Arq Neuropsiquiat r 2002;60(4):909-911
NUM BER AND VIABILITY OF PARASITE INFLUENCE
SEIZURE FREQUENCY IN CHILDREN WITH
NEUROCYSTICERCOSIS
Lisiane S. Ferreira
1, Li M in Li
2, Verônica A. Zanardi*
2, M arilisa M . Guerreiro
2ABSTRACT - We invest igat ed t he relat ionship bet w een CT findings - number and t he viabilit y phase of t he parasites - and the seizure frequency in children w ith neurocysticercosis before and short-term after antiepileptic drug (AED) int roduct ion. We only found a significant int eract ion bet w een st age of parasit ic infect ion and number of lesions on seizure frequency aft er AED t reat ment . Pat ient s w it h more t han five lesions on act ive or t ransit ional st ages had higher seizure frequency predict ing a w orse short -t erm prognosis.
KEY WORDS: neurocyst icercosis, epilepsy, childhood.
Número e viabilidade do parasita influenciam a frequência de crises epilépticas em crianças com neurocisticercose
RESUM O - No present e est udo, invest igou-se a relação ent re os achados t omográficos – número e est ágio de viabilidade dos parasit as – e a frequência de crises epilépt icas em crianças com neurocist icercose ant es e logo após a int rodução do t rat ament o com drogas ant iepilépt icas. Encont ramos que a int eração ent re o est ágio do parasita e o número de lesões influenciam significativamente a frequência de crises somente após o tratamento. Pacient es com mais do que cinco lesões em fase at iva ou t ransicional t iveram maior frequência de crises predizendo um pior prognóst ico.
PALAVRAS-CHAVE: neurocist icercose, epilepsia, infância.
Depart ament os de Neurologia e * Radiologia, Universidade Est adual de Campinas (UNICAM P), Campinas SP, Brasil: 1Pós-graduanda; 2Professor Dout or.
Received 22 M arch 2002, received in final form 1 July 2002. Accept ed 15 July 2002.
Dra. M arilisa M . Guerreiro - Depart ament o de Neurologia – FCM /UNICAM P - Caixa Post al 6111 - 13083-970 Campinas SP - Brasil. E-mail: mmg@f cm.unicamp.br
Neurocyst icercosis (NC) is a main healt h problem in developing count ries. It affect s pat ient s of all ages and it is endemic among children as w ell as adult s in Lat in America1. It is also becoming increasingly
common in developed count ries due t o migrat ion of carriers from endemic areas.
Epilept ic m anif est at ions appear t o depend on number and localizat ion of t he cyst s2. Nevert heless,
some aut hors have not found any difference in sei-zure frequency or in clinical charact erist ics bet w een pat ient s w it h a single and mult iple lesions3.
The object ive of t his st udy w as t o invest igat e t he relat ionship bet w een CT findings - number and t he viabilit y phase of t he parasit es - and t he seizure fre-quency in children w it h NC.
M ETHOD
This is a hist oric cohort st udy. We select ed 28 epilept ic pat ient s less t han 16 years w it h probable or definit ive diag-nosis of NC according t o Del Brut o et al.4. Sixt een w ere
girls, t he mean age w as 7.2 years, and t he mean follow -up w as 64.5 mont hs. All pat ient s had parenchymal form of NC and normal neurological examinat ion.
We obtained all information on the 28 patients on revi-sion of their medical records, complemented w ith direct interview w ith patients and guardians w henever possible.
A semi-structured protocol w as filled in for every patient, considering: seizure frequency before AED introduction (to-tal number of seizures w as classified5 as: 1-3 per year = 5;
4-11 per year = 6; 3 per month = 7; 6 per w eek = 8; 1-3 per day = 9; 4-10 per day = 10; > 10 per day = 11); and, seizure frequency after AED introduction (seizure-free = 1, plus same classification as above).
The prot ocol and t he informed consent w ere approved by t he et hical commit t ee of our universit y hospit al.
