portuguesa SciELO Brasil w w w .scielo.br/ rlae
HOSPI TAL CARE: ASSESSMENT OF USERS’ SATI SFACTI ON DURI NG HOSPI TAL STAY
Sônia Maria Alves de Paiva1
Elizabet h Laus Ribas Gom es2
Paiva SMA, Gom es ELR. Hospit al care: assessm ent of users’ sat isfact ion during hospit al st ay. Rev Lat ino- am Enferm agem 2007 set em bro- out ubro; 15( 5) : 973- 9.
Healt h car e t eam s hav e follow ed t he Nat ional Healt h Sy st em ’s ( SUS) pr inciples t o ensur e qualit y im provem ent in healt hcare, and pat ient sat isfact ion is one of t he inst rum ent s used t o evaluat e qualit y. This st udy aim ed t o evaluat e pat ient sat isfact ion regarding t he assist ance t o t heir needs during hospit alizat ion, in a general hospit al of a cit y in t he int erior of São Paulo. Dat a were collect ed t hrough part icipant observat ion and use of focal group t echniques in t his qualit at ive research. A t hem e guide was used and a t ot al of 20 subj ect s part icipat ed in t he st udy. Dat a were analyzed t hrough cont ent analysis and int erpret ed t hrough t riangulat ion. Study results dem onstrate that patients were satisfied with the care rendered. However, the researcher concluded that the institution’s work organization is not directed to the attainm ent of quality.
DESCRI PTORS: qualit y of healt h care; pat ient sat isfact ion; evaluat ion
ATENCI ÓN HOSPI TALARI A: EVALUACI ÓN DE LA SATI SFACCI ÓN DE LOS PACI ENTES
DURANTE SU PERÍ ODO DE I NTERNACI ÓN
El equipo de salud ha tom ado com o base los principios del SUS para asegurar la calidad de la atención. La sat isfacción de los pacient es ha sido ut ilizada com o uno de los inst rum ent os de evaluación. Est e est udio busca evaluar la satisfacción de los pacientes con la atención de sus necesidades durante la internación, en un hospit al general del int erior de Sao Paulo. Se adopt ó com o m et odología la invest igación cualit at iva y, com o t écnica de r ecolect a de dat os, la obser v ación par t icipant e y el gr upo focal. Se ut ilizó un guía de t em as y part iciparon en la invest igación doce suj et os. El análisis de los dat os se basó en el análisis de cont enido. Para la interpretación se utilizó la técnica de triangulación. Los resultados dem ostraron que los pacientes se sintieron satisfechos con la atención. No obstante, la investigadora concluyó que la form a de organización del trabaj o de la inst it ución no evidencia una preocupación por la calidad de la at ención.
DESCRI PTORES: calidad de la at ención de salud; sat isfacción del pacient e; evaluación
ASSI STÊNCI A HOSPI TALAR: AVALI AÇÃO DA SATI SFAÇÃO DOS USUÁRI OS DURANTE SEU
PERÍ ODO DE I NTERNAÇÃO
A equipe de saúde t em se baseado nos princípios do SUS para assegurar a m elhoria do at endim ent o dos serviços de saúde e a satisfação dos usuários e tem sido utilizada com o um dos instrum entos de avaliação da qualidade. Este estudo obj etivou avaliar a satisfação dos usuários com o atendim ento de suas necessidades durant e a int ernação, num hospit al geral do int erior do Est ado de São Paulo. Adot ou- se, com o m et odologia, a pesquisa qualitativa e, com o técnica de coleta de dados, a observação participante e o grupo focal. Foi utilizado um guia de t em as e part iciparam da pesquisa doze suj eit os. Realizou- se a análise de cont eúdo dos dados e, par a a int er pr et ação, ut ilizou- se a t écnica de t r iangulação. Os r esult ados dem onst r ar am que os usuár ios ficaram sat isfeit os com o at endim ent o. Ent ret ant o, a pesquisadora concluiu que a organização do t rabalho da inst it uição não t em com o m et a o alcance da qualidade.
