w w w . r b o . o r g . b r
Updating
Article
Osteochondroma:
ignore
or
investigate?
夽
Antônio
Marcelo
Gonc¸alves
de
Souza
a,
Rosalvo
Zósimo
Bispo
Júnior
b,c,∗aSchoolofMedicine,FederalUniversityofPernambuco(UFPE),Recife,PE,Brazil bSchoolofMedicine,FederalUniversityofParaíba(UFPB),JoãoPessoa,PB,Brazil cUniversityCenterofJoãoPessoa(UNIPÊ),JoãoPessoa,PB,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received23August2013 Accepted31October2013 Availableonline27October2014
Keywords:
Osteochondroma/etiology Osteochondroma/physiopathology Osteochondroma/diagnosis Boneneoplasms
a
b
s
t
r
a
c
t
Osteochondromasareboneprotuberancessurroundedbyacartilagelayer.Theygenerally affecttheextremitiesofthelongbonesinanimmatureskeletonanddeformthem.They usu-allyoccursingly,butamultipleformofpresentationmaybefound.Theyhaveavery charac-teristicappearanceandareeasilydiagnosed.However,anatypicalsite(intheaxialskeleton) and/ormalignanttransformationofthelesionmaysometimesmakeitdifficultto iden-tifyosteochondromasimmediatelybymeansofradiographicexamination.Inthesecases, imagingexaminations thataremorerefinedarenecessary.Although osteochondromas donotdirectlyaffectthesepatients’lifeexpectancy,certaincomplicationsmayoccur,with varyingdegreesofseverity.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Osteocondroma:
ignorar
ou
investigar?
Palavras-chave:
Osteocondroma/etiologia Osteocondroma/fisiopatologia Osteocondroma/diagnóstico Neoplasiasósseas
r
e
s
u
m
o
Osteocondromas sãoprotuberânciasósseas envolvidasporumacamada decartilagem. Atingem, habitualmente,asextremidades dos ossos longosno esqueletoimaturo e os deformam.Emgeralsãoúnicos,masaformadeapresentac¸ãomúltiplapodeser encon-trada.Deaspectobastantecaracterístico,sãodefácildiagnóstico.Contudo,porvezes,a localizac¸ãoatípica(esqueletoaxial)e/ouamalignizac¸ãodalesãopodemdificultarasua prontaidentificac¸ãoporexamesradiográficos.Nessescasos,examesdeimagemmais apura-dossãonecessários.Apesardenãoafetaremdiretamenteaexpectativadevidadoportador, algumascomplicac¸ões,comvariadosgrausdegravidade,podemocorrer.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora Ltda.Todososdireitosreservados.
夽
Pleasecitethisarticleas:deSouzaAMG,BispoJúniorRZ.Osteocondroma:ignorarouinvestigar?.RevBrasOrtop.2014;49:555–564.
∗ Correspondingauthor.
E-mail:[email protected](R.Z.BispoJúnior).
2255-4971/$–seefrontmatter©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
556
rev bras ortop.2014;49(6):555–564Introduction
Debatecontinuesastowhetherosteochondromaisa devel-opmental disorder (pseudotumoral lesion) or a neoplasm.1
Nonetheless, irrespectiveof whetherit is apseudotumoral lesionoramorecommonbenignbonetumor,2itiscertainlyan
exostosis(externalboneproliferationthatdeformsthebone).3
Thisboneprotuberanceisgenerallyfoundintheimmature skeletonofchildrenandadolescents(Fig.1).
AccordingtotheWorldHealthOrganization(WHO), osteo-chondromas are bone projections enveloped bya cartilage coverthatariseontheexternalsurfaceofthebone.1Despite
theirpredominantcomposition ofbone,their growthtakes placeinthecartilaginousportion.4
Theypresent two distinct clinical forms5: singlelesions
(solitary osteochondromas) and several lesions (multiple osteochondromas).
Solitary
osteochondroma
This entity is also known as an osteochondromatous exostosis,1 osteocartilaginous exostosis4,5 or simply
exostosis.2
Multiple
osteochondromas
Among the various synonyms used in the literature, the commonestonesare:hereditarymultipleexostosis,multiple cartilaginousexostosis,hereditaryosteochondromatosisand multiplehereditaryosteochondromatosis.