910 Arq Neuropsiquiat r 2002;60(4)
(calcified lesions on CT) based on t he viabilit y of t he para-sit e as proposed by Carpio et al.6. When lesions in different
st ages w ere found in t he same pat ient , t hey w ere classified according t o t he most act ive lesion det ect ed (act ive > t ransit ional > inact ive). Lesions on CT w ere grouped in different cat egories: number (= 5, > 5) and st age (act ive plus t ransit ional and inact ive).
We used mult ivariat e analysis of variance (M ANOVA) and simple main effect and post -hoc pairw ise comparison in order t o assess w het her t he st age of parasit ic infect ion (act ive-t ransit ional and inact ive) and t he number of lesions (= 5 and > 5 lesions) might have main or int eract ive effect on seizure f requency bef ore and short -t erm af t er AED t reat ment.
RESULTS
Concerning the evolutionary stage of the parasite, 17 pat ient s w ere at inact ive phase, six at t ransit ional phase and five children had act ive lesions on CT. Re-garding number of lesions, 18 pat ient s had five or less, and 10 pat ient s had more t han five lesions.
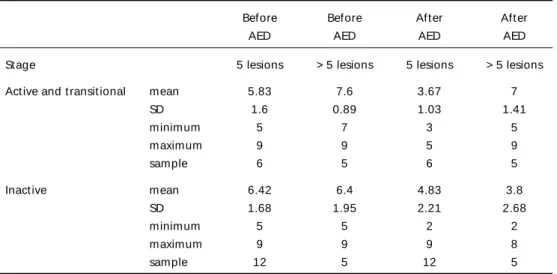
Seizure f requency bef ore and short -t erm af t er AED is show n in Table 1.
M ult ivariat e ANOVA show ed t hat t he seizure fre-quency before AED t reat ment w as not significant ly af f ect ed b y t h e st ag e o f p ar asi t i c i n f ect i o n [F(1,27)= 0.23, p= 0.638] or t he number of lesions [F(1,27)= 1.82,p= 0.19], or interaction betw een stage o f p ar asi t i c i n f ect i o n an d n u m b er o f l esi o n s [F(1,27)= 1.89, p= 0.182].
M ult ivariat e ANOVA show ed t hat short -t erm sei-zure frequency aft er t he AED t reat ment w as not sig-nificant ly affect ed by t he st age of parasit ic infect ion [F(1,27)= 1.59, p= 0.219] or t he number of lesions [F(1,27)= 2.04,p= 0.166]. How ever, there w as a
signi-ficant interaction betw een stage of parasitic infection and number of lesions [F(1,27)= 7.35, p= 0.012]. Sim-ple main effect analysis, seeking the significant factor in t he int eract ion bet w een t he st age of parasit ic infection and number of lesions on seizure frequency, show ed t hat t he st age of parasit ic infect ion had no sig nif icant ef f ect on p at ient s w it h = 5 lesions [F(1,24)= 1.05, p= 0.315], but had a significant effect on patients w ith > 5 lesions [F(1,24)= 7.89, p= 0.009]. Simple main effect analysis of number of lesions w ith respect to the seizure frequency from different stage of t he parasit ic infect ion show ed t hat number of lesions had significant effect on patients w ith active-transitional stage of parasitic infection [F(1,24)= 8.56, p= 0.007], but not on patients w ith inactive stage of parasitic infection [F(1,24)= 0.82, p= 0.373].
DISCUSSION
Neuroimaging has attained enormous progress du-ring last decade. Despite that, CT is very helpful in NC because it is a safe, precise and noninvasive method w it h more t han 95% accuracy t o def ine number, localization and evolutionary stage of the parasite, especially in the parenchymal form of the disease7. In
developing count ries w here M RI machines are not alw ays available, and considering t he f act t hat calcifications are the main radiological finding in NC, CT is still the most performed and useful examination. Epilepsy is t he most common clinical manifes-t amanifes-t ion in NC. Imanifes-t occurs in 70-90% of all children w imanifes-t h t he parenchymal form of t he disease, usually being it s primary present at ion7,8. The pat hophysiology of
t he seizures due t o NC is not complet ely underst ood
Table 1. Seizure f requency bef ore and short -t erm af t er AED.