I NTRODUCTI ON
T
h e in t er est on t h e qu alit y of ser v ices is pr esen t on t h e pr in ciples of SUS ( Nat ion al Healt h Pr o g r a m ) a n d i s p a r t o f t h e r o u t i n e o f h o sp i t a l organizat ions( 1). Qualit y can be defined as a priorit y,feat ure, or condit ion of t hings and people t hat m ake t h em d i f f er en t f r o m o t h er s an d d et er m i n e t h ei r nat ure( 2). To cont rol and ensure qualit y of act ions in
the health sector, it is essential to introduce indicators t o a sse ss t h e o u t co m e s r e a ch e d a n d p l a n t h e necessary changes( 3- 4).
To assess m eans t o det erm ine t he value of som et hing m ak ing t he not ion of qualit y ex plicit( 2 ).
Am ong t he indicat or s used, w e can highlight social indicat ors ( illit eracy rat e, level of educat ion, incom e, an d u n em p loy m en t r at e) ; st an d ar d in d icat or s of hospit al m anagem ent , focusing on hum an resources ( ab sen t eei sm , t u r n o v er ) ; i n d i cat o r s f o cu si n g o n hospital m anagem ent ( rate of bed use) and indicators focusing on t he client s ( m ort alit y rat e, infect ion rat e, and client sat isfact ion)( 6).
I n addition to those, there are the indicators that assess care using three com ponents( 5), structure,
involving physical, hum an, m at erial, equipm ent and f i n a n ci a l r e so u r ce s n e e d e d f o r m e d i ca l ca r e ;
processes, that refer to the activities involving health p r o f e ssi o n a l s a n d p a t i e n t s; a n d o u t co m e s,
corresponding t o t he final product of t he care given; I n nursing, crit ical point s of care are com m only used t o assess qualit y of car e, such as nur sing r ecor ds, et h ical pr ocesses, appear an ce of pr essu r e u lcer s, f a l l s, a d m i n i st r a t i o n o f m e d i ca t i o n s, o r g a n i zi n g p e r so n n e l , a m o n g o t h e r s( 7 ). Cu r r e n t l y, u se r s’
sat isf act ion h as been con sider ed as an im por t an t com ponent of quality of care, as part of the m odel of participative care proposed by SUS and because users ar e m or e aw ar e of t h eir r ig h t s; t h ey also p lay a significant role in the interaction between care givers and users, because it expresses the expectations and the evaluations of users regarding the care received( 3-4 ). Usi n g u se r s’ sa t i sf a ct i o n a s a n a sse ssm e n t
inst r um ent m eans t o under st and and act accor ding to their needs regarding the services and products of t h e t eam , con sider in g t h eir su bj ect iv it y an d t h eir percept ion on t he process of work( 8).
Based on t hese st at em ent s, t his st udy w as d ev el o p w i t h t h e o b j e ct i v e o f a ssessi n g u ser s’ sat isf act ion r egar din g m eet in g t h eir h ealt h n eeds during hospital stay, as an elem ent to assess quality.
METHODOLOGY
Met h o d o l o g y ch o sen w a s t h e q u a l i t a t i v e research, and data collection started after the proj ect was approved by the Ethical Com m ittee of the Nursing School of Ribeirão Pret o ( EERP- USP) . The st udy was conduct ed in t he Unidade de Clínica Médica ( Clinical Un i t ) o f a p r i v a t e p h i l a n t h r o p i c h o sp i t a l i n t h e countryside of the State of São Paulo. Data collection t ech n iq u es w er e u sed t og et h er w it h p ar t icip at iv e o b ser v a t i o n a n d f o cu s g r o u p , co m p l em en t ed b y docum ent al assessm ent of t he chart s.
Par t icipat iv e obser v at ion w as im por t ant for t h e st u dy, becau se it en abled t o ch ar act er ize t h e con t ex t of t h e u n it , u n d er st an d h ow t h e w or k is organized t echnically and socially, and t he aspect s of the relationship of the team and users. Additionally, it enabled cont inuous int er act ion w it h t he subj ect s t o hear about t heir experiences, t heir relat ionship wit h professionals and it was essential to notice the “ cues” t hat allowed t o select t he subj ect s t o conform t o t he focus groups. I t was conducted from May to July 2005, daily, in t he m orning.
