I NTERACTI ON EXPERI ENCE FOR FAMI LI ES W HO LI VES W I TH
THEI R CHI LD’S DI SEASE AND HOSPI TALI ZATI ON
1Aline Oliv eir a Silv eir a2 Mar gar et h An gelo3
Silveira AO, Angelo M. I nt eract ion experience for fam ilies w ho lives w it h t heir child’s disease and hospit alizat ion. Rev Lat in o- am En f er m agem 2 0 0 6 n ov em br o- dezem br o; 1 4 ( 6 ) : 8 9 3 - 9 0 0 .
St ar t ing fr om t he r esear ch quest ion about t he m eanings t he fam ily at t r ibut es t o int er act ions exper ienced d u r in g t h eir ch ild ’s h osp it alizat ion , t h is st u d y t r ied t o u n d er st an d t h e in t er act ion ex p er ien ce of f am ilies in pediat r ic hospit als, as w ell t o ident ify t he int er v ent ions consider ed effect iv e t he fam ily ’s per spect iv e. Sy m bolic I nt er act ionism w as t he t heor et ical fr am ew or k t hat suppor t ed t he dat a analy sis pr ocess, and Gr ounded Theor y w as t he m et hodological fr am ew or k . Six fam ilies w it h hospit alized childr en par t icipat ed. The r esult s allow ed us t o ident ify t he phenom ena “ feeling secur e t o assum e r isks” and “ feeling insecur e t o assum e r isks” , r epr esent ing t h e sy m bolic m ean in gs at t r ibu t ed t o r elat ion al con t ex t s t h at em er ge f r om in t er act ion bet w een f am ilies an d healt h pr ofessionals. The ident ified concept s significant ly cont r ibut e t o achiev e a bet t er under st anding of t he f am ily - cen t er ed car e appr oach an d pr ov ide a w ay t o r ef lect on in t er act ion an d in t er v en t ion w it h f am ilies in pediat r ic clinical car e pr act ice.
DESCRI PTORS: fam ily ; child; disease; hospit alizat ion; int er per sonal r elat ions; fam ily w ell- being; fam ily nur sing
LA EXPERI EN CI A DE I N TERACCI ÓN DE LA FAMI LI A QUE
VI VE LA ENFERMEDAD Y HOSPI TALI ZACI ÓN DEL NI ÑO
A par t ir del cuest ionam ient o sobr e cuales son los significados at r ibuidos por la fam ilia a las int er acciones vivenciadas a lo lar go de la hospit alización del niño, est e est udio buscó com pr ender la exper iencia int er accional d e la f am ilia en el h osp it al p ed iát r ico así com o id en t if icar las in t er v en cion es con sid er ad as ef ect iv as en la p er sp ect iv a d e la f am ilia. El est u d io t u v o com o or ien t ación t eór ica el I n t er acion ism o Sim b ólico, q u e d io sust ent ación al pr oceso del análisis de los dat os, y t uvo com o r efer encial m et odológico la Teor ía Fundam ent ada en los Dat os. Par t icipar on del est udio 6 fam ilias de niños hospit alizados. Los r esult ados per m it ier on ident ificar d os f en óm en os: “ si n t i én d ose seg u r a p ar a asu m i r r i esg os” y “ si n t i én d ose i n seg u r a p ar a asu m i r r i esg os” , r epr esent at ivos de los significados sim bólicos at r ibuidos a cont ext os r elacionales que em er gen de la int er acción de la fam ilia con los pr ofesionales de salud. Los concept os ident ificados cont r ibuy en en especial par a am pliar la com pr ensión de la apr ox im ación de cuidado cent r ada en la fam ilia, adem ás de pr opor cionar un cam ino a la r eflex ión con r espect o a la int er acción e int er v ención con la fam ilia en la pr áct ica pediát r ica.
DESCRI PTORES: f am ilia; n iñ o; en f er m ed ad ; h osp it alización ; r elacion es in t er p er son ales; b ien est ar f am iliar ; enfer m er ía de la fam ilia
A EXPERI ÊN CI A DE I N TERAÇÃO DA FAMÍ LI A QUE
VI VEN CI A A DOEN ÇA E HOSPI TALI ZAÇÃO DA CRI AN ÇA
A par t ir do quest ionam ent o sobr e quais os significados at r ibuídos pela fam ília às int er ações vivenciadas dur ant e a hospit alização da cr iança, est e est udo buscou com pr eender a ex per iência int er acional da fam ília no hospit al pediát r ico e ident ificar as int er v enções consider adas efet iv as sob a per spect iv a da fam ília. O est udo t ev e com o or ient ação t eór ica o I nt er acionism o Sim bólico, que confer iu sust ent ação ao pr ocesso de análise dos dados e com o r efer encial m et odológico a Teor ia Fundam ent ada nos Dados. Par t icipar am do est udo 6 fam ílias de cr ianças hospit alizadas. Os r esult ados per m it ir am a ident ificação dos fenôm enos “ sent indo- se segur a par a assu m ir r iscos” e “ sen t in d o- se in seg u r a p ar a assu m ir r iscos” , r ep r esen t at iv os d os sig n if icad os sim b ólicos at r ibuídos aos cont ex t os r elacionais que em er gem da int er ação ent r e a fam ília e os pr ofissionais de saúde. Os con ceit os id en t if icad os con t r ib u em esp ecialm en t e p ar a am p liar a com p r een são d a ab or d ag em d e cu id ad o cen t r ado n a f am ília e pr opor cion am u m cam in h o par a a r ef lex ão acer ca da in t er ação e in t er v en ção com a fam ília na pr át ica clínica pediát r ica.