Fig.1–Anteroposterior(AP)radiograph(A)andlateralradiograph(B)oftheleftknee.Noteexostosis(osteochondroma– arrows)intheproximalregionofthetibiainaskeletallyimmaturepatient.
Epidemiology
Solitaryosteochondroma
This formconstitutes 10% of all bone tumorsand,among these, 35% (20–50%) of the benign tumors.1,4–8 Single
lesions arefoundin85% ofthe individualsdiagnosedwith osteochondroma.5Theexostosisiscommonlyidentified
dur-ingchildhoodoradolescence.1,4
Osteochondromasmorefrequentlyaffecttheappendicular skeleton(upperandlowerlimbs).5Thelongbonesofthelower
limbsarethebonesmostcommonlyaffected.6,9–11Theknee
istheregionmostaffected(40%ofthecases)(Fig.2).5–7,12After
theknee,theproximalportionsofthefemurandthehumerus are thesitespreferentiallyaffected.Afterosteochondromas appearinthelongbones,theyusuallybecomelocatedinthe metaphysisandonlyrarelyinthediaphysis.2Flatboneslike
thescapulaandhipmayalsobeinvolved(Fig.3).5
Despitetheslightpredominanceofthemalegenderover thefemalegenderthathasbeenreportedbysomeauthors,4,5,7
it seemsthatthereisnoeffectivepredilectionaccordingto sex.1
Multiple
osteochondromas
Some authors have reported that the incidence of mul-tiple osteochondromas is 1:50,000 individuals.1,13 Among
patients withexostosis,15%havemultiplelesions.1 Inthis
presentation, osteochondromas tend to be large and ses-sile, withalobulated abundantcartilaginouscover.5 In the
Fig.2–Thelongbonesofthelowerlimbs(kneeregion)aremostcommonlyaffected.(A)Simplelateralradiograph.(B) Computedtomographywith3Dreconstruction.Notelesion(arrows)intheproximalregionofthetibia.
osteochondromashaveapredilectionforthemetaphysisof the long bones, and especially those of the lower limbs (Fig.4).14
Theagesofpatientswithmultiplelesionsare similarto thoseofothers withsingleexostoses, and thereisalsono predilectionaccordingtosex.1
Etiology
The cause of osteochondromas remains unknown. Based onthesimilarityofthecartilaginouscover oftheexostosis tothe growth cartilage (growth plate) ofthe bone, several hypotheseshave been put forward, all of them relating to alterationstothegrowth plate.1 Anotherfact that
corrobo-ratesthe possiblecorrelation betweenthe cartilage (of the osteochondromaand epiphyseal plate) isthat when skele-tal maturity is reached (after adolescence), the growth of the lesion usually also ceases.2 Thus, the lesion seems to
result from separation of a fragment of growth cartilage (from the immature skeleton), which suffers herniation.2
Continuous growth of this loosepiece of cartilage and its subsequentendochondralossificationformsasaliencethat projects from the bone surface, coated with a covering of cartilage.2 However, it is still unclear how this separation
actuallyoccurs.2
Thevariantwithmultiplelesionsisadominant autoso-malalteration15,16 that istransmittedbybothsexes and is
characterizedbythepresenceofseveralosteochondromas.2
Inthisgroup,mostoftheindividualshaveapositivefamily historyand/ormutationinoneoftheEXTgenes.17,18 These
genes(EXT1,EXT2andEXT3)arefoundinchromosomes8,11 and19,respectively.19–22
Clinical
diagnosis
Solitaryosteochondroma
Among solitary osteochondromas, the vast majority are asymptomatic.7,8,15,23 Infact,theyareusuallydiscoveredby
chance.Aftertheyhavebeendetected,theypresent slowly increasingbulgingandhardenedconsistency,butarepainless (Fig.5).1,2
Symptomatic cases are often related to the size and location of the exostosis. In the immature skeleton, the
558
rev bras ortop.2014;49(6):555–564Fig.4–Hereditarymultipleexostosis.(AandB)Intheknees,radiographsshowingmultiplelesionsintheproximalregions ofthetibiasandfibulas.
osteochondromagrowsslowlyand progressivelyalongwith the bone involved, and it stops when skeletal maturity is reached.24
Inafewcases,painofgreaterintensitymaybepresent, associatedwithcomplicationsofamechanicalorigin1 that
arepromotedbytheprojectionofhardtissue(bone)intothe softtissues.14 Whetherduetosimplecontact,compression
orfriction,varyingdegreesofparesthesia,paresis,cracking, edema,rednessorpallorcanbeobserved,dependingonthe anatomicalstructureaffectedbytheexostosis.
