w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Preoperative
staging
of
rectal
cancer
with
MRI:
correlation
with
pathologic
staging
Soraia
Filipa
Macado
Abreu
a,b,
Sandra
Fátima
Fernandes
Martins
a,b,c,∗ aLifeandHealthSciencesResearchInstitute(ICVS),SchoolofHealthSciences,UniversityofMinho,Braga,PortugalbICVS/3B’s,PTGovernmentAssociateLaboratory,Braga/Guimarães,Portugal
cSurgeryDepartment,HospitalarCenterofTrás-os-MonteseAltoDouro,DistritodeVilaReal,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received20December2014 Accepted20February2015 Availableonline20April2015
Keywords: Rectalcancer
Pelvicmagneticresonance Accuracy
Sensibility Specificity
a
b
s
t
r
a
c
t
Introduction:Anaccuratepreoperativerectalcancerstagingiscrucialtothecorrect man-agement of the disease. Despitegreat controversy around this issue, pelvic magnetic resonance(RM)issaidtobetheimagiologicstandardmodality.Thisworkaimedto evalu-atemagneticresonanceaccuracyinpreoperativerectalcancerstagingcomparingwiththe anatomopathologicalresults.
Methods:Wecalculatedsensibility,specificity,positive(VPpositive)andnegative(VP neg-ative) predictivevalues foreachTandN.We evaluatedtheconcordancebetweenboth methodsofstagingusingtheCohenweightedK(Kw),andthroughROCcurves,weevaluated
magneticresonanceaccuracyinrectalcancerstaging.
Results:41patientsmettheinclusioncriteria.Weachievedanefficacyof43.9%forTand61% forNstaging.Therespectivesensibility,specificity,positiveandnegativepredictivevalues are33.3%,94.7%,33.3%and94.7%forT1;62.5%,32%,37.0%and57.1%forT2;31.8%,79%, 63.6%and50%forT3and27.8%,87%,62.5%and60.6%forN.Weobtainedapoorconcordance forTandNstagingandtheanatomopathologicalresults.TheROCcurvesindicatedthat magneticresonanceisineffectiveinrectalcancerstaging.
Conclusion: Magneticresonancehasamoderateefficacyinrectalcancerstagingandthe majordifficultyisindifferentiatingT2andT3.
©2015SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
Estadiamento
pré-operatório
do
câncer
do
reto
por
ressonância
magnética:
correlac¸ão
com
estadiamento
anatomopatológico
Palavras-chave: Câncerdoreto
r
e
s
u
m
o
Introduc¸ão: Umestadiamentopré-operatóriodoCâncerdoReto(CR)éessencialnagestãoda doenc¸a.Apesardegrandecontrovérsia,aressonânciamagnéticapélvica(RM)éapontada
∗ Correspondingauthor.
E-mail:[email protected](S.F.F.Martins). http://dx.doi.org/10.1016/j.jcol.2015.02.005
Ressonânciamagnéticapélvica Acuidade
Sensibilidade Especificidade
comomodalidadeimagiológicastandard.Comestetrabalhopretendeu-seavaliaraacuidade daRMnoestadiamentodoCR,comparandocomosresultadosanatomopatológicosdapec¸a cirúrgica.
Materiaisemétodos: Calculou-seasensibilidade,especificidade,valorpreditivopositivo(VP positivo)enegativo(VPnegativo)paraTeN.Avaliou-seaconcordânciaentreambasas formasdeestadiamentoatravésdovalordeKdeCohenponderado(Kw)e,atravésdecurvas ROC,avaliou-seaprecisãodoestadiamentoporRM.
Resultados: 41doentescumpriramoscritériosdeinclusão.Obteve-seumaeficáciade43.9% paraTe61%paraN.Verificou-seumasensibilidade,especificidade,VPpositivoenegativo, respectivamente,de33.3%,94.7%,33.3%e94.7%paraT1,62.5%,32%,37.0%e57.1%paraT2, 31.8%,79%,63.6%e50%paraT3,27.8%,87%,62.5%e60.6%paraN.Aconcordânciacalculada foipobreparaTeN.AscurvasROCindicaramqueoestadiamentodoCRporRMfoiineficaz. Conclusão: ARMapresentaacuidademoderadanoestadiamentodoCR,ondeamaior difi-culdadeestánadistinc¸ãoentreT2-T3.