DESCRI TORES: fam ília; cr iança; doença; hospit alização; r elações int er pessoais; bem - est ar fam iliar ; enfer m agem
f am iliar
1
Paper ext r act ed fr om t he Mast er ’s Thesis, Par t of t he I nt egr at ed Pr oj ect : Nur sing int er vent ions in fam ilies of sick childr en: concept ions and act ions, funded by CNPq; 2 RN, M.Sc. in Pediat r ic Nur sing, Doct oral st udent , e- m ail: [email protected] ; 3 RN, Full Pr ofessor, Pr oj ect coor dinat or, e- m ail: angelm @usp.br. Univer sit y of São Paulo College of Nur sing
I NTRODUCTI ON
N
ur sing has incr easingly dedicat ed at t ent ion t o t h e f a m i l y a s a r e s e a r c h a n d c a r e u n i t . Th e t h e o r e t i c a l d e v e l o p m e n t o f f a m i l y n u r s i n g h a s p r o g r e ssi v e l y sh o w n t h e i m p o r t a n ce a n d n e e d t o include t he fam ily in nursing care, cont ribut ing t o t he adopt ion of fam ily - cent er ed car e pr inciples by healt h sy st em s( 1 - 2 ).The foundat ions of t he fam ily - cent er ed car e a p p r o a c h e m p h a s i z e t h e i n t e g r a l r o l e o f f a m i l y m em ber s in t he child’s life and w ell- being( 3), t ur ning t he cr eat ion of a collabor at iv e env ir onm ent bet w een nurses and fam ilies int o a m ain t arget , in w hich bot h s i d e s c a n e x p e r i m e n t m u t u a l t r u s t , e f f e c t i v e com m u n icat ion an d cooper at ion in at t en din g t o t h e fam ily ’s healt h car e dem ands( 4).
Healt h car e r elat ion s ar e ack n ow led g ed as a n ex t r em el y i m p o r t a n t i n f l u en ce o n t h e f a m i l y ’ s disease ex per ien ce, an d ar e n ot on ly con sider ed as cen t r al f or car e in it self, b u t as car e i t sel f( 5 ). Th e relat ion is seen as a dist inct int ervent ion form , w hich r epr esent s t he cor e of w or k w it h t he fam ily( 6).
The focus of int er est of fam ily int er v ent ions is t he nur se’s behav ior and indiv iduals and fam ilies’ r esp on ses t o cu r r en t or p ot en t ial h ealt h p r ob lem s, and t hey ar e aim ed at br inging about changes in t he cognit iv e, affect iv e and fam ily funct ioning dom ains( 6). I nt er vent ion can be defined as any act ion or response by a professional, w hich includes t herapeut ic a c t i o n s a n d e v i d e n t i n t e r n a l c o g n i t i v e - a f f e c t i v e r esp on ses t h at occu r r ed in a r elat ion al con t ex t , t o affect t he individual, fam ily or com m unit y funct ioning t he professional is responsible for( 7). I nt er vent ions ar e defined and updat ed in t he cont ex t of a t her apeut ic relat ion( 6, 8). Hence, t hey are inherent ly int eract ional( 7) n a t u r a l p h e n o m e n a a n d c o v e r “ e v e r y t h i n g t h a t fam ilies say m ak es a differ en ce”( 8 ). Th e v iew of t h e t h er ap eu t ic r elat ion is locat ed in a con d it ion called “ cont ext for change”, t hat is, t he cir cum st ances needed for int ervent ions t o act so as t o influence t he significant change in t he fam ily unit( 8).
Th e o r e t i ca l f a m i l y i n t e r v e n t i o n m o d e l s i n nursing, such as t he Calgar y I nt er vent ion Model( 6) and t h e Belief Mod el( 9 ), an d f am ily t h er ap y m od els lik e t h e Fam ily Resilien cy Mod el of St r ess, Cop in g an d Ad ap t at i o n( 1 0 ) an d t h e Fam i l y Resi l i en cy Mo d el( 1 1 ), a m o n g o t h e r s , p r e s e n t s o m e c o u r s e s t h a t h e l p p r of ession als w or k in g w it h f am ilies t o t h in k ab ou t i n t e r v e n t i o n . H o w e v e r, t h e p o s s i b i l i t y t h a t a n
i n t e r v e n t i o n w i l l a ct u a l l y m a k e a ch a n g e i n t h e pr oblem t he fam ily pr esent s inv olv ing ack now ledging t he r eciprocit y bet w een nur ses’ know ledge, t heir ideas and opinions, and t he fam ily ’s disease ex per ience( 6). Th i s s h o w s t h a t f a m i l y r e s e a r c h h a s si g n i f i ca n t l y co n t r i b u t e d t o t h e u n d e r st a n d i n g o f f a m i l i e s ’ a n s w e r s i n d i s e a s e s i t u a t i o n s , t o t h e com pr ehension of how healt h r elat ions ar e pr ocessed a n d ex p er i en ced . Th ese st u d i es h a v e i d en t i f i ed a series of int ervent ions t hat are considered efficacious. H o w e v e r, c o n c e r n s a b o u t t h e i n t e r a c t i o n a n d in t er v en t ion pr ocess in v olv in g fam ilies ar e r ecen t in n u r si n g , a n d f e w st u d i e s h a v e f o cu se d o n t h e se a sp e ct s, i m p e d i n g a w i d e r u n d e r st a n d i n g o f t h e ph en om en on an d t h e pr act ical applicabilit y of t h ese con cep t s.
Br azilian pediat r ic h ealt h sy st em s h av e n ot y et in cor por at ed t h e f am ily - cen t er ed car e appr oach int o t heir car e philosophy. Never t heless, fam ilies ar e i n ser t ed i n t h e car e p r o cess f o r t h ei r h o sp i t al i zed ch ild r en , an d , h en ce, ar e in t er act in g , in t er p r et in g , giving m eaning t o and act ing upon t he sit uat ion t hey ex p er i en ce.
W h e n a r t i cu l a t i n g t h i s f a ct w i t h a v a i l a b l e scien t ific k n ow ledge, k n ow ledge gaps ar e iden t ified, especially in t er m s of t h e m ean in gs em er gin g f r om fam ilies’ int eract ional experiences in t he child’s healt h car e env ir onm ent , as w ell as int er v ent ion for m s and fam ily expect at ions. The lat t er is an em er ging aspect in n u r sin g r esear ch , in t h e sen se of ap p r ox im at in g p r of ession als an d sen sit izin g t h em t o t h in k of t h e fam ily car e unit .
Based on t he quest ion “ w hat m eanings does t he fam ily at t r ibut e t o t he int er act ions exper ienced in
t he cont ex t of t he child’s hospit alizat ion?” , t his st udy
aim ed t o u n d er st an d t h e in t er act ion ex p er ien ce of fam ilies w ho live a child’s disease and hospit alizat ion, as w ell as t o ident ify effect ive int er vent ions fr om t he f am ily ’s p er sp ect iv e.