In osteochondromas of pedunculate type (see imaging diagnosticssection),acutepainmayoccurduetofracturing ofthebaseofthepediclefollowinglocaltrauma.1,4,14,25
Multipleosteochondromas
Inthemultipleformofthiscondition,lowheight,deformities ofthebonesaffectedanddisproportionbetweenthetrunkand limbscanbeobserved.2,5,14,17,26–28Severeinvolvementofsome
bonespromotesshorteningandosteoarticulardeformity,with
consequentlimitationofjoint rangeofmotion.14Themain
examplesofthiscomprisedeformityoftheforearm(dueto shorteningoftheulna),inequalityofthelengthsofthelower limbsandangling(varusorvalgus)oftheknee(Fig.6).13,29,30
Malignanttransformation
Rapidly increasing lesion size and local pain processes suggest that sarcomatous transformation is occurring in individuals with osteochondroma that was previously asymptomatic.1,16,28,30,31 Continuing growth of the lesion
afterskeletalmaturityisreachedshouldalsoawaken such suspicions. Other clinical findings that are occasionally reportedincludeslightincreasesinsofttissues,elevationof temperatureandlocalerythema.30
Imaging
diagnostics
Simpleradiographs
Theradiographicappearancereflects thecomposite nature ofthelesion,formedbycorticalandmedullarybonetissue,2
whichprojectsoutwardsfromtheaffectedbone.Itisprecisely thecontinuityofthelesionwiththesurfaceofthehostbone thatispathognomonicforosteochondroma.2Thiscontinuity
iseasilyobservedinlesionsthat“inhabit”thelongbones,2in
thestandard radiographicviews(twoimagesinorthogonal planes).However,inplanarbones (pelvisand scapula)and irregularbones(vertebrae),thisrelationshipandconsequently thediagnosismaynotbeevidentonsimpleradiographsalone (Fig.7).2
The characteristic image consists of an external bone protuberance1,4 and it may havea wide base(sessile) or a
Fig.6–Radiographofanindividualwithhereditary multipleexostosis.Notethedeformityoftheforearm(due toshorteningoftheulna).
560
rev bras ortop.2014;49(6):555–564Fig.8–Differenttypesofosteochondroma.Notethatinexamination(A),thelesiononthehumerusissessile(withwide base–arrows),whilein(B),itispedicledorpedunculated(narrowbase[arrow],i.e.lessinrelationtoitsheight).
narrowbase(pedicled or pedunculated)(Fig. 8). Becauseof thesingularappearanceoftheselesions,itispossibleinmost cases,forexample,todoawaywithbiopsiesfordiagnosing them.
The cartilaginous cover is often not visible in these examinations, because its density is similar to that of
the surrounding soft tissues.15 However, cartilaginous
cal-cifications may sometimes be observed.15,23,31 Irregular
calcification is sometimes seen.1 However, on radiographs
with excessive calcification of “flake” type,1
sarcoma-tous transformation of the osteochondroma should be suspected.
Fig.10–Computedtomographyimagesfacilitatelocatingtheexostoses(whiteovalfigures)atanatomicalsitesofgreater complexity(suchasthespine–sacralregion).(A)Axialimage.(B)3Dreconstruction.
Computedtomography
Thistechniquecomplementsradiographsandshowsdetails ofthecontinuityofthecorticalandspongyboneinsidethe lesion32–37andtheirrelationshipwiththeadjacentsofttissues
(Fig.9).Axialtomographicslicesfacilitateinterpretation2 of
thelesionslocatedinanatomicalsitesofgreatercomplexity,23
suchasthespineandthebeltsoftheupperandlowerlimb (Fig.10).