©2015SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
The incidence and mortality of oncological diseases have increased at an alarming rate worldwide, and according toWorld Health Organization, the incidenceofcancer will increaseto22million/yearinthenexttwodecades.1
In Portugal, colorectal cancer (CRC) is the second most frequentcancerinbothmenandwomen,withanoverall inci-denceof14.5%and15.7%mortality.In2012,thisdiseasewas appointedasthesecondleadingcauseofcancerdeathinboth genders.2Rectalcancer(RC),inparticular,exhibitedin north-ernregionofthiscountryin2008anincidenceof24.6/1,00,000 inhabitants;aprogressiveincreaseinthisvaluesince1999was found.InthedistrictofBraga,itsincidenceinthisyearwas 16.8/1,00,000inhabitants.3
RCprognosishasimprovedgreatlyinrecentdecadesand this was mainly due to advances in preoperative staging, whichwas reflectedinthe therapeuticapproach,4 wherea changewasobserved,fromapurelysurgicaltreatmenttoa multidisciplinaryapproach,5,6loweringthelowerlocal recur-rencerateto11%andimprovingthesurvivalrateat5yearsto 58%,7comparedtopreviousvalues(27and48%,respectively).5 PreoperativestagingofRCisdividedintolocalandremote staging.8–10 Theinformation(bothclinicalandpathological) gatheredfrom thestagingisgroupedaccording to “Tumor-Node-Metastasis”(TNM)classificationoftheAmericanJoint Committee on Cancer in different prognostic groups or anatomicalstages.11,12 TandNstagesarethebest determi-nantsofprognosis,beingcriticalcomponentsofpreoperative staging.13Thus,inadditiontotheuseofareliableimaging modalityand withhigh accuracyinpreoperativestagingof CRbeacrucialprognosisfactor,14 thisprocedurealsohelps in choosing the best therapeutic strategy, enabling a bal-ance between oncologicalsafety and quality of life ofthe patient.10,12
Nowadays,thereareseveralimagingmodalitiesfor preop-erativestagingofRC,includingcomputedtomography(CT), pelvicmagneticresonance imaging(MRI),endorectal ultra-sound(EUS),andpositronemissiontomography(PET).10
EUS and MRI are the main instruments ofpreoperative staging.15 However, there is no consensus about the best method.5,16SeveralstudiessuggestMRIasbeingsuperiorto EUS,9,17–20andthereforeMRIistheroutineimagingmodality forpreoperativestagingofRC.5,21AstoTstaging,MRIshows anacuitybetween55and86%;astoNstaging,theaccuracy variesfrom39to95%.5
InRCstaging,themainroleofMRIliesintheevaluation oftumorsinadvancedandocclusivestages.15,22Withrespect tostagesT3andT4,sensitivityandspecificityof74and76% (forT3)and82and96%(forT4)wereobserved,respectively.22 ForT1andT2stages,MRIislesssensitiveversusEUS,withno differencerelativetoT3andT4stages.16
Detection of N isthe biggest challenge of any imaging examination,with66%sensitivityofMRIinitsevaluationand 76%specificity.5
ThisstudyaimstoevaluatetheaccuracyofMRinthe pre-operativestagingofRC,comparedtotheanatomopathological resultofthesurgicalspecimen.
Materials
and
methods
Population
Thetargetpopulationforthisstudyconsistsof216patients withhistologicaldiagnosisofRCtreatedintheGeneralSurgery Service,HospitaldeBraga(HB)betweenJanuary1st,2007and December31,2013.
Inclusion criteria forthis study were:patientswith his-tological diagnosis ofrectaladenocarcinoma; patientswith a conclusive preoperative staging by MRI, and patients withpathology stagingresultsbasedonthe surgical speci-men.
Table1–MRandanatomopathologicalstagingrelatedto TandN.
RMstaging Anatomopathologicalstaging Frequency(%) Frequency(%)
T0 0(0) 0(0)
T1 3(7.2) 3(7.2) T2 27(65.9) 16(39.0) T3 11(26.8) 22(53.7)
T4 0(0) 0(0)
N0 36(87.8) 23(56.1) N+ 5(12.2) 18(43.9)
Sample
A convenience sample of 41 patients who meet inclu-sion/exclusioncriteriapreviouslydefinedwasstudied.