I nclusion crit eria in focus groups was users t h at st ay ed in t h e h ospit al for at least fou r day s, because t his w as consider ed t he per iod necessar y for their adaptation to the hospital environm ent; adults liv ing in t he cit y, t hat could com m unicat e ver bally, t hat w er e chr onologically and spat ially aw ar e, and t hat were self- sufficient regarding physical m obilit y.
Th e ch o i ce t o u se f o cu s g r o u p s a s a m et hodological st r at egy w as because w e believ e it allow s a br oad pr ocess of ex per iences, infor m at ion and because individuals are m ore susceptible of being encour aged w hen t hey ar e w it h ot her s r at her t han alone( 9).
Users were inform ed about t he research and t hose w ho agr eed t o t ak e par t , r eceiv ed guidelines on the confidentiality and anonym ity of the inform ation and on t he writ t en consent . The docum ent was read with them , and then, they were asked to sign it. They were also explained about the need for recording and not ing down t he m eet ing. Thus, 12 people t ook part on t he survey.
Tw o f ocu s g r ou p s w er e f or m ed , g r ou p A, form ed by I ara, Márcio, Carolina, Ronaldo and Fabrício ( fictional nam es) and group B, form ed by Natal, Fábio, Selm o, Ana, Jair, Álvaro and Naldo ( fict ional nam es) , from t he t heoret ical reference( 10). We have chosen t o
discharge, because we considered t hat hospit al st ay could int erfere in t he answer of users. Places chosen were t he Basic Healt h Unit s near t heir hom es. Basic r ules for liv ing, t im e, and dur at ion of each session were established so that each group would work. The com m itm ent of each person and the confidentiality of what was discussed were reassured.
Two m eet ings t ook place for each group and a t hem e guide was used wit h guiding quest ions t hat led t hem t o r eflect on t he car e t hey had r eceiv ed fr om pr ofession als du r in g t h e t im e t h ey st ay ed in hospit al:
- what difficulties did you face to be adm itted? - w ho w er e t he pr ofessionals t hat car ed for t hem ? How did you like the care?
- how did you assess if care was good?
- what situations m ade you happy about hospital stay? To perform wit h t he groups, t he researcher had the help of a nursing student playing the role of observer who was previously guided for this role and that was in charge of recording the com m ents of the g r ou p , m on it or in g t im e, an d con t r ollin g t h e t ap e r ecor der.
Content analysis was used in data analysis( 11) .
Based on this perspective of analysis, tapes have been transcribed and the data obtained in observations were sy st em at ized as t ex t s; nex t , t he m at er ial of focus groups was organized. We aim ed at working with the set of obser v at ion s an d st at em en t s of t h e gr ou ps h or izon t ally, m ak in g t h e cu t s, cat eg or izat ion an d coding in the pre- analysis stage. I n the second stage, we cut off the significant unities, getting to the register nuclei and, on the third stage, data interpretation was perform ed, using t riangulat ion of t he st at em ent s of g r o u p s, o f t h e d a t a o f t h e f i el d d i a r i es, a n d o f part icipat ive observat ion( 12).
OUTCOMES AND CASE DI SCUSSI ON
Charact erizat ion of t he subj ect s
Dat a dem on st r at ed t h at 6 of t h e su bj ect s were retired, 2 did household chores, 2 were workers, 1 was a student, and 1 was unem ployed. Males were predom inant, with 10 subj ects. Mean age was 54 and, r eg ar d in g ed u cat ion , 1 1 h ad f in ish ed elem en t ar y school. These dat a was im port ant because it enabled t o l e a r n t h a t p a r t i ci p a n t s p r e se n t e d a l o w socioeconom ic and cult ural level.
