Effect of different ferrule designs on the fracture
resistance and failure pattern of endodontically
ceramic crowns
Haneef SHERFUDHIN1, Joseph HOBEICH2, Carlos Augusto CARVALHO3, Moustafa N. ABOUSHELIB4, Walid SADIG5,
Ziad SALAMEH6
1- BDS, MDS, Assistant Professor, Department of Prosthetic Dental Sciences, College of Dentistry, King Saud University, Riyadh, Saudi Arabia. 2- DUA, DSc, Assistant Professor, Department of Fixed Prosthodontics and Occlusion, Saint Joseph University, Beirut, Lebanon.
3- DDS, MSc, PhD student, Department of Operative Dentistry, Endodontics and Dental Material, University of São Paulo, Bauru School of Dentistry, Bauru, SP, Brazil; and PhD student, Department of Fixed Prosthodontics and Dental Materials, Policlinico Le Scotte, University of Siena, Italy.
4- DDS, MSc, PhD, Dental Biomaterials Department, Faculty of Dentistry, Alexandria University, Egypt.
BDS, MSc, Professor, Department of Prosthetic Dental Sciences, College of Dentistry,King Saud University,Riyadh, Saudi Arabia.
6- DDS, MSc, PhD, Assistant Professor/Researcher,Eng.A.B Research Chair for Growth Factors and Bone Regeneration, King Saud University, Riyadh, Saudi Arabia; Research Department, School of Dentistry, Lebanese University, Beirut, Lebanon.
Corresponding address: Carlos Augusto Carvalho - Julia Miranda 18 - 36.400-000 - Conselheiro Lafaiete - Minas Gerais - Brasil - Phone: +55 31 37633077 - Fax: +55 31 37637070 - e-mail: [email protected]
!
ABSTRACT
O
bjective: This study investigated the effect of different ferrule heights on endodontically ! ! "# Ivoclar-Vivadent) luted with self-polymerized resin cement (Multilink, Ivoclar Vivadent) while the coronal section was restored with hybrid composite core build-up material (Tetric Ceram, Ivoclar-Vivadent), which received all-ceramic crown. Different ferrule heights were investigated: 1-mm circumferential ferrule without post and core (group 1 used as control), a circumferential 1-mm ferrule (group 2), non-uniform ferrule 2-mm buccally and 1-mm lingually (group 3), non-uniform ferrule 3-mm buccally and 2-mm lingually (group 4), and $%&' groups were investigated by applying axial load to the ceramic crowns (n=10). Data were analyzed statistically by one-way ANOVA and Tukey’s post-hoc test was used for pair-wisecomparisons (D*++%& ' $ $
load of all tested groups (P<0.780). The control group had the lowest fracture resistance (891.43±202.22 N) and the highest catastrophic failure rate (P<0.05). Compared to the $/ $ $ $ 6 specimens. Conclusions: Within the limitations of this study, increasing the ferrule length 6 $ ; $ of these restorations under function.
INTRODUCTION
Endodontically treated teeth often loose substantial tooth structure from previous caries, pre-existing restorations, and/or endodontic treatment18, which reduce tooth bulk and thickness of healthy dentin resulting in increased chances of fracture under function8. Controversy exists as to whether endodontic procedures are the primary cause for loss of strength. Panitvisai and
Messer23 (1995) 6
increased with increasing the extension of cavity preparations and was greatest when endodontic access was incorporated into a preparation. It has been reported that endodontically treated teeth and their contralateral vital pairs exhibited similar biomechanical properties, such as punch shear strength, toughness, and load required for fracture28.
Although the insertion of a post does not strengthen or reinforce endodontically treated
teeth11,12/ ?
retention of the core material which in turn is used @ 15. For the inserted post to perform its function, several variables must be put into consideration such as post length, diameter, geometric design, and surface configuration15. Additionally, special attention should be given to the material the post is made of in order to ensure adequate distribution of the absorbed stresses and to prevent root fracture during29. Regarding with consideration to the well-known success of metallic posts there are now many concerns regarding the associated inhomogeneous stress distribution, biological side effects due to microleakage and /6B an all-ceramic restorations5.