Datacollection
Clinicalandstagingdatacollectedinclude:age,gender, onco-logicalhistory,tumorlocation,andT/Nstagingbymeansof MRI.
PathologicaldatacomprisethehistologicaltypeandTNM staging.
Follow-updataarerelatedtotheoccurrenceofrelapseand death.
ThisprojectwasapprovedbyHB’sEthicsCommitteeand alsobyEthicsSubcommitteeforLifeandHealthSciences.
Statisticalanalysis
Thecollected datawere organized inan Excel(Microsoft®
Office2010)database, andthe StatisticalPackageforSocial Sciences(SPSS)version22.0(SPSSInc.,Chicago,IL,USA)was alsoused.
A descriptive analysis of the variables under study, to providefrequencies,meansandstandarddeviations,was per-formed.
Sensitivity,specificity,positiveandnegativepredictive val-ues(PV)ofRMstaging,relatedtoTandN,werecomparedwith pathologyresults.Forthispurpose,theonlinetoolMedCalc®
availableinhttp://www.medcalc.org/calc/diagnostictest.php, was used. Efficacy was calculated by the formula (TP+TN/n)and theconfidenceinterval (CI)bytheformula: P−Z×√P(1−P)/√n;P+Z×√P(1−P)/√N.
The agreement between the staging results obtained by MRI and anatomopathological study was assessed by calculating the value of weighted Cohen’s Kappa (Kw); to this end, we used the online toolVassarStats, available in http://vassarstats.net/kappa.html.AvalueofKwbetween0.00 and 0.20 indicates poor agreement; between0.21 and 0.40 reveals a considerable agreement; between 0.41 and 0.60, pointstoamoderateagreement;between0.61and0.80 indi-catesa good agreement;and between0.81 and 1.00shows excellentagreement.23
Finally,usingSPSSprogram,weusedROCcurvesfora com-parativestudy ofMRIandanatomopathological staging,by meansofareaunderthecurve(AUC)calculation.ROCcurve withAUCassessmentisagoodpredictoroftheaccuracyof
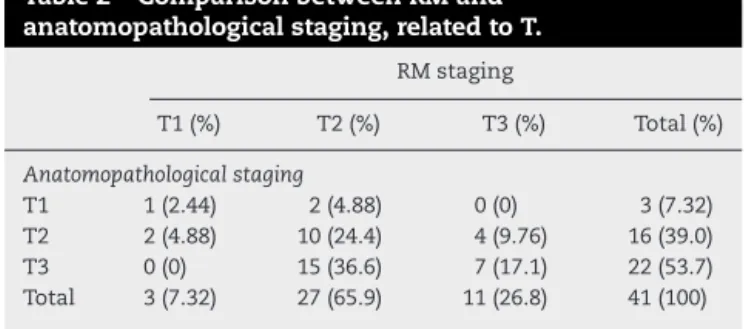
Table2–ComparisonbetweenRMand anatomopathologicalstaging,relatedtoT.
RMstaging
T1(%) T2(%) T3(%) Total(%)
Anatomopathologicalstaging
T1 1(2.44) 2(4.88) 0(0) 3(7.32) T2 2(4.88) 10(24.4) 4(9.76) 16(39.0) T3 0(0) 15(36.6) 7(17.1) 22(53.7) Total 3(7.32) 27(65.9) 11(26.8) 41(100)
atest.TheclosertheAUCisto1,thebettertheexamination is.Values≤0.50representapoororineffectivetest;between ≥0.70and<0.80indicateantestwithaverageorreasonable
accuracy;andvalues≥0.80predictagoodorexcellenttest.24 Forall tests,it wasassumedasignificanceof0.05anda confidenceinterval(CI)of95%.
Results
Samplecharacterization
Thestudypopulationconsistsof41subjectswhomeet inclu-sionandexclusioncriteria.Ofthese,58.5%(n=24)aremale, agedbetween31and88years.
In12.2%(n=5)ofpatients,thereisapersonalhistoryof anothercancer.
As for tumor localization,14.6% (n=6) ofthe casesare locatedinthelowerthird,68.3%(n=28)inthemiddlethirdand 17.1%(n=7)intheupperthirdoftherectum.Disease recur-rencewasobservedin22%(n=9)patients.UntilAugust2014 therewere10deathsinthestudypopulation.