Analy sis Cat egor y
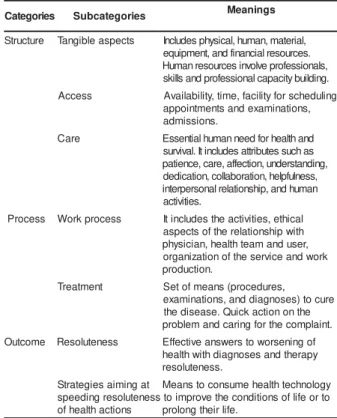
Analy sis w as per for m ed w it h t he help of a t h e o r e t i c a l r e f e r e n c e s t r u c t u r e f o l l o w i n g Don abedian ’s m odel, based on st r u ct u r e, pr ocess, and out com es( 5). Thus, t he t angible aspect s em erged
f r om t h e cat eg or y st r u ct u r e; t h e su b cat eg or ies: access, car e, w or k pr ocess and t r eat m ent em er ged from t he cat egory pr oce ss; and t he subcat egories: r eso l u t en ess an d st r at eg i es f o r sp eed i n g h eal t h act ions em erged from t he cat egory out com e. These dat a ar e pr esen t ed on Table 1 , accor din g t o t h eir m e a n i n g s , a c h i e v e d f r o m t h e a n a l y s i s , a n d int er pr et at ion of t hem at ic sent ences.
Table 1 - Analysis and m eaning of speech of subj ects based on Donabedian’s principles
I t is wort h m ent ioning t hat t hese out com es present ed are im port ant t o t his populat ion st udied.
Regar ding st r u ct u r e , t he t angible aspect s w er e r elat ed t o pr oblem s w it h t he facilit ies, as w e could see.
I t needs painting, the windows have to be fixed, those
in our bedroom were all broken ( Natal) .
Cleaning of the place was also m entioned and t here were cont radict ory opinions.
I liked the cleaning, the cleaner com es all the tim e, and
good care is taken ( I ara) . s e i r o g e t a
C Subcategories Meanings
e r u t c u r t
S Tangibleaspects Includesphysica,lhuman,mateira,l . s e c r u o s e r l a i c n a n if d n a ,t n e m p i u q e , s l a n o i s s e f o r p e v l o v n i s e c r u o s e r n a m u H . g n i d li u b y ti c a p a c l a n o i s s e f o r p d n a s ll i k s s s e c c
A Avaliablitiy,itme,faclitiyforscheduilng , s n o it a n i m a x e d n a s t n e m t n i o p p a . s n o i s s i m d a e r a
C Essenitalhumanneedforheatlhand s a h c u s s e t u b ir tt a s e d u l c n i tI .l a v i v r u s , g n i d n a t s r e d n u , n o it c e ff a , e r a c , e c n e it a p , s s e n l u f p l e h , n o it a r o b a ll o c , n o it a c i d e d n a m u h d n a , p i h s n o it a l e r l a n o s r e p r e t n i . s e it i v it c a s s e c o r
P Workprocess tIincludestheacitviites,ethical h ti w p i h s n o it a l e r e h t f o s t c e p s a ,r e s u d n a m a e t h tl a e h , n a i c i s y h p k r o w d n a e c i v r e s e h t f o n o it a z i n a g r o . n o it c u d o r p t n e m t a e r
T Setofmeans(procedures, e r u c o t ) s e s o n g a i d d n a , s n o it a n i m a x e e h t n o n o it c a k c i u Q . e s a e s i d e h t .t n i a l p m o c e h t r o f g n ir a c d n a m e l b o r p e m o c t u
The wom en’s toilet is very bad; we have to take a shower
5 o’ clock in the m orning, after six it is im possible to shower. The
cleaners clean it, but there are tim es there is no condition for use
(Ana).
Re g a r d i n g m a i n t e n a n ce o f t h e u si n g co n d i t i o n s o f t h e t o i l e t s, i t w a s co n si d e r e d a s unsat isfact ory unanim ously am ong t he part icipant s.
The showers near t he corner and at t he back were t he
only that were hot, you get electric shock from all of them , you
have to use a t owel ( Nat al) .
Regar ding hum an r esour ces, user s not iced t he short age of st aff.
I was very well t reat ed, no doubt about it , the nurses
were well trained, careful, but there was a sm all num ber of nurses
for the am ount of patients, I think they share there 4 bedroom s
for each 2 of them , so they have no tim e left for them , they get
exhausted, som etim es it is tim e for m edications, after a short
while it is in t hat hurry again ( Ronaldo) .