TH EORETI CAL AN D M ETH OD OLOGI CAL
FRAMEW ORK
based on t h e u n der st an din g t h at t h e m ean in gs t h e fam ily at t r ibut es t o t he ev ent s it ex per iences ar e co-const ruct ed in social int eract ion and t hat int ervent ions a r e i n t e n s e l y i n t e r a c t i o n a l p h e n o m e n a , w h o s e r e s p o n s e s f o u n d b y t h e f a m i l y ( i n t e r v e n t i o n s ) con st it u t e in t r a as w ell as in t er p er son al in t er act ion elem en t s.
The int eract ionist per spect ive concent rat es on t h e n at u r e o f i n t er act i o n s, t h e d y n am i cs o f so ci al act iv it ies am ong per sons, t he m eaning of ev ent s for p e o p l e i n t h e w o r l d t h e y l i v e i n , t h e n a t u r a l env ir onm ent s of t heir daily life and t he act ions t hey p e r f o r m( 1 2 ). I n t h i s p e r s p e c t i v e , t h e f a m i l y i s under st ood as a social gr oup t hat int er act s m ut ually and w it h t he elem ent s present in t he experiences t he g r o u p l i v e s , a t t r i b u t i n g m e a n i n g s t o t h e s e ex per iences, w hich r esult fr om t heir int er act ions( 13).
Gr o u n d e d Th e o r y i s a q u a l i t a t i v e m et h od olog ical ap p r oach t h at seek s t o u n d er st an d t h e m ean in g of t h e ph en om en on or ev en t f r om t h e par t icipant s’ per spect ive. These m eanings der ive from t h e est ablish ed social in t er act ion . I t is a sy st em at ic qualit at ive dat a collect ion and analysis process, aim ed at pr oducing t heor y t hat ex plains and allow s for t he under st anding of social and cult ur al phenom ena( 14).
Place of st udy
Th e st u d y w as car r ied ou t at t h e Ped iat r ic Hospit alizat ion Unit of a Teaching Hospit al in São Paulo Cit y - SP.
Et h ical Aspect s
The field r esear ch st ar t ed aft er t he appr ov al and aut hor izat ion by t he Resear ch Et hics Com m it t ee at t h e Un iv er sit y of São Pau lo Colleg e of Nu r sin g . The aspect s of Resolut ion CNS196/ 96 w er e r espect ed, w it h a v iew t o gu ar an t eein g t h e st u dy par t icipan t s’ r ight s. Subj ect s officially confir m ed t heir decision t o p a r t i ci p a t e i n t h e st u d y b y si g n i n g t h e f r e e a n d in for m ed con sen t t er m .
Dat a collect ion
Dat a w er e collect ed t hr ough obser vat ions and int erview s. The observat ions focused on t he relat ives’ behavior and on t he int er act ion m om ent s am ong t hese r el at i v es an d o t h er p er so n s p r esen t i n t h e ch i l d ’s h ospit alizat ion con t ex t .
Th e i n t e r v i e w w a s t h e s e c o n d s t r a t e g y adopt ed t o obt ain t he fam ilies’ nar r at iv e about t heir in t er act ion al ex per ien ces. Fam ilies w er e appr oach ed and pr epar ed for t he int er view by filling out t he fam ily’s for m , including t he genogr am and ecom ap.
Relat iv es pr esent dur ing hospit alizat ion w er e inv it ed t o par t icipat ing, independent ly of t he fam ily ’s ch a r a ct er i st i cs, h o sp i t a l i za t i o n t i m e o r t h e ch i l d ’ s m edical diagnosis. St udy part icipant s w ere six fam ilies w h o e x p e r i e n c e d t h e c h i l d ’ s d i s e a s e a n d h ospit alizat ion .
The int er v iew s st ar t ed w it h a br oad guiding quest ion: What is it lik e for y ou t o hav e a sick and hospit alized child. To t he ext ent t hat t he nar rat ive w as
obt ained and int er act ional aspect s em er ged, anot her br oad guiding quest ion w as int r oduced: How is y our r el at i o n w i t h h eal t h p r o f essi o n al s? w i t h a v i ew t o
ex plor in g t h e fam ily ’s in t er act ion ex per ien ce.
Dat a an aly sis
We follow ed t he st ages r ecom m ended by t he Const ant Com par at ive Met hod of Gr ounded Theor y( 14), st ar t ing w it h open dat a coding. I n t his fir st st age, aft er in it ial codin g, t h e codes w er e gr ou ped accor din g t o t h eir con cept u al sim ilar it ies an d differ en ces, leadin g t o ca t e g o r i e s. Th e n , w e m o v e d o n t o t h e o r e t i ca l co d i n g . Th i s se co n d st a g e a i m s t o i n t e g r a t e t h e c a t e g o r i e s r e f e r r i n g t o o n e a n d t h e s a m e p h e n o m e n o n , w i t h a v i e w t o u n d e r s t a n d i n g t h e p h en om en a t h at r ep r esen t ed t h e i n t eg r at i v e b on d am ong cat egor ies and per m it t ed t he dev elopm ent of a gr ou n ded t h eor y.
RESULTS: TH E FAM I LY’S I N TERACTI ON
EXPERI ENCE
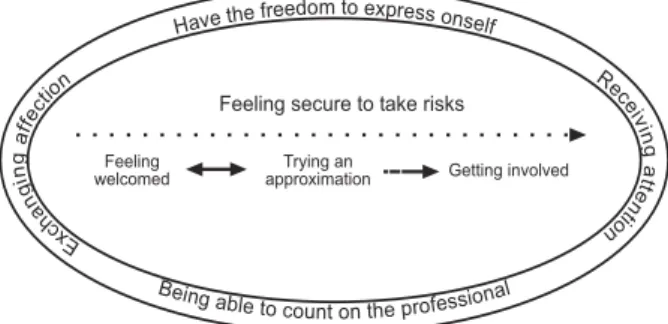
gener at e a cont ext t hat fam ily is FEELI NG WELCOMED in. The feeling of w elcom ing allow s t he fam ily t o feel secu r e an d dr iv e it t o in v olv e in a m or e in t egr at ed and par t icipat or y m ov em ent , t hat is, t ak ing r isk s by TRYI N G AN APPROXI MATI ON a n d t a k i n g r i s k b y GETTI NG I NVOLVED.
