Luiz Sekio Tanaka*, Cássia Cilene Dezan**, Karen Barros Parron Fernandes***,
Flaviana Bombarda de Andrade Ferreira****, Luiz Reynaldo de Figueiredo Walter*****, Alcindo Cerci Neto******, Silvia Fernandes Chadi*******
The influence of asthma onset and
severity on malocclusion prevalence in
children and adolescents
Objective: The influence of asthma, its severity levels and onset time on malocclusion
occurrence were investigated. Methods: The sample was composed by 176
children/ado-lescents, of both genders, aged 3 to 15 years, that were divided in two groups. The asthma group (AG) enrolled 88 children/adolescents that were seen at the Breathe Londrina Pro-gram. The asthma-free group (AFG) enrolled 88 preschool and school children recruited in 2 public schools. Malocclusion diagnosis was made according to WHO criteria (OMS, 1999). Results: A higher prevalence in malocclusions in asthmatic patients in mixed denti-tion was observed when compared to controls (p<0.05). On the other hand, these results were not observed for deciduous (p>0.05) and permanent dentition (p>0.05). A significant association was seen between asthma onset time and marked maxillary overjet (p<0.05), and open bite (p<0.05) in the mixed dentition, being both conditions more common among
those that have presented the symptoms of asthma prior to 12 months of age. Conclusion:
The results of this study indicate that the early manifestation of asthma at first year of life can cause dentofacial changes. Therefore, the prompt diagnostic of the illness, as well as the establishment of a proper therapy could improve the symptoms and chronic complications of asthma and also reduce its impact on craniofacial development.
Abstract
Keywords: Asthma. Malocclusion. Child. Adolescent.
* MSc, School of Dentistry, University of Northern Paraná (UNOPAR).
** MSc, PhD, Associate Professor of Pediatric Dentistry, State University of Londrina (UEL). *** MSc, PhD, Associate Professor of Pharmacology, UNOPAR.
**** MSc, PhD, Associate Professor of Endodontics, Bauru Dental School, University of São Paulo (USP). ***** PhD, Chairman of Pediatric Dentistry, UEL.
****** MSc, PhD, Associate Professor of Pneumology, UEL. ******* Dental student, School of Dentistry, UNOPAR.
How to cite this article: Tanaka LS, Dezan CC, Fernandes KBP, Ferreira FBA, Walter LRF, Cerci Neto A, Chadi SF. The inluence of asthma onset and sever -ity on malocclusion prevalence in children and adolescents. Dental Press J Orthod. 2012 Jan-Feb;17(1):50.e1-8.
» The authors report no commercial, proprietary, or inancial interest in the
intROduCtiOn
Asthma is a chronic disease that affects mil-lions of people around the world from different ethnic and social background.12 Its incidence has increased in recent decades, and according to an estimate by the World Health Organization, in 2005, the costs of asthma medication outstrip the costs for AIDS treatment.5 In Brazil, it affects about 20% of infantile population.23
Asthma affects lower airway and it causes nar-rowing in bronchial tubes resulting in air flow limitation, which can be reversed spontaneously or after treatment. It’s symptoms vary from the form of simple coughing episode up to recurrent severe dyspnea, and may even cause death.8 As it is a respiratory disorder, asthma may be associated with mouth breathing, which can cause changes in functional posture of oral muscles and as a con-sequence, changes in craniofacial development, dental position and occlusion can be observed.9,21
Dental literature shows contrasting results among respiratory disorders and malocclusion occurrence, especially concerning bronchial asthma. Therefore, this study aimed to evalu-ate the influence of asthma severity and onset in malocclusion prevalence, and in this way, pro-vide information so that suitable dental preven-tive programs and therapeutic approaches can be proposed in order to reduce possible orofacial deformities related to asthma.
MAtERiAL And MEtHOdS
Experimental design and study population The University of Northern Paraná Ethical Committee (Londrina-PR, Brazil) approved this study. This cross-sectional comparative study evaluated relation between asthma se-verity and onset on the prevalence of maloc-clusion in 3 to 15 years-old children. The study population was composed by two groups: Asthma group and control group (both were divided according to the dentition phase in de-ciduous, mixed and permanent).