Magneticresonance
Thisisanexaminationthatalsodemonstratesthecorticaland medullarycontinuitybetweentheosteochondromaandhost bone.2Inthesame wayasseeninanormalpieceofbone,
thecorticalboneoftheexostosispresentslowsignalintensity (hyposignal)inallsequences,whereasthemedullary compo-nentcontinuestohavetheappearanceoftheyellowmedulla (Fig.11A).2
Thisisacceptedasthe safestimagingmethodfor eval-uatingstructures adjacent to the osteochondroma and for observingandmeasuringthecartilagecover2,30thatenvelops
theexostosis.Thethicknessofthislayerisusedasacriterion fordifferentiatingsuspectedsarcomatousmalignant transfor-mationfromcartilaginoustissue1,30(Fig.11B).However,there
isnoconsensusofopinionsinthisregard.30Someauthors1,4,38
havesuggestedthatathicknessgreaterthan2cm(inadults) maybeindicativeofmalignanttransformation,whileothers haveacceptedthispossibilitywhenitisgreaterthan1.5cm.2
Ithastobeborne inmindthatduringchildhood,this car-tilagelayerisnaturallythickerthan inthematureskeleton andmayreach3cm.Calcifiedareasofthecoverpresentlow signalintensityinT1andT2-weightedsequences.2However,
highconcentrationsofwaterinthenon-calcifiedportionof thislayershowanintermediatetolowsignalonT1-weighted imagesandahighsignalonT2-weightedimages.2
Bonescintigraphy
Thecartilaginoustissue(cover)oftheexostosismayormay notpresenthighuptakeofradiopharmaceuticals,bothunder conditionsofnormalityandinsituationsofmalignant trans-formation(secondarychondrosarcoma).Forthisreason,bone
scintigraphy does not have great value in differentiating betweenbenignandmalignantcartilaginouslesions.39
Anatomopathological
diagnosis
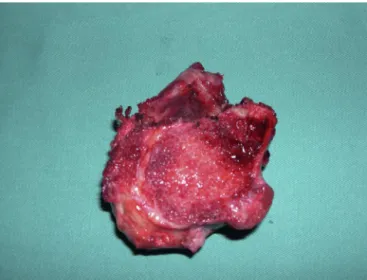
Macroscopicappearance
The lesion surface is lobulated and has an abundant car-tilaginous cover (Fig. 12).5 These are lesions that vary in
562
rev bras ortop.2014;49(6):555–564Fig.12–Intraoperativephotographofexcisionofan osteochondroma.Noteitsmultilobulatedsurfaceand cartilagecover.
size considerably: from 1 to 10cm.2 The cartilage cover
maypresent dimensionsof1–3cminthicknessinyounger patients.6,9,12,32,33,40,41
Microscopicappearance
Solitary and multiple osteochondromas are histologically similar.30 Thelesion presents threelayers1: perichondrium
(mostexternal),cartilage(intermediate)andbone(most inter-nal).
Malignanttransformation
Differentiationfromnormalcartilageisgenerallydonein rela-tiontosecondarychondrosarcomaoflow-grademalignity.30
Lossofcartilagearchitecture,mitoticactivity,presenceofcell atypiaandnecrosisaresomeofthefindingsthatmayindicate secondarymalignanttransformation.1
Treatment
Solitaryosteochondroma
Presenceofanexostosisis,initself,insufficientreasonforits surgicalexcision,especiallyinisolatedcases.42Forindividuals
withsinglelesions,themanagementisexpectantinthegreat majorityofthecases,withsuccessivereturnvisitsbecauseof thechance(albeitsmall)ofmalignanttransformation.
Surgicalremovalisindicatedifthetumorcausespainor functionalincapacity,4eitherduetoneurovascular
compres-sionorduetolimitationofjointmovement(Fig.13).Another situationforsurgicalremovalrelatestofracturingofthebase oftheosteochondroma.25
Multipleosteochondromas
Inthesepatients,thetreatmentismorecomplex.Inthe multi-pleformsofthispathologicalcondition,osteochondromasare
Fig.13–Surgicalresection(specimen)waschosenforthis exostosisthatwascausingvascularcompressioninthe poplitealregion.
removedsurgicallyforcosmeticreasons,43inordertoavoid
progressionofthebonedeformities.Intheforearm,for exam-ple,simpleexcisionofthelesion(inthedistalportionofthe ulna)mayimpedelocaldeformity.44
Malignanttransformation
Sarcomatoustransformationisgenerallytreatedbymeansof widesurgicalresection,withpreservationofthelimb,30while
followingrigorousoncologicalcriteria.