FEELI NG WELCOMED r esult s fr om a r elat ional cont ext in w hich t he fam ily perceives t hat t he personal an d p r of ession al q u alit ies of p eop le r elat iv es m eet d u r i n g t h e i r e x p e r i e n c e a c c o m m o d a t e t h e i r ex pect at ions and pr ov ide for t he est ablishm ent of a r elat ion t hat allow s t hem t o feel secur e t o act in t he sit uat ion and t o t ake r isks in or der t o at t end t o t heir h ealt h car e n eeds. Th e fam ily feels w elcom ed w h en int er act ing w it h people and ex per iencing act ions lik e r eceiv ing at t ent ion, ex changing affect ion, ex changing
f r i e n d s h i p , r e c e i v i n g c o m f o r t i n g w o r d s , w h e n
per ceiv ing t hat t hey ar e being able t o count on t he p r o f e ssi o n a l a n d h a v i n g t h e f r e e d o m t o e x p r e ss
t h em sel v es.
Re c e i v i n g a t t e n t i o n s i g n a l s t h a t t h e pr ofessionals ar e concer ned and under st and w hat t he fam ily is feeling and needs at t hat m om ent and cover s or ien t at ion s an d ex p lan at ion s r eceiv ed at t h e r ig h t t i m e , w i t h o u t e x t e n d i n g t h e i r u n c e r t a i n t i e s a n d an g u ish .
. . . t he doct or her self t alk ed t o us quit e a lot , she
ex p l ai n ed m e ev er y t h i n g v er y w el l an d , so , t h o se l ad i es
volunt eer s com e by, w ho com e t o pray, but I go t o t he chapel
e v e r y d a y t o o , h i s ( t h e so n ’s) f a t h e r, g r a n d f a t h e r a n d
grandm ot her ar e evangelicals, t hey com e her e t o pr ay, and it
helps, you k now ?, w hen you hear, like t hat , a fr iendly w or d, it
alw ay s helps, y ou k now ? Fr om t he people w ho hav e fam ily
her e t oo, t hey see us cr y ing lik e t hat , desper at e, and t hey
co m e t o t a l k a h . . . m y so n w e n t t h r o u g h t h i s, d o n ’ t g e t
dow nhear t ed... w e becom e fr iends and end up t alking...
People’s affect , ev idenced in k ind w or ds and g e st u r e s, sy m b o l i ze s co m p a ssi o n , h u m a n i t y a n d e m o t i o n a l i n v o l v e m e n t w i t h t h e f a m i l y. W h e n int eract ions ar e loaded w it h affect ion, t hey t end t o be m or e significant in t he fam ily ’s ex per ience.
Th e ex ch an g e of f r ien d sh ip r ep r esen t s t h e aw ak en in g of m u t u al con f id en ce in t h e in t er act ion . The professionals’ at t it ude is seen as friendly w hen it does not pose t hr eat s t o t he fam ily, w hen it does not im pose con dit ion s an d, in gen er al, w h en in t er act ion o ccu r s sp o n t a n e o u s a n d t r a n sp a r e n t l y, r e v e a l i n g int ent ions t o help and pr ofessional sincer it y.
Com for t ing w or ds t r ansm it st r engt h and help t h e f am ily t o h av e m or e f ait h an d h op e ab ou t t h e
sit u at ion t h ey ar e liv in g. Th ey can com e as pr ay er s o r o f f e r e l e m e n t s t h a t a l l o w t h e f a m i l y t o f e e l w elcom ed in t heir r eligious and spir it ual needs and, at t he sam e t im e, shar e t heir beliefs.
The fam ily feels w elcom ed w hen it per ceiv es t hat it can count on t he healt h professionals not only t o t ake car e of t he child, but also t hat t heir qualit ies and possibilit ies t o help ex t end t o t he fam ily ’s needs as a w hole. The fam ily’s feeling t hat it can t alk openly em er g es w h en p eop le ad op t an em p at h ic at t it u d e, dem onst r at ing int er est , under st anding and desir e t o h elp .
FEELI NG WELCOMED is t h e con sequ en ce of a r elat ional cont ext t hat is int er pret ed posit ively and, at t he sam e t im e, is t he cause, i.e. t he init ial condit ion f or t h e f am ily t o g et in v olv ed in a m ov em en t t h at seek s t o in t er act w it h t h e pr of ession al, TRYI NG AN APPROXI MATI ON.
TRYI NG AN APPROXI MATI ON r epr esen t s t h e fam ily’s m ovem ent , dr iven by t he feeling of w elcom ing an d secu r it y, con t in u in g t h e sear ch t o in t er act w it h t he pr ofessional, in t he at t em pt t o find answ er s t o it s needs and r each it s goals. The fam ily t r ies t o get closer t o t h e h ealt h p r of ession al b y u sin g st r at eg ies lik e ask ing for help, ask ing quest ions and opening up t o
t h e pr of ession al.
Ask in g f or h elp is a d iscr et e m ov em en t b y t h e f am ily t o g et closer t o t h e h ealt h p r of ession al, and const it ut es an at t em pt t o par t icipat e. When feeling t hat t hey can count on t he pr ofessionals, t he fam ily does not feel int im at ed t o ask for help w it h r espect t o it s n eeds, pr oblem s or in adequ acies in car e f or t h e ch ild.
When feeling t hat t he professional is open t o inquir ies and w illing t o clar ify any doubt s, t he fam ily get s closer, ask in g qu est ion s abou t t h e disease an d a b o u t h o sp i t a l f u n ct i o n i n g . Qu e st i o n s a b o u t t h e d isease m ost ly cen t er on t h e p h y sician r esp on sib le f or t h e ch ild , as t h e f am ily b eliev es h e is t h e on ly p er so n cap ab l e o f g i v i n g ex act i n f o r m at i o n , w h i l e quest ions about issues involving t he hospit al dynam ics and funct ioning ar e dir ect ed at t he nur se.
opens up t o t he pr ofessional and, at t he sam e t im e, also capt ures new perspect ives, configured in different p o ssi b i l i t i es t o f ace t h e d i f f i cu l t i es cau sed b y t h e disease an d h ospit alizat ion .