One hundred children and adolescents from Breathe Londrina Program were invited to join the research. However, two patients were exclud-ed because they were using orthodontic appli-ances and 10 patients missed the dental appoint-ment scheduled for clinical exam. Therefore, the sample from asthma group (AG) was composed by 88 asthmatic children and adolescents.
The asthma-free group (AFG) was also com-posed by 88 children and adolescents of age, gender and social background similar to the AG group, randomly selected from two public schools, one in the west region and other in the south of the municipality.
data gathering
Data gathering was performed from Febru-ary to October 2007 by two dentists, one was responsible for the interview and the other for the nasal breathing test and clinical examina-tion. Before any methodological procedure, the parents/legal guardians were informed about the risks and benefits of the study and only af-ter a written informed consent was obtained, the patient was included in the research, as de-manded by Brazilian CNS 196/96 resolution.
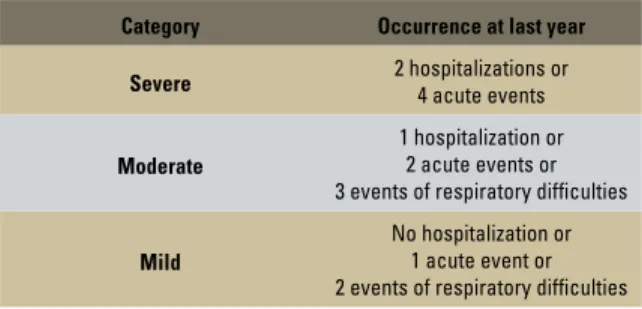
The parents were interviewed on medical and dental history of their children, with spe-cial regard to bronchial asthma history (dis-ease onset and its pharmacological treatment). These data were used to classify asthma sever-ity (Table 1), which was confirmed through patients’ medical records. Moreover, retro-spective data concerning non-nutritive sucking (such as digital sucking and pacifier’s use) and the presence of allergic rhinitis were also as-sessed by the questionnaire.
The test described by Menezes et al13 was performed to evaluate the nasal breathing. In this test, the patient must put water into the mouth and keep the lips closed without swal-lowing water during 3 minutes. The patients who open the lips or swallow the water are con-sidered mouth breathers.
Clinical examination was performed by one previously calibrated orthodontist (kappa = 0.96) according to the criteria described by World Health Organization14 for diagnosis of crowding and spac-ing in the anterior segments; maxillary and man-dibular overjet; overbite; anterior open bite; pos-terior crossbite. The molar relation was based on Angle’s classification1 for permanent teeth and To-mita, Bijella, Franco20 criteria for deciduous ones.
Statistical analysis
A multivariate logistic regression (Forward Stepwise Likelihood Ratio) was performed, with the following variables included in the model: Asthma, allergic rhinitis, digital suction, impaired nasal breathing and pacifier use after 2 years of age.
Chi Square test (X2) was used, with 95% con-fidence interval and 5% significance level, to ascer-tain the associations between malocclusions and asthma (severity and onset). To allow bivariate analysis, the variables that presented more than one category were grouped and converted to
di-chotomous variables. When the cells showed re-duced numbers, G-test with Yate’s correction was applied instead of Chi Square test.
Statistical analysis was performed at the Statisti-cal Package for Social Sciences 15.0 (SPSS) software.