' composite (FRC) posts helped improving stress distribution because their elastic modulus is similar to that of dentin as indicated by several clinical and laboratory studies10,17,33. FRC post systems showed more frequent favorable failure modes than did metal post systems11,14 G$ posts proved effective in withstanding compressive loads in posterior teeth1, they behave differently in anterior teeth where non-axial biting forces ?6@? more effective27. Recent studies15-30 suggested that $ and strengthening of endodontically treated teeth under full coverage crowns.
A ferrule or encircling band of cast metal around the remaining coronal surface can provide protective reinforcement to endodontically treated teeth by encapsulation of the remaining coronal structure and by resisting functional lever forces during mastication. A minimum 1 to 2 mm of ferrule
height is necessary to achieve such protective effect20. Recent clinical studies reported that the ? 6 clinical success rate of endodontically treated events were due mainly to post debonding3,9. An in vitro study reported that incomplete crown ferrule was associated with greater variation in load capacity after chewing simulation19, while other studies found no effect of different ferrule heights in
6,22,24.
The aim of this study was to evaluate the fracture resistance and failure pattern of endodontically treated mandibular premolars restored with $ posts and all-ceramic crowns. The null hypothesis was that different ferrule heights do not improve the fracture resistance or the failure pattern of the tested restorations.
MATERIAL AND METHODS
Preparation of specimens
extracted for orthodontic reasons. All external debris were removed with an ultrasonic scaler, and @ #+@$ verify the absence of cracks, defects and dental caries. Teeth were stored in a 0.5% chloramine T (Prolabo, Paris, France) in saline solution. Buccolingual and mesiodistal coronal dimensions plus root length of all selected teeth were measured using a digital caliper (Digimatic Calipers, Mitsutoyo, Tokyo, Japan) and only teeth with the following mean dimensions were selected: 14.1 mm root length, 7.3 mm buccolingual width, and 4.9 mm mesiodistal width.
Standardized root canal preparations were made using the following procedure: initial probing using #+ Q @ / / U$ / Switzerland); the root canal length was established $ ? @$ from the apical foramen. The specimens were then prepared endodontically with a stepback procedure with size 45 (Flex R file; Union Broach, York PA). After intermittent rinsing with 2.5% sodium hypochlorite solution, the endodontic treatment was completed using manual lateral condensation method (AH Plus, Dentsply, De Tray, Konstanz, Germany).
embedded along their long axis using a surveyor (Ney Surveyor; Dentsply).
Full crown preparation
The teeth were randomly divided into 5 groups of 10 teeth each. Crown margins were prepared under constant water cooling and using 2.5x optical loops. A new diamond point (Lot-NR 1599, DFS Dental and Technical Products, GmbH, Germany) was attached to the milling machine (K9 Milling Apparatus-990, Kavo, Germany) for every group. The MRD gauged diamond had a self-limiting tip, which produced a 1-mm-deep chamfer and the margins and the angle of convergence were standardized.
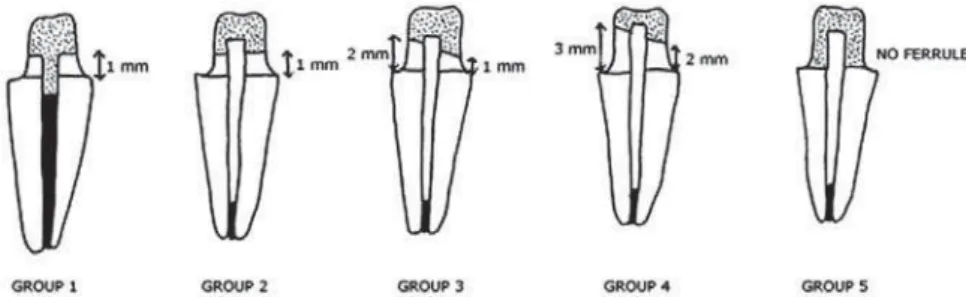
G / @ $$ 1): Group 1 (control): 1 mm circumferential ferrule $$?$ _` {# resin core; Group 3: non-uniform ferrule height (2 #$& and resin core; Group 4: a non-uniform ferrule height (3 mm buccally and 2 mm lingually) with _ ` % ?