As a co n seq u en ce o f an ap p r o x i m at i o n i n w hich t he fam ily m em ber s exper ience t hat t he healt h p r o f essi o n a l a ccep t s a n d v a l u es t h ei r ef f o r t s, t h e feeling of secur it y is st r engt hened ov er t im e and t he f am ily t ak es n ew r isk s, m ov in g f r om t h e p h ase of TRYI NG AN APPROXI MATI ON t o GETTI NG I NVOLVED. GETTI NG I NVOLVED is t he consequence of a r ecipr ocal appr ox im at ion bet w een t he fam ily and t he professional, w hich m akes it possible t o m aint ain and dev elop t h e in t er act ion ov er t im e. Wh en per ceiv in g t h a t t h e p r o f e s s i o n a l c o r r e s p o n d e d t o t h e i r ex p ect at ion s, t h e f am ily in v est s in t h e in t er act ion , m ot iv at ed by t he posit iv e m eanings appr ehended in ear lier in t er act ion s, w h ich p er m it t ed t h em t o h av e g r e a t e r co n t r o l a n d f e e l m o r e se cu r e a b o u t t h e ex p er ien ced ev en t s. Th e f am ily ’s in v olv em en t w it h t he healt h pr ofessional is sy m bolized in t he fam ily ’s e x p e r i e n ce a s e st a b l i sh i n g f r i e n d sh i p b o n d s a n d est ablishing a t r ust r elat ionship.
I n t h e f a m i l y ’ s ex p er i en ce, est a b l i sh i n g a f r ien d sh ip b on d acq u ir es t h e m ean in g of a r elat ion t h a t g o e s b e y o n d t h e p r o f e s s i o n a l d i m e n s i o n , ex ch a n g es a n d a n sw er s a r e l o a d ed w i t h p er so n a l e x p e r i e n c e a n d t h e r e l a t i o n i s m a r k e d b y t h e sanct ioning of convent ional roles. The friendship bond is an essen t ially af f ect iv e in v olv em en t , m ar k ed b y i n cr ea si n g co m p r eh en si o n , r esp ect a n d sy m p a t h y bet w een fam ilies and professionals. The professionals’ at t it udes and feelings ar e consider ed m or e im por t ant t h a n t h e i r t h e o r e t i c a l k n o w l e d g e a n d t e c h n i c a l com p et en cies.
Est ablishing a t rust relat ionship represent s t he f a m i l i e s’ i n v o l v e m e n t w i t h p r o f e ssi o n a l s’ cl i n i ca l pr act ice, w it hout ex cessiv e affect iv e inv olv em ent , in w h i ch p r o f essi o n al - p er so n l i m i t s an d co n v en t i o n al roles are m aint ained t hroughout t he relat ionship. The t r ust r elat ionship is an inv olv em ent in w hich fam ilies feel t hat t hey ar e under st ood by pr ofessionals w hen m an if est in g m ean in gs r elat ed t o t h e ch ild’s disease a n d h o sp i t a l i za t i o n , ch a r a ct e r i ze d b y t r a n sp a r e n t act ions, sensit iv e r ecept iv eness, w ar m int er est in t he f a m i l i e s ’ d o u b t s a n d f e e l i n g s a n d p r o f e s s i o n a l s ’ com m it m ent t o t he fam ily unit s’ w ell- being.
The fam ily’s secur it y is m aint ained over t im e t h r o u g h a s e r i e s o f s i g n i f i c a n t i n t e r p e r s o n a l int er act ions. The under st anding about t he t her apeut ic
r e l a t i o n t h a t a s s u m e s t h e s y m b o l i c m e a n i n g o f FEELI NG SECURE TO TAKE RI SKS i n t h e f a m i l y ’ s ex per ien ce allow ed for t h e iden t ificat ion of effect iv e in t er v en t ion s.
I n t e r v e n t i o n s co n si d e r e d e f f e ct i v e i n t h e fam ily ’s per spect iv e, because t hey pr ov ide r elief and w e l l - b e i n g , i n c l u d e : r e c e i v i n g i n f o r m a t i o n a n d e x p l a n a t i o n s; r e ce i v i n g so ci a l su p p o r t ; r e ce i v i n g r elig iou s an d sp ir it u al su p p or t ; r eceiv in g ad eq u at e c a r e f o r t h e c h i l d ; r e c e i v i n g w o r d s o f c o m f o r t ; r eceiv ing em ot ional suppor t ; shar ing t he ex per ience; sh ar in g car e for t h e ch ild an d t alk in g open ly t o t h e p r of ession al.
Figur e 1 - Phenom enon: Feeling secur e t o t ak e r isk s
FEELI NG I NSECURE TO TAKE RI SKS: t h e fam ily feels insecur e t o t ak e r isk s w hen it int er pr et s t h e in t er act ion al con t ex t as t h r eat en in g t o it s self, leading t o t he per cept ion of FEELI NG HELPLESS.
Th e e x p e ct a t i o n s f a m i l i e s b r i n g i n t o t h e in t er act ion w it h h ealt h pr ofession als an t icipat e t h eir n e e d s a n d a l so a k i n d o f i d e a l i ze d p r o f e ssi o n a l . Fam ilies not only need t o but expect pr ofessionals t o g et closer, b e com m u n icat iv e an d u n d er st an d w h at t h e y a r e g o i n g t h r o u g h b e ca u se o f t h e i r ch i l d ’ s hospit alizat ion, grant ing condit ions for a respect ful and pleasan t r elat ion al con t ex t .
FEELI NG HELPLESS is t he feeling ar oused in t he fam ilies’ experience w hen t heir expect at ions about h ealt h pr of ession als ar e n ot at t en ded t o du r in g t h e in t er act ion , en t ailin g t h e f eelin g of in secu r it y abou t est ablishing a line of act ion or behavior in t he sit uat ion. Th e f a m i l y f e e l s h e l p l e s s e x p e r i e n c i n g t h e p r o f e ssi o n a l ’ s d i st a n ce , e x p e r i e n ci n g a b se n ce o f
co m m u n i ca t i o n , n o t b e i n g u n d e r st o o d , su f f e r i n g
im posit ions and hav ing it s beliefs dest r oy ed.
Bot h dist ance and absence of com m unicat ion w it h h ealt h pr of ession als con t r ibu t e t o t h e f am ilies’ uncom fort able feeling of helplessness, as t hey consider t hat t hey cannot count on t he pr ofessionals t o at t end t o t heir needs.