Tstaging
RegardingMRtumorstaging,7.32%(n=3)ofthetumorsare classifiedasT1,65.9%(n=27)arestagedasT2and26.8%(n=11) asT3.Withregardtoanatomopathologicalstagingofsurgical specimens,7.32%(n=3)neoplasmsareclassifiedasT1,39% (n=16)arestagedasT2and53.7%(n=22)asT3(Table1).
Table3–KwvaluesrelatedtoTandNstaging.
Kw(95%CI) p
T 0.14(0–0.38) >0.05 N 0.16(0–0.42) >0.05
ThevalueofKwforTstagingwascalculated,inorderto
determinethecorrelationbetweenMRversus anatomopatho-logical staging. There is poor agreement between the two formsofstaging:Kw=0.14(95%CI,0–0.38)p>0.05(Table3).
Theevaluation of MRI stagingaccuracy, by formulating ROCcurvesandAUCdetermination,revealsanAUCvalueof 0.26(95%CI,0.00–0.54),p=0.18forT1,0.46(95%CI0.28–0.64), p=0.63forT2and0.61(95%CI,0.43–0.78),p=0.24forT3(Fig.1).
EstadiamentoN
WithrespecttoNstagingdonebyMRandshowninTable1, 87.8% (n=36)of all tumorsare classified as N0, and 12.2% (n=5)asN+. Astoanatomopathologicalstagingofsurgical specimens,56.1% (n=23) ofthe tumorsdonothave lymph nodeinvolvement;in26.8%(n=11)thereisaN1staging,and 9.76%(n=4),receivedaN2staging.In7.32%(n=3)oftumors isnotpossibletoclassifyN,sincetheminimumof12lymph nodes were not obtained for the analysis. However, since
Table4–ComparisonbetweenRMand anatomopathologicalstaging,relatedtoN.
RMstaging
N0(%) N+(%) Total(%)
Anatomopathologicalstaging
N0 20(48.7) 13(31.7) 33(80.5) N+ 3(7.31) 5(12.2) 8(19.5) Total 23(56.1) 18(43.9) 41(100)
theanalyzedgangliaweremetastasized,forthesakeofthe statisticalanalysisthesegangliaareconsideredasbeingN+. Thus, the anatomopathologicalanalysis, shownin Table3, revealsnodalinvolvementin43.9%(n=18)ofcases,andno suchinvolvementintheremaining56.1%(n=23).
ComparingthestagingrelativetoNobtainedbyRMandby anatomopathologicalanalysis,asubstagingisnotedin31.7% (n=13)ofcases,andanoverstagingin7.32%(n=3).Table4 comparesbothformsofstaging.
Mstaging
AsforMstaging,90.2%(n=37)ofpatientsarestagedasM0and 4.88%(n=2)asM1;in4.88%(n=2)ofcasesitisnotpossibleto determinetheexistenceofdistantmetastases.
1.0
1.0 0.8
0.8 0.6
0.6 0.4
0.4 1 - specificity ROC curve for T1
Sensitivity
0.2
0.2 0.0
0.0
1.0
1.0 0.8
0.8 0.6
0.6 0.4
0.4 1 - specificity ROC curve for T2
Sensitivity
0.2
0.2 0.0
0.0
1.0
1.0 0.8
0.8 0.6
0.6 0.4
0.4 1 - specificity ROC curve for T3
AUC – 0.26 AUC – 0.45
AUC – 0.61 AUC – 0.55
Sensitivity
0.2
0.2 0.0
0.0
1.0
1.0 0.8
0.8 0.6
0.6 0.4
0.4 1 - specificity ROC curve for N
Sensitivity
0.2
0.2 0.0
0.0
Discussion
AprecisepreoperativestagingofCRiscriticalfortheproper managementofthisdisease,sincethetherapeuticstrategies shouldbeindividualized.10,12,25Moreover,thisstagingisalso apredictorofprognosis.12,26
Therefore,theimagingtechniquesusedintumorstaging provedtobedecisive,anditisextremelyimportantto ascer-taintheireffectiveness.26EUSandMRarethemaintoolsof preoperativestaging,butthereisnoconsensusonwhichis thebestmethod5,16;however,severalstudiesindicateMRto besuperiorto EUS;therefore, MRIisthe standard imaging modalityforpreoperativestagingofRCs.9,18–20
Thisstudy wasdesignedwiththeaimtodeterminethe accuracyofMRinthepreoperativestagingprocessforRC.