Before Before Aft er Aft er
AED AED AED AED
St age 5 lesions > 5 lesions 5 lesions > 5 lesions
Act ive and t ransit ional mean 5.83 7.6 3.67 7
SD 1.6 0.89 1.03 1.41
minimum 5 7 3 5
maximum 9 9 5 9
sample 6 5 6 5
Inact ive mean 6.42 6.4 4.83 3.8
SD 1.68 1.95 2.21 2.68
minimum 5 5 2 2
maximum 9 9 9 8
sample 12 5 12 5
Arq Neuropsiquiat r 2002;60(4) 911
yet . In act ive and t ransit ional forms, seizures may be t he consequence of compression or inflammat ory react ion. In inact ive f orm , perilesional gliosis is probably t he cause of t he seizures. Chronic inflam-mat ory react ion somet imes t akes several years t o di-sappear and it may have an import ant role in t he pat hophysiology of focal epilepsy in NC9,10.
Parenchymal NC is the most frequent form in chil-dren7. In this age group, the disease behaves
differen-tly from adults in several aspects, w hich have impor-tant implications in diagnosis, management and prog-nosis. Massive infestation and multiple lesions, for exam-ple, occur more frequently in children than adults2.
In t his st udy, w e demonst rat ed t hat t here w as an int eract ion bet w een number and viabilit y of t he pa-rasit es on seizure frequency aft er AED int roduct ion. Our dat a show ed t hat pat ient s w it h > 5 lesions in act ive and t ransit ional st ages had higher seizure fre-quency aft er AED int roduct ion, predict ing a w orse prognosis. The explanat ion may be t hat NC in chil-dren has a peculiar behavior. A massive infest at ion by t he eggs of Taenia solium, w hich develop t o viable
cyst s represent ing t he larval form of t he disease, may occur in t his age group. For a variable period of t ime t hese cyst s remain unchanged and exhibit a st at e of immune t olerance w it h t he host . Pat ient s may have
seizures, or may remain asympt omat ic. Event ually t he cyst s die and dying cyst s have a much great er likelihood of being sym pt om at ic9. Dying cyst s at
dif f erent t im es m ay cause successive periods of exacerbat ion of sympt oms. This is a dynamic process t hat may t ake years t o resolve complet ely and may lead t o recurrence of seizures.
REFERENCES
1. White AC Jr. Neurocysticercosis: a major cause of neurological disease worldwide. Clin Infect Dis 1997;101-115.
2. Sotelo J, Del Bruto OH. Brain cysticercosis: review article. Arch Med Res 2000;31:3-14.
3. M o nteiro L, N unes B, M end o nça D. Sp ectrum o f ep ilep sy in neurocysticercosis: a long term follow up of 143 patients. Acta Neurol Scand 1995;92:33-40.
4. Del Bruto OH, Wadia NH, Dumas M, Tsang VCW, Schantz P.M. Proposal of diagnostic criteria for human cysticercosis and neurocys-ticercosis. J Neurol Sci 1996;142:1-6.
5. Engel J Jr, Van Ness PC, Rasmussen TB, Ojemann LM. Outcome with respect to epileptic seizures In: Engel J Jr, (Ed.) Surgical treatment of the Epilepsies, 2.Ed. New York: Raven Press, 1993:609-621. 6. Carpio A, Marcelo P, Santillan F, Alfonso E. A proposal for classification
of neurocysticercosis. CanJ Neurol Sci 1994;21:43-47.
7. Garcia MR, Astiazarán AG, Franco FR. Neurocysticercosis in children: clinical experience in 122 patients. Child’s Nerv Syst 1997;13:608-612. 8. Bittencourt PRM, Adamolekum B, Bharucha N,et al. Epilepsy in tropics: II. Clinical presentations, pathophisiology, immunologic diagnosis, economics, and therapy. Epilepsia 1996;37:1128-1137.
9. Carpio A, Escobar A, Hauser WA. Cysticercosis and epilepsy: a critical review. Epilepsia 1998;39:1025-1040.