w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Review
Article
Impact
of
anti-TNF
agents
in
postoperative
complications
in
Crohn’s
disease:
a
review
Mansur
Saab
a,
Bárbara
Saab
a,
Márcia
Olandoski
b,
Cláudio
Saddy
Rodrigues
Coy
c,
Paulo
Gustavo
Kotze
a,∗aColorectalSurgeryUnit,PontifíciaUniversidadeCatólicadoParaná(PUC-PR),Curitiba,PR,Brazil
bBiostatisticsDepartment,PontifíciaUniversidadeCatólicadoParaná(PUC-PR),Curitiba,PR,Brazil
cColorectalSurgeryUnit,UniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received9January2015 Accepted20February2015 Availableonline8April2015
Keywords: Crohndisease
Tumor-necrosisfactoralpha Colorectalsurgery
a
b
s
t
r
a
c
t
Therealimpactofbiologicaltherapy(anti-TNFagents)inabdominaloperationssecondaryto Crohn’sdiseaseisamatterofdebateintheinternationalliterature.Severalstudies demon-stratedthattherecanbeanincreaseinpostoperativecomplicationsinpatientspreviously treatedwiththeseagents.Ontheotherhand,themajorityofstudiespublishedoverthe lastyearsquestionthiseffect,anddidnotdemonstrateanyrelationshipbetweenbiologics andoutcomesrelatedtosurgicalpostoperativecomplications.Somemeta-analyseswere published,withdifferentoutcomesanddifferentconclusions.Experimentalstudiesin ani-malswerealsorecentlypublished,withoppositeresults,despitesimilarmethodology.In thisreview,theauthorsresumealltherelevantpapersintheinternationalliteraturewith respecttothetheme,anddemonstratetheheterogeneityofthestudies,aswellasthe dis-parityoftheirresultsandoutcomes.Therealimpactofanti-TNFagentsonpostoperative complicationsinCrohn’sdiseaseisstillcontroversial,andneedstobebetterelucidated. Controlledtrialsmustbeperformedtobetteraddressthisissue.
©2015SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
Impacto
dos
anti-TNF
nas
complicac¸ões
pós-operatórias
na
doenc¸a
de
Crohn:
uma
revisão
Palavras-chave: Doenc¸adeCrohn
Fatordenecrosetumoral-alfa Cirurgiacolorretal
r
e
s
u
m
o
Orealeverdadeiroimpactodaterapiabiológica,constituídapor inibidoresdofator de necrosetumoral(TNF)alfa,emoperac¸õesabdominaisnadoenc¸adeCrohn,aindaé exten-samentedebatidonaliteratura.Hámuitosestudosquereferemaumentodapossibilidade decomplicac¸õesempacientestratadospreviamentecomessesagentes.Poroutrolado,há
umasériemaiordetrabalhosquequestionamesseaumento,nãodemonstrandoqualquer
impactodessasdrogasnosdesfechospós-operatórios.Algumasmetanálisesforam publi-cadas,comresultadosligeiramentediversos.Trabalhosexperimentaisemanimaisforam
∗ Correspondingauthor.
E-mail:[email protected](P.G.Kotze).
http://dx.doi.org/10.1016/j.jcol.2015.02.003
recentemente realizados, igualmente com resultados opostos, apesar de metodologia semelhante.Nessarevisão,osautoresdiscorremsobretodosostrabalhosrelevantesna literaturanacionaleinternacionalsobreotema,edemonstrama heterogenicidadedos mesmos,bemcomoadisparidadedosresultadosedesfechos.Orealimpactodosagentes anti-TNFsobreoperac¸õesabdominaisnadoenc¸adeCrohnaindaécontroverso,eprecisaser melhorelucidado.Estudoscontroladosdevemserrealizadosparamelhorelucidac¸ãodessa questão.
©2015SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
In recent years,remarkable progress in the medical
treat-mentofCrohn’sdisease(CD)wasachieved,particularlywith
theadventoftumornecrosisfactor(TNF)inhibitors.1,2 The
clinicalresponse tothesedrugs hasbeen demonstrated in
somerandomizedtrialsand,subsequently,otherstudieshave
shownreductioninhospitalizationsandsurgeriesanda
con-sequentchange in thenatural history ofthe disease,with
the possibility of preventing complications in some
sub-groupsofresponders.3,4Infliximab(IFX)wasthefirstanti-TNF
drug approvedfor CD, and knowledgeon this drugin the
managementofpatientswasconsolidatedbymorethan14
years ofclinical experience.5 Subsequently, in2007, a
sec-ondbiologicalagentofTNF-inhibitorclasswasapprovedby
regulatoryagenciesforCDtherapy,adalimumab(ADA).More
recently,athirdbiologicdrug,certolizumabpegol(CTZ),was
approved as an option for CD therapy. These agents
con-stitute what is known today as biological therapy in the
management of CD. Its use is growing exponentially, and
currently, these biologicals are considered the most
effec-tivedrugsinthemedicalmanagementofmoderatetosevere
disease.5
TheindicationsforbiologicaltreatmentinCDaredirected
mainly for severe forms of this disease,3,4 and frequently
a surgical treatment will be indicated during the use of
thesedrugs.5Asthesedrugsarepotentimmunosuppressants, thereisanobviousconcern,ifthisreductioninthedefenses somente,retirarbody’scouldleadtogreaterpossibilitiesof
surgical and infectious complications in the postoperative
periodofabowelresectioninCDpatients.Thereisalso con-troversyontheeffectsoftheseagentsattissuelevel,inbowel
anastomosis healing process. Data from the literature are
conflicting,and retrospectivestudies ofcaseseriesshowed equallyconflictingconclusions.
Againstthisscenarioofdoubt, wheretherereallyexists
insecurity of surgeons in operating patients previously
exposed to biological agents, it is critical to elucidate the
relationship between these drugs and the rates of
surgi-caland medicalcomplications in the postoperative period
afterintestinalresectionsinCD. Thereisa notablelackof
solid and consistent data on the subject. Hence, this
sce-nario justifies the conduction of this review, in order to
verify,throughafullsearchoftheliterature,informationon
the actualoutcome related to complicationsafter
abdomi-nalsurgeryinCDpatientswithpriorexposuretobiological therapy.