Complications
Amongthepossiblecomplicationsoftheselesionsare frac-tures (generally of pedunculated exostoses, at their base), vascular lesions (formation of pseudoaneurysm) and neu-rological complications (compression of peripheral nerves, which involves the spine or the periarticular regions), for-mation ofa bursa (whichaffects the cartilaginous surface of the lesion, resulting from local friction) and malignant transformation.5,14,30,45 Thislastcomplication, whichisthe
mostfearedofallthecomplications,isveryvariablein fre-quency: insolitaryosteochondromacases,it occurs inless than 1%1,16,23,45; while in patients with multiple lesions it
mayrangefrom1%to30%1,4–6,9,46–48indifferentseries.
How-ever, studies conductedmorerecentlyhave suggestedthat theprevalenceislower:3%to5%inindividualswithmultiple osteochondromatosis.49–54
Final
remarks
Osteochondromasare benignlesions thatdonotaffectlife expectancy.However,theriskofmalignanttransformation(to secondarychondrosarcoma)shouldbetakenonto consider-ation,especiallyincasesofmultipleexostoses.
aviewtomakingaprecisediagnosis.Furthermore,ifthereis clinicalsuspicionofmalignanttransformationand/or radio-graphic alterations in comparison with old examinations, magneticresonance imaging is well indicated for detailed analysisonthethicknessofthecartilaginouscoating.
Insituationsinwhichexcisionoftheosteochondromais chosen,thisisusuallycurative.Recurrenceisseenincasesof incompleteremoval.
Theoverall survivalofpatientswithsarcomatous trans-formation is generally good. However, those with poorly differentiatedlesionshaveamuchworseprognosis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. KhuranaJ,Abdul-KarimF,BovéeJVM.Osteochondroma.In:
FletcherCD,UnniKK,MertensF,editors.Pathologyand
geneticsoftumoursofthesofttissuesandbones.Lyon:IARC
Press;2002.p.234–7.
2. MurpheyMD,ChoiJJ,KransdorfMJ,FlemmingDJ,GannonFH.
Imagingofosteochondroma:variantsandcomplicationswith
radiologic–pathologiccorrelation.Radiographics.
2000;20(5):1407–34.
3. CosteiraO.Termoseexpressõesdapráticamédica.Riode
Janeiro:Farmoquímica;2001.
4. UnniKK.Osteochondroma.Dahlin’sbonetumors:general
aspectsanddataon11,087cases.5thed.Springfield:
Thomas;1996.p.11–23.
5. DorfmanHD,CzerniakB.Osteochondroma.Bonetumors.St.
Louis:Mosby;1998.p.331–46.
6. ResnickD,KyriakosM,GreenwayGD.Osteochondroma.In:
ResnickD,editor.Diagnosisofboneandjointdisorders.3rd
ed.Philadelphia:Saunders;1995.p.3725–46.
7. GiudiciMA,MoserRPJr,KransdorfMJ.Cartilaginousbone
tumors.RadiolClinNorthAm.1993;31(2):237–59.
8. ScarboroughMT,MoreauG.Benigncartilagetumors.Orthop
ClinNorthAm.1996;27(3):583–9.
9. MirraJM.Benigncartilaginousexostoses:osteo-chondroma
andosteochondromatosis.Bonetumors:clinical,radiologic,
andpathologiccorrelations.Philadelphia:Lea&Febiger;1989.
p.1626–59.
10.MilgramJW.Theoriginsofosteochondromasand
enchondromas.Ahistopathologicstudy.ClinOrthopRelat
Res.1983;(174):264–84.
11.KeithA.Studiesontheanatomicalchangeswhich
accompanycertaingrowth-disordersofthehumanbody:I.
Thenatureofthestructuralalterationsinthedisorderknown
asmultipleexostoses.JAnat.1920;54Pt2–3:101–15.
12.UnniKK.Chondrosarcoma(primary,secondary,
dedifferentiated,andclear-cell).Dahlin’sbonetumors:
generalaspectsanddataon11,087cases.5thed.Springfield:
Thomas;1996.p.71–108.
13.SchmaleGA,ConradEU3rd,RaskindWH.Thenaturalhistory
ofhereditarymultipleexostoses.JBoneJointSurgAm.
1994;76(7):986–92.
14.StieberJR,DormansJP.Manifestationsofhereditarymultiple
exostoses.JAmAcadOrthopSurg.2005;13(2):110–20.
15.SteinerGC.Benigncartilagetumors.In:TaverasJM,Ferrucci
JT,editors.Radiology:diagnosis–imaging–intervention.
Philadelphia:JBLippincott;1992.p.1–3.