With regard to T staging, when comparing the staging performed byMR withthe anatomopathological staging, a substagingoccurredin4.88%(n=2)ofcasesstagedbyRMas beingT1;therewasoverstagingin4.88%(n=2)ofpatientsand substagingin36.6%(n=15)ofthosetumorsstagedbyMRIas T2andanoverstagingin9.76%(n=4)patientsstagedasT3. Giventhat, ingeneral,superficialtumors(T1andT2) with-outmetastaticlymphnodesaretreatedsolelywithsurgery, whilelocallyadvanced tumorsor thosewith nodal metas-tases are subjected to primary treatment priorto surgical recession,14 anundertreatmentoccurred in36.6%(n=15)of patients,consideringthatthesesubjectswerestagedasT2, andtheiranatomopathologicalresultsshowedthatactually thesewereT3,andthusdidnotperformprimarytherapy.
ThelargestnumberofcasesofincorrectstagingbyMRIwas observedinthedistinction betweenstagesT2andT3.This mayinpartbeexplainedbythepresenceofadesmoplastic reactioninperitumoraltissues,makingitdifficultto distin-guishbetweenspiculationofperirectalfat,causedsimplyby fibrosis,andthatthatcontainsviabletumorcells.13,16,27
Asforthe4patientswhowere overstagedbyRMasT3, whenactuallythesewereT2tumors,thesecouldhavebeen overtreated.However,thatdidnothappenforreasons unre-latedtothisstudy.
WithrespecttothecalculationoftheMRIsensitivityforT staging,valuesof33.3%forT1,62.5%forT2,and31.8%forT3 wereobserved.Thesevaluesarelowerthan thoseobserved inseveral other studies.10,14,22,28 However, Beaumont et al. obtainedevensmallervaluesinrelationtoT1andT2stages, namely:27%forT1and59%forT2.16
Thevaluesforspecificitywereof94.7%forT1,32%forT2 and79%forT3.WithrespecttoT1andT3,theresultswere consistentwiththebibliography.10,16InthecaseofT2,these valueswerelowerthanthosefoundinmostofthereferred studies.
ThepositivePVcalculatedwas33.3%forT1,37.0%forT2 and63.6%forT3.RegardingnegativeVP,thesevalueswere 94.7%forT1,57.1%forT2and50%forT3.Thesevalueswere lower than thoseobserved byUc¸aret al. andAkasuet al., exceptinthecaseofnegativeVP forT1,whichwassimilar tothatcalculatedbyIannicellietal.4,19
Thediagnosticefficacy fortumorstaginghasbeen ben-efited from improvements due to the development of MR techniques;inearlystudies,theefficiencyreachedabout60%;
currently,thisindicatorisbetween92and94%forTstageand 63%forNstage.5UsuallytheefficiencyincreaseswithTstage andvaries,accordingtosomeauthors,between67and94% or55and86%.23–29 EfficacycalculatedforTstagewas43.9%, particularly90.2%forT1,43.9%forT2,and53.7%forT3.The resultsforTingeneralandforT2andT3werelowerthan thosefoundbyotherauthors.4,19,23,25TheeffectivenessforT1 stagewassimilarthatinanotherstudy.4
Ndetectionisthemostchallengingdetectionofany imag-ingexamination.5Thecriterion“size”fordetectionoflymph nodemetastasesisapoorpredictor,sincenon-tumorenlarged nodescanexist,andthereverseisalsotrue.29Theirregular contourandheterogeneoussignalintensityaremorespecific criteriaformetastazisation.4,17,29
Inthisstudytherewassubstagingin31.7%(n=13)ofcases classified as N0, and overstaging in 7.32% (n=3); in 31.7% (n=13),undertreatmentofsubstagedpatientsoccurred.