Clinical
studies
with
a
trend
for
further
postoperative
complications
with
the
use
of
biologicals
A study conductedatthe ClevelandClinic inOhio (United
States), published in 2008, compared the effects of IFX in
patients undergoing ileocolectomy for CD into 3 groups:
operatedpatientswithoutIFXinpre-biologicalera,patients
in the era after drug commercialization, and patients
pre-viously exposed to IFX before surgery. Retrospectively, 60
patientsoperatedwithpriorexposuretoIFXwithin3months
beforethe procedure showedhigherrisk ofsepsis,
abdom-inal abscesses,re-admissions and anastomoticdehiscence.
Theauthorsalsosuggestedthatproximaldiversionstomas
wereprotectivefactorsinrelationtothesehigherrisks,and
couldberecommendedinpatientswithprevioususeofthis
medication.6
Rizzoetal.,inanItaliansingle-centerretrospectivestudy,
analyzedthesurgicaloutcomesin114patientswithCDand
ulcerative colitis, with prior exposure to anti-TNF agents
(n=54)comparedtoacontrolgroupwithoutuseofthesedrugs (n=60).Withnodistinctionbetweenthetypeofinflammatory disease,theauthorsconcluded,inanunivariateanalysis,that
infectious complicationsweremorefrequentinindividuals
previouslytreatedwithbiologicals(60%versus13%;p=0.023). However,inamultivariateanalysis,anincreasein postopera-tivecomplicationsrelatedtoprevioususeofbiologicalswere notfound.Onlyhighdosesofcorticosteroidshavebeenlinked tohigherratesofinfection.7
Inameta-analysispublishedin2012,Kopylovetal.
ana-lyzedeightstudiesonthesubject,allincludedinthisreview, withatotalof1641patients.Afterthepooledanalysisofdata
fromthesestudies,theauthorsconcludedthattherewasa
greaterriskofinfectiouscomplicationratesinpatients
pre-viously treated withIFX, predominantly notrelated to the
surgical site. They also founda tendency (not statistically
confirmed)towardanincreaseintheratesofoveralland non-infectiouscomplications.8
In a French multicenter retrospective study, Serradori
etal.analyzedthelevelsofpostoperativeinfectionsafter217
majorabdominaloperationssecondarytoCD.Inaunivariate
analysis,theauthorsfoundthatpatientsolderthan25years andwithprevioususeofcorticosteroids,ofanti-TNFagents, andofbiologicalstogetherwithcorticosteroidswererisk
fac-tors forinfections. On the other hand,in the multivariate
analysis only the concomitant preoperative use of
infectious complications (odds ratio [OR]=8.03, 95% confi-denceinterval[CI]=1.93–33,43;p=0.035).9
Syedetal.,in2013,publishedastudyincludingpatients
undergoingvarioustypesofabdominaloperations,evennot
relatedtoCD.325operativeprocedureswerestudiedin211
patients, and 150 of these procedures were performed in
subjectswithpriorexposuretobiologicalagents.Inthe
mul-tivariate analysis, the authors found that previous use of
TNF-alpha inhibitors (including IFX, ADA and CTZ) was a
risk factor for overall higher rates of infectious complica-tions(OR=2.43;95%CI=1.18–5.03)andsurgicalsiteinfections (OR=1.96;95%CI=1.02–3.77).10
Four meta-analyses on the possible impact ofanti-TNF
agentsonpostoperativecomplications inCDpatients have
recently been published. Interestingly, all meta-analyzes
includevirtuallythesamestudies(allincludedinthis
liter-aturereview),andthroughslightlydifferentmethods,these
studies came to only slightly different conclusions. From
thesemeta-analyses,onlyone,whichpooledeightstudies,
pointedtoanon-influenceofbiologicaltherapyon postopera-tiveoutcomes;thiswillbediscussedatthe nextsession.11
The other three meta-analyzes concluded that a negative
influenceoftheuseofthesedrugsinpostoperative compli-cationsinCDmayexist.Narulaetal.reported,afterinclusion
of18studies and4659patients, thatbiologicalagentsmay
slightlythe riskofpostoperativecomplications,and,above all, this can signify an analysis bias, and not the biologi-cal effect of these drugs per se.12 El-Hussuna et al., after
including 14 studies with 679 patients exposed to
biologi-calsversus2363controls,concludedthat,instudieswithless
potential for bias, previous use of these agents increased
theriskofanastomoticdehiscence.13 Finally,Yangetal.,in
theirmeta-analysisanalyzing18studiesand 5769patients,
showedanassociationbetweenprevioususeofbiologicalsand complications (OR=1.45, 95% CI=1.04–2.02) and infectious (OR=1.47 95% CI=1.08–1.99) and non-infectious (OR=2.29, 95%CI=1.14–4.61)complications,respectively,inthe postop-erativeperiod.Theauthorssuggestamodestincreaseinthe riskofcomplicationsinpatientspreviouslyexposedto anti-TNFagents.14
Thefirstprospectivestudyonthetheme“biologicals
ver-sus surgicalcomplications” inthe management ofCD was
published byLau et al.in 2014. In this study, the authors
measuredIFXserumlevels7daysbeforethesurgical
proce-dure,inanattempttorelatehigherserumlevelswithhigher ratesofcomplications.Fromatotalsampleof217patients,
123were CD patients. Using anIFX serumlevel of3g/ml
as a cutoff point, overall (OR=2.5, p=0.03) and infectious (OR=3.0,p=0.03)complications inthe postoperativephase
weremorefrequentinpatientswithserumlevelsabovethis
abovethis level. Higherrates ofpostoperative overall
com-plicationsand ofre-admissions in patientswith IFXlevels
≥8g/mlalsowerenoted,comparedtothose subjectswith
IFXlevels<3g/ml.Thesechangeshavenotbeenconfirmed inpatientswithulcerativecolitissubmittedtosurgical
proce-dures,probablyduetoamorerapidwashoutofthedrugin
thesepatients.15
Thestudiesdescribedinthisreviewsessionare
summa-rizedwiththeirrespectivemethodologiesandkeyfindingsin
Table1.