RESuLtS
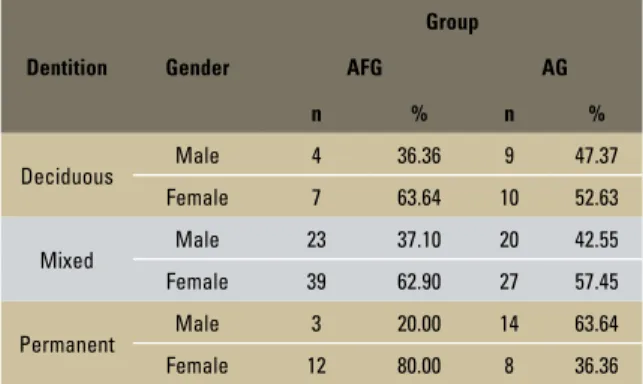
One hundred seventy six children and adoles-cents were recruited for this research, being 88 in the asthma group (AG) and 88 in the asthma-free group (AFG). The patients were split into three groups: Deciduous dentition (n=30), mixed den-tition (n= 109) and permanent denden-tition (n=37). Regarding gender, 103 patients were female while 73 were male (Table 1). The mean age of children from AG was similar to the mean age of those from AFG, except in the mixed dentition group, whereas AFG age was higher than AG (Table 2).
No statistical differences were observed be-tween the groups concerning the following vari-ables: molar relation (Chi Square= 0.390 and p> 0.05), spacing in anterior region (Chi Square= 0.846 and p>0.05), crowding (Chi Square= 0.834 and p>0.05), crossbite (Chi Square= 1.10 and p>0.05), maxillary overjet (Chi Square= 0.112 and p>0.05) and open bite (Chi Square= 0.226 and p>0.05). Despite the prevalence of malocclu-sion seems to be higher in the asthma group, no statistical differences were observed between the groups (Chi Square= 2.79 and p>0.05).
However, an increased malocclusion preva-lence in the asthma group was observed in the mixed dentition when compared to asthma-free group (Chi Square= 4.54 and p<0.05). On the other hand, no differences were observed for the deciduous (G test= 0.44 and p>0.05) and perma-nent dentitions (G test= 0.01 and p>0.05).
Considering that malocclusion occurrence was higher in asthma group and that other variables such as impaired nasal breathing and non-nutri-tive sucking habits are involved in malocclusion etiology, a multivariate analysis was performed in order to control these variables.
FIGURE 1 - Classification of asthma severity (adapted from Shulman et al,17 2001).
Category Occurrence at last year
Severe 2 hospitalizations or 4 acute events
Moderate
1 hospitalization or 2 acute events or 3 events of respiratory difficulties
Mild
onset and the presence of open bite was also ob-served in mixed dentition. In this subgroup, all the patients showing open bite had asthma onset at one year of age (Table 5).
diSCuSSiOn
The present study is part of a project designed to evaluate asthma’s impact on oral health where-as the following variables were studied: dental car-ies, oral hygiene, dental enamel defects (enamel opacities and dental fluorosis), salivary levels of cariogenic bacteria (S. mutans and Lactobacillus ssp) as well as Candida ssp; salivary properties and malocclusion prevalence. The children and ado-lescents enrolled in this research are assisted by Breathe Londrina Program. This program started in 2003 aiming to improve the quality of health assistance provided to asthmatic patients. It aims to integrate the activities of primary, specialized and hospital care, as well as to qualify measures to control home environment and use the most appropriate drug therapy for each clinical situa-tion. Drug therapy is based on the use of beclo-metasone in powder form, inhalation or spray, and albuterol in the form of an inhaled spray. Dentition Gender
Group
AFG AG
n % n %
Deciduous Male 4 36.36 9 47.37 Female 7 63.64 10 52.63
Mixed Male 23 37.10 20 42.55 Female 39 62.90 27 57.45
Permanent Male 3 20.00 14 63.64 Female 12 80.00 8 36.36 TABLE 1 - Distribution of the studied population according to group, den-tition and gender.
TABLE 3 - P value, odds ratio and confidence intervals of malocclusion prevalence according to the presence of asthma, allergic rhinitis, paci-fier use after 2 years of age, digital suction and impaired nasal breathing TABLE 2 - Comparison of mean age according to group and dentition.