Assessm ent of the structure also includes the technical skills of the nursing team and knowing how t o d o. Tech n i cal sk i l l s w er e r el at ed t o t ech n i cal perform ance and the behavior of care givers. Technical p er f or m an ce in v olv ed h ow t o m an ag e an d in j ect m edicat ion, punct ure a vein, and how t o perform a bed bat h.
I noticed they were trained because of how they do the
j ob, how they apply an inj ection, place the serum , I m ean,, what
is basic for a “ nurse” , within their standards, they do everything
perfectly, I ’ve noticed that ( Ronaldo) .
The behav ior of car e giv er s inv olv ed t heir at t ribut es, as I ara’s st at em ent illust rat es.
Ah, I saw t hem t ak ing car e of t he old lady w it h
tenderness, bath her on the bed, soaking the cloth with soap,
passing it on her skin gently, one worker passes it and the other
dries, very gent ly, and when t hey had t o change her, t hey were
very careful, I t hought t his was very beaut iful ( I ara) .
Th e se st a t e m e n t s d e m o n st r a t e t h a t t h e assessm ent of t he perform ance of t he professionals was t echnical and very lim it ed, because t hey did not have scient ific knowledge enough t o assess if a care was well done, and in t he hum an dim ension t hrough t he r elat ionship of t hem and t he pr ofessionals w ho t ook care of t heir healt h.
Diet was consider ed good for t he m aj or it y, and t hey m ent ioned food present at ion, preparat ion, and t he am ount , as posit ive aspect s.
Although data dem onstrate that the infirm ary structure was poor, expressed by m inim um conditions t h at cou ld b e im p r ov ed , an d t h at w ou ld m ak e a difference in care, there was resignation in the attitude
of part icipant s. We believe t hat t his was due t o t heir l o w so ci o e co n o m i c a n d cu l t u r a l l e v e l . Ho w e v er, thinking about quality and hum anization in health care, a l so i m p l i e s t h i n k i n g a b o u t t h e e n v i r o n m e n t condit ions, including invest m ent s t o recover physical facilities of the institutions, and renovating equipm ent and t echnology t o im prove t he infrast ruct ure( 13).
The cat egory Process enabled t o conform t o t he subcat egor ies: access, car e, w or k pr ocess, and t r eat m ent .
Dat a sh ow ed t h at m ost p ar t icip an t s w er e sat isfied wit h access, exem plified by I ara’s st atem ent in group A.
I arrived at 6h 30 in t he m orning, m y adm ission was
done im m ediat ely, when it was 6 h 50 I was already in t he
bedroom , I had no problem s with adm ission, they did not ask m e
anyt hing ( I ara) .
Regar din g car e, dat a ex pr ess t h at , in t h e user s’ opinion, car e m ust go beyond t he pr ocedur e and it is to take into account the hum an essence and t o value t heir m ost essent ial needs. The at t it udes of care givers, according t o t he st at em ent s, m ust have t he follow ing char act er ist ics: hum an w ar m t h, car e, love, dedicat ion.
I will put here som ething I want to say, because there
are m any people who think hospitals are cold places, that people
are working there, taking care of people j ust because its their
obligation, and what I saw there was com pletely different, I saw
t her e, hum ane people t ak ing car e of hum an beings, w it h
tenderness, love, you know, I was touched to see people there
getting paid to perform a job, but they are not there just to do the
j ob out of obligation, I saw tenderness, dedication of the nurses
taking care of patients ( I ara) .
As w e can see, r espect t o t he ot her w er e im p or t an t in t h e sat isf act ion of car e, b ecau se it rescues hum anizat ion and do not appear as rej ect ion t o t h e t ech n ical aspect s bu t r at h er as a cr eat iv e, intuitive, and affective way that form the professional side of nursing, reinforcing the definition that nursing is a career that integrates science and art in the care of hum an beings( 14).
This at t it ude requires a reflexive process on t h e v alu es an d p r in cip les t h at g u id e p r of ession al pr act ice, assu m in g besides t r eat m en t , pr oper an d welcom ing care, a new et hical post ure
Care was also relat ed t o gender in nursing, as we could see.