Clinical
studies
with
no
trend
for
further
complications
with
postoperative
use
of
biologicals
Thefirststudyonthesubject“biologicalsandsurgical
com-plications in CD” in the literature was carried out in the
UnitedStatesin2003.Inthisarticle,Tayetal.retrospectively
demonstrated that patients with previoususe of
immuno-suppressantsinitsvariousformsandundergoingabdominal
operations secondary to CD did not show higher rates of
intra-abdominalsepticcomplications(abscesses,dehiscence,
enterocutaneousfistulas)versussubjectswithoutassociated
immunosuppression(5.6%inimmunocompromisedpatients
versus25%inthoseuntreated,p<0.01).Inamultivariate anal-ysis,theauthorsalsoquestionedapossibleprotectiveeffect
ofimmunosuppression(withsomepatientsusingbiological
agents),withreducedratesofcomplicationscomparedtothe
controlgroup.16
Colombeletal.,in2004,publishedastudyreportingthefirst experienceoftheMayoClinicinMinnesota,UnitedStates,for
possibleconsequencesofperioperativeuseofIFXin
postop-erativecomplications.Fromatotalof270patientsundergoing
abdominaloperationsforCDoverthetimeperiodconsidered
(allwithintestinalresections),52wereexposedtoIFX.These
authors found noincreasedrisk ofsepticcomplicationsin
patientswhoreceivedIFXintheperioperativeperiod.17 Marchaletal.,in2004,reportedtheexperienceofaBelgian
referralcentre,where40patientspreviouslyexposed toIFX
undergoingintestinalresectionhadtheiroutcomescompared
to39matchedpatientsaccordingtoageandtypeofprocedure.
The objective was to evaluate,between groups, the
occur-renceofearlyandlatemajorandminorcomplications.These
authorsdidnotfoundhigherratesofcomplicationsbetween
groupsandnodifferencebetweeninin-hospitallengthofstay forthesepatients.Atrendtowardahigherincidenceof
infec-tionsingeneralinthegrouppreviouslyexposedtoIFXwas
found,butwithoutstatisticalsignificance.18
In2008,anamericanstudy conductedbyKunitakeetal.
reportedtheisolated experienceofanUSreferralcenterin
the management of IBDin relationto possiblechanges in
postoperativecomplicationratesinpatientswho have
pre-viouslyusedIFX. Fromatotalof413patientsstudied,only
188hadCD.Inthatstudy,patientswithulcerativecolitisand
indeterminateinflammatoryboweldiseasewereincluded.In
theirpaper,theauthorsdidnotclarifytheexactnumberofCD
patientswithprioruseofIFX.However,theyconcludedthat
therewerenooveralldifferences(withoutdistinguishingthe
typeofinflammatoryboweldisease)inclinicalandsurgical
complicationrates(16.8%inthegroupwithIFXvs.15.7%in
controlgroup;p=1.0).Nevertheless,therewasahighermean ofin-hospitallengthofstayforthegroupofoperatedpatients whohadbeenpreviouslytreatedwithIFXversuscontrolgroup (12.2vs.10.2days,p<0.0001).19
In2009,aseriesof112CDpatientsoperatedattheMayo
ClinicinArizona,UnitedStates,wasretrospectivelydescribed,
andpossiblechangescausedbycorticosteroids,
immunosup-pressants and biologicals on postoperative outcomes were
evaluated. Ofthese 112patients, only17 used IFXpriorto
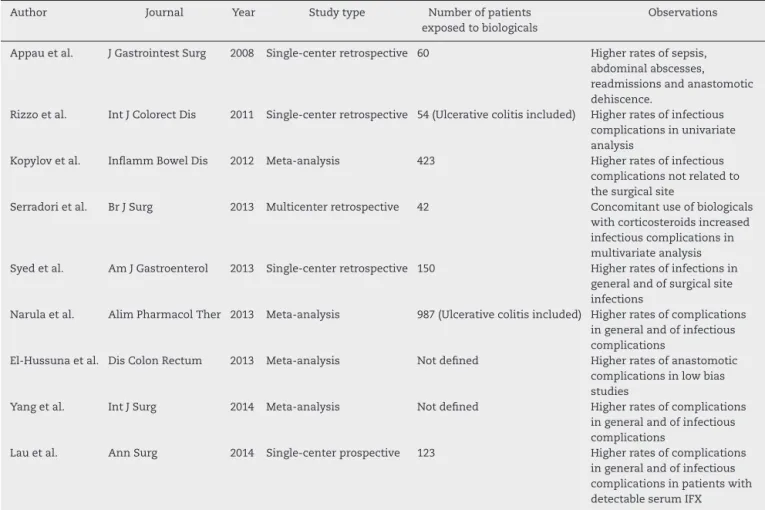
Table1–MajorstudiesshowingapossiblenegativeimpactoftheuseofbiologicalsinpostoperativecomplicationsinCD, withhigherratesofcomplications.
Author Journal Year Studytype Numberofpatients exposedtobiologicals
Observations
Appauetal. JGastrointestSurg 2008 Single-centerretrospective 60 Higherratesofsepsis, abdominalabscesses, readmissionsandanastomotic dehiscence.