Post-space preparation
In the control group, excess gutta-percha was removed to a depth of 2 mm from the coronal surface of the preparation, using a carbide bur (171L-012, Brasseler, USA). The coronal walls were etched with 36% phosphoric acid (Total Etch, Ivoclar-Vivadent, Schaan, Liechtenstein) for 15 s, washed with water spray and then gently air-dried. One coat of adhesive resin (Excite, Ivoclar-Vivadent) was applied using a microbrush and light polymerized for 20 s (Astralis 10, Ivoclar-Vivadent). A hybrid composite resin (Tetric Ceram, Ivoclar-Vivadent) was applied and light polymerized for 40 s.
For the remaining groups, post space was created using no. 1 Peeso reamer (Union Broach Co., Long Island, NY, USA) and corresponding calibrating drill ! ! /"#/;?|?&?$} mm of apical gutta-percha intact. A translucent $ ! ! "# ;?|?/ ~/ & was used. Each post was cut to a suitable length
with a diamond bur so that it was covered with at least 2 mm of resin composite occlusally.
Post cementation was carried out with self-polymerized resin cement (Multilink, Ivoclar Vivadent) following manufacturer’s instructions. Silane coupling agent (Monobond-S, Ivoclar-Vivadent) was applied on the post surface for 60 s and then air-dried. After post cementation, the surrounding dentin surface was etched with 36% phosphoric acid (Total Etch, Ivoclar-Vivadent) for 15 s, washed with water spray and gently air-dried. One coat of adhesive resin (Excite, Ivoclar-Vivadent) was applied using a microbrush and light polymerized for 20 s (Astralis 10, Ivoclar-Vivadent). Then core build-up was performed using hybrid composite resin (Tetric Ceram, Ivoclar-Vivadent) in 1-mm-thick increments and light polymerized (Astralis 10; Ivocar-Vivadent) for 40 s until the core was restored to predetermined dimensions. ' $ matrix to allow for shape consistency between specimens. The dimensions of the prepared cores $ +@$ %
A single-phase impression was made using poly-vinylsiloxane impression material (Virtual, Ivoclar-Vivadent) and master dies were fabricated with type 4 die stone (Jad Stone, Whip Mix, Louisville, Kentucky, USA). A press ceramic (e max, A3, Ivoclar-Vivadent) was selected to fabricate all-ceramic crowns of the restored specimens. Crown dimensions were standardized by using a mold for the external shape of each specimen. The $ 6;!~$$/;? Vivadent) for 20 s, rinsed off, air dried, silanized for 60 s and air dried. Dentine primer liquids were mixed and applied on the whole prepared tooth surface for 15 s. Resin cement was dispensed from the automix syringe directly into the inner surface of the crowns which were seated and held in position @{+_@ ? immediately with a micro brush. Exposed margins were covered with glycerin gel and rinsed off after complete polymerization of the resin cement. The specimens were stored in distilled water at 37°C for 7 days prior to testing.
Fracture resistance
All specimens were subjected to cyclic loading according to the following regime: sinusoidal load between 50 and 200 N at a rate of 2 hertz. All specimens received 15,000 cycles and surface damage was prevented by insertion of a 0.5 mm silicon sheet between the occlusal surface of the ceramic crown and the loading indenter (3 mm diameter) of the pneumatically activated loading machine. After completion of cyclic loading, a universal testing machine (Instron 8500 Plus, Instron, 100 Royal St. Canton, MA, USA) was used to deliver a compressive load to the specimens at a crosshead speed of 1 mm/min at 45 degree angle to the long axis of the teeth (root apex tilted lingually) until failure. Load-time curves were recorded using a universal testing machine’s computer software. The load was measured in Newton. The failure load of the specimen was determined when the force-versus-time graph showed an abrupt change in load, indicating a sudden decrease in the specimen’s resistance to compressive loading.
After loading, the failure mode recorded for each ? above the cement-enamel junction (repairable) or catastrophic fracture of the root below cement-enamel junction (non repairable). These inspections were made using a stereomicroscope (Stereoscopic zoom microscope, SMZ-1000, Nikon, Japan) and during inspection, the teeth were trans-illuminated with a fiber optic cable. Complete or partial debonding of the crown or of the post and core were also considered as favorable failure modes. Data were analyzed statistically by one-way ANOVA and Tukey’s post-hoc test was used for pair-wise comparisons (D=0.05).