Havethe freedom to express onself
Being able to count on the professional Ex
ch a n g
in
ga ffect
ion Rece
iv ing
a
tte
n tio n Feeling secure to take risks
Feeling welcomed
Trying an
...you don’t have your fam ily, t her e’s nobody ar ound,
you’r e living an at ypical sit uat ion, a sit uat ion t hat is difficult t o
bear , so it w ould be good if t he pr ofessionals w er e closer , w er e
m or e consider at e, som et im es y ou don’t ev en see a nur se or
auxiliar y, t hey w alk in and out , and you end up not even having
cont act ...
Fam ilies’ per cept ion abou t bein g ign or ed as s o m e o n e i m p o r t a n t i n t h e c h i l d ’ s c a r e p r o c e s s em er ges w hen pr ofessionals ar e seen as closed and im posin g, becau se t h ey do n ot t alk w it h t h e fam ily. Th ese at t it u d es cr eat e t h e f eelin g of h elp lessn ess, a c c o m p a n i e d b y c o n c e r n s , a n g u i s h a n d u n r e s t because t hey t hink t hey ar e being a bur den, t hat t hey ar e not w elcom e in t he hospit al cont ext , and because t h ey do n ot f in d ex plan at ion s f or t h e pr of ession al’s act ion s.
I n su f f er in g im p osit ion s, f am ilies f eel t h at t h e i r i n d i v i d u a l i t y a n d a u t o n o m y a r e b e i n g d i s r e s p e c t e d . Th e y i n t e r p r e t t h e c o n t e n t s o f professionals’ discourse, as w ell as t heir gest ures and t o n e o f v o i c e a s i m p o s i t i o n s , m a k i n g t h e m f e e l w eak ened and, at t he sam e t im e, helpless.
The feeling of helplessness also appears w hen t he fam ilies’ beliefs ar e dest r oyed, t hr ough w or ds t hat d o n o t t a k e i n t o a cco u n t t h ei r d i f f i cu l t i es a t t h a t m om ent and t heir need t o m aint ain hope and fait h in o r d e r t o a v o i d a c o l l a p s e . Th i s f a c t i s s e e n a s disr espect for t heir r eligious beliefs and feelings.
Fam ilies experience absence of underst anding w h en t h e p r of ession al’s an sw er s ar e d isap p oin t in g , arouse negat ive feelings like m ist rust , anguish, anger; w hen t he pr ofessional infer s j udgm ent s and w hen t hey do not r eceiv e pr oper at t ent ion.
Th e f eel i n g o f h el p l essn ess t h r ea t en s t h e fam ily ’s secu r it y, for cin g it t o m ake decision s on it s p o s i t i o n i n t h e s i t u a t i o n : S U B M I TTI N G TO TH E S I TUATI O N o r PERS I S TI N G TO W A RD S TH E ACHI EVEMENT OF I TS NEEDS.
SUBMI TTI NG TO THE SI TUATI ON is a fam ily d e ci si o n t h a t r e f l e ct s i t s i n se cu r i t y t o w a r d s t h e e x p e r i e n ce d si t u a t i o n a n d t h e l a ck o f a b i l i t y a n d f l e x i b i l i t y t o co p e w i t h p r e ssu r e s i n t h e h o sp i t a l cont ext , and evidences it s dist ancing fr om t he healt h pr ofessional. SUBMI TTI NG TO THE SI TUATI ON ent ails t he fam ily ’s at t em pt t o pr ot ect it self against conflict s a n d f u r t h e r e x h a u s t i o n . Th u s , f a m i l i e s s u b m i t t hem selv es, r esigning t o t he sit uat ion, being obliged t o r e s p e c t d i f f e r e n c e s a n d w a i t i n g f o r t h e
pr of ession al’s in it iat iv e or appr ox im at ion .
Fam ilies see no alt ernat ives t o cope w it h t he sit uat ion and t r y t o adj ust t hem selv es, accept ing t he fact t hat t hey cannot count on t he pr ofessional t o help t hem w it h t heir needs. Hence, t hey t r y t o go t hr ough t he sit uat ion w it h t he suppor t of ot her fam ily m em ber s, f am ilies t h at sh ar e t h e sam e ex p er ien ce an d t h eir int er nal for ce, fait h and hope.
Th e fam ilies k n ow t h at n ot all pr ofession als ar e equal and t hat t heir ex pect at ions cannot alw ay s be at t ended t o, facing a sit uat ion t hat needs t o r espect an d accep t d if f er en ces in or d er t o liv e t og et h er in har m ony and av oid conflict s in t he hospit al cont ex t .
I m m o b i l i ze d b y t h e f e e l i n g o f i n se cu r i t y, f am ilies let t h em selv es b e g u id ed b y p r of ession als’ act ion s, w ait in g f or t h eir appr ox im at ion or in it iat iv e t o i n t e r a ct . Th e t e n si o n p e r m e a t i n g t h e f a m i l i e s’ su bm ission an d block s t h eir act ion s is pr ov ok ed by t he pr ofessionals’ at t it udes as w ell as by t he fam ily’s difficult y t o express it s percept ions and int erpret at ions of t he sit uat ion.
Fam ilies can also r espond t o t he sit uat ion of h e l p l e s s n e s s b y PERS I S TI N G TO W A RD S TH E ACHI EVEMENT OF THEI R NEEDS, w h ich con sist s in t heir at t em pt t o r ecov er and/ or m aint ain t heir sense o f se cu r i t y. Th e f a m i l y i n si st s t h a t i t s n e e d s b e at t ended t o, being aw ar e of it s r ole and being aw are of t he pr ofessional’s dut y .
Th e g o a l s t h e f a m i l y t r i e s t o a ch i e v e i n in t er per son al m eet in gs ar e pr ofou n dly in flu en ced by it s n eeds, w h ich m ot iv at e t h e in t er act ion . How ev er, t h e f a m i l y ’ s m o b i l i za t i o n i s a l so i n f l u en ced b y i t s a w a r e n e s s a b o u t i t s r o l e a n d a b o u t t h e h e a l t h pr ofessional’s dut y. By being awar e of it s r ole as t he c h i l d ’ s c a r e p r o v i d e r a n d d e f e n d e r, t h e f a m i l y elaborat es st rat egies and faces all difficult ies in order t o g u a r a n t e e i t s r i g h t s a n d r e sp o n se s i n v i e w o f em er gin g dem an ds, does n ot su bor din at e it s v alu es and beliefs and, t hus, does not subm it t o inst it ut ional rules or st at us and pow er pressures, w hich are im plied in t he exchanges processed in int eract ions w it h healt h p r of ession als.