I was very well treated, I loved the girls and the boys,
but I will confess som ething, in m y opinion, wom en take better
The pr act ice of car e in nur sing has alw ay s been relat ed t o t he fem ale figure and t his issue, in the institution, is still m ore present due to the presence of religious people in t he hospit al, which brings back t h eir v ocat ion f or n u r sin g, gu ided by t h e ideal of ser v in g.
Th e p r o c e s s , r e p r e se n t e d b y t h e subcat egor y w or k pr ocess, w as designed fr om t he analysis of dat a obt ained by t he st at em ent s of users in the groups and by participative observation, and it m a y b e sa i d t h a t t h e l a t e r w a s a n i m p o r t a n t assessm ent t ool t hat enabled t o learn how work was organized in the institution, being a reference to base t h e i n f o r m a t i o n b r o u g h t b y u se r s, t o e st a b l i sh com parisons, and t o m ake a crit ical reflect ion on t he concret e realit y of t he em pirical field.
Th u s, it w as p ossib le t o lear n t h at w or k organizat ion follows t he funct ional m odel of scient ific approach of m anagem ent, in a hegem onic and rational work concept ion. Work is not perform ed as a t eam ; each pr ofessional is r esponsible for t heir act iv it ies. Work is broken and it loses it s art iculat ion wit h t he work process, represented by a set of routine practices that are repetitive and m echanical. I t occurs so as to ensure m edical act ivit y and det erm ines t he relat ion of power and authority of physicians towards the other pr ofessionals.
I n addit ion t o t his t echnical div ision of t he nur sing t eam , t her e is t he div ision of t he w or k of nur ses in m anagem ent and car e funct ions, and as there is one nurse for each work shift in the Unit, this occurs basically regarding t he m anagem ent funct ion, w her e t hey coor dinat e t he w or k per for m ed by t he n u r si n g t e a m a n d d i v i d e s t h e m se l v e s b e t w e e n list ening t o t he m edical orders and passing t hem on t o t he nurse assist ant s and t echnicians.
Mo st n u r si n g r eco r d s ar e d o n e b y n u r se assist ant s and t echnicians; and sy st em at izat ion of nursing has yet to be introduced on the unit. Guidelines and r out ines ar e st andar dized on a nur sing guide. Working under these characteristics and with overload cannot offer conditions to perform their work in a m ore hum ane w ay.
Wor k er s, t h em selv es, f r equ en t ly com plain about t he working condit ions, as we can see in t he st at em ent of one of t he nursing t echnicians sharing his feelings.
There are tim es you are seeing a user or giving the
m edication and there is another patient’s relative asking you to
change the patient, it is so m uch work, that you do not know what
t o do, som et im es I t hink I ’ll get crazy, because if t here is
som et h in g left for t h e n igh t sh ift , t h e w or k er s com plain ,
som etim es, I leave m y j ob so nervous that I cannot sleep at
night because I ’m t ired and worried.
Sh or t age of per sonn el, and w or k ov er load were noticed by users and pointed out in the groups, as we could see.
There is no doubt I was very well treated, the nurses
were skilled and helpful, but I but there was a sm all num ber of
nurses for t he am ount of pat ient s, I t hink t hey share t here 4
bedroom s for each 2 of them , so they have no tim e left for them ,
they get exhausted, som etim es it is tim e for m edications, after a
short while it is in that hurry again, som etim es they leave som e
things undone ( Ronaldo) .
Anot her im port ant aspect w ort h m ent ioning is t he lack of flexibilit y in t he nursing rout ine. I n all hospit al environm ent , nursing act ions are driven by routine that are generally strict m aking it m ore difficult for users to adj ust to this context.
Then you go with all that difficulty take a shower, then
you get an electric shock, there is lot of cold water, it is too m uch,
you’ll get a bad cold because it’s cold, then the “ nurse” com es and
says good m orning, when she says that “ good m orning” (Fabrício).
I t w as also not iced t hat t he subj ect s could i d e n t i f y, a m o n g h e a l t h p r o f e ssi o n a l s, f i r st t h e phy sicians and t he nur sing t eam . I n t heir opinion, m e d i ca l ca r e w a s co n si d e r e d sa t i sf a ct o r y unanim ously, highlight ing t he punct ualit y of care as an im port ant fact or.