RESULTS
All specimens survived the cyclic loading program without any sign of external failure. Statistical ? $ the failure load of the tested groups and the control group restored without fiber post (P<0.780). Although fracture resistance of the control group
was comparable to that of the other groups that ? / $ failure rate (70%) in the control specimens in the form of vertical root fracture. The groups restored / / complete favorable fracture in the form of cervical fracture above the cervical line, previous data are summarized in Table 1.
In all specimens, the cemented ceramic crown was fractured without evidence of debonding of either the crown or the cemented post. The internal surface of the fractured ceramic fragments demonstrated evidence of resin cement and part of the core material indicating cohesive fracture of the resin core.
DISCUSSION
Considering the results obtained in this study, different ferrule heights did not improve the fracture resistance or the failure pattern of the tested specimens. On the other hand, the use of of dentin changed the catastrophic failure type of the control group to almost complete favorable fracture for the other four groups. The proposed hypothesis was thus accepted. The dynamic cyclic loading program was intended to quickly screen any possible weakness in the cemented restorations. Providing occlusal protection prevented generation of cone cracks in the brittle ceramic crowns which was the reason why all specimens survived without failure. Longer periods of cyclic loading are required to shed light on the long-term performance of these restorations, but investigating this issue was not within the scope of this study7.
The results of the fracture resistance test showed that the amount of residual coronal structure (ferrule height) did not increase significantly the fracture resistance of endodontically treated teeth. These results are in agreement with those of previous studies2,6,22; while contrary results were reported by other authors25,34. This could be @ the forces and distributed the loading stresses over Group Failure load (N) Number of favorable fracture Number of catastrophic fracture
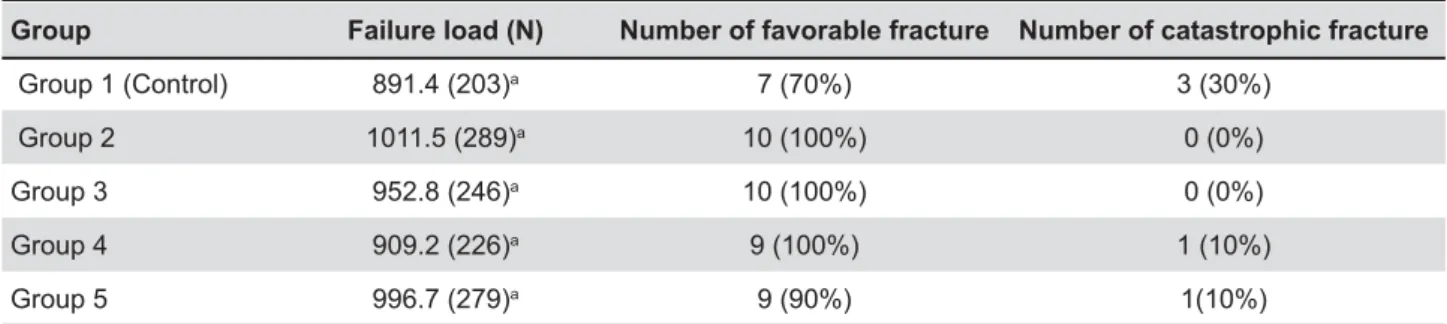
Group 1 (Control) 891.4 (203)a 7 (70%) 3 (30%)
Group 2 1011.5 (289)a 10 (100%) 0 (0%)
Group 3 952.8 (246)a 10 (100%) 0 (0%)
Group 4 909.2 (226)a 9 (100%) 1 (10%)
Group 5 996.7 (279)a 9 (90%) 1(10%)
Table 1- Failure load (standard deviation) and failure type of tested groups
a bigger surface area of the tooth structure similarly for all tested groups7,16. These results may also be resin composite core exerted a reinforcing effect by supporting the remaining tooth structure regardless of the ferrule design6,27. These non-metallic post systems have gained widespread popularity in recent years because of other advantages such as their superior esthetics, ease of retrievability, and simple application technique, which allow the clinician to complete the procedure in a single short appointment6.