Dentition Group n
Age
t p
mean SD
Deciduous AFG 11 4.55 1.44 0.04 0.97 AG 19 4.53 0.84
Mixed AFG 62 9.16 1.43 2.26 0.03 AG 47 8.40 2.06
Permanent AFG 15 12.40 1.45 0.18 0.87 AG 22 12.32 1.25
Variable P value OR CI 95%
Asthma 0.02 2.47 1.14 - 5.37
Allergic rhinitis 0.11 0.47 0.18 - 1.20
Pacifier use 0.45 0.75 0.36 - 1.58
Digital suction 0.72 1.24 0.38 - 4.00
Impaired nasal
breathing 0.00 6.24 2.08 - 18.73
Asthma and impaired nasal breathing were related to malocclusion occurrence through lo-gistic regression. However, no association was observed between allergic rhinitis or non-nutri-tive sucking habits and malocclusion (Table 3). Indeed, asthma was not related to functional changes in stomatognathic system, such as nasal breathing and tongue position. Asthma severity did not seem to influence neither the molar re-lation nor the presence of crossbite, overjet and open bite in the studied population.
Those enrolled in the program have monthly meetings and lectures with health professionals, where they receive information about the disease. The assessment of its impact was very positive because there was reduced number of crises and hospitalizations, which resulted in less suffering for patients and savings for the health system.4
There are many reports about the association between malocclusion and upper airway tract diseases. However, there is a lack of information about lower airway tract disorders, such as asthma, and malocclusion development. Upper and lower
airway disorders have the same pathogenesis6,19
and they are usually present at the same patient. Epidemiological studies showed that nearly 74% to 81% of asthmatic patients have also allergic
rhinitis.7,11,19 It is important to point out that pa-tients with allergic rhinitis or asthma as well as patients with nasal septum deviation, enlarged adenoids or nasal polyp generally present mouth breathing,3,16 which is often related to malocclu-sion etiology.18 Barros et al,2 in a cross-sectional study, observed a positive correlation between al-lergic rhinitis and mouth breathing. Venetikidou21 also reported a higher prevalence of mouth breath-ing in asthmatic patients. On the other hand, no association between asthma and impaired nasal breathing was observed in this study, even in pa-tients with moderate or severe asthma. However, through multivariate analysis, it was observed that patients with an impaired nasal breathing showed a higher occurrence of malocclusion.
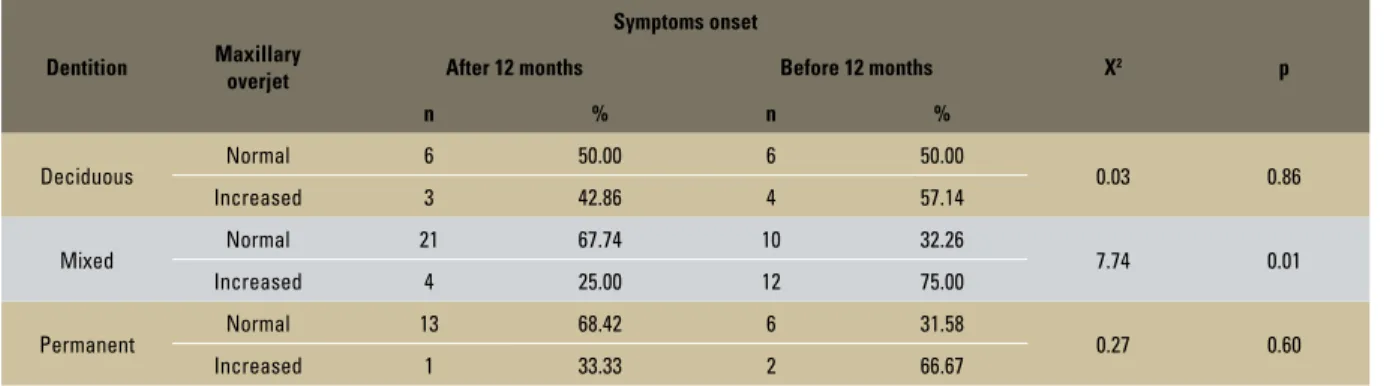
TABLE 4 - Relation between maxillary overjet and asthma onset symptoms, according to dentition phase.
TABLE 5 - Relation between the presence of open bite and asthma onset symptoms, according to dentition phase.