16.HarmsSE,GreenwayG.Musculoskeletaltumors.In:StarkDD,
BradleyWG,editors.Magneticresonanceimaging.2nded.St.
Louis:MosbyYearBook;1992.p.2132–3.
17.Legeai-MalletL,MunnichA,MaroteauxP,LeMerrerM.
Incompletepenetranceandexpressivityskewingin
hereditarymultipleexostoses.ClinGenet.1997;52(1):12–6.
18.BovéeJV,HogendoornPC.Multipleosteochondromas.In:
FletcherCD,UnniKK,MertensF,editors.WorldHealth
OrganizationClassificationofTumours.Pathologyand
geneticsoftumoursofsofttissueandbone.Lyon:IARCPress;
2002.p.360–2.
19.WuYQ,HeutinkP,deVriesBB,SandkuijlLA,vanden
OuwelandAM,NiermeijerMF,etal.Assignmentofasecond
locusformultipleexostosestothepericentromericregionof
chromosome11.HumMolGenet.1994;3(1):167–71.
20.LüdeckeHJ,JohnsonC,WagnerMJ,WellsDE,TurleauC,
TommerupN,etal.Moleculardefinitionoftheshortest
regionofdeletionoverlapintheLanger-Giedionsyndrome.
AmJHumGenet.1991;49(6):1197–206.
21.ParrishJE,WagnerMJ,HechtJT,ScottCIJr,WellsDE.Molecular
analysisofoverlappingchromosomaldeletionsinpatients
withLanger-Giedionsyndrome.Genomics.1991;11(1):54–61.
22.HechtJT,HogueD,StrongLC,HansenMF,BlantonSH,Wagner
M.Hereditarymultipleexostosisandchondrosarcoma:
linkagetochromosomeIIandlossofheterozygosityfor
EXT-linkedmarkersonchromosomesIIand8.AmJHum
Genet.1995;56(5):1125–31.
23.ResnickD,KyriakosM,GreenwayGD.Tumorsandtumor-like
lesionsofbone:imagingandpathologyofspecificlesions.In:
ResnickD,NiwayamaG,editors.Diagnosisofboneandjoint
disorders.2nded.Philadelphia:Saunders;1988.p.3648–720.
24.MargolisM,McLennanMK.Radiologyrounds.
Osteochondroma.CanFamPhysician.1995;41(216):220–2.
25.TanigawaN,KariyaS,KojimaH,KomemushiA,FujiiH,
SawadaS.Lowerlimbischaemiacausedbyfractured
osteochondromaofthefemur.BrJRadiol.2007;80(952):e78–80.
26.WicklundCL,PauliRM,JohnstonD,HechtJT.Naturalhistory
studyofhereditarymultipleexostoses.AmJMedGenet.
1995;55(1):43–6.
27.McCormickC,DuncanG,TufaroF.Newperspectivesonthe
molecularbasisofhereditarybonetumours.MolMedToday.
1999;5(11):481–6.
28.HennekamRC.Hereditarymultipleexostoses.JMedGenet.
1991;28(4):262–6.
29.ShapiroF,SimonS,GlimcherMJ.Hereditarymultiple
exostoses.Anthropometric,roentgenographic,andclinical
aspects.JBoneJointSurgAm.1979;61(6):815–24.
30.ShahZK,PehWC,WongY,ShekTW,DaviesAM.Sarcomatous
transformationindiaphysealaclasis.AustralasRadiol.
2007;51(2):110–9.
31.GreenspanA.Tumorsofcartilageorigin.OrthopClinNorth
Am.1989;20(3):347–66.
32.KenneyPJ,GilulaLA,MurphyWA.Theuseofcomputed
tomographytodistinguishosteochondromaand
chondrosarcoma.Radiology.1981;139(1):129–37.
33.LangeRH,LangeTA,RaoBK.Correlativeradiographic,
scintigraphic,andhistologicalevaluationofexostoses.JBone
JointSurgAm.1984;66(9):1454–9.
34.HudsonTM,SpringfieldDS,SpanierSS,EnnekingWF,Hamlin
DJ.Benignexostosesandexostoticchondrosarcomas:
evaluationofcartilagethicknessbyCT.Radiology.
1984;152(3):595–9.
35.KobayashiH,KotouraY,HosonoM,FujimotoR,TsuboyamaT,
ItohH,etal.3D-spiralCTofmultipleexostoses.ComputMed
ImagingGraph.1995;19(5):419–22.