According to the results of the present study, $ & revealed higher catastrophic failure rate compared to the other groups, which indicates that insertion of
endodontically treated teeth even if the failure load remains relatively not effected27,30. The presence of a uniform 1-mm-thick coronal structure (group 2) resulted in the highest fracture resistance value, especially when compared to the control group, which is in agreement with the results of previous studies31,32.
A point of clinical relevance is that the fracture resistance of specimens with non-uniform coronal structure (group 3 and 4) was lower than the specimens without a ferrule (group 5), with consideration to maintaining as much as possible of sound tooth structure. It could be advised to adjust the coronal structure evenly to provide a 6 / improve the fracture resistance of endodontically, treated teeth. Further research is needed to fully cover this issue21,26.
Lithia disilicate-based all-ceramic crowns were $ 6@ $}++!&/ $6 acid, readily silanized and bonded with any suitable resin cement. It has also been reported that the mean chewing force of adults ranges between 7 to 15 kg, and the maximum biting force could reach up to 90 kg34. As the fracture loads in all groups in the present study were found to be greater than the ordinary chewing force, and even greater than the maximum biting force, their mechanical strength could be considered satisfactory from a clinical point of view10.
In terms of the failure modes, the obtained results are in accordance with those of previous
studies15,27/ $
posts resulted in more favorable fracture patterns4 while the specimens restored without posts showed a higher incidence of catastrophic failure. It could reinforced post systems offered more homogenous stress distribution due to their modulus of elasticity close to that of dentin resulting in a better
stress distribution that occurs at the post-dentin interface24,34 . This could explain why all favorable fractures were limited to the cervical portion of the root including the core-dentin interface, since the stresses were concentrated in the cervical area and the outer root surface. Supporting this opinion is the cohesive fracture of the resin core material, which remained attached to the fractured segments of ceramic crowns, thus indicating good bond strength between the core build up material and the cemented ceramic crown. The limited number of $ the complexity of functional loads in the oral environment may be some of the shortcomings of the present study. Further investigations including $$ studies are recommended to complement the present study.
CONCLUSION
Within the limitations of this study, it may be concluded that increasing the ferrule length did not improve the fracture resistance of endodontically treated teeth restored with glass ceramic crowns. ; $ of catastrophic failure of these restorations under functional loads.
REFERENCES
1- Akkayan B, Gülmez T. Resistance to fracture of endodontically treated teeth restored with different post systems. J Prosthet Dent. 2002;87:431-7.
2- Al-Hazaimeh N, Gutteridge DL. An in vitro study into the effect of the ferrule preparation on the fracture resistance of crowned teeth incorporating prefabricated post and composite core restorations. Int Endod J. 2001;34:40-6.
3- Cagidiaco MC, García-Godoy F, Vichi A, Grandidni S, Goracci C, ! affects the 3-year survival of endodontically treated premolars. Am J Dent. 2008;21:179-84.
4- Cagidiaco MC, Radovic I, Simonetti M, Tay F, Ferrari M. Clinical teeth: 2-year results. Int J Prosthodont. 2007;20:293-8. % ` / J Am Dent Assoc. 1996;127:1397-8.
6- Dikbas I, Tanalp J, Ozel E, Koksal T, Ersoy M. Evaluation of the effect of different ferrule designs on the fracture resistance of endodontically treated maxillary central incisors incorporating / Dent Pract. 2007;8:62-9.
7- Duret B, Duret F, Reynaud M. Long-life physical property preservation and postendodontic rehabilitation with the Composipost. Compen Contin Educ Dent Suppl. 1996;20:S50-6. 8- Eakle WS, Maxwell EH, Braly BV. Fractures of posterior teeth in adults. J Am Dent Assoc. 1986;112:215-8.
9- Ferrari M, Cagidiaco MC, Grandidni S, De Sanctis M, Goracci C. Post placement affects survival of endodontically treated premolars. J Dent Res. 2007;86:729-34.
11- Fokkinga WA, Kreulen CM, Vallittu PK, Creugers NH. A structured analysis of in vitro failure loads and failure modes of // ;! 2004;17:476-82.