Medical care was very good the physician is good; she
would go in t he m orning and in t he night t o see m e ( Ana) .
I liked m y doct or’s punct ualit y very m uch, every day
at seven, seven thirty, he would go there to check on m e, he did
not m iss one day, he was one of the first to com e all days ( Natal) .
Re g a r d i n g n u r si n g ca r e , p a r t i ci p a n t s d em on st r at ed som e d isin f or m at ion an d con f u sion regarding Professional cat egory. When t hey referred t o t h e n u r se , a ct u a l l y t h e y w e r e r e f e r r i n g t o professionals who had finished high school.
There were the nurses, the father, and the nun too (Natal).
There is the standard nurse that takes care of the nursing
area, the nuns that com e and check if we need anything (Naldo).
These st at em ent s enabled t o suppose t hat t his sit uat ion m ay occur because nurses do not t ake t heir space as t herapy agent s, and because t hey do not place users as t he cent er for t heir approach.
St ill in t he process cat egory, assessm ent of t he t reat m ent was considered posit ive.
The care I received was excellent, m y doctor checked
For m e it was very good, I was very well treated, the
doctor would go there twice or three tim es a day to visit m e, I
have not hing t o com plain about ( Álvaro) .
Medications were good, I im proved ( Márcio)
The out com e of health services is the effect of the program s and interventions on the users’ health and, according t o t he st at em ent s of t he subj ect s in t he group, it was possible t o see t hat m ost of t hem were sat isfied wit h t he out com es of care.
I can sum up t his way, I was adm it t ed, underwent
treatm ent, it was great, I left, I have nothing to com plain about,
I reached m y goal ( Fabrício) .
I was satisfied because I was taken here, and I left
walking. I am still in pain, but that is how it is, it is not healed,
it will be good j ust in October when winter is over ( Jair) .
Users w ere also sat isfied w it h t he speed of resolut eness in healt h act ions
I w a s p l ea sed w i t h a d m i ssi o n b eca u se a l l m y
exam inations were advanced (Márcio).
When you are adm it t ed, t hen all exam inat ions are
conducted, but when you schedule them it takes two, three m onths
and then another two, three m onths to look for them , I don’t know
why that occurs if it is ready, why t aking so long t o look for an
X-Ray, two, three m onths ( Álvaro) .
Or g an izat ion of SUS r eq u ir es con t r ol an d assessm en t o f h eal t h car e d ep ar t m en t s t h r o u g h m o n i t o r i n g o f m e d i ca l a p p o i n t m e n t s a n d t h e p e r f o r m a n ce o f co m p l e m e n t a r y a n d l a b o r a t o r y e x a m i n a t i o n s, a ssu r i n g n e ce ssa r y q u a l i t y a n d resolut eness for adequat e work of healt h services( 15).
These statem ents, however, dem onstrate that t he public depart m ent s of t he cit y are not organized t o pr ov ide fast and r esolut e healt h ser v ices t o t he
population, and adm ission was used in som e cases to speed up t he exam inat ions.
FI NAL CONSI DERATI ONS
We h a v e l e a r n e d , b y t h e p a r t i ci p a n t s’ st at em ent s, t hat t hey hav e point ed out significant elem ents that expressed their satisfaction with health care received during adm ission and t hat showed t he qualit y of car e, t hus dem onst r at ing t he cor r elat ion bet ween sat isfact ion and qualit y.
However, t he out com es obt ained lead t o t he conclusion that users’ practice very little their rights to be cared for in public services, placing t hem selves in a subm issive position as if they were receiving a favor and not perform ing their right to health. Putting care in a broader perspect iv e, led t he researcher, from her experience as an observer of t he em pirical field, t o consider t hat the organizat ion of t he work process in the hospital, does not aim at reaching quality of care. To m anage a health service aim ing at quality of h ealt h act ion s r eq u ir es ch an g in g t h e f ocu s of at t ent ion from t he disease t o t he healt h product ion focusing on t he subj ect , t he work cannot be broken up, individualized, and hegem onic. The hospit al does not follow the considerations of the 9t h National Health
Conference, which advocat es healt h care m odels not to be lim ited to individual and healing care, but rather t o develop pr ogr am s t hat aim at gr oup w or ks, and act ions on healt h educat ion, cont inuous per sonnel educat ion, and ensuring favorable working condit ions t o all healt h professionals.