Thesensitivity,specificity,positiveVPandVPnegative rel-ative toN were 27.8%,87%, 62.5% and 60.6%, respectively. Thevalueforsensitivitywaslowerthanthosefoundin sev-eralpreviousstudies;however,thespecificityshowedvalues higher thanthose foundinthese samestudies.5,10,13,14,16,19 Positive and negative VPs were similar to those obtained inother studies.16,19 TheeffectivenessofMRfor Nstaging was 61%,afiguresimilartothat foundbyseveralauthors, varyingbetween39and95%.5,14,16,19Theagreementbetween the stagingresultsobtainedbyMRand anatomopathologi-cal results,evaluated byKw valueforTand N,were given as:Kw=0.14,p<0.05andKw=0.16,p<0.05,respectively.These figures revealedapooragreementbetweenthe twostaging forms;additionally,theydifferfrommoststudiesconsulted, whereKwvaluesbetween0.71and0.89forTandbetween0:40 to0:56toNwereobtained.4,14,19ThestudybyTytherleighMG etal.wasthatthatobtainedtheclosestvaluestoours,namely: 0:37(p<0.001)forTstagingand0.25(p<0.002)forNstaging.30 TheevaluationofMRaccuracythroughROCcurveswith AUC determinationshowedvaluesfor AUCof0.26,p=0.18 for T1,0.46, p=0.63 forT2, 0.61,p=12.24 forT3, and 0.40, p=0.40 forNstaging.Thus,RMprovedtobeanineffective orpoormethodforNstaging.Thesevalueswerediscordant withthosefoundbyotherauthors,rangingfrom0.81to0.94 forTstagingandfrom0.57to0.78forNstaging.8
This study has some limitations, suchas the relatively small number ofpatients, particularly those staged as T1. There arealsobiasesassociatedwithretrospectivestudies, suchas selectionbias,and the resultsshouldbe validated by future prospective multicenter studies. MR and anato-mopathological stagingwerenotalwaysmadebythesame radiologistandpathologist;thismaybeanerrorfactor.
In addition, RMbegan operating inRCstagingin HBin 2007.Asinanymodality,thereisalearningcurveassociated withthisimagingtechnique,andthismayhavecontributed tosomeofthereportedstagingerrors.
Finally,publicationbiasmaybeanotherreasonforthe dis-parateresultsfoundinmostoftheliterature.
Conclusion
evaluated the accuracy of MR in the preoperative staging ofRC, comparedtoanatomopathologicalresultsofsurgical specimens.
MRshowedamoderateacuityinRCstaging,withefficacy valuesbetween43.9and90.2%forTstagingand61%forN staging.RMwasmoresensitiveforT2stageandmorespecific forT1and N+stages.Thisimagingmodality revealedlittle sensitivitytobothT1andN+(33.3and27.8%,respectively), beingmoreusefulforexclusion,thantoconfirmthesestages. MoststagingerrorsoccurredonthedistinctionbetweenT2 andT3stages,resultingincasesofundertreatment.
TheagreementbetweenvaluesobtainedbyMRand anato-mopathologicalresultswaspoorforbothTandNstages.Thus, inthisstudy,itwasanineffectiveorpoormethodforRC stag-ing.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. InternationalAgencyforResearchonCancer[homepagena internet].WorldCancerReport;2014.Availableat:
http://www.iarc.fr/en/mediacentre/pr/2014/pdfs/pr224E.pdf [accessed18.06.14].
2. GLOBOCANFactsheet[homepagenainternet].Colorectal cancerestimatedincidence,mortalityandprevalence worldwidein2012;2012.Availableat:
http://globocan.iarc.fr/Pages/factsheetscancer.aspx [accessed18.06.14].
3. Top10–Roreno–RegistoOncológicoRegionaldoNorte [homepagenainternet].Taxasdeincidênciadecancrona regiãoNortedePortugal;2014.Availableat:
http://www.roreno.com.pt/pt/estatisticas/graficos/top-10.html [accessed18.06.14].
4. IannicelliE,DiRenzoS,FerriM,etal.Accuracyof
high-resolutionMRIwithlumendistentioninrectalcancer stagingandcircumferentialmargininvolvementprediction. KoreanJRadiol.2014;15:37–44.
5. TapanÜ,ÖzbayrakM,ThatS.MRIinlocalstagingofrectal cancer:anupdate.DiagnIntervRadiol.2014;20:390–8. 6. SauerR,BeckerH,HohenbergerW,etal.Preoperativeversus
postoperativechemoradiotherapyforrectalcancer.NEnglJ Med.2004;351:1731–40.
7. KarolinskaB,CedermarkG,LundellC,etal.Improved survivalwithpreoperativeradiotherapyinresectablerectal cancerSwedishRectalCancerTrial.NEnglJMed.1997;336: 980–7.