Dentition Maxillary overjet
Symptoms onset
X2 p
After 12 months Before 12 months
n % n %
Deciduous Normal 6 50.00 6 50.00 0.03 0.86
Increased 3 42.86 4 57.14
Mixed Normal 21 67.74 10 32.26 7.74 0.01
Increased 4 25.00 12 75.00
Permanent Normal 13 68.42 6 31.58 0.27 0.60
Increased 1 33.33 2 66.67
Dentition Maxillary overjet
Symptoms onset
X2 p
After 12 months Before 12 months
n % n %
Deciduous Absent 6 40.00 9 60.00 0.47 0.49
Present 3 75.00 1 25.00
Mixed Absent 25 59.52 17 40.48 4.66 0.03
Present 0 0.00 5 100.00
Permanent Absent 14 63.64 8 36.36 ** **
The contrasting results of this study in com-parison to Barros et al2 and Venetikidou21 could be explained considering the fact that asthmatic patients enrolled in this study take part of a pro-gram whereas the treatment is based on use of inhaled corticosteroid,4 powerful
anti-inflamma-tory drugs15 which reduce the inflammation on
upper and lower airway tract and, consequently, improve nasal breathing.10 Wenzel et al22 reported that inhaled budesonide can reduce nasal obstruc-tion in allergic children and, therefore, normalize possible changes in craniocervical angulations ob-served. However, cohort studies are necessary to evaluate if pharmacological treatment of asthma can effectively improve nasal breathing, prevent-ing the establishment of malocclusion.
Bivariate and multivariate analysis showed higher prevalence of malocclusion and conse-quent facial changes in asthmatic children and ad-olescents when compared to control ones. These changes in occlusal features (increased maxillary overjet and open bite) are more common in pa-tients with an early disease onset, when the dis-ease started at the first year of age, especially in mixed dentition group. Faria et al9 also reported an association between asthma onset and dento-facial changes observed in adults. Actually, the authors verified that crossbite and crowding are often observed in asthmatic adults in whom the
disease begun before 14 years of age. However, Venetikidou21 showed no statistically differences among overbite and overjet prevalence in asthma group when compared to control one.
Dental crowding can be influenced by func-tional changes, such as impairment of nasal breathing and presence of lower airway tract dis-eases (asthma).9 On the other hand, no associa-tion between asthma and dental crowding was ob-served at this study.
No differences were observed among asthma and control group concerning the crossbite inci-dence, even when asthma severity and the dis-ease onset are considered in the analysis. Never-theless, Venetikidou21 and Faria et al9 reported a positive correlation between asthma and cross-bite prevalence.
In this study, there were no association be-tween asthma severity and the presence of any change in occlusal features related to maloc-clusion, such as modified molar relation, pres-ence of spacing in the anterior regions, increased maxillary overjet or open bite. These results are in agreement with Faria et al9 who found no as-sociation between asthma severity and malocclu-sion in adults, despite other study have previously reported this correlation in children.22
evoke dentofacial changes. Therefore, the prompt diagnosis of asthma, as well as the correct phar-macological treatment, could improve not only its symptoms and chronic complications, but also it could reduce its impact on craniofacial devel-opment. Special oral health attention should be provided to asthmatic children and adolescents as well as it can be recommended that dentists should be included at the multidisciplinary team involved in asthma assistance.
COnCLuSiOnS
According to the present results, it can be con-cluded that:
» Asthma is associated to malocclusion prev-alence.
» There is no correlation between asthma se-verity and malocclusion.
» Asthma onset can influence malocclusion’s establishment, especially when the disease started at the first year of age.
1. Angle EH. Classiication of malocclusion. Dent Cosmos. 1899;
41:248-64.
2. Barros JR, Becker HM, Pinto JA. Evaluation of atopy among mouth-breathing pediatric patients referred for treatment to a tertiary care center. J Pediatr (Rio J). 2006;82(6):458-64. 3. Becker JM. The athlete, asthma, and allergy. Clin Rev Allergy
Immunol. 2005; 29(2):73-4.