Rizzoetal. IntJColorectDis 2011 Single-centerretrospective 54(Ulcerativecolitisincluded) Higherratesofinfectious complicationsinunivariate analysis
Kopylovetal. InflammBowelDis 2012 Meta-analysis 423 Higherratesofinfectious complicationsnotrelatedto thesurgicalsite
Serradorietal. BrJSurg 2013 Multicenterretrospective 42 Concomitantuseofbiologicals withcorticosteroidsincreased infectiouscomplicationsin multivariateanalysis Syedetal. AmJGastroenterol 2013 Single-centerretrospective 150 Higherratesofinfectionsin
generalandofsurgicalsite infections
Narulaetal. AlimPharmacolTher 2013 Meta-analysis 987(Ulcerativecolitisincluded) Higherratesofcomplications ingeneralandofinfectious complications
El-Hussunaetal. DisColonRectum 2013 Meta-analysis Notdefined Higherratesofanastomotic complicationsinlowbias studies
Yangetal. IntJSurg 2014 Meta-analysis Notdefined Higherratesofcomplications ingeneralandofinfectious complications
Lauetal. AnnSurg 2014 Single-centerprospective 123 Higherratesofcomplications ingeneralandofinfectious complicationsinpatientswith detectableserumIFX
inusersofIFX.However,theauthorsdidfoundthatbloodloss >400ml(p<0.003)andemergencysurgery(p<0.005)werethe onlyriskfactorsforincreasedpostoperativecomplications.20 Nasiretal.publishedin2010anupdateoftheexperience
oftheMayoClinicinMinnesota(UnitedStates)onthe
sub-ject,thisbeingthefirststudytoincludepatientsusingADA andCTZinaseries.Theauthorsincludedpatientspresenting anyintra-abdominalsutureline,asaresultofthesurgical pro-cedureforCD.Theresultsof119patientspreviouslyexposed toanti-TNFagents,comparedto251whodidnotuse biologi-cals,weresimilarwithrespecttopostoperativecomplications (27.9%vs.30.1%,p=0.63),showingnohigherratesof compli-cationsinpatientsusinganti-TNFagentspriortosurgery.21
InBrazil,Kotzeetal.presentedin2011,duringtheCrohn’s
andColitisFoundationofAmerica(CCFA–USA)meeting,the
resultsofapilotsampleofpatients,withlackofassociation
betweensurgicalcomplicationsandprevioususeof
biologi-calsinCDpatients.76patientswerestudied,19ofthemwith priorexposuretobiologicalagents(12toIFXand7toADA). Theratesofoverallpostoperativecomplications,anastomotic
dehiscence,urinarytractinfectionandpneumoniawere
sim-ilar betweenthesetwogroups. Thiswasthe firststudy on
thesubjectinBrazilianpatients, andalthoughpublishedin
abstract form, showed interestingresults, compatible with
thosefoundinmostpapersfromtheinternationalliterature.22 Canedoetal.publishedtheresultsofaretrospectivestudy fromtheClevelandClinic,Weston,Florida,UnitedStates.The
study included225patientsundergoingbowelresectionfor
CDdividedinto3groups:thosewithpreviousIFX,thoseon
immunosuppressants and corticosteroids,and finallythose
on aminosalicylatesonly. Inthis series, there were no
dif-ferencesbetweenthegroupsregardingpneumonia(p=0.14),
surgicalsiteinfection(p=0.35),abscess(p=0.34)and anasto-moticdehiscence(p=0.44)rates.Thus,theauthorsconcluded
that theprevious use ofIFX wasnotrelated tochangesin
postoperativeoutcomesinpatientswithDCinneedofmajor
abdominalsurgery.23
El-Hussuna et al., in a Danish study that included 417
patients operatedinfourdifferenthospitals, comparedthe
postoperativeoutcomes of32 patientsoperatedwith
previ-oususeofbiologicalsversus385patientswithoutprevioususe
ofthisagents.Nohigherratesofanastomoticpostoperative
complications were foundinthe grouppreviouslyexposed
to biologicalagents versusnon-exposed group (9%vs. 12%;
p=0.581).Inthisstudy,amultivariateanalysisshowedthat prioruseofcorticosteroidsindailydoses>20mgand
colon-colonicanastomosesweremainriskfactorsforanastomotic
dehiscenceinCDpatients.24
Ina Germanstudy,Kasparek etal.analyzedthe impact
of prior use of IFX in abdominal operations secondary to
CD. Asmethodology, these authors matchedtheir patients
with control-cases.Ineach group, 48 patientswith similar
demographic characteristicsand minorcomplicationswere
andanastomoticcomplicationswasfoundbetweengroups, besidesin-hospitallengthofstay.Theauthorssuggestedthat thereisnoneedforachangeinsurgicalstrategyinCDpatients onlyinfaceoftheuseofIFXperse.25
Mascarenhas et al. studied possible complications
sec-ondarytoileocolicresectionfromadifferentperspective,but
alsoretrospectively.Theseauthorscomparedthe
complica-tions in93 CD patients (19 withprevious use ofbiological
therapy) versus 698 patients undergoing ileocolectomy for
othercauses.Inasubanalysisoftheirstudy,theseauthors foundnoincreaseintheoverallcomplicationrateinpatients withCDwithorwithoutprevioususeofbiologicals.26
Norgardetal.,inDenmark,reportedtheirfindingsina
full-countrydatabasewithover2000patients.Thepostoperative
outcomesaftermajorabdominalsurgeryforCDin214patients
withprevioususe ofbiologicalagentswere comparedwith
theoutcomesfrom2079patientswithoutexposuretothese
drugs,inthelargeststudyonthesubjecteverpublishedin
literature.Theauthorsconcludedthattherewasnodifference incomplicationsbetweenthetimeofprevioususeofIFX(less
thantwoweeksfromthedateoftheoperationand2–12weeks
fromthedateoftheprocedure)versuscontrolgroup.These
authorsalsoconcludedthat nohigherratesofreoperation,
anastomoticdehiscenceandbacteremiaoccurredinpatients
withprioruseofanti-TNFagents.27
In an interestingCanadian study, Waterman et al. also
comparedtheeffectsofpriorexposuretobiological agents
inabdominaloperationssecondarytoCD.Inthisseries,195
patientshadpreviouslyusedIFXorADA(orboth)ina popula-tionof473patients,includingpatientswithulcerativecolitis
and indeterminate IBD. In patients with a combination of
biologicals with immunosuppressive drugs prior to their
surgery,higherratesofurinarytractandsurgicalsiteinfection werefound.Thetimeelapsedsincethelastdoseofthe biolog-icalagenttosurgery(lessthan2weeks,2–4weeksand30–180 days)didnotinfluencepostoperativecomplicationrates.One ofthenoveltiesofthisstudywasthedeterminationofserum
levelsofIFXpreviouslytotheprocedure, andpatientswith
detectablelevelsofthedrughadearlycomplicationsinsimilar numberstothosewithundetectablelevels.28
Baffordet al. publishedin2013 the MountSinai
Hospi-talexperienceforsurgicalcomplicationsin196CDpatients,
dividedinto2groups–withandwithoutuseof
immunosup-pressivedrugs(includingbiologicalagents).Likemanystudies intheliterature,theauthorsidentifiedahigherriskof com-plicationsin users of biological agents. Additionally, these
authorshavenotconcludedinfavorofanincreasedriskof
postoperativecomplicationsinpatientspreviouslymedicated
withcorticosteroids, thiopurines,orwith acombination of
morethanoneimmunosuppressiveagent.29
A meta-analysis published in 2013 by Billioud et al.