12- Goodacre CJ, Spolnik KJ. The prosthodontic management of endodontically treated teeth; a literature review. Part I. Success and failure data, treatment concepts. J Prosthodont. 1994;3:243-50.
13- Guzy GE, Nicholls JI. In vitro comparison of intact endodontically treated teeth with and without endo-post reinforcement. J Prosthet Dent. 1979;42:39-44.
14- Hayashi M, Takahashi Y, Imazato S, Ebisu S. Fracture resistance of pulpless teeth restored with post-cores and crowns. Dent Mat. 2006:22:477-85.
15- Heydecke G, Butz F, Strub JR. Fracture strength and survival rate of endodontically treated maxillary incisors with approximal cavities restoration with different post and core systems: an in-vitro study. J Dent. 2001;29:427-33.
# ; / U Q/ ? ` ' 6 length and crown ferrule on the resistance to cyclic loading of bovine teeth with prefabricated titanium post. Int J Prosthodont. 1999;12:78-82.
#/`/$ post-resin core unit: a scanning electron microscopy evaluation. Dent Mat. 2004;20:176-83.
18- Nagasiri R, Chitmongkolsuk S. Long-term survival of endodontically treated molars without crown coverage: a retrospective cohort study. J Prosthet Dent. 2005;93:164-70. 19- Naumann M, Preuss A, Rosentritt M. Effect of incomplete crown ferrules on load capacity of endodontically treated maxillary / / ceramic crowns: an in vitro evaluation after chewing simulation. Acta Odontol Scand. 2006;64:31-6.
{+$/GU;/$U/`$$ G/ B Effect of no ferrule on failure of teeth restored with bonded posts and cores. Gen Dent. 2004;52:143-6.
{#$/$U/GU;/`$$ G/ B ;6 $ fracture resistance of restored endodontically treated anterior teeth. J Prosthet Dent. 2006;95:290-6.
22- Oliveira JA, Pereira JR, Lins do Valle A, Zogheib LV. Fracture resistance of endodontically treated teeth with different heights composite resin core by intermittent loading. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;5:52-7.
{!? !/ 6 to endodontic and restorative procedures. J Endod. 1995;21:57-61.
24- Pegoretti A, Fambri L, Zappini G, Bianchetti M. Finite element $ Biomaterials. 2002;23:2667-82.
25- Pierrisnard L, Bohin F, Renault P, Barquins M. Corono-radicular $ element analysis. J Prosthet Dent. 2002;88:442-8.
26- Salameh Z, Ounsi HF, Aboushelib MN, Sadig W, Ferrari M. Fracture resistance and failure patterns of endodontically treated $ with a zirconia-ceramic crown. J Dent. 2008;34:842-6.
27- Salameh Z, Sorrentino R, Ounsi HF, Goracci C, Tashkandi E, Tay F, et al. Effect of different all-ceramic crown system on fracture resistance and failure pattern of endodontically treated maxillary $ 2007;33:848-51.
28- Sedgley CM, Messer HH. Are endodontically treated teeth more brittle? J Endod. 1992;18:332-5.
29- Shillingburg HT, Hobo S, Whitsett L, Jacobi R, Brackett S. Fundamentals of fixed prosthodontics. 3rd ed. Chicago:
Quintessence Publishing; 1997. p.194-209.
30- Sorrentino R, Aversa R, Ferro V, Auriemma T, Zarone F, Ferrari /' stress distributions in endodontically treated maxillary central incisors restored with different post, core and crown materials. Dent Mater. 2007;23:983-93.
31- Sorensen JA, Engelman MJ. Ferrule design and fracture resistance of endodontically treated teeth. J Prosthet Dent. 1990;63:529-36.
32- Sorensen JA, Martinoff JT. Intracoronal reinforcement and coronal coverage: a study of endodontically treated teeth. J Prosthet Dent. 1984;51:780-4.
33- Toksavul S, Zor M, Toman M, Gungor MA, Nergiz I, Artunç C. Analysis of dentinal stress distribution of maxillary central incisors subjected to various post-and-core applications. Oper Dent. 2006;31:89-96.