Figure 2 - Phenom enon: Feeling insecur e t o t ake r isks
RESULT DI SCUSSI ON
Th e si g n i f i ca n t i n t e r p e r so n a l i n t e r a ct i o n s dev eloped dur ing t he fam ily ’s ex per ience ev idence a w ay of being and being w it h t he fam ily, w hose effect ive
i n t e r v e n t i o n s r e f l e ct a t t i t u d e s a n d co m p e t e n ci e s r elat ed t o healt h pr ofessionals.
U n d e r s t a n d i n g t h e f a m i l y ’ s i n t e r a c t i o n ex p er ien ce allow ed f or t h eor et ical ad v an ces ab ou t in t er act ion an d in t er v en t ion p h en om en a an d t h ese r e s u l t s p a r t i c u l a r l y c o n t r i b u t e t o a b r o a d e r under st anding of t he concept s involved in t he fam ily-cen t er ed car e appr oach .
Fa m i l y - c e n t e r e d c a r e w i d e l y c o v e r s t h e concept s of parent s’ part icipat ion in care for t he child’s healt h; inv olv em ent and cooper at ion bet w een healt h t eam an d p ar en t s in d ecision m ak in g ; p r ov id in g a p leasan t h osp it al en v ir on m en t t h at n or m alizes t h e fam ily’s funct ioning in t he healt h care cont ext as m uch as possible and deliver ing car e t o fam ily m em ber s as w ell as t o t he sick child( 3).
U n d e r s t a n d i n g t h e f a m i l y ’ s i n t e r a c t i o n ex per ien ce dem on st r at es t h at , bey on d par t icipat in g or get t ing involved in care for t he child, par ent s need t o f e e l w e l c o m e d a n d s e c u r e i n t h e h o s p i t a l en v ir on m en t , v alu in g pr of ession als’ act ion s su ch as b e i n g w i t h t h e f a m i l y , sh a r i n g b o t h t h e f a m i l y ’ s
ex per ience and car e for t he child.
Pr om ot in g a w elcom in g r elat ion al con t ex t , w hich allow s t he fam ily t o feel secur e t hr oughout it s e x p e r i e n c e a n d p r o v i d e s f o r n e w c o m p e t e n c y d e v e l o p m e n t a n d c o p i n g r e s o u r c e s , i s a n o t h e r fundam ent al elem ent of fam ily - cent er ed car e, as t he at t em pt t o find secur it y in a non- fam iliar envir onm ent is t h e m ain n eed of r elat iv es ex per ien cin g a ch ild’s hospit alizat ion and inv olv es bot h fam ily secur it y and guar ant eeing t he child’s secur it y( 15).
Fam ilies’ decisions t o persist or subm it t o t he sit uat ion are influenced by t heir sense of securit y and
c o m p e t e n c e , w h i c h a r e s t r o n g l y a f f e c t e d b y professionals’ at t it udes. Their securit y is achieved and s t r e n g t h e n e d o v e r t i m e w h e n t h e y m a n a g e t o est ab l i sh a r el at i on of i n v ol v em en t an d m u t u al i t y, expr essed in bonds of fr iendship and t r ust w it h healt h p r of ession als.
I n t e r v e n t i o n s f a m i l i e s f i n d e f f e c t i v e t h r o u g h o u t i t s i n t er act i o n ex p er i en ce i n cl u d e n ew r esources, w hich pr om ot e secur it y in t he per for m ance of com pet encies t o m anage em er ging dem ands and, consequent ly, pr om ot e balance in fam ily funct ioning, r elief and w ell- being.
The im por t ance of t he r elat ional com ponent in fam ily- cent ered care is especially evidenced by t he d e v e l o p m e n t o f a co l l a b o r a t i v e r e l a t i o n b e t w e e n f am ilies an d h ealt h p r of ession als. Fam ily m em b er s v alu e pr of ession als w h o u n der st an d t h at each ch ild and fam ily is unique and ident ify t hat t he essence of a collabor at iv e r elat ion inv olv es confidence and open com m u n icat ion , w h ich capacit at e n egot iat ion s abou t t he respect ive roles assum ed in t he relat ion and allow f or t h e accom m odat ion of each ch ild’s an d f am ily ’s specificit ies and ex pect at ions( 1 6 ).
The r esult s of t his st udy suppor t t he evidence t h at bot h sick ch ildr en an d t h eir f am ilies h av e car e n eeds. Th er ef or e, pr ov idin g f or a r elat ion al con t ex t i n w h i ch t h e f am i l y m an ag es t o est ab l i sh i t s r o l e t h r o u g h o u t t h e ex p er i en ce i s f u n d am en t al f o r t h e fam ily t o get involved in a m ovem ent t o seek answ er s t o em er ging dem ands in t he ex per ienced sit uat ion.
B y i n c r e a s i n g i t s c a p a c i t y t o o v e r c o m e difficult ies and r esist t o per sist ing st r ess, t he fam ily al so co n q u er s v i t al r eso u r ces t o co p e w i t h f u t u r e ch a l l e n g e s( 1 1 ). H e n ce , a n y i n t e r v e n t i o n i s a l so a p r ev en t iv e m easu r e, w h ich can in f lu en ce b ot h t h e fam ily unit ’s im m ediat e and long- t er m w ell- being( 11).
FI NAL CONSI DERATI ONS
The sy m bolic m eanings t he fam ily at t r ibut es t o it s int er act ion ex per iences allow ed for t heor et ical a d v a n c e s a b o u t i n t e r a c t i o n a n d i n t e r v e n t i o n p h e n o m e n a i n v o l v i n g f a m i l i e s , b r o a d e n e d t h e u n d e r st a n d i n g a b o u t t h e co n ce p t s a n d e l e m e n t s inv olv ed in t he fam ily - cent er ed car e per spect iv e and in dicat ed a cou r se for r eflect in g abou t an d apply in g t he appr oach in pr act ice.