included 21 studies on the effect ofbiologicals in
abdom-inal surgery for IBD in general (CD and ulcerative colitis
analyzed together).The authors concluded that there was
anincreasedriskofinfections ingeneralinthe postopera-tiveperiodinCDpatients(OR=1.45;95%CI=1.03–2.05),but
emphasized thatpotential influencing factors,mainly
con-comitanttherapies,mightnotbeadequatelystudied.30These resultsweresimilartothoseinameta-analysispublishedby Rosenfeldetal.in2013,whofoundnoinfluenceofbiological
therapyoncomplicationsinpatientsfromalmostthesame
studies.11
Also retrospectively, Krane et al. studied possible
con-sequences of IFX use in operations conducted solely by
laparoscopy.ThisUSsampleincludedCDandulcerative
coli-tispatients,and65CDpatientswereoperatedwithprevious
useofIFX,andtheirresultsintermsofcomplicationswere
comparedto194patientswiththesamediseaseandwithout
priorbiologicaltreatment.Therewasnodifferencebetween
groups regardingthe conversion rates tolaparotomy,
over-allcomplications,anastomoticdehiscence,thromboembolic
eventsandinfections.Theauthorsconcluded,througha
mul-tivariateanalysis,thatthereisnoinfluenceofIFXonsurgical outcomesafterlaparoscopicoperations.31
InaScandinavianstudy,Myrelidetal.studied298patients
from six referral centers,111 ofwhom previously exposed
tothe useofbiologicalsbeforesurgery.Theprimary
objec-tive of the study was to analyze comparatively the two
groups in relation to the previous use of these drugs and
anastomotic complications. Infectionsingeneralwere
sec-ondarilyanalyzed.Theauthorsdemonstratedthattherewas
no difference between groups for anastomotic
complica-tions(7.2%versus8%;p=0.976),postoperativecomplications and infections ingeneral. Similarly,differencesintermsof
anastomoticdehiscencebetweengroupswerenotfoundina
multivariateanalysis(OR=0.89;95%CI=0.37–2.17),revealing norelationshipbetweenprevioususeofbiologicalsandworse postoperativeoutcomes.32
Inamorerecentcriticalreview,Papaconstantinouetal., throughasystematicliteraturereview,carefullyanalyzedthe
mostimportantstudiesdiscussedinthissession,andusing
scores ofstudies byMINORScriteria, wereunableto reach
firmconclusionsabout thereal impactofbiologicalagents
onpostoperativeoutcomesinCrohn’sdisease.33Theresults
ofthemainstudiesthatdidn’tshowapossibleeffectof
bio-logicalagentsonpostoperativeoutcomesinCDpatientsare
summarizedinTable2.
Experimental
studies
Aninterestingexperimentalstudyonthe“surgeryand biolog-icals”themewaspublishedbyLopesetal.in2008.34Wistar
rats,allocatedinto,withandwithoutasinglesubcutaneous
doseof5mg/kgofIFX,wereoperated.Amedianlaparotomy
was performedintheseanimalsand,aftereuthanasia,the
tensileforcerequiredforopeningthesuturelineinthe
abdom-inal wallwasmeasured.Itwasobservedinthisstudy that
ratswithpriorIFXneededlesstensilestrengthtoopenthe
suturelineversuscontrolgroupondays3and7after laparo-tomy.ThisstudysuggestedapotentialeffectofIFXonchanges
ininflammatoryandproliferativephasesofwoundhealing,
whichcouldhaveanimpactonapossibleincreaseontherates ofanastomoticdehiscence.34
Morerecently,theinternationalliteraturehasbeen
con-cerned with an understanding, at the physiological and
cellularlevel, on theeffects ofanti-TNF agentsinthe
pro-cessofanastomosishealing,andconsequentlyonapossible
impactonthesuccessofthesurgicaloutcome.Thus,some
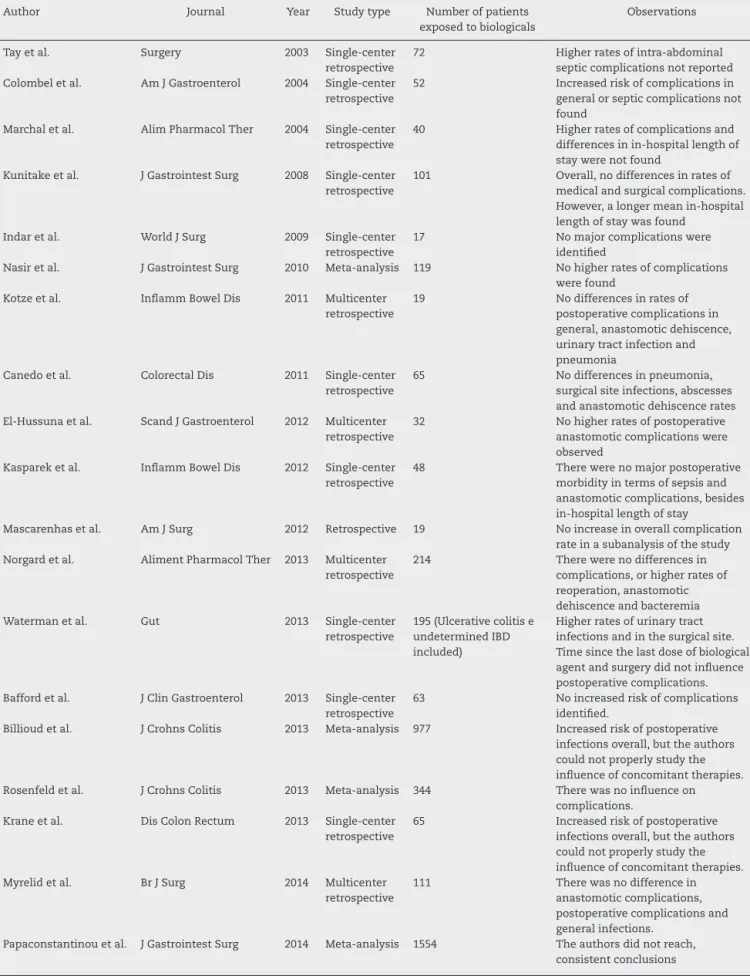
Table2–MainstudiesshowingnodifferenceintherateofpostoperativecomplicationsinpatientswithCDusing biologicals.