4. Cerci Neto A, Kohatsu M, Moreira AC. Programa Respira Londrina - ampliando a integralidade na atenção ao paciente asmático no PSF de Londrina. Divulgação em Saúde para Debate. 2005; 32:53-60.
5. Cerci Neto A, Kohatsu M, Moreira AC. Programa Respira Londrina. In: Cerci Neto, A. organizador. Asma em Saúde
Pública. São Paulo: Manole; 2007. p. 79-92.
6. Corren J. Allergic rhinitis and asthma: How important is the link?
J Allergy Clin Immunol. 1997;99(2):S781-6.
7. Corren J, Manning BE, Thompson SF, Hennessy S, Strom BL. Rhinitis therapy and the prevention of hospital care for asthma: a
case-control study. J Allergy Clin Immunol. 2004;113(3):415-9.
REfEREnCES
8. Ersin NK, Gülen F, Eronat N, Cogulu D, Demir E, Tanaç R, et al. Oral and dental manifestations of young asthmatics related to medication,
severity and duration of condition. Pediatr Int. 2006;48(6):549-54. 9. Faria VC, de Oliveira MA, Santos LA, Santoro IL, Fernandes AL.
The effects of asthma on dental and facial deformities. J Asthma.
2006;43(4):307-9.
10. Grzincich G, Capra L, Cammarata MG, Spaggiari C, Pisi G. Effectiveness of intranasal corticosteroids. Acta Biomed. 2004; 75(1):22-5.
11. Leynaert B, Neukirch C, Kony S, Guénégou A, Bousquet J, Aubier M, et al. Association between asthma and rhinitis according to atopic sensitization in a population-based study.
J Allergy Clin Immunol. 2004 Jan;113(1):86-93.
12. Lugogo NL, Kraft M. Epidemiology of asthma. Clin Chest Med. 2006; 27(1):1-15.
13. Menezes VA, Leal RB, Pessoa RS, Pontes RMES. Prevalência e
fatores associados à respiração oral em escolares participantes do projeto Santo Amaro-Recife, 2005. Rev Bras Otorrinolaringol.
19. Thomas M. Allergic rhinitis: evidence for impact on asthma. BMC
Pulm Med. 2006; 30;6 Suppl 1:S4.
20. Tomita NE, Bijella VT, Franco LJ. Relação entre hábitos bucais
e má oclusão em pré-escolares. Rev Saúde Pública. 2000;
34(3):299-303.
21. Venetikidou A. Incidence of malocclusion in asthmatic children. J Clin Pediatr Dent. 1993;17(2):89-94.
22. Wenzel A, Höjensgaard E, Henriksen JM. Craniofacial morphology and head posture in children with asthma perennial
rhinitis. Eur J Orthod. 1985;7(2):83-92.
23. Zamboni MM. Prefácio. In: Cerci Neto A. Asma em saúde pública. São Paulo: Manole; 2007.
14. Organização Mundial da Saúde. Levantamentos Básicos em
Saúde Bucal. 4ª ed. São Paulo: Ed. Santos, 1999.
15. Phua GC, Macintyre NR. Inhaled corticosteroids in obstructive airway disease. Respir Care. 2007;52(7):852-8.
16. Rizzo MC, Solé D. Inhaled corticosteroids in the treatment of
respiratory allergy: safety vs eficacy. J Pediatr (Rio J). 2006;82(5 Suppl):S198-205.
17. Shulman JD, Taylor SE, Nunn ME. The association between asthma and dental caries in children and adolescents: A population-based case-control study. Caries Res. 2001;35(4):240-6.
18. Suliano AA, Borba PC, Rodrigues MJ, Caldas Júnior AF, Santos
FAV. Prevalência de más oclusões e alterações funcionais
entre escolares assistidos pelo Programa Saúde da Família em Juazeiro do Norte, Ceará, Brasil. Rev Dental Press Ortod Ortop Facial. 2005;10(6):103-10.
Contact address
Cássia Cilene Dezan Garbelini Rua Pernambuco, 520
Zip code: 86.020-120 – Londrina/PR, Brazil E-mail: [email protected]