REFERENCES
1. Feldm an LB, Cunha I CKO. I dent ificação dos cr it ér ios de av aliação d e r esu lt ad os d o ser v iço d e en f er m ag em n os p r o g r a m a s d e a cr e d i t a çã o h o sp i t a l a r. Re v La t i n o - a m Enfer m agem 2006 j ulho- agost o; 14( 4) : 540- 5.
2 . Fer r eir a ABH. Dicion ár io da lín gu a por t u gu esa. Rio de Janeiro ( RJ) : Nova Front eira; 1977.
3. Sant os PS. Avaliação dos serviços públicos de at enção à saú d e d a cr ian ça sob a ót ica d o u su ár io. [ d isser t ação] . Salvador ( BA) : Universidade Federal da Bahia; 1995. 4 . Ca d a h C. Av a l i a çã o d a q u a l i d a d e d a a ssi st ên ci a d e e n f e r m a g e m so b a ó t i ca d a sa t i sf a çã o d o s p a ci e n t e s. [ dissert ação] . São Paulo ( SP) : Escola de Enferm agem / USP; 2 0 0 0 .
5 . D o n ab ed i an A. Th e m et h o d s an d f i n d i n g s o f q u al i t y assessm ent and m onit oring: an illust rat ed analysis. Ann Arbor ( MI ) : Healt h Adm inist r at ion Pr ess; 1985.
6. Car v alho MA. I ndicador es de av aliação de desem penho em est ab elecim en t os assist en ciais d e saú d e. I n : Fór u m Perm anent e e I nt erdisciplinar de Saúde; 2003 novem bro 18; Cam pinas; Br asil; 2003.
7 . Ma t su d a LM. Sa t i sf a çã o p r o f i ssi o n a l d a e q u i p e d e enfer m agem de um a UTI - adult o: per spect iv as de gest ão para a qualidade. [ dout orado] . Ribeirão Pret o ( SP) : Escola de Enferm agem de Ribeirão Pret o/ USP; 2000.
8. Motta PR. Desem penho em equipes de saúde. Rio de Janeiro ( RJ) : FGV; 2001.
9. Olm st ed MS. O pequeno gr upo social. São Paulo ( SP) : Her d er / EDUSP; 1 9 7 0 .
1 0 . Dall´ Ag n ol CM, Ciam p on e MHT. Gr u p os f ocais com o est r at égia m et odológica e pesquisas na enfer m agem . Rev Gaúch Enfer m agem 1999 j aneir o; 20( 1) : 5- 25.
1 2 . Go m e s R, So u za ER, Mi n a y o MCS. Or g a n i za çã o , processam ent o, análise e int erpret ação de dados: o desafio d a t r i an g u l ação. I n : Mi n ay o MCS, Assi s SG, Sou za ER, or ganizador es. Avaliação por t r iangulação de m ét odos. Rio de Janeiro ( RJ) : Fiocruz; 2005. p. 185- 222.
1 3 . Mi n i st é r i o d a Sa ú d e ( BR) . Pr o g r a m a n a ci o n a l d e h u m a n i za çã o d a a ssi st ê n ci a h o sp i t a l a r. Br a síl i a ( D F) : Secret aria da Saúde; 2001.
14. Waldow VR. Cuidado hum ano: o resgat e necessário. 2ª ed. Port o Alegre ( RS) : Sagra Luzzat o; 1999.
1 5 . Mi n i st é r i o d a Sa ú d e ( BR) . Re l a t ó r i o f i n a l d a 1 1 ª Con f er ên cia Nacion al d e Saú d e; 2 0 0 0 . d ezem b r o 1 5 - 1 9 ; Brasília; Brasil. São Paulo ( SP) : Conselho Nacional de Saúde; 2 0 0 0 .