Author Journal Year Studytype Numberofpatients exposedtobiologicals
Observations
Tayetal. Surgery 2003 Single-center retrospective
72 Higherratesofintra-abdominal septiccomplicationsnotreported Colombeletal. AmJGastroenterol 2004 Single-center
retrospective
52 Increasedriskofcomplicationsin generalorsepticcomplicationsnot found
Marchaletal. AlimPharmacolTher 2004 Single-center retrospective
40 Higherratesofcomplicationsand differencesinin-hospitallengthof staywerenotfound
Kunitakeetal. JGastrointestSurg 2008 Single-center retrospective
101 Overall,nodifferencesinratesof medicalandsurgicalcomplications. However,alongermeanin-hospital lengthofstaywasfound
Indaretal. WorldJSurg 2009 Single-center retrospective
17 Nomajorcomplicationswere identified
Nasiretal. JGastrointestSurg 2010 Meta-analysis 119 Nohigherratesofcomplications werefound
Kotzeetal. InflammBowelDis 2011 Multicenter retrospective
19 Nodifferencesinratesof postoperativecomplicationsin general,anastomoticdehiscence, urinarytractinfectionand pneumonia
Canedoetal. ColorectalDis 2011 Single-center retrospective
65 Nodifferencesinpneumonia, surgicalsiteinfections,abscesses andanastomoticdehiscencerates El-Hussunaetal. ScandJGastroenterol 2012 Multicenter
retrospective
32 Nohigherratesofpostoperative anastomoticcomplicationswere observed
Kaspareketal. InflammBowelDis 2012 Single-center retrospective
48 Therewerenomajorpostoperative morbidityintermsofsepsisand anastomoticcomplications,besides in-hospitallengthofstay
Mascarenhasetal. AmJSurg 2012 Retrospective 19 Noincreaseinoverallcomplication rateinasubanalysisofthestudy Norgardetal. AlimentPharmacolTher 2013 Multicenter
retrospective
214 Therewerenodifferencesin complications,orhigherratesof reoperation,anastomotic dehiscenceandbacteremia Watermanetal. Gut 2013 Single-center
retrospective
195(Ulcerativecolitise undeterminedIBD included)
Higherratesofurinarytract infectionsandinthesurgicalsite. Timesincethelastdoseofbiological agentandsurgerydidnotinfluence postoperativecomplications. Baffordetal. JClinGastroenterol 2013 Single-center
retrospective
63 Noincreasedriskofcomplications identified.
Billioudetal. JCrohnsColitis 2013 Meta-analysis 977 Increasedriskofpostoperative infectionsoverall,buttheauthors couldnotproperlystudythe influenceofconcomitanttherapies. Rosenfeldetal. JCrohnsColitis 2013 Meta-analysis 344 Therewasnoinfluenceon
complications. Kraneetal. DisColonRectum 2013 Single-center
retrospective
65 Increasedriskofpostoperative infectionsoverall,buttheauthors couldnotproperlystudythe influenceofconcomitanttherapies. Myrelidetal. BrJSurg 2014 Multicenter
retrospective
111 Therewasnodifferencein anastomoticcomplications, postoperativecomplicationsand generalinfections.
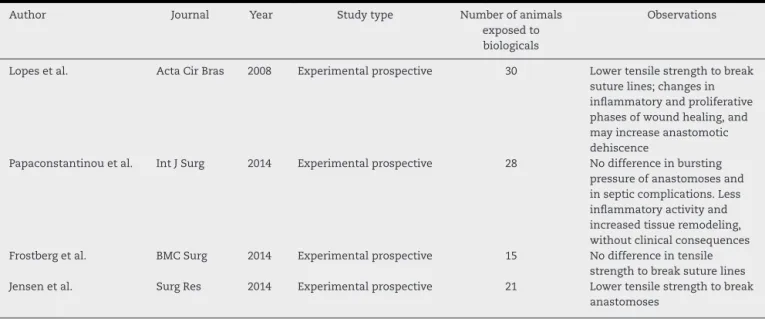
Table3–MainexperimentalstudiesanalyzingtheimpactoftheuseofbiologicalsinpostoperativecomplicationsinCD.
Author Journal Year Studytype Numberofanimals
exposedto biologicals
Observations
Lopesetal. ActaCirBras 2008 Experimentalprospective 30 Lowertensilestrengthtobreak suturelines;changesin inflammatoryandproliferative phasesofwoundhealing,and mayincreaseanastomotic dehiscence
Papaconstantinouetal. IntJSurg 2014 Experimentalprospective 28 Nodifferenceinbursting pressureofanastomosesand insepticcomplications.Less inflammatoryactivityand increasedtissueremodeling, withoutclinicalconsequences Frostbergetal. BMCSurg 2014 Experimentalprospective 15 Nodifferenceintensile
strengthtobreaksuturelines Jensenetal. SurgRes 2014 Experimentalprospective 21 Lowertensilestrengthtobreak
anastomoses
A study from Greece sought possible effects of IFX in
intestinalanastomosesinrats.Afterresectionofthe
termi-nal ileum in their animals, the authors proceeded with a
macroandmicroscopicanalysisofanastomoses,besides dos-ingsomecytokinesbyimmunohistochemistry.Inthisstudy,
there was no difference in anastomosis bursting pressure,
aswellasinsepticcomplicationsinanimalsexposedtoIFX
versuscontrols.Additionally,theauthorsfoundanincreased expressionofTGF-beta1,MMP2andcollagenVinthose
ani-malspreviouslyexposedtoIFX,showinglessinflammatory
activityandincreasedtissueremodeling,butwithoutclinical consequencesfortheanimals.35
Tworecentstudieshavetriedtoanalyzesimilaraspects,
butinrabbitexperimentalmodels.Frostbergetal.,in
anas-tomoses performed in30 rabbits (15 with asingle dose of
IFX10mg/kg)foundnodifferencebetweengroupsintermsof
tensilestrengthtobreakthesuturelines.36Inanother
exper-imentalstudyfromDenmark,Jensenetal.showedopposite
results.In32operatedrabbits,theseauthorsverifiedthatless
tensilestrengthwouldbeusedtobreaktheanastomosesin
rabbitspreviouslyexposed toIFX(1.94±0.44NinIFXgroup versus3.33±0.39Ninplacebogroup,p<0.001).37Theresults ofthemainexperimentalstudiesonthissubjectaredetailed inTable3.