8. BeetsG,Beets-TanR.Pretherapyimagingofrectalcancers: ERUSorMRI?SurgOncolClinNAm.2010;19:733–41. 9. SameeA,SelvasekarCR.Currenttrendsinstagingrectal
cancer.WorldJGastroenterol.2011;17:828–34. 10.HeeHeoS,KimJ,ShinS,JeongY,KangH.Multimodal
imagingevaluationinstagingofrectalcancer.WorldJ Gastroenterol.2014;20:4244–55.
11.EdgeBE,ByrdD,ComptonC,FritzA,GreeneF,TrottiA.AJCC cancerstagingmanual.7thed.NewYork:Springer-Verlag; 2010.p.173–206.
12.DieguezA.Rectalcancerstaging:focusontheprognostic significanceofthefindingsdescribedbyhigh-resolution magneticresonanceimaging.CancerImaging.2013;13:277–97. 13.HalefogluAM,YildirimS,AvlanmisO,SakizD,BaykanA.
Endorectalultrasonographyversusphased-arraymagnetic resonanceimagingforpreoperativestagingofrectalcancer. WorldJGastroenterol.2008;14:3504–10.
14.YimeiJ,RenZ,LuX,HuanZ.Acomparisonbetweenthe referencevaluesofMRIandEUSandtheirusefulnessto surgeonsinrectalcancer.EurRevMedPharmacolSci. 2012;16:2069–77.
15.SwartlingT,KäleboP,DerwingerK,GustavssonB,KurlbergG. Stageandsizeusingmagneticresonanceimagingand endosonographyinneoadjuvantly-treatedrectalcancer. WorldJGastroenterol.2013;19:3263–71.
16.BeaumontC,PandeyT,FrickeG,LaryeaJ,JambhekarK.MR evaluationofrectalcancer:currentconcepts.CurrProbl DiagnRadiol.2013;42:99–112.
17.KlessenC,RogallaP,TaupitzM.Localstagingofrectalcancer: thecurrentroleofMRI.EurRadiol.2007;17:379–89.
18.SmithN,BrownG.Preoperativestagingofrectalcancer.Acta Oncol.2008;47:20–31.
19.AkasuT,IinumaG,TakawaM,YamamotoS,MuramatsuY, MoriyamaN.Accuracyofhigh-resolutionmagneticresonance imaginginpreoperativestagingofrectalcancer.AnnSurg Oncol.2009;16:2787–94.
20.MollR.Diagnosisofrectalcancer:proMRI.DtschMed Wochenschr.2012;137:2164.
21.BattersbyNJ,MoranB,YuS,TekkisP,BrownG.MRimagingfor rectalcancer:theroleinstagingtheprimaryandresponseto neoadjuvanttherapy.ExpertVerGastroenterolHepatol. 2014;8:703–19.
22.LambregtsD.Reginabeets-TanR.Optimalimagingstagingof rectalcancer.EJC.2013;11:38–44.
23.FleissJL.Themeasurementofinterrateragreement. Statisticalmethodsforratesandproportions.2nded.New York:Wiley;1981.p.212–36.
24.HosmerDW,LemeshowS.Appliedlogisticregression.2nded. NewYork:JohnWiley&Sons,Inc.;2000.p.156–64.
25.ChunHK,ChoiD,KimMJ,etal.Preoperativestagingofrectal cancer:comparisonof3-Thigh-fieldMRIandendorectal sonography.AJR.2006;187:1557–62.
26.BurgueteA,ZabalzaJ,IbiricuL,GarcíaJLS,MendiorozFJJ. PreoperativestagingMRIforrectalcancerandpathologic correlation.AnSistSanitNavar.2011;34:167–74.
27.GiustiS,BucciantiP,CastagnaM,etal.Preoperativerectal cancerstagingwithphased-arrayMR.RadiatOncol.2012;7:29. 28.Fernández-EsparrachG,Ayuso-ColellaJ,SendinoO,etal.EUS
andmagneticresonanceimaginginthestagingofrectal cancer:aprospectiveandcomparativestudy.
GastroentestinalEndoscopy.2011;74:347–54.
29.Beets-TanRG,BeetsGL,VliegenRF,etal.Accuracyofmagnetic resonanceimaginginpredictionoftumourfreeresection margininrectalcancersurgery.Lancet.2001;357:497–504. 30.TytherleighMG,VivienN,PittathankalAA,WilsonMJ,Farouk