U n d e r s t a n d i n g t h e f a m i l y ’ s i n t e r a c t i o n e x p e r i e n c e i n t h e c o n t e x t o f t h e c h i l d ’ s c a r e Not being understood
Feeling insecure to take risks
Ha ving
itsbe
liefs d
estroyed
Experiencingabsence of com
muni cati
on Suffering
im po
sitio
n
E xp
erien cing th
e professionals dista nce Feeling helpless
Submitting to the situation
Persisting towards the achievement
dem on st r at es t h at it is possible t o t ak e car e of t h e fam ily, prom ot e and m aint ain fam ily funct ioning, r elief and w ell- being in view of sit uat ions of suffering, such as a ch ild’s disease an d h ospit alizat ion . How ev er, it also dem onst r at es t hat fam ily car e is not an ex plicit com pon en t of h ealt h pr of ession als’ r ole, ev iden cin g t h at m an y ch allen ges st ill n eed t o be ov er com e f or f a m i l y - ce n t e r e d ca r e t o d e v e l o p a s a p r e v a i l i n g pr act ice in t he cont ex t of pediat r ic car e.
Despit e t his st udy’s cont ribut ions, t here is st ill a need for a br oader under st anding about t he fam ily’s int er act ion ex per ience, about t he ident ified concept s
and int er v ent ion possibilit ies inv olv ing fam ilies, t hus cont r ibut ing t o t he v alidat ion and ex pansion of t hese r esu lt s.
Ther e ar e count less t heor et ical and pr act ical ch allen ges an d t h is st u dy r epr esen t s t h e st ar t of a l o n g r o a d a h e a d . S t u d i e s a i m e d a t c l a r i f y i n g in t er act ion al p r ocesses an d in t er v en t ion s in v olv in g fam ilies are ext rem ely relevant for t he t heoret ical and p r a ct i ca l a d v a n cem en t o f f a m i l y n u r si n g . I t i s b y focusing on t he int eract ional and int ervent ion process t h at som et h in g can sy st em at ically b e d on e t o h elp fam ilies( 1 7 ).
REFERENCES
1. Pauli MC, Bousso RS. Crenças que perm eiam a hum anização
d a assist ên cia em u n id ad e d e t er ap ia in t en siv a p ed iát r ica.
Rev Lat ino- am Enfer m agem 2003 m aio- j unho; 11( 3) : 280- 6.
2 . Co l l e t N , Ro ch a SMM. Cr i a n ça h o sp i t a l i z a d a : m ã e e
e n f e r m a g e m co m p a r t i l h a n d o o cu i d a d o . Re v La t i n o - a m
En f er m ag em 2 0 0 4 m ar ço- ab r il; 1 2 ( 2 ) : 1 9 1 - 7 .
3 . Fr a n ck LS, Ca l l e r y P. Re- t h i n k i n g f a m i l y - cen t r ed ca r e
acr oss t h e con t in u u m of ch ild r en ’s h ealt h car e. Ch ild : Car e
Heal t h Dev el 2 0 0 4 ; 3 0 ( 3 ) : 2 6 5 - 7 7 .
4 . Th or n e S, Rob in son CA. Healt h car e r elat ion sh ip s: t h e
chr onic illness per spect ive. Res Nur s Healt h 1988; 11( 5)
293-3 0 0 .
5 . Robin son CA. Healt h car e r elat ion sh ips r ev isit ed. J Fam
Nu r s 1 9 9 6 ; 2 ( 2 ) : 1 5 2 - 7 3 .
6. Wr ight LM, Leahey M. Enfer m eir as e fam ílias: um guia par a
a av aliação e int er v enção na fam ília. São Paulo ( SP) : Roca;
2 0 0 2 .
7. Wr ight LM, Bell JM. The fut ur e of fam ily nur sing r esear ch:
int er v ent ions, int er v ent ions, int er v ent ions. Japan J Nur s Res
1 9 9 4 ; 2 7 ( 2 - 3 ) : 4 - 1 5 .
8 . Rob in son CA, Wr ig h t LM. Fam ily n u r sin g in t er v en t ion s:
w h at f am ilies say m ak es a d if f er en ce. J Fam Nu r s 1 9 9 5 ;
1 ( 3 ) : 3 2 7 - 4 5 .
9. Wr ight LM, Wat son WL, Bell JM. Beliefs: t he hear t of healing
in fam ilies and illness. New Yor k : Basic Book s; 1996.
1 0 . McCu b b i n H, Th o m p so n A, McCu b b i n M, ed s. Fa m i l y
assessm en t : r esilien cy, copin g an d adapt at ion - inv en t or ies
for r esear ch and pr act ice. Madison: Univ er sit y of Wisconsin
Sy st em ; 1 9 9 6 .
1 1 . Walsh F. For t alecen do a r esiliên cia f am iliar. São Pau lo:
Ro ca; 2 0 0 5 .
12. Char on JM. Sy m bolic int er act ionism : an int r oduct ion, an
int er pr et at ion, an int egr at ion. Englew ood Cliffs: Pr ent ice- Hall;
1 9 8 9 .
1 3 . An g e l o M. Co m a f a m íl i a e m t e m p o s d i f íce i s: u m a
per spect iva de enfer m agem . [ Tese] . São Paulo ( SP) : Escola
de Enfer m agem da USP; 1997.
14. Glaser BG, St rauss AL. The discover y of gr ounded t heor y.
New Yor k : Aldin e; 1 9 6 7 .
15. MacKean GL, Thur st on WE, Scot t CM. Br idging t he divide
bet w een f am ilies an d h ealt h pr of ession als’ per spect iv es on
f am ily - cen t r ed car e. Healt h Ex p ec 2 0 0 5 ; 8 : 7 4 - 8 5 .
1 6 . Hallst r öm I , Ru n n eson I , Elan der G. Obser v ed par en t al
n eeds du r in g t h eir ch ild’s h ospit alizat ion . J Ped Nu r s 2 0 0 2 ;
1 7 ( 2 ) : 1 4 0 - 8 .
1 7 . Bel l JM. Pr o cess a n d o u t co m e i n f a m i l y i n t er v en t i o n
r e s e a r c h : Me t h o d o l o g i c a l c h a l l e n g e s . I n : I n t e r n a t i o n a l
Nu r si n g Re se a r ch Co n f e r e n ce ; 1 9 9 4 ; Va n co u v e r. Br i t i sh
Colu m b ia: Can ad á; 1 9 9 4 .