Final
considerations
Inshort,thecontroversyabouttherealimpactofbiological
agentsper se on the postoperativeoutcomes of abdominal
surgerywithresectioninCDpatientsstillpersists.38Thereis asignificantdiversityinmethodologiesusedinreviewed
ret-rospectivestudiesandinmeta-analysespublished.Theonly
prospectivestudyonthesubjectsuggeststhatpatientswith
higherserumlevelsofIFXcouldpresenthigherratesof
post-operativecomplications,butthesampleofpatientsineach
subgroupwassmall.ManystudiesintermingledCDwith
ulcer-ativecolitispatients;thismayalsohaveimpliedsomebiasto theirrespectiveresults.Somestudiesfocusedonoverall com-plications,othersonlyininfectiouscomplications,andeven
othersexclusivelyonsurgicalcomplications,whichpreventa detailedconclusiononthesubject.Acontrolled,multicenter, prospectivestudycalledPUCCINItrialiscurrentlybeing con-ductedintheUnitedStates.39Itisexpectedthatmoresolid answerswillbeobtainedinastudylikethis,morerobustand withahigherlevelofevidence.Associatedfactorssuchas pre-vioususeofcorticosteroidsandmalnutritionshouldalwaysbe consideredinpatientsusingbiologicaltherapybefore
abdom-inal surgical procedures in CD patients. An individualized
decisiononthetypeofprocedureandonthebesttimingfor
itsexecutionshouldbetaken;thesurgeonmuststudythe sit-uationasawhole,notconsideringonlythetypeofmedication usedbythepatient.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.NivatvongsS,GordonPH.Crohn’sdisease.In:GordonPH, NivatvongsS,editors.Principlesandpracticeofsurgeryofthe colon,rectumandanus.3rded.NewYork:Taylor&Francis; 2007.p.819–908.
2.TarganSR,HanauerSB,VanDeventerSJH,MayerL,Present DH,BraakmanT,etal.Ashort-termstudyofchimeric monoclonalantibodycA2totumornecrosis-factoralfafor Crohn’sdisease.NEnglJMed.1997;337(15):1029–35.
3.HanauerSB,FeaganBG,LichtensteinGR,MayerLF,Schreiber S,ColombelJF,etal.MaintenanceinfliximabforCrohn’s disease:theACCENTIrandomisedtrial.Lancet. 2002;359:1541–9.
4.SandsBE,AndersonFH,BernsteinCN,CheyWY,FeaganBG, FedorakRN,etal.Infliximabmaintenancetherapyfor fistulizingCrohn’sDisease.NEnglJMed.2004;350:876–85.
5.VermeireS,VanAsscheG,RutgeertsP.Reviewarticle:altering thenaturalhistoryofCrohn’sdisease:evidenceforand againstcurrenttherapies.AlimentPharmacolTher. 2006;25:3–12.
resectionisassociatedwithadversepostoperativeoutcomes inCrohn’spatients.JGastrointestSurg.2008;12(10):
1738–44.
7. RizzoG,ArmuzziA,PuglieseD,VerboA,PapaA,MatanaC, etal.Anti-TNF-alphatherapiesdonotincreaseearly postoperativecomplicationsinpatientswithinflammatory boweldisease.AnItaliansingle-centerexperience.IntJ ColorectalDis.2011;26:1435–44.
8. KopylovU,Ben-HorinS,ZmoraO,EliakimR,KatzLH. Anti-tumornecrosisfactorandpostoperativecomplications inCrohn’sdisease:systematicreviewandmeta-analysis. InflammBowelDis.2012;18:2404–13.
9. SerradoriT,GermainA,ScherrerML,AyavC,PerezM,Romain B,etal.Theeffectofimmunetherapyonsurgicalsite infectionfollowingCrohn’sdiseaseresection.BrJSurg. 2013;100(8):1089–93.
10.SyedA,CrossRK,FlasarMH.Anti-tumornecrosisfactor therapyisassociatedwithinfectionsafterabdominalsurgery inCrohn’sdiseasepatients.AmJGastroenterol.
2013;108:583–93.
11.RosenfeldG,QianH,BresslerB.Therisksofpost-operative complicationsfollowingpre-operativeinfliximabtherapyfor Crohn’sdiseaseinpatientsundergoingabdominalsurgery:a systematicreviewandmetaanalysis.JCrohnsColitis. 2013;7:868–77.
12.NarulaN,CharletonD,MarshallJK.Meta-analysis: peri-operativeanti-TNF␣treatmentandpost-operative
complicationsinpatientswithinflammatoryboweldisease. AlimentPharmacolTher.2013;37:1057–64.
13.El-HussunaA,KragA,OlaisonG,BendtsenF,GluudLL.The effectofantitumornecrosisfactoralphaagentson
postoperativeanastomoticcomplicationsinCrohn’sdisease: asystematicreview.DisColonRectum.2013;56(12):
1423–33.
14.YangZP,HongL,WuQ,WuKC,FanDM.Preoperative infliximabuseandpostoperativecomplicationsinCrohn’s disease:asystematicreviewandmeta-analysis.IntJSurg. 2014;12(3):224–30.
15.LauC,DubinskyM,MelmedG,VasiliauskasE,BerelD, McGovernD,etal.Theimpactofpreoperativeserum anti-TNF␣therapylevelsonearlypostoperativeoutcomesin
inflammatoryboweldiseasesurgery.AnnSurg. 2015;261:487–96.