36.LeePC,ChenWJ,TuYK,ChenLH.Solitaryosteochondromaof
thelumbarspinewithcordcompression:acasereport.
564
rev bras ortop.2014;49(6):555–56437.MoriwakaF,HozenH,NakaneK,SasakiH,TashiroK,AbeH.
Myelopathyduetoosteochondroma:MRandCTstudies.J
ComputAssistTomogr.1990;14(1):128–30.
38.LeeJK,YaoL,WirthCR.MRimagingofsolitary
osteochondromas:reportofeightcases.AJRAmJRoentgenol.
1987;149(3):557–60.
39.LeeFY,YuJ,ChangSS,FawwazR,ParisienMV.Diagnostic
valueandlimitationsoffluorine-18fluorodeoxyglucose
positronemissiontomographyforcartilaginoustumorsof
bone.JBoneJointSurgAm.2004;86(12):2677–85.
40.MalghemJ,VandeBergB,NoëlH,MaldagueB.Benign
osteochondromasandexostoticchondrosarcomas:
evaluationofcartilagecapthicknessbyultrasound.Skeletal
Radiol.1992;21(1):33–7.
41.GarrisonRC,UnniKK,McLeodRA,PritchardDJ,DahlinDC.
Chondrosarcomaarisinginosteochondroma.Cancer.
1982;49(9):1890–7.
42.BispoJúniorRZ,deSouzaAMG,MelloJúniorCF.
Osteocondroma.In:BispoJúniorRZ,MelloJúniorCF,editors.
OrtopediaBásica.Cap6.RiodeJaneiro:Revinter;2014.p.63–9.
43.BovéeJV.Multipleosteochondromas.OrphanetJRareDis.
2008;3:3.
44.AkitaS,MuraseT,YonenobuK,ShimadaK,MasadaK,
YoshikawaH.Long-termresultsofsurgeryforforearm
deformitiesinpatientswithmultiplecartilaginousexostoses.
JBoneJointSurgAm.2007;89(9):1993–9.
45.SeveroA,CalieronLG,KuhnA.Compressäodonervofibular
comumporosteocondroma:relatodecaso.RevBrasOrtop.
2001;36(9):356–8.
46.MeissnerSA,ViethV,AugustC,WinkelmannW.
Radiology–pathologyconference:osteosarcomaina
cartilaginousexostosisofthefemur.ClinImaging.
2006;30(3):206–9.
47.PierzKA,StieberJR,KusumiK,DormansJP.Hereditary
multipleexostoses:onecenter’sexperienceandreviewof
etiology.ClinOrthopRelatRes.2002;(401):49–59.
48.LeeKC,DaviesAM,Cassar-PullicinoVN.Imagingthe
complicationsofosteochondromas.ClinRadiol.
2002;57(1):18–28.
49.FischgrundJS,CantorJB,SambergLC.Malignantdegeneration
ofavertebralosteochondromawithepiduraltumor
extension:areportofthecaseandreviewoftheliterature.J
SpinalDisord.1994;7(1):86–90.
50.YoungCL,SimFH,UnniKK,McLeodRA.Chondrosarcomaof
boneinchildren.Cancer.1990;66(7):1641–8.
51.NormanA,SissonsHA.Radiographichallmarksofperipheral
chondrosarcoma.Radiology.1984;151(3):589–96.
52.WillmsR,HartwigCH,BöhmP,SellS.Malignant
transformationofamultiplecartilaginousexostosis–acase
report.IntOrthop.1997;21(2):133–6.
53.BellRS.Musculoskeletalimages.Malignanttransformationin
familialosteochondromatosis?CanJSurg.1999;
42(1):8.
54.OstlereSJ,GoldRH,MirraJM,PerlmanRD.Casereport658:
chondrosarcomaoftheproximalphalanxofrightfourth
fingersecondarytomultiplehereditaryexostoses(MHE).




![Fig. 11 – Magnetic resonance images. (A) T1-weighted sagittal image (note hyposignal of the cortical bone and the lesion [open arrows] and hypersignal of the bone medulla in both [filled arrows])](https://thumb-eu.123doks.com/thumbv2/123dok_br/19087714.496069/7.918.504.814.575.1039/magnetic-resonance-weighted-sagittal-hyposignal-cortical-hypersignal-medulla.webp)