16.TayGS,BinionDG,EastwoodD,OttersonMF.Multivariate analysissuggestsimprovedperioperativeoutcomeinCrohn’s diseasepatientsreceivingimmunomodulatortherapyafter segmentalresectionand/orstrictureplasty.Surgery. 2003;134:565–72.
17.ColombelJF,LoftusEVJr,TremaineWJ,PembertonJH,Wolff BG,Young-FadokT,etal.Earlypostoperativecomplications arenotincreasedinpatientswithCrohn’sdiseasetreated perioperativelywithinfliximaborimmunosuppressive therapy.AmJGastroenterol.2004;99:878–83.
18.MarchalL,D’HaensG,VanAsscheG,VermeireS,NomanM, FerranteM,etal.Theriskofpost-operativecomplications associatedwithinfliximabtherapyforCrohn’sdisease:a controlledcohortstudy.AlimentPharmacolTher. 2004;19(7):749–54.
19.KunitakeH,HodinR,ShellitoPC,SandsBE,KorzenikJ, BordeianouL.Perioperativetreatmentwithinfliximabin patientswithCrohn’sdiseaseandulcerativecolitisisnot associatedwithanincreasedrateofpostoperative complications.JGastrointestSurg.2008;12(10): 1730–6.
20.IndarAA,Young-FadokTM,HeppellJ,EfronJE.Effectof perioperativeimmunosuppressivemedicationonearly outcomeinCrohn’sdiseasepatients.WorldJSurg. 2009;33:1049–52.
21.NasirBS,DozoisEJ,CimaRR,PembertonJH,WolffBG, SandbornWJ,etal.Perioperativeanti-tumornecrosisfactor therapydoesnotincreasetherateofearlypostoperative complicationsinCrohn’sdisease.JGastrointestSurg. 2010;14(12):1859–65.
22.KotzePG,AlbuquerqueIC,SobradoCW.Biologicaltherapy doesnotincreasepostoperativecomplicationsaftermajor abdominalsurgeryinCrohn’sdiseaseBrazilianpatients. InflammBowelDis.2011;17(12):S43.
23.CanedoJ,LeeSH,PintoR,Murad-RegadasS,RosenL,Wexner SD.SurgicalresectioninCrohn’sdisease:is
immunosuppressivemedicationassociatedwithhigher postoperativeinfectionrates?ColorectalDis.2011;13:1294–8.
24.El-HussunaA,AndersenJ,BisgaardT,JessP,HenriksenM, OehlenschlagerJ,etal.Biologictreatmentor
immunomodulationisnotassociatedwithpostoperative anastomoticcomplicationsinabdominalsurgeryforCrohn’s disease.ScandJGastroenterol.2012;47:662–8.
25.KasparekMS,BruckmeierA,BeigelF,MüllerMH,BrandS, MansmannU,etal.Infliximabdoesnotaffectpostoperative complicationratesinCrohn’spatientsundergoingabdominal surgery.InflammBowelDis.2012;18:1207–13.
26.MascarenhasC,NunooR,AsgeirssonT,RiveraR,KimD, HoedemaR,etal.Outcomesofileocolicresectionandright hemicolectomiesforCrohn’spatientsincomparisonwith non-Crohn’spatientsandtheimpactofperioperative immunosuppressivetherapywithbiologicsandsteroidson inpatientcomplications.AmJSurg.2012;203:
375–8.
27.NørgårdBM,NielsenJ,QvistN,GradelKO,deMuckadellOB, KjeldsenJ.Pre-operativeuseofanti-TNF-␣agentsandthe
riskofpostoperativecomplicationsinpatientswithCrohn’s disease–anationwidecohortstudy.AlimentPharmacolTher. 2013;37:214–24.
28.WatermanM,XuW,DinaniA,SteinhartAH,CroitoruK, NguyenJC,etal.Preoperativebiologicaltherapyand short-termoutcomesofabdominalsurgeryinpatientswith inflammatoryboweldisease.Gut.2013;62:387–94.
29.BaffordAC,PowersS,HaC,KruseD,GorfineSR,ChessinDB, etal.Immunosuppressivetherapydoesnotincrease operativemorbidityinpatientswithCrohn’sdisease.JClin Gastroenterol.2013;47:491–5.
30.BillioudV,FordAC,TedescoED,ColombelJF,RoblinX, Peyrin-BirouletL.Preoperativeuseofanti-TNFtherapyand postoperativecomplicationsininflammatoryboweldiseases: ameta-analysis.JCrohnsColitis.2013;7:853–67.
31.KraneMK,AllaixME,ZoccaliM,UmanskiyK,RubinMA,Villa A,etal.Preoperativeinfliximabtherapydoesnotincrease morbidityandmortalityafterlaparoscopicresectionfor inflammatoryboweldisease.DisColonRectum. 2013;56(4):449–57.
32.MyrelidP,Marti-GallostraM,AshrafS,SundeML,TholinM, OreslandT,etal.ComplicationsinsurgeryforCrohn’sdisease afterpreoperativeantitumournecrosisfactortherapy.BrJ Surg.2014;101(5):539–45.
33.PapaconstantinouI,ZeglinasC,GazouliM,NastosK, YiallourouA,PapaloisA,etal.Theimpactofperi-operative anti-TNFtreatmentonanastomosisrelatedcomplicationsin Crohn’sdiseasepatients.Acriticalreview.JGastrointestSurg. 2014;18(6):1216–24.
34.LopesJV,FreitasLA,MarquesRD,BoccaAL,SousaJB,Oliveira PG.Analysisofthetensilestrengthonthehealingofthe abdominalwallofratstreatedwithinfliximab.ActaCirBras. 2008;23(5):441–6.
36.FrostbergE,StrömP,GerkeO,QvistN.Infliximab’sinfluence onanastomoticstrengthanddegreeofinflammationin intestinalsurgeryinarabbitmodel.BMCSurg.2014;14:23.
37.JensenJS,PetersenNB,BiaginiM,BollenP,QvistN.Infliximab treatmentreducestensilestrengthinintestinalanastomosis. JSurgRes.2015;193:145–52.
38.KotzePG,CoyCS.Theimpactofpreoperativeanti-TNFin surgicalandinfectiouscomplicationsofabdominal
proceduresforCrohn’sdisease:controversystillpersists.Am JGastroenterol.2014;